
Abstract
A 6-year-old Domestic Shorthair cat was presented with a history of subcutaneous mass of the lateral left hind limb. The subcutaneous mass developed over a period of approximately 16 months subsequent to administration of Feline leukemia virus vaccines. Based on the histopathological and immunohistochemical examination, the subcutaneous mass was diagnosed as vaccine-associated fibrosarcoma with keloidal differentiation.
Vaccine-associated sarcomas have been reported frequently in cats. Epidemiological evidences suggest a strong association between the administration of inactivated Feline leukemia virus (FeLV) and Rabies virus vaccines with subsequent development of soft tissue sarcomas at the vaccination sites.13,14 The prevalence of vaccine-associated sarcoma varies from approximately 1 to 2 cases per 10,000 Rabies virus or FeLV vaccines.10,12 There are rare reports of keloidal fibrosarcomas in dogs.17,20 The current report describes the histopathological and immunohistochemical features of a vaccine-associated fibrosarcoma with keloidal differentiation in a cat.
A 6-year-old, female, spayed Domestic Shorthair cat was presented to a private veterinary practitioner with a history of a painful, subcutaneous mass of the lateral aspect of the left hind limb. The subcutaneous mass (3–4 cm in diameter) had been present for approximately 10 days. The cat had been vaccinated with a FeLV vaccine in April 2008 at the same location on the left hind limb. Another dose of FeLV vaccine was administered in May 2009 at the same location, and the subcutaneous mass was noted in September 2009. A presumptive diagnosis of vaccine-associated fibrosarcoma was made. The mass was surgically excised with wide margins, and tissue samples were submitted to the Louisiana Animal Disease Diagnostic Laboratory, Louisiana State University (Baton Rouge, LA) for histopathological examination. The subcutaneous mass was moderately firm, nodular, pale tan with a central area of necrosis. The tissue sections from the subcutaneous mass were fixed in 10% neutral buffered formalin, routinely processed, paraffin-embedded, sectioned at 5 µm, and stained with hematoxylin and eosin.
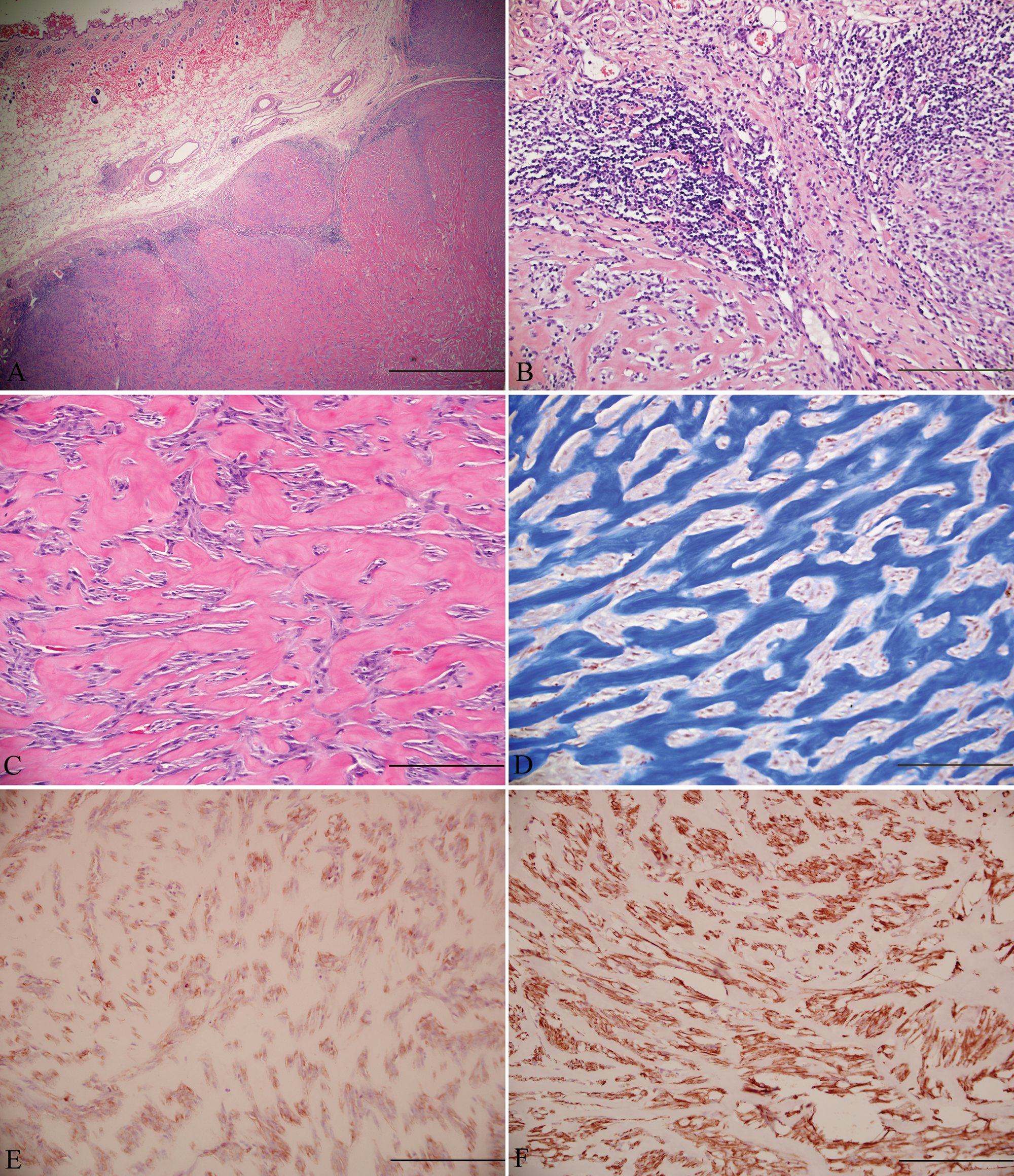
