
Abstract
A 15-year-old female Domestic Medium Hair cat presented to the referring veterinarian with a 2-month history of multiple, raised, disseminated, nodular skin lesions. A biopsy of 1 of the lesions was submitted to the Oklahoma Animal Disease Diagnostic Laboratory for evaluation. Histologically, there were multiple dermal nodules composed of sheets of neoplastic round cells. Multifocally, the neoplastic cells formed multiple small clusters of 3–5 cells within the epidermis. Distinct cytoplasmic granules were evident within the neoplastic cells with toluidine blue and Giemsa stains. The neoplastic cells were immunoreactive for c-KIT and lacked immunoreactivity for cluster of differentiation 3 with immunohistochemistry. Based on these findings, multiple epitheliotropic cutaneous mast cell tumors were diagnosed. The cat's health declined rapidly despite aggressive treatment, and the animal was humanely euthanatized. A complete necropsy revealed sheets of similar neoplastic mast cells within the spleen, liver, and individual cells scattered within the bone marrow. Exon 11 of the c-KIT messenger RNA from 1 of the cutaneous masses and the spleen was amplified with reverse transcription polymerase chain reaction, sequenced, and compared with the published c-KIT messenger RNA sequence from fetal cat tissues. The maximum identity was 100% for both tissue samples. To the authors’ knowledge, the present report is the first to describe disseminated cutaneous mast cell tumors with epitheliotropism and systemic mastocytosis in a domestic cat.
Cutaneous mast cell tumors (MCTs), or mastocytomas, are relatively common dermal or subcutaneous neoplasms that are most commonly found on the head and trunk in cats older than 4 years. 4,11,12,15,17,19,21,22,29 The grading scheme outlined for canine MCTs described previously does not appear to be prognostically significant in cats. 10,16,22,23 Instead, MCTs in cats are commonly divided into 2 groups that have prognostic significance: well differentiated and poorly differentiated. 15,16 Poorly differentiated MCTs are characterized by marked anisocytosis, uninucleated or multinucleated neoplastic giant cells, and a high mitotic rate. 16,17 Although most feline cutaneous MCTs are typically benign, local recurrence and visceral metastasis have been reported in less than 20% of cases with the poorly differentiated form. 8,15,16,20–22 Complete excision of well-differentiated MCTs is typically curative. 6,19,22,26
An uncommon histiocytic variant is seen in Siamese cats. 7,12,21 In this form, the neoplastic cells are typically large with indistinct cytoplasmic granules and a slightly indented nucleus. This lesion can be confused with inflammation histologically. This variant is also typically benign and has been reported to eventually regress. 7,25
Visceral involvement of cutaneous MCTs is rare. 24 Visceral MCT in cats, commonly referred to as systemic mastocytosis, has been reported and is considered a separate disease from cutaneous MCTs. 3,18 There are 2 types of visceral MCTs: the splenic form and the intestinal form. 24 In cats, metastasis of the splenic form of systemic mastocytosis has been reported in the liver, lymph nodes, bone marrow, lung, and intestines. 24 With the intestinal form, metastasis has been reported in the liver, lymph nodes, bone marrow, and lungs. 24 Although only a paucity of cats with systemic mastocytosis exist in the veterinary literature, reported survival ranges from 2 to 38 months. 18,28
Epitheliotropic neoplasms in cats are limited to cutaneous epitheliotropic lymphoma and progressive feline histiocytosis. 1,11 Other intraepidermal neoplasms include carcinomas of basal cell or squamous cell origin, adenocarcinomas, and melanomas. 11,13 In the current case report, disseminated cutaneous MCTs with epitheliotropism and systemic mastocytosis in a cat are described.
A 15-year-old female Domestic Medium Hair cat presented to the referring veterinarian with a 2-month history of disseminated nodular skin lesions. The skin lesions were raised, red, hairless, slightly firm, and 1 mm to 2 cm in diameter (Fig. 1). Pruritis was not observed, and the lesions did not appear to be painful. The regional lymph nodes and the abdomen were within normal limits on palpation. A scraping was taken for fungal cultures. At that time, the cat was administered 10 mg of enrofloxacin subcutaneously and placed on 50 mg of amoxicillin drops twice daily. The fungal culture yielded only contaminant fungi after 2 months.
