
Abstract
The selective inhibition of platelet function in whole blood coagulation testing may allow insights into the nature of hypercoagulability in dogs with critical illness. To determine the effects of cytochalasin D and abciximab on hemostatic parameters in canine citrated whole blood, an in-vitro study was designed using thromboelastography (TEG) and a platelet function analyzer (PFA-100®). 8 clinically healthy mixed breed dogs donated blood that was anticoagulated with 3.2% sodium citrate in a 9:1 blood-to-citrate ratio. Addition of cytochalasin D to citrated whole blood from 6 dogs at concentrations ranging from 0 µg/ml to 10 µg/ml caused a maximal reduction of TEG maximum amplitude (MA) at a concentration of 7.5 µg/ml (52.7 ± 4.3 to 14.3 ± 7.8 mm). Addition of abciximab to canine citrated whole blood at concentrations of either 20 µg/ml or 40 µg/ml did not affect the TEG tracing; however, addition of abciximab to citrated canine whole blood at concentrations of 10 µg/ml and 20 µg/ml significantly prolonged PFA-100 closure times (72.5 ± 15 to 149.2 ± 91 sec and 275.6 ± 54 sec, respectively, P < 0.04). Inhibition of canine platelet function by cytochalasin D is demonstrated by TEG, but abciximab did not change TEG tracings. Abciximab does, however, inhibit platelet aggregation under shear stress as measured by the PFA-100. Inhibition of canine platelet function with cytochalasin D may allow further TEG studies in dogs with clinical disease.
Introduction
The in-vitro addition of platelet-inhibiting substances to common coagulation tests can aid in the diagnosis of hypercoagulable diseases. Specifically, the addition of platelet inhibitors to whole blood aggregation tests such as thromboelastography (TEG) and the PFA-100® platelet function analyzer system a can give information about the contribution of platelets to hypercoagulable states, and potentially allow clinicians to customize anti-thrombotic therapy. This approach has been investigated in human patients following major abdominal and cardiac surgery, 12,17 as well as in healthy rabbits. 14 Many diseases in dogs have been associated with hypercoagulability and formation of venous or arterial thrombi, 11 and although antiplatelet medications (such as aspirin or clopidogrel) or anticoagulant medications (e.g., heparin) are frequently recommended, there are no data to delineate whether factor-related hypercoagulability, platelet hyperactivity, or both contribute to the development of thrombi in a given patient. Knowledge of the primary component of hypercoagulability may allow more tailored thromboprophylactic treatments.
Thromboelastography refers to a whole blood viscoelastic coagulation monitoring protocol that depicts the combined activity of the cellular and plasmatic aspects of coagulation, in addition to fibrinolysis. 9 Thromboelastography has been used to demonstrate hypercoagulable tendencies in dogs with a variety of conditions. 7 Primary TEG measurements include the reaction time (R), the alpha angle (Ang), and the maximum amplitude (MA). Reaction time primarily evaluates the intrinsic pathway of coagulation, and thus represents interactions between coagulation factors VIII, IX, XI, and XII. 7 Alpha angle represents the rate of clot formation, and is influenced by concentrations of coagulation factors II and VIII and fibrinogen, in addition to platelet number and function. Maximum amplitude represents the maximum clot strength, and reflects contributions from soluble factors and fibrinogen, in addition to platelets. Mathematical transformation of the MA results in a value known as the G value, or the elastic shear modulus, which occasionally is reported in lieu of MA. 32
The PFA-100 system evaluates platelet aggregation under conditions of simulated shear, and has been evaluated and validated for use in dogs. 5,20 The PFA-100 system uses citrated whole blood aspirated at high shear rates through disposable plastic cartridges coated with collagen and adenosine diphosphate (ADP) as activators (a cartridge with collagen and epinephrine is also available, but is not frequently used in evaluation of dogs). 5 The end point of the assay is the time to occlusion of blood flow through the aperture of the membrane, expressed in seconds and reported as closure time (CT), or nonclosure if CT exceeds 300 sec. 5 In dogs, CT prolongations are seen with aspirin administration, von Willebrand disease, and thrombocytopenia. 5,20 The PFA-100 system is also sensitive for platelet function disturbances in dogs caused by exogenous substances such as hetastarch. 31
