
Abstract
The present case report describes the isolation of the fungus Cokeromyces recurvatus from the intestinal tract of a canine patient. Infection by this fungus is rare, having only been reported in 8 human beings and 1 cat. The fungus is not reported to exhibit tissue invasion. Cokeromyces recurvatus is most likely an opportunistic agent, and most cases described involve some degree of immunosuppression.
A 9-year-old spayed female West Highland White Terrier dog was referred to the Iowa State University Lloyd Veterinary Medical Center (Ames, Iowa) for diagnostic evaluation of refractory protein-losing enteropathy (PLE). The dog had been initially presented to the referring veterinarian 6 weeks earlier for decreased appetite and weight loss. Over the next several weeks, progressive gastrointestinal signs including intermittent vomiting and diarrhea were noted. The dog was treated for presumptive immune-mediated chronic enteropathy. Upon presentation, the dog was bright and alert, weighed approximately 6 kg, and had a body condition score of 5 out of 9. Mild hepatomegaly was noted on abdominal palpation. Digital rectal examination revealed soft stool with hematochezia.
Complete blood cell count, serum biochemistry, and urinalysis were performed. The hematologic and biochemical analyses were consistent with enteric plasma protein loss (i.e., PLE), possibly with gastrointestinal bleeding. Urinalysis was interpreted as normal. Direct and indirect fecal examinations for nematode or protozoal parasites were negative. Abdominal ultrasound revealed hyperechoic, perpendicular mucosal striations along the small intestinal mucosa, suggesting intestinal lymphangiectasia as the cause for the PLE. 11 The intestinal bowel loops appeared uniformly normal in thickness with all layers present. Thoracic radiographs were normal.
The dog was anesthetized, and esophagogastroenteroscopy was performed. Multiple endoscopic biopsies of the stomach and duodenum were obtained for histopathologic examination. Gastric, duodenal, and rectal brush cytology was performed using guarded cytology brushes. Gastric cytology revealed mild neutrophilic inflammation with a mixed bacterial population intermixed with occasional large (approximately 50–75 μm) thick-walled yeasts. Duodenal cytology revealed mixed inflammatory infiltrate. Rectal cytology revealed mixed bacteria and frequent large, round-to-oval, deeply basophilic structures, similar to Coccidioides immitis (Fig. 1). Serum was tested for anti–C. immitis immunoglobulin (Ig)G and IgM antibody by agar gel immunodiffusion.
Histologic examination of biopsy specimens revealed moderate lymphoplasmacytic gastroenteritis and lymphangiectasia. Periodic acid–Schiff and Warthin–Starry staining did not reveal fungal organisms. The histologic changes were consistent with idiopathic inflammatory bowel disease causing PLE.
No C. immitis IgG and IgM antibody titers were detected. The rectal brush was submitted for fungal culture by inoculating the collected material onto sheep blood agar, Sabouraud dextrose (SD), a Mycosel, b Emmons SD, a and then incubating at 25°C and 35°C with and without CO2. No growth was found on Mycosel media, and there was overgrowth of Proteus spp. on the blood agar. However, fungal growth was seen on SD at 11–12 days incubated at 25°C with no CO2. Cokeromyces recurvatus was confirmed by observing typical sporangiophores with terminal vesicles and recurring stalks on lactophenol cotton blue staining 4 (Fig. 2).
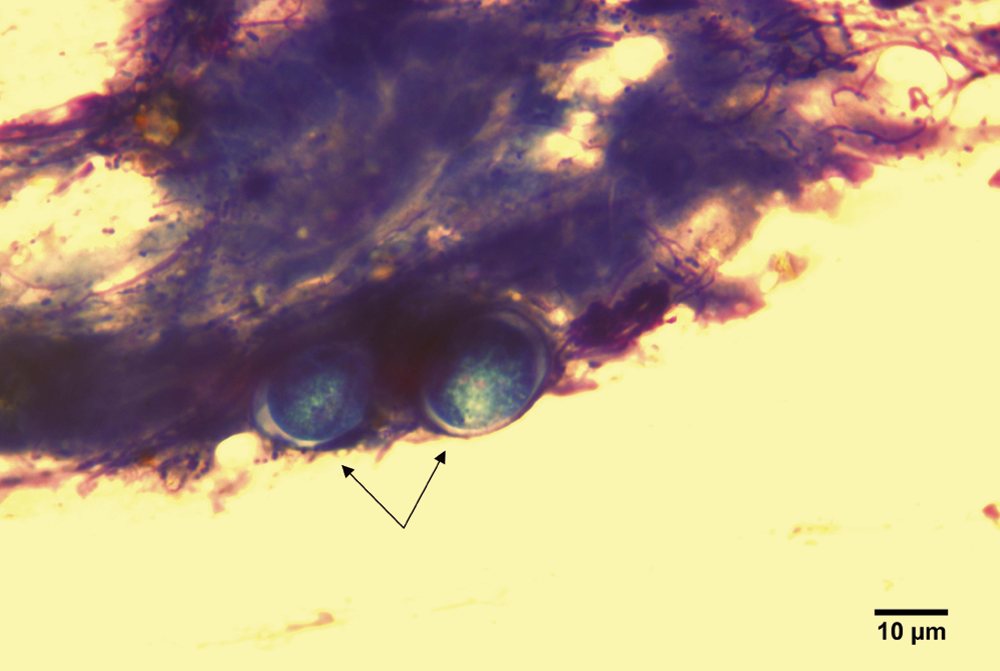
Rectal cytology revealing 2 Cokeromyces recurvatus thick-walled yeast organisms (arrows). Wright stain. Bar = 10 µm.
