
Abstract
Necrotizing sialometaplasia (NS) is a self-limiting, benign, ischemic, inflammatory disease that is most often described in the submandibular glands of dogs, with clinical and histologic features that resemble malignancy. Unilateral swelling of the parotid salivary gland in a 7-year-old Cocker Spaniel dog was diagnosed as NS. The dog also had otitis externa on the same side as the parotid gland lesions. The main histologic features were included lobular necrosis of salivary tissue; fibrinoid necrosis of some arteries; marked squamous metaplasia of duct and/or acinar epithelium, with intercellular bridge formation; preservation of salivary lobular morphology; and variable inflammation and fibrosis. Etiologic factors for NS in both humans and animals remain obscure.
In humans, necrotizing sialometaplasia (NS) is a self-limiting, benign, ischemic, inflammatory, metaplastic disease of minor salivary glands that has clinical and histopathologic features often confused with malignancy. 1,4,7 The cause of NS is unknown, although some authors suggest that trauma or chemical injury to blood vessels may induce ischemia, followed by infarction of the gland and necrosis. 3,7,13 In dogs, NS is a rare disease but has been reported to account for 6% (9/160) of canine salivary gland diseases. 4,13 Canine NS usually affects submandibular salivary glands, and its occurrence in parotid salivary glands has not been previously re-ported. 4,6,8,9,11,13 In the present report, the pathological and immunohistochemical features of a case of NS affecting the parotid salivary gland in a Cocker Spaniel dog are described.
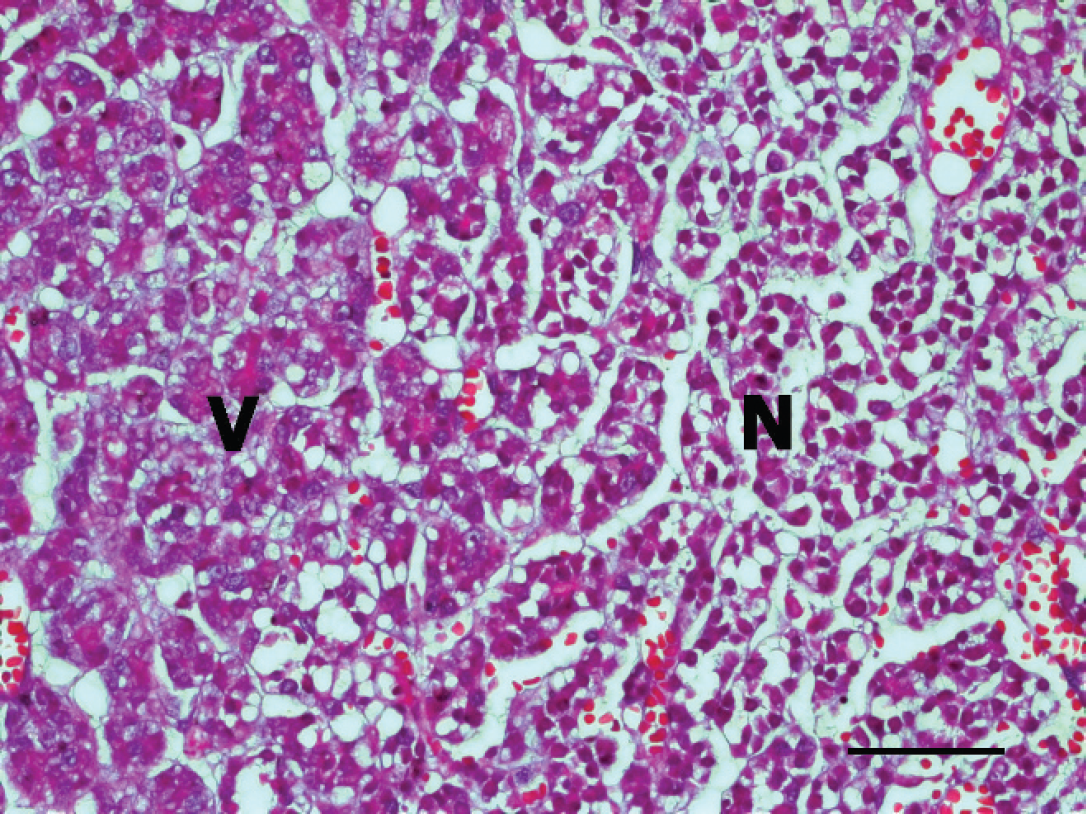
Parotid gland, dog. Note the extensive coagulative necrosis (N) and viable salivary gland (V). Hematoxylin and eosin. Bar = 50 μm.