Cytochalasin D is a fungal metabolite that prevents microtubule assembly within the platelet and thus prevents cytoskeletal reorganization in response to platelet activation. 27 The platelet cytoskeleton is responsible for platelet shape change and secretion of platelet granule contents. 8 The platelet granules contain procoagulant and proaggregatory substances that promote platelet recruitment and contribute to secondary hemostasis at sites of tissue injury. 2 Because of the global effects on platelet activation, the expected effects of cytochalasin D on TEG tracings are a decrease in both MA and Ang. In-vitro studies that have used TEG or the related technology rotational thromboelastometry (ROTEG) to evaluate the effects of cytochalasin D on whole blood coagulation have been performed in human beings, rabbits, and pigs, and have confirmed these expectations. 14,22,30
Abciximab is a monoclonal Fab-fragment directed against the human platelet GPIIb/IIIa receptor. 29 The presence of abciximab prevents fibrinogen binding by the human GPIIb/IIIa receptor. As such, it is a potent inhibitor of platelet aggregation, and is used clinically in human patients undergoing coronary procedures such as stent placement. 26 The effects of abciximab on TEG tracings in human beings include a decreased Ang and decreased MA, presumably due to inhibition at the GPIIb/IIIa receptor. 14 Of note, results of a study in rabbits failed to demonstrate a change in the TEG tracing after ex vivo addition of abciximab. 22 Because abciximab is a monoclonal antibody directed against the human fibrinogen receptor, a significant receptor homology is necessary for the drug to have similar effects in other species, and the drug may not work as well in nonhuman species, including the dog.
The objectives of the current study were to investigate the effect of different in-vitro concentrations of cytochalasin D and abciximab on the TEG tracings of healthy dogs. The hypothesis was that the addition of cytochalasin D would result in a dose-dependent decrease in MA and Ang, while abciximab would not change TEG parameters due to receptor variations between species. A third objective was to investigate the effect of similar concentrations of in-vitro abciximab on the platelet function analyzer (PFA) CTs of healthy dogs. The hypothesis was that abciximab would not prolong closure times by use of collagen/ADP cartridges, again secondary to receptor differences amongst species.
Materials and methods
Cytochalasin D b was diluted with sterile 0.9% saline c from a stock solution (90 mg/ml) in dimethyl sulfoxide (DMSO) b to a concentration of 180 µg/ml and added to TEG reaction cups to achieve serial concentrations (see below). A control solution was made with diluted DMSO. The commercially available injectable abciximab d was diluted with sterile 0.9% saline c and added to the whole blood samples 5 min prior to analysis to final concentrations of 10, 20, and 40 µg/ml.
Thromboelastography analysis
Eight adult mixed-breed dogs deemed healthy by physical exam, complete blood cell counts, and coagulation profiles (prothrombin and activated partial thromboplastin times) were studied. Blood samples were obtained by jugular venipuncture by use of a 20-gauge needle and vacutainer adapter. Blood was collected by vacuum into 3-ml plastic tubes e containing 3.2% sodium citrate, for a final citrate-to-blood ratio of 1:9. These samples rested at room temperature (20–22°C) for 30 min prior to TEG analysis. The first tube obtained by this method was not analyzed, to limit the effect of venipuncture artifact on the tracings.
Thromboelastography analysis was performed on calibrated channels on 4 TEG analyzers. f Twenty µl of 0.2 M calcium chloride solution g was placed in a TEG cuvette warmed to 37°C for 1 min prior to addition of whole blood. For test runs, an additional 1–10 µl of cytochalasin D or 10 µl of dilute DMSO was added and mixed with the warmed calcium chloride solution by gentle aspiration with the pipette. Dilute cytochalasin D (180 µg/ml, as described above) was added to the reaction cup to result in final concentrations of 0.5, 1.0, 2.5, 5.0, 7.5, or 10 µg/ml. Dilute abciximab was added directly to the tubes of citrated whole blood to result in final concentrations of 10 and 20 µg/ml in 3 dogs, and 20 and 40 µg/ml in 6 dogs (1 dog had all 3 concentrations evaluated, in addition to a control sample). Abciximab was added 5 min prior to initiation of analysis, and the tube was inverted 5 times to distribute the drug. To all mixtures of drug and calcium chloride or calcium chloride alone, 340 µl of citrated whole blood was added to start the reaction, without the use of additional activators or mixing of the sample. Thromboelastography tracings were recorded on a computer with specialized software, h which also calculated and displayed all measured TEG parameters.