Two months later, the cat had not responded to treatment and the skin lesions had increased in size and were dark red. One of the raised lesions was biopsied and placed in 10% neutral buffered formalin. The sample was submitted to the Oklahoma Animal Disease Diagnostic Laboratory (Stillwater, OK) for histologic evaluation. The cat was placed on 5 mg of prednisone twice daily.
The biopsy sample was sectioned and paraffin embedded, and the 4–5-μm sections were prepared and stained with hematoxylin and eosin. Sections were also routinely stained with toluidine blue, Giemsa, and Gomori methenamine silver. Immunohistochemistry for c-KIT and cluster of differentiation 3 using a horseradish peroxidase-streptavidin method were performed on sections according to the manufacturer's guidelines. A canine MCT and a canine lymph node were used as positive controls for c-KIT and cluster of differentiation (CD) 3 immunohistochemistry, respectively.
Histologically, multiple highly cellular, variably sized, moderately well-demarcated dermal nodules were composed of densely packed sheets of neoplastic round cells admixed with small numbers of eosinophils. Multifocally, the neoplastic cells formed small clusters of 3–5 cells within the overlying epidermis, follicular epithelium, and adnexal glands (Figs. 2, 3). The neoplastic cells had a moderate amount of amphophilic cytoplasm with indistinct cytoplasmic granules and poorly defined cell borders. The nuclei were round with reticular chromatin and occasionally contained a single prominent nucleolus. There was moderate anisocytosis and anisokaryosis. There were 4 mitotic figures in 10 random 400x fields. Admixed with the neoplastic cells were multiple small clusters of lymphocytes and plasma cells.
Distinct, fine, metachromatic cytoplasmic granules were visualized within the neoplastic cells with both toluidine blue and Giemsa stains (Fig. 4). Cytoplasmic immuno-reactivity for c-KIT was detected within the neoplastic cells and was characterized by punctate staining evenly distributed throughout the cytoplasm (Fig. 5). The neoplastic cells lacked immunoreactivity to CD3 (Fig. 6). Fungal organisms were not detected within the sections with the Gomori methenamine silver stain. Histologic findings were consistent with disseminated cutaneous epitheliotropic MCTs.
The prednisone treatment was continued for another month with no response. The cat had stopped eating and was listless. The cat was placed on 20 mg itraconazole once a day, 25 mg enrofloxacin twice a day, and 5 mg diphenhydramine twice a day in addition to the prednisone previously prescribed. A week later, the cat began eating and drinking. However, the cat was in poor body condition with an unkempt coat and would frequently vomit. The prednisone and diphenhydramine were continued, and famotidine was administered at 5 mg once a day. One month later, the cat developed conjunctivitis, went into respiratory distress, and was humanely euthanatized. The cat was submitted to the Oklahoma Animal Disease Diagnostic Laboratory for complete necropsy examination.
On gross examination, the cat weighed 2.4 kg and had moderate muscle atrophy, although adequate body fat was present. Scattered along all haired skin surfaces were hundreds of pinpoint to 2 cm in diameter, flat to raised, red to tan, soft masses with adherent crusts. The liver was diffusely mottled yellow, tan, and red with vague, pale, circular, flat areas that extended into the parenchyma on section. Along the left lateral liver lobe, there was a 1-cm-in-diameter, green to yellow, raised, fluctuant, multi-lobulated, loculated mass composed of small cystic structures filled with clear fluid, which was interpreted as a biliary cystadenoma. Approximately 1 cm of the mid-duodenum was tightly adhered to the visceral surface of the caudate lobe and the left medial liver lobe with dense fibrous tissue. Approximately 2 cm of duodenum surrounding this area was markedly thickened. The mucosal surface of this area was also thickened with extensive ulceration. The spleen was mildly enlarged and meaty in texture.