A 7-year-old, male, neutered Cocker Spaniel was presented at the local animal hospital with a painful mass around the auditory canal. On physical examination, an ulcerated mass was present under the right ear. The mass had developed over the previous year, while the dog was under treatment for otitis externa of the right ear. Blood chemistry values were within reference ranges, and no lesion was seen upon radiography of the neck. The mass was surgically removed, and a part of the mass was submitted to the Animal Disease Diagnostic Center, National Veterinary Research and Quarantine Service (Anyang, Gyeonggi-do, Republic of Korea), for histopathological examination. Grossly, the surface of the 12 cm × 6 cm mass was brown to gray, red in some areas of its cut surface, and moderately firm. Sections of the tissue were fixed in 10% neutral buffered formalin, processed routinely, and embedded in paraffin. Four-μm thick tissue sections were cut and stained with hematoxylin and eosin. Additional tissue sections were immunolabeled with anticytokeratin antibody a using high-molecular-weight cytokeratin (CK-HMW) clone 34βE12. Immunohistochemical staining was performed using a streptavidin-biotin amplification system and an automated platform. b The tissue sections were incubated for 8 min with protease 1, b then incubated with primary antibodies for 30 min, followed by the incubation with LSAB2 biotinylated link for streptavidin (K1015) a for 10 min. Next, diaminobenzidine b was applied for 5 min as the chromogen. All sections were counterstained with hematoxylin and bluing reagent. b Canine skin sections were used as the positive control. For the negative control, phosphate buffered saline was applied in place of the primary antibody.
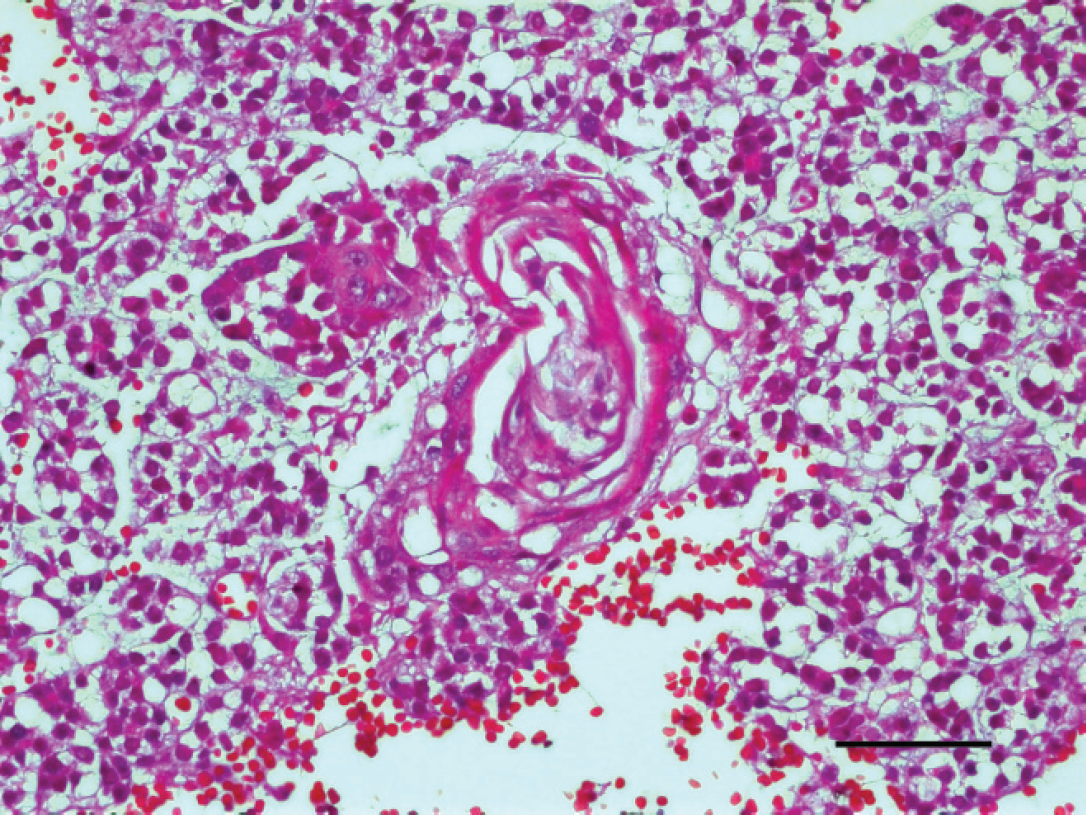
Parotid gland, dog. Note the metaplastic glandular epithelial cells with intercellular bridge formation. Hematoxylin and eosin. Bar = 50 μm.