PFA-100 analysis
To evaluate the effect of abciximab on canine platelet function, blood was collected from 6 of the previously studied dogs using the same collection protocol. The citrated blood was divided into three 800-µl aliquots to which either nothing, 10 µg/ml of abciximab, or 20 µg/ml of abciximab were added. As with the samples for TEG analysis, abciximab was added 5 min prior to analysis. Cytochalasin D was not evaluated in this system based on pilot data that showed a general insensitivity to the different concentrations tested in the current study (i.e., results were frequently >300 sec).
Samples were run on the PFA-100 a using collagen/ADP cartridges, as previously described. 5 Eight hundred µl of citrated whole blood with or without abciximab at the tested concentrations was placed into the cartridge, and the machine was allowed to record the CT without any modification. If CT was greater than 300 sec, the machine only reported >300 sec as a CT; for statistical analysis, these samples were treated as if they were 300 sec. The CT was evaluated at 37°C for all samples. Any samples that generated flow errors were repeated within 10 min.
Statistical analysis
Thromboelastography data for measured parameters (R, Ang, MA) at each concentration of inhibitor were analyzed with a commercial statistical analysis program. i Parametric data were analyzed by use of a one-way analysis of variance, while nonparametric data were analyzed with a Kruskal–Wallis one-way analysis of variance on ranks. The same testing methodology was used to compare the TEG tracings that resulted from different concentrations of abciximab, as well as the PFA data from different abciximab concentrations. When significant differences were found, post-hoc testing by means of either the Holm–Sidak or Dunn method was conducted to identify significant comparisons. Significance was set at P < 0.05.
Results
Baseline TEG parameters and complete blood cell counts for all dogs were within the reference intervals for the authors’ institution. Mean platelet count was 296.7 ± 35 × 103/µl (reference interval: 242–407 × 103/µl). Mean hematocrit of all dogs was 46.9 ± 4.5% (reference interval: 36.6–59.6%). Cytochalasin D caused a significant decrease in MA in canine citrated whole blood at all concentrations (P < 0.02; Table 1). While a strong trend toward a decreasing angle was seen (P = 0.01), this change failed to maintain significance when corrections were made for multiple comparisons. There was no change in R-values at any dose of cytochalasin D (P = 0.438). There were no significant differences between the baseline TEG values and the DMSO control samples (Table 1). The addition of any concentration of abciximab to canine citrated whole blood did not significantly change TEG parameters compared to baseline (Table 2). Abciximab significantly prolonged the PFA CT at both 10 µg/ml and 20 µg/ml (P = 0.033 and P = 0.001, respectively; Table 3). Only 2 samples generated flow errors, and thus the tests for those samples were repeated.