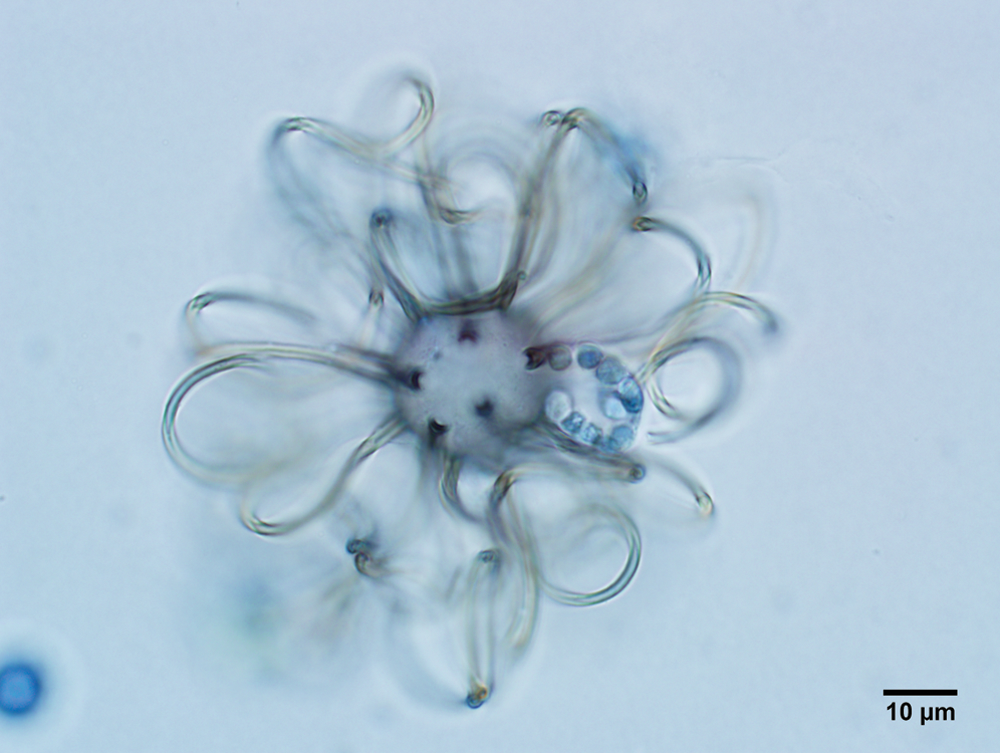
Cokeromyces recurvatus terminal vesicle of sporangiophore with recurving stalks and a sporangiolum. Lactophenol cotton blue stain. Bar = 10 µm.
Earlier case studies have indicated that C. recurvatus may act as an opportunistic pathogen and contribute to the pathogenesis of intestinal inflammation in human beings.2,7-9,12 Based on these earlier reports, the dog was administered anti-fungal treatment. On re-examination 2 weeks later, the dog had lost another 0.318 kg. There was evidence of persistent PLE and gastrointestinal bleeding. Due to the lack of therapeutic improvement and declining patient prognosis, the dog was humanely euthanized, and a necropsy was performed.
Gross changes included a thickened jejunal wall and thick, red–brown luminal contents in the ileum and colon, consistent with intestinal hemorrhage. Gastric and colonic samples were submitted for fungal culture. Histologic examination of the intestines revealed lymphoplasmacytic enteritis. The intestinal crypts were tortuous in areas of more intense lamina proprial inflammation, and moderate numbers of crypt abscesses and dilated villar lymphatic vessels were present. Infectious agents were not observed in periodic acid–Schiff-stained sections. There was no evidence of disseminated fungal disease. Fungal agents were not cultured from either sample.