Representative sections were immersion fixed in 10% formalin and routinely processed. On histologic examination, the dermal nodules noted on necropsy examination resembled those described in the biopsy sample, although the cytoplasmic granules were much less distinct. Neoplastic mast cells with distinct cytoplasmic granules were present within the spleen, liver, bone marrow, and lung. Within the spleen, the neoplastic cells formed dense sheets that effaced the red pulp (Fig. 7). The neoplastic cells within the liver formed rows and clusters within the hepatic sinusoids that occasionally obscured the adjacent hepatocellular architecture (Fig. 8). There was no evidence of emperipolesis or infiltration of the bile ducts with neoplastic cells. The bone marrow was markedly hypercellular. With a Giemsa stain, individually scattered mast cells were evident as a background population to the erythroid
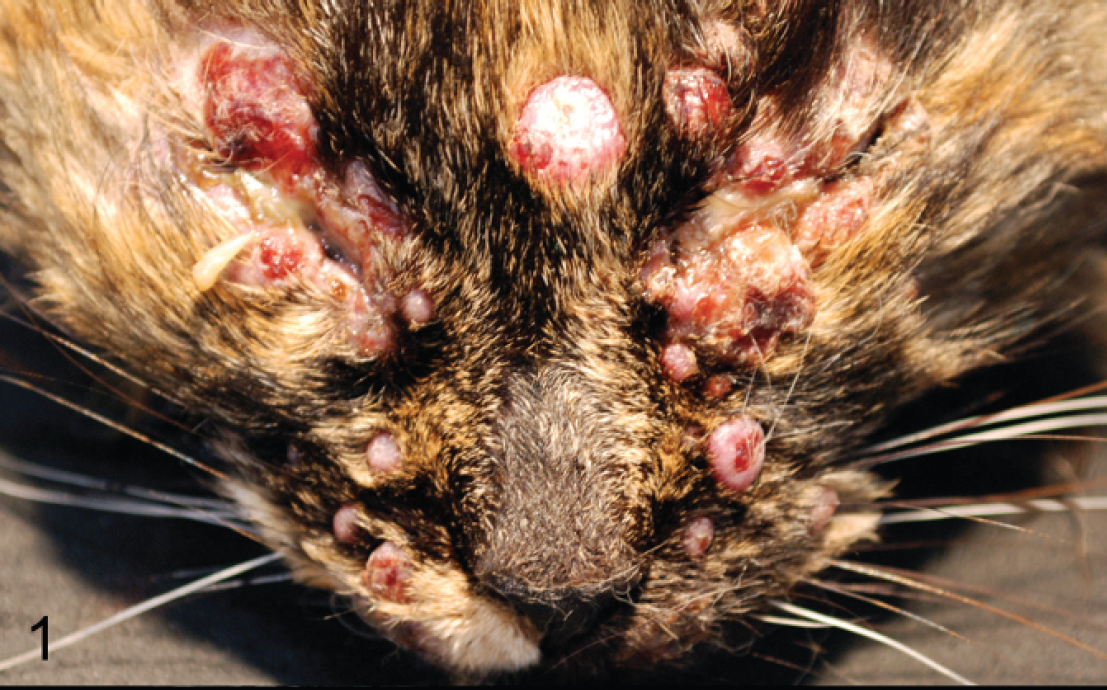
There are multiple disseminated, coalescing, hairless nodules.

Neoplastic mast cells form dense sheets within the dermis (asterisk) and small clusters within the epidermis (arrows). Hematoxylin and eosin stain. Bar = 200 μm.

Neoplastic mast cells individually infiltrate the epithelium of an apocrine gland (arrows). Hematoxylin and eosin stain. Bar = 100 μm.

Neoplastic mast cells with metachromatic cytoplasmic granules expand the dermis (asterisk) and form small clusters within the epidermis (arrows). Toluidine blue stain. Bar = 100 μm.

Cytoplasmic immunoreactivity for c-KIT is evident within neoplastic cells within the dermis (asterisk) and within the epidermis (arrows). Streptavidin-horseradish peroxidase for c-KIT counterstained with Mayer hematoxylin. Bar = 100 μm.

The neoplastic cells are not immunoreactive for cluster of differentiation (CD)3 (arrows). A few scattered non-neoplastic lymphocytes in the dermis are immunoreactive (arrowhead). Streptavidin-horseradish peroxidase for CD3 counterstained with Mayer hematoxylin. Bar = 100 μm.
and myeloid precursors in the bone marrow (Fig. 9). The lung and pancreas had individually scattered mast cells within the lumens of large and medium caliber arteries, respectively. The sections of duodenum revealed extensive ulceration with no evidence of mast cell infiltration or epitheliotropism. Necropsy findings support the diagnosis of disseminated cutaneous MCTs with epitheliotropism and systemic mastocytosis.