Thromboelastography (TEG) values (median (range) or mean ± standard deviation) for 6 dogs after in-vitro exposure of citrated whole blood to varying concentrations of cytochalasin D.*
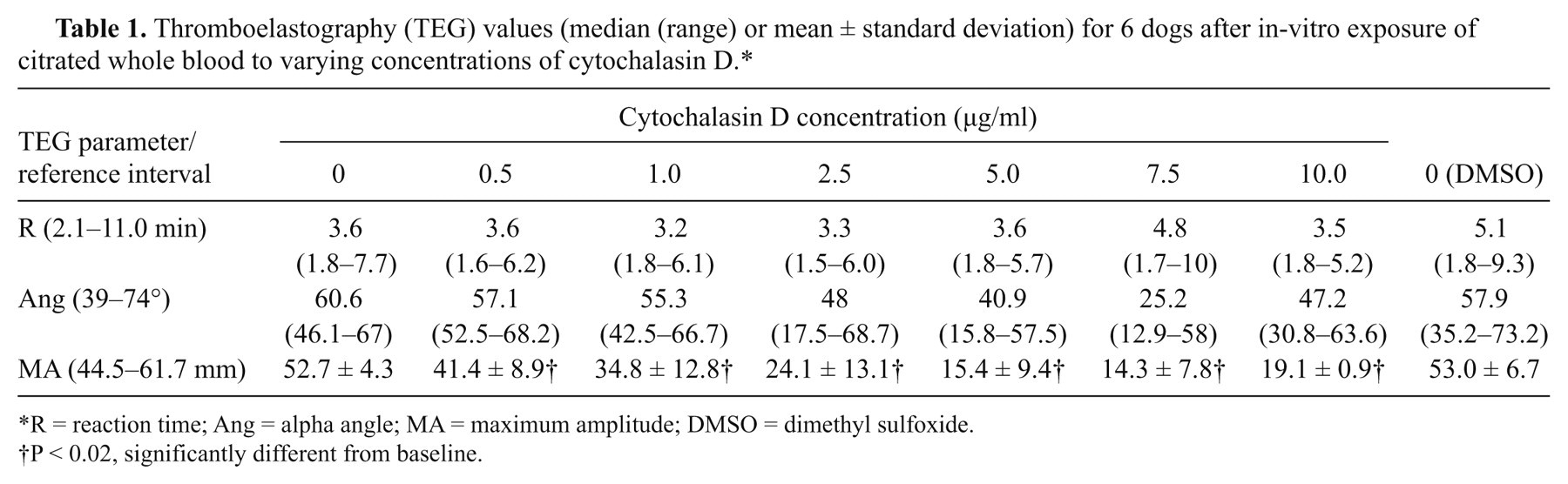
R = reaction time; Ang = alpha angle; MA = maximum amplitude; DMSO = dimethyl sulfoxide.
P < 0.02, significantly different from baseline.
Thromboelastography (TEG) values (mean ± standard deviation) for 6 dogs after in-vitro exposure of citrated whole blood to varying concentrations of abciximab.*
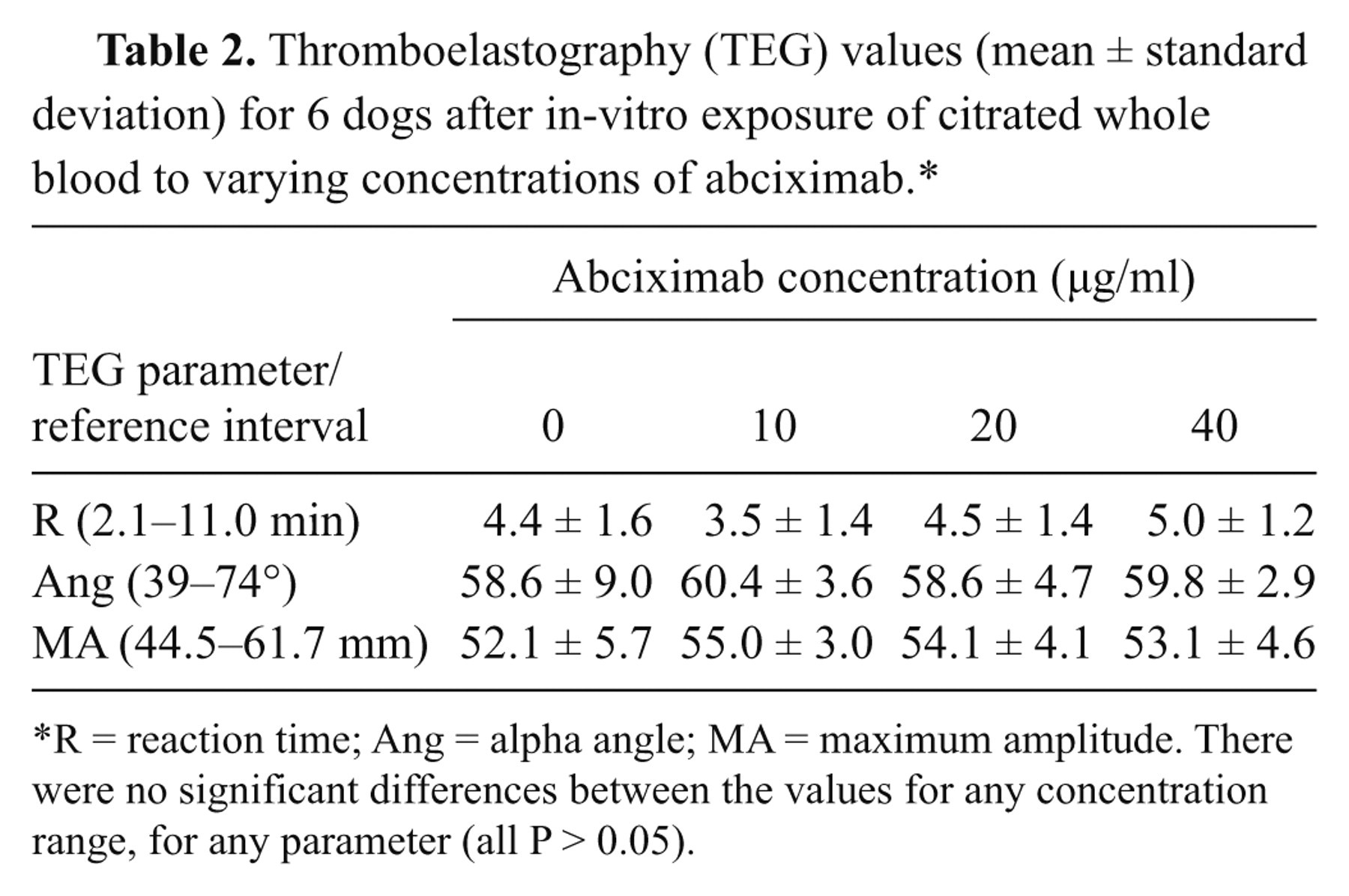
R = reaction time; Ang = alpha angle; MA = maximum amplitude. There were no significant differences between the values for any concentration range, for any parameter (all P > 0.05).
PFA-100® system closure times (mean ± standard deviation) using collagen–adenosine diphosphate cartridges in 6 dogs after in-vitro exposure of blood samples to varying concentrations of abciximab.