Cokeromyces recurvatus is a sporangiola-forming dimorphic fungus belonging to the family Thamnidiaceae. 8 It was first cultured in 1949 from rabbit feces in Illinois and has since been isolated from the soil and the feces of several small rodents and lizards in other North American locations.8,10 As a dimorphic fungus, C. recurvatus exists in both yeast and filamentous forms. Its dimorphism may depend on culture medium, incubation temperature, and degree of anaerobiosis. 8
At room temperature in air, C. recurvatus grows as a filamentous fungus. Growth usually appears within 1 week and tan–gray colonies with concentric rings or zones of color are often noted. Cokeromyces recurvatus will transform into a yeast form in conditions that encourage fermentation (i.e., anaerobiosis, increased CO2 concentrations, increased temperatures, pH between 5.8 and 6.5, glucose availability, and inhibitors of respiration or mitochondrial protein synthesis). 8 Cokeromyces recurvatus is a large (30–90 μm), spherical, thick-walled yeast that is similar in morphology to C. immitis and Paracoccidioides brasiliensis.6,8
Differentiation of C. recurvatus from other sporangiola producers may be based upon morphological characteristics, such as the number of cells in the sporangiole, the length and morphology of the sterigmata, and the production of zygospores. Cokeromyces recurvatus produces multi-celled sporangioles on long recurving stalks and zygospores homothallically (without mating), thus allowing for excellent growth within a single isolate. 8 Despite the existence of some serologic tests for zygomycosis, the limited availability and lack of specificity render the tests of minimal clinical benefit in this and other clinical situations. Additionally, experimental molecular techniques have been employed in epidemiologic studies and to determine taxonomic placement; however, such techniques are of little use in making a primary diagnosis. 2
A potential pathogenic role of C. recurvatus has been made in only a few human studies. Immunosuppression was a common thread among these human cases, lending support to the notion that this fungus is an opportunistic agent.1,3,5,7, 12 The fungus has been isolated from the vagina, cervix, gastrointestinal tract, bladder, urine, and pleural and peritoneal fluids of human beings. Cokeromyces recurvatus has also been isolated from the peritoneal cavity of a cat with septic fungal peritonitis associated with intestinal lymphosarcoma. In the feline case report, the fungus was initially misidentified as C. immitis. Similar to infected human beings, the cat was likely immunocompromised due to the underlying neoplasia. 6 Tissue invasion has not been a consistent finding with this organism in human beings or animals, making it difficult to assess the organism’s true pathogenicity. Even with tissue colonization, minimal inflammation is expected. It is theorized that disease pathogenesis is mediated by 1 or more extracellular mycotoxins. 8
In human beings, gastrointestinal disease associated with zygomycosis is relatively uncommon. The stomach is the most common area of the gastrointestinal tract affected, followed by the colon. The small intestine and esophagus are rarely affected. 2 Risk factors associated with gastrointestinal zygomycosis include protein-calorie malnutrition, diarrhea, and gastrointestinal ulceration. 8 The dog in the present report exhibited all of these negative risk factors. Other factors contributing to zygomycosis infection include intercurrent disease caused by diabetes mellitus and/or diabetic ketoacidosis, chronic metabolic acidosis, skin or soft tissue damage, and the prolonged use of broad-spectrum antibiotic and antifungal therapies. 2 Three forms of gastric zygomycosis exist: colonization, infiltration, or vascular invasion. Colonization often occurs in preexisting ulcers and is infrequently fatal. The invasive form involves the formation of necrotic gastrointestinal ulcers. Perforation and peritonitis are potential consequences, and ultimately this form of disease is fatal.8,13 Clinical signs of gastric zygomycosis include abdominal pain, nausea, vomiting, diarrhea, hematemesis, melena, and hematochezia. 2
In view of the fact that the dog of the present report had received immunosuppressive doses of corticosteroids in an effort to manage idiopathic inflammatory bowel disease, it is reasonable to hypothesize that the enteric fungal infection occurred secondary to corticosteroid-induced immunosuppression. The diarrhea, intestinal ulceration, and malnutrition were additional risk factors for impaired barrier function that allowed fungal growth. Little is known about the true pathogenicity of C. recurvatus; however, immunosuppression likely is a contributing risk factor for colonization. Based on the lack of evidence of tissue invasion, it is proposed that this fungus may cause or contribute to disease via extracellular mycotoxins. Lack of tissue invasion also makes infection difficult to diagnose on routine histopathology. Cytology and/or fungal culture may be more reliable diagnostic tools to diagnose C. recurvatus infection in animals. This organism should be considered as a potential complicating disease factor in immunocompromised patients so that the veterinary profession may gain a better understanding of its role in pathogenesis.
Footnotes
Acknowledgements
The authors acknowledge Dr. Heather A. Flaherty, Dr. Jelena Palić, and Ann E. Greazel for their assistance with figures. Acknowledgements also go to Joann Kinyon and Jessica Schnellbacher for their assistance in culturing the C. recurvatus organism.
a.
BD Diagnostic Systems, Sparks, MD.
b.
Remel, Lenexa, KS.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.