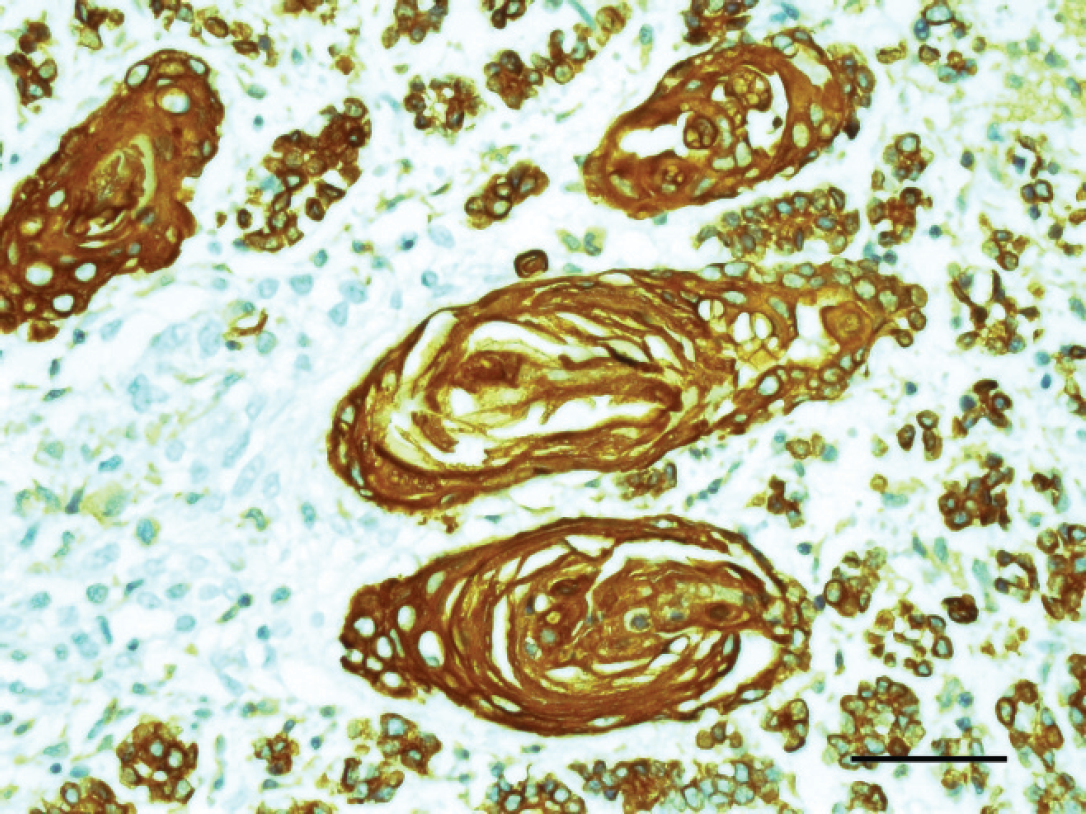
Parotid gland, dog. Note the metaplastic squamous epithelial cells showing strong cytoplasmic immunoreactivity for high-molecular-weight cytokeratin (clone 34βE12). Streptavidin-biotin-diaminobenzidine, counterstained with hematoxylin. Bar = 50 μm.