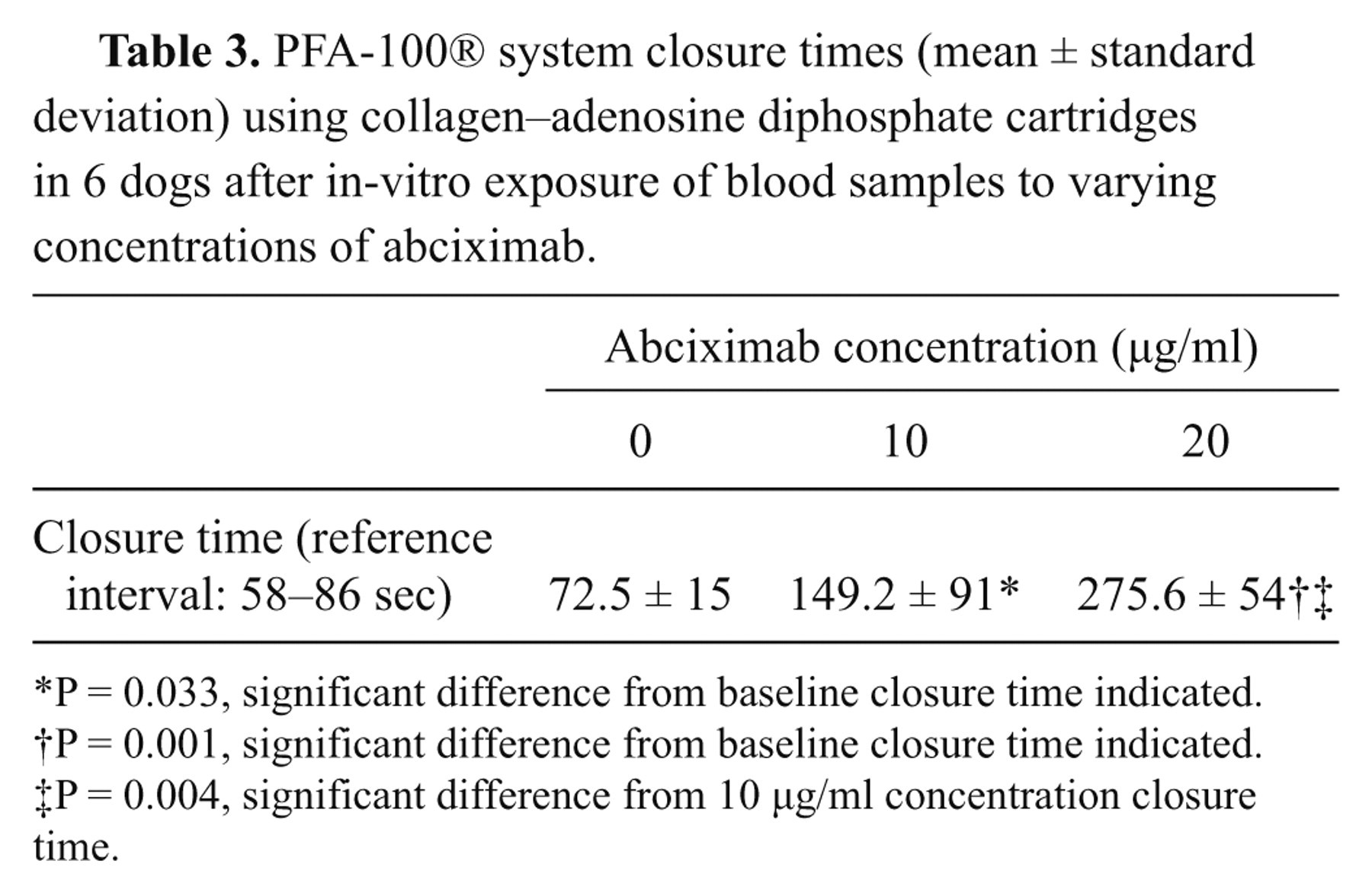
P = 0.033, significant difference from baseline closure time indicated.
P = 0.001, significant difference from baseline closure time indicated.
P = 0.004, significant difference from 10 µg/ml concentration closure time.
Discussion
Cytochalasin D added to canine citrated whole blood resulted in a significant decrease in MA at all concentrations, with a maximal decrease at 7.5 µg/ml. Cytochalasin D suppresses platelet shape change, phosphatidylserine externalization, granule release, and clot retraction as a result of effects on the platelet cytoskeleton. 27 These platelet functions are important to initiate and sustain coagulation in vivo, and are expected to contribute to in vitro whole blood coagulation as well. 2,21 The inhibition of platelet function in these samples likely contributed to the significant effects on the TEG tracing.
The addition of cytochalasin D to canine citrated whole blood did not change the R time from baseline values. This was expected, as the platelet contribution to coagulation is not evaluated by R, which is primarily dependent on contact activation in the recalcified sample (Ralph AG, Koenig A, Pittman JR, et al.: 2010, The effect of corn trypsin inhibitor on thrombelastography endpoints of citrated canine whole blood. J Vet Emerg Crit Care 20(Suppl s1):A6. Abstract). The effects of cytochalasin D on TEG parameters are consistent with prior reports in human patients. 6 While abciximab at a number of doses extrapolated from human studies did not alter the TEG tracing in dogs, the effect of these same (and lower) doses on the ability of platelets to aggregate in the PFA-100 assay was profound. The difference between these 2 assays most likely illustrates the difference between the role of the GPIIb/IIIa receptor in platelet function under conditions of high and low shear.