Histologically, the subcutaneous mass was a well-demarcated, moderately cellular, unencapsulated mesenchymal neoplasm with peripheral lymphoid aggregates (Fig. 1A, 1B). The spindle cells were arranged in interlacing streams and bundles, which frequently dissected large thick bundles of well-defined eosinophilic homogeneous hyalinized fibers (Fig. 1C). The eosinophilic homogeneous hyalinized fibers stained deep blue with Masson trichrome stain confirming abundant dense collagen in the neoplasm (Fig. 1D). Neoplastic cells were plump and fusiform with small amounts of eosinophilic fibrillar cytoplasm and indistinct cell borders. Nuclei were elongated to oval with finely stippled to vesicular chromatin and a single nucleolus. Mitotic figures were 27 per 10 high power fields of view. Anisokaryosis and anisocytosis were moderate.
Immunohistochemical staining of formalin-fixed, paraffin-embedded tissue sections was performed for cluster of differentiation (CD)18 (monoclonal mouse anti-feline, clone FE3.9F2), vimentin (monoclonal mouse anti-vimentin antibody, clone V9), and α-smooth muscle actin (α-SMA; monoclonal mouse anti-human antibody, clone 1A4) using streptavidin–biotin–peroxidase method. a The performance of positive and negative controls was within normal limits. All the neoplastic spindle cells showed strong positive immunostaining for vimentin, and approximately 50–60% of these cells also labeled for α-SMA (Fig. 1E, 1F). There were few scattered CD18-positive cells on the periphery of the neoplasm. The histomorphological features of the neoplastic cells, and immunohistochemical and histochemical stains in the current case were indicative of vaccine-associated fibrosarcoma with keloidal differentiation.
Subcutaneous mass; feline.
There are many reports of vaccine-associated fibrosarcomas, but the keloidal variant of fibrosarcoma has not been reported in the cats. Most vaccine-associated sarcomas are categorized as fibrosarcomas. Other types of sarcomas associated with vaccination sites in cats include rhabdomyosarcomas, myxosarcomas, chondrosarcomas, undifferentiated sarcomas, and malignant fibrous histiocytomas.7,12 Vaccine-associated sarcomas are also characterized by presence of follicular aggregates of lymphocytes and small numbers of plasma cells usually located at the tumor periphery, which was consistent with the current case. 8 These lesions occasionally contain large round macrophages with blue gray cytoplasm, most probably associated with phagocytosed adjuvant material. The average interval between tumor development and the post–FeLV vaccine administration is approximately 11 months. 16 The animal in the current case developed a tumor over a period of approximately 16 months following multiple FeLV vaccinations at the site of tumor development.