Areas of normal parotid salivary gland tissue in the tissue section confirmed the anatomical site of the mass (Fig. 1). Microscopically, the mass was unencapsulated, and extensive lobular coagulative necrosis was observed (Fig. 1). The necrotic acinar cells were pyknotic, and some cells displayed cytoplasmic vacuolation (Fig. 1). Scattered blood vessels within the necrotic areas of the gland had fibrinoid necrosis within the tunica media and luminal thrombosis; however, vasculitis was not seen. In areas peripheral to the necrosis, severe fibrosis, neovascularization, abundant mucin, hemorrhage, and congestion were observed. Multifocal areas of marked squamous metaplasia of the glandular and/or ductular epithelium were observed. Intercellular bridge formation and/or keratin pearls were seen in the necrotic areas and occasionally in viable tissues (Fig. 2). However, no pleomorphism of nuclei was detected in the metaplastic squamous epithelium. Immunohistochemically, CK-HMW had strong cytoplasmic immunoreactivity in the normal glandular epithelium and metaplastic squamous epithelium (Fig. 3). There was recurrence of the disease 4 months after the initial surgery, at which time the mass was again excised. The clinical signs of NS, including extreme pain, anorexia, gagging, and vomiting, have been described in dogs, 4,6,8,9 but in the current case, there were no signs other than severe pain.
It is assumed that because the parotid salivary gland was involved, the mass did not put pressure on the larynx and esophagus to cause the anorexia, gagging, and vomiting that has been described in NS of the mandibular salivary gland. In one retrospective report, 12 most dogs with salivary necrosis had underlying esophageal problems, and when the esophageal disease was successfully treated, the salivary gland lesions resolved. This led to the suggestion that the esophageal lesions and afferent vagal reflex were possible causes of NS in dogs. 12 Type III hypersensitivity has been suggested as a cause of NS in dogs, where blood vessels in the salivary gland react with immunoglobulin G and complement. 9 Moreover, Bartonella spp. infection has been reported as a potential cause of NS in the dog, with systemic granulomatous disease in parenchymal tissues as well as in the submandibular gland. 11 The etiology of NS in the dog has not, however, been elucidated. Moreover, in the current case, the cause of disease also was unclear. Clinical data from more cases of NS should be evaluated to help elucidate its cause.
In human beings, a few cases of NS of the parotid gland have been reported. 3,10 In dogs, no such cases have been reported previously, despite the parotid gland's superficial and vulnerable location. 13 The reason for this discrepancy is not clear.
Although relapses are usually infrequent, a single case with recurrent lesions in a human being has been published. 2 In dogs, no recurrence has been reported in NS of the submandibular gland. 13 However, in the present study, there was recurrence in the parotid salivary gland after 4 months, requiring surgical removal. The recurrence might be due to incomplete excision of the initial mass. Although NS in human patients and dogs has a benign behavior, squamous metaplasia may lead to misdiagnosis as carcinoma and to inappropriate treatments, such as radical surgery and chemotherapy 4,7 ; therefore, correct diagnosis is important for disease management.
The histopathology of the lesion in the present study, including extensive necrosis of the parotid gland, chronic inflammation, and sialometaplasia, was identical to that observed in the submandibular gland of dogs, cats, and human beings. 1,3,6,8,11,13 The vasculopathy including vascular thrombosis and/or fibrinoid degeneration was observed in many, 3,4,6,10,13 but not all, 1,11 cases of NS of dogs and human beings. However, vasculopathy was not found in cats. 5
Squamous cell carcinoma and mucoepidermoid carcinoma should be considered in the differential diagnosis. 1 In the current case, it was not difficult to differentiate NS from neoplastic disease because of the absence of atypical nuclei in the metaplastic squamous epithelium, the presence of prominent fibrous tissue, and the maintenance of the general lobular structure of the parotid gland. 1 In immunohistochemical staining, the epithelial cytoplasm of the metaplastic salivary gland reacted strongly with antibody to cytokeratin and therefore was confirmed to be of epithelial origin. In conclusion, based on its characteristic histopathology, the present case was diagnosed as NS.
Acknowledgements. The authors thank Mr. Jung-Won Park for preparation of the histopathological examination. This study was supported by a grant from the National Veterinary Research and Quarantine Service, Ministry of Food, Agriculture, Forestry and Fisheries, Anyang, Republic of Korea.
Footnotes
a.
Dako Denmark A/S, Glostrup, Denmark.
b.
Discovery® XT, DAB Map kit, Ventana Medical Systems Inc., Tucson, AZ.