The expression of the GPIIb/IIIa receptor is the final common pathway for many different platelet agonists. Expression of this receptor allows the platelet to anchor fibrin or fibrinogen and to be integrated within a clot. The GPIIb/IIIa receptor is also critically important for binding small molecular weight von Willebrand factor (vWF) molecules that allow attachment of additional platelet aggregates to the basal layer of platelets that interacts directly with subendothelial collagen. 25 Without adequate GPIIb/IIIa function, platelets cannot bind together to form a strong clot under high shear conditions. By contrast, when there is low shear, such as in the TEG assay, the effects of abciximab are much less obvious, as the formation of a clot can proceed without a need for strong platelet binding to fibrinogen. Platelets, in the presence of GPIIb/IIIa inhibition, are still able to be activated, and the shape-change reaction, granule secretion, and membrane changes (i.e., exposure of phosphatidylserine) are able to occur and support the initiation and propagation of a clot. 26 Thromboelastography analysis can be performed with citrated plasma alone, if there is sufficient fibrinogen concentration and a strong coagulation activator. 33 This may explain the lack of effect of abciximab; initiation of clot formation was able to proceed as normal, and the plasma components were able to form a clot in this low shear environment, regardless of platelet binding of fibrinogen.
There is strong homology between the canine and human GPIIb/IIIa receptors, especially in the area of the fibrinogen-binding site on the IIIa portion, and abciximab is expected to bind to similar epitopes as on the human receptor. 24 The lack of full sequence homology may, however, result in altered binding of this drug, and incomplete inhibition of the binding of either fibrin or vWF. There is also evidence that abciximab has affinity for the human vitronectin receptor (alphavbeta3), which plays a role in cell adhesion, migration, and proliferation. 16 Additional studies are required to describe the kinetics of abciximab association with canine GPIIb/IIIa receptor and other cellular components.
The results of other studies in dogs support the importance of abciximab in attenuating platelet adherence under high shear conditions. With a maximum intravenous dose of 0.8 mg/kg, abciximab resulted in a dose-dependent inhibition of thrombosis of a nitinol stent placed in an ex-vivo arteriovenous shunt. 18 In a canine model of coronary artery thrombosis, the use of abciximab at intravenous doses of 0.6 mg/kg and 0.8 mg/kg slowed thrombosis of coronary arteries exposed to an electrical thrombotic stimulus. 28
The kinetics of abciximab in dogs may be different from those in human beings. Human platelets contain approximately 70–80% of GPIIb/IIIa receptors on their surface with the remaining 30% located within alpha-granules and the open canalicular system. 10 This internal pool is only expressed as a functional surface receptor upon platelet activation, and thus, the exposure of this pool of GPIIb/IIIa may counteract the effects of the initial abciximab dose. In addition, there is some evidence that 80% of the GPIIb/IIIa receptors on human platelets become bound with abciximab after 30 min 1 ; a longer incubation time (especially if the epitopes are slightly different between species) in the current study may have resulted in more profound effects on TEG analysis. The effects of the PFA analysis, however, would argue against this hypothesis.
Researchers pursuing a similar study 14 using in vitro addition of abciximab to human whole blood at similar concentrations did report a significant effect on automated ROTEG activated with Integ j (a proprietary contact activator for the intrinsic system containing ellagic acid and phospholipids), and specifically described a decrease in Ang and MA. An additional decrease in MA was seen with the addition of cytochalasin D to these mixtures. Similar results were also seen in a study in which investigators evaluated the effects of in vitro abciximab and cytochalasin D on tissue-factor–activated TEG. 13 A more recent study to evaluate the effect of in vitro addition of abciximab on kaolin-activated TEG in human blood failed to duplicate these results, 1 although the results of clinical studies using abciximab–TEG have shown a strong correlation of MA with fibrinogen concentration (compared to a weaker correlation between routine TEG MA and fibrinogen concentration in the same patient population). 12 The results of a study in rabbits also failed to show an effect of abciximab on TEG analysis, which was thought to be due to species differences in receptors, although further study was not pursued. 21 It is unclear why there was a difference between the species, and between the results of conspecific studies, but differences in incubation times, activators of coagulation, and other analytic and preanalytic variables may have contributed. The study 21 protocols also did not evaluate aggregation under high shear conditions. In the current study, a validated TEG protocol 23 failed to show effects of abciximab in canine citrated whole blood.