A section of fresh frozen skin and spleen were saved for reverse transcription polymerase chain reaction (RT-PCR).
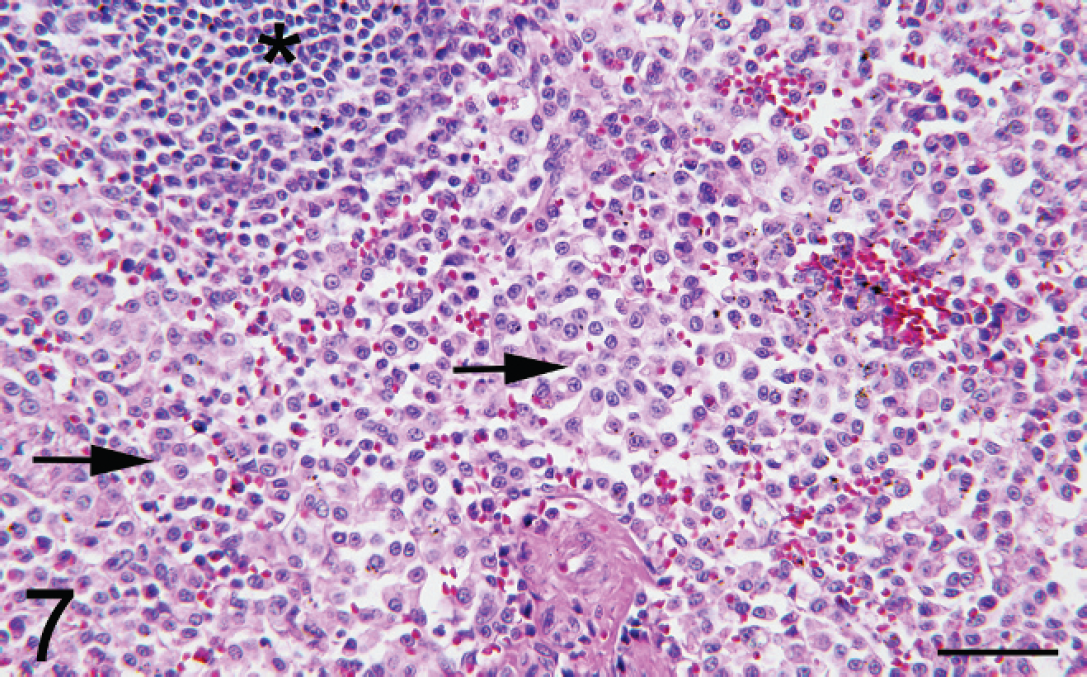
Neoplastic mast cells form dense sheets within the splenic red pulp (arrows). The white pulp is marked with an asterisk. Hematoxylin and eosin stain. Bar = 100 μm.
The samples were processed for messenger RNA extraction using a commercial purification kit. a The RT-PCR was then performed on the sample for mRNA of c-KIT specifically targeting exon 11 using a 1-step RT-PCR kit. a Primers used for exon 11 were the same as previously described for feline MCT. 9 The conditions of the RT-PCR technique were 50°C for 30 min, 95°C for 15 min, 94°C for 1 min, 48.3°C for 1 min, and 72°C for 1 min (40 cycles) with a final extension at 72°C for 10 min. The annealing temperature was optimized using a gradient of temperatures. The resulting products were analyzed using gel electrophoresis with a 2% agarose gel. The resulting band of the expected product size (127 bp) was purified and sent for sequencing. The sequence from both the skin and spleen had 100% homology (maximum identity) to the published feline messenger RNA c-KIT sequence.
Differential diagnoses for cutaneous epitheliotropic round cell neoplasms in cats include epitheliotropic lymphoma and progressive feline histiocytosis. 1,10 In the current case, the neoplastic cells lacked immunoreactivity to CD3, ruling out an epitheliotropic lymphoma. Furthermore, the neoplastic cells had distinct metachromatic cytoplasmic granules with special stains and were immunoreactive