Keloidal fibrosarcoma is an unusual variant of fibrosarcoma and is characterized by the presence of thick bands of hyalinized collagen. 20 Keloid formation following dermal injury has been hypothesized to result from altered growth factor regulation, aberrant collagen turnover, genetics, and immune dysfunction. 1 The keloid-derived fibroblasts were significantly resistant to Fas-mediated apoptosis. 5 Dysregulation of apoptosis and hypoxia have been implicated in keloid formation.2,18 Keloid formation has also been reported in human beings following vaccination with Bacillus Calmette-Guérin, 4 small pox, 24 and hepatitis B vaccines. 9 Keloids are distinct from hypertrophic scars. Keloids extend beyond the borders of the original wound or inflammatory process and do not regress spontaneously. 21 In human beings, keloids are present as firm nodules that are either skin colored or erythematous, and can be painful or pruritic. 23 The texture of keloid ranges from soft and doughy to rubbery and hard. Histologically, the keloidal collagen is arranged haphazardly or in whorls instead of parallel to the epidermis as in normal tissue and hypertrophic scars. 23 Unlike keloids, hypertrophic scars never occur spontaneously or extend beyond the margins of the scar. 3
In dogs, keloidal fibromas are nodular, plaque like, and gradually blend into the adjacent dermis and/or panniculus. Histologically, canine keloidal fibromas are composed of streams of thick hyalinized collagen surrounded by closely packed plump cells. 20 In contrast, canine keloidal fibrosarcomas are invasive nodular subcutaneous tumors comprised of tightly packed interlacing fascicles of fusiform cells with thick hyalinized collagen. 20 Typical fibrosarcomas are composed of interlacing streams and bundles of spindle cells in a mature collagenous stroma. Fibrosarcomas usually lack hyalinized collagen; however, it has been noted that sclerotic stroma can be seen in fibrosarcomas. 11 Feline fibrosarcomas often have mild to moderate peripheral lymphoplasmacytic inflammation, even in cases without vaccination. 11 In the current report, diagnosis of vaccine-associated fibrosarcoma was made based on clinical history and histological features although no vaccine adjuvant was apparent. There is also a brief mention of feline keloidal fibrosarcoma arising due to vaccination. 11 However, there is a paucity of veterinary literature that can differentiate keloidal fibrosarcoma from sclerotic fibrosarcoma. In human beings, sclerotic fibromas display distinctive collagen fibers with a storiform pattern.19,22 The hyalinized collagen in the present case did not exhibit storiform arrangement. Therefore, the keloidal variant of vaccine-induced fibrosarcoma was diagnosed.
Immunohistochemically, stromal cells of canine keloidal fibromas and fibrosarcomas are strongly positive for vimentin and negative for α-SMA indicating their fibroblast origin. 20 In contrast, the myofibroblasts are the predominant cell type in human keloids or hypertrophic scars. 15 In the present case, neoplastic spindle cells stained diffusely for vimentin, and approximately 50–60% of these cells stained positive for α-SMA suggesting a mixed cell population of fibroblasts and myofibroblasts. This finding was consistent with feline vaccine-induced fibrosarcomas, which demonstrated immunoreactivity for vimentin and α-SMA. 6 It was noted that the α-SMA–positive cells were either part of the tumor or formed a capsule around the neoplastic nodules. 6
A previous study described canine keloidal fibromas and fibrosarcomas containing approximately 10–40% of CD18-positive cells in the vicinity of hyalinized collagen, which were interpreted as macrophages. 20 The authors suggested that canine keloidal fibrosarcoma is a reactive inflammatory lesion rather than a true neoplasm. 20 In the present case, there were small numbers of CD18-positive cells on the periphery of the neoplasm. Therefore, it is difficult to conclude the role of macrophages in the pathophysiology of keloidal differentiation in felines on the basis of a single case, although malignant transformation of inflammatory lesions has been reported frequently in cats.8,16 Monitoring of more cases is required for the assessment of this finding.
The histomorphological features in the current case present a variant of vaccine-associated fibrosarcoma that resembled human and canine keloidal tumors. The neoplasm recurred 6 weeks post-excision suggesting an aggressive nature of keloidal variant of vaccine-associated fibrosarcoma in felines. In contrast, there was no evidence of recurrence or metastasis 6–9 months post-excision in canine keloidal tumors. 20 Monitoring of more cases is warranted to characterize the behavior of feline vaccine-associated fibrosarcoma with keloidal differentiation. In conclusion, the current report presents an interesting case of keloidal variant of vaccine-associated fibrosarcoma in a cat, which was likely triggered by administration of FeLV vaccine.
Footnotes
Acknowledgements
The authors would like to thank Dr. Sherwood Gill for providing the detailed clinical history of this case.
a.
EnVision+ System-HRP Labeled Polymer (DAB), Dako North America Inc., Carpinteria, CA.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.