Thromboelastography may not be an appropriate or reliable modality for evaluation of platelet inhibitors such as abciximab in dogs. It is known that platelet antagonists such as aspirin and clopidogrel do not affect TEG tracings in dogs, 3,4 and that TEG tracings may be generated in the absence of any functional platelets, 33 which indicates that the use of a GPIIb/IIIa inhibitor may be an unreliable method to isolate the platelet contribution to the TEG tracing in dogs. One concern about using cytochalasin D rather than abciximab to evaluate the platelet component of a TEG tracing is that the aspects of platelet activation that support coagulation (e.g., exposure of phosphatidylserine) are maintained with abciximab, but are not present with the addition of cytochalasin D due to inhibition of microtubule assembly, although cytochalasin E has been reported to have no effect on platelet granule secretion. 15
Genetic polymorphisms in human beings result in variability of surface expressed P-selectin, GPIIb/IIIa–bound fibrinogen, and activated GPIIb/IIIa in response to low-dose ADP. 19 Human platelets with more surface bound ligands were found to have an enhanced response to abciximab. 18 Given the existence of this polymorphism in human beings, a similar scenario may exist in dogs, and may explain some of the variability seen in the current study population, although these were unrelated mixed-breed dogs. Further investigation is needed to characterize the surface expression of canine platelet surface ligands.
Hypercoagulable disease states are diagnosed with increasing frequency in veterinary medicine. 11 The diagnosis may be made with TEG, but a true diagnosis of hypercoagulability requires corroborating evidence such as fibrinogen concentrations, antithrombin levels, or gross evidence of thrombosis. 11 In veterinary medicine, platelet inhibitors and other anticoagulant medications are used based upon clinician preference, generally without knowledge of the underlying basis of the hypercoagulable state. Removal of the contribution of the platelet component of the TEG analysis may allow the clinician to extrapolate (based on comparison with an uninhibited tracing) the platelet contribution to hypercoagulability. With this information (and an appropriately generated reference interval for cytochalasin D–inhibited TEG), the clinician may be able to more accurately choose therapies for hypercoagulable patients (i.e., the choice between a platelet inhibitor such as clopidogrel and a coagulation inhibitor such as heparin).
Limitations of the current study include the small number of dogs tested, and the in-vitro nature of the drug application. If polymorphisms exist in canine platelet receptors, some of the results and conclusions in the present study may have been biased. The use of mixed-breed dogs was chosen to limit the possibility for breed-specific variability, but this is always a possibility. Although coagulation profiles were evaluated in the dogs, fibrinogen concentrations were not evaluated (although all dogs had previously tested within the reference interval). If alterations in plasma fibrinogen concentrations were present, actual effects of the tested drugs on TEG tracings may have been minimized. In the absence of advanced studies of the interaction of the abciximab antibody with the canine GPIIb/IIIa receptor (and other receptors), it is impossible to derive the exact site of action of this drug in the canine platelet. Cytochalasin D may be added for in-vitro inhibition of platelet function to allow TEG analysis of the relative contributions of coagulation factors and platelets to clot formation.
Footnotes
Acknowledgements
The authors acknowledge the assistance of Drs. Curtis Cathcart and Amy Dixon-Jimenez for PFA analyses.
a.
Siemens Healthcare Diagnostic, Deerfield, IL.
b.
Sigma Chemical, St. Louis, MO.
c.
Hospira Inc, North Chicago, IL.
d.
ReoPro, Eli Lilly, Indianapolis, IN.
e.
Vacutainer, BD, Franklin Lakes, NJ.
f.
TEG 5000, Haemoscope (now Haemonetics), Niles, IL.
g.
Haemoscope, Niles, IL.
h.
TEG Software v.4.3, Haemoscope, Niles, IL.
i.
Sigma Stat 3.5, Systat Inc., Chicago, IL.
j.
Integ-LS Activator, NOBIS, Endingen, Germany.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the UGA Critical Care research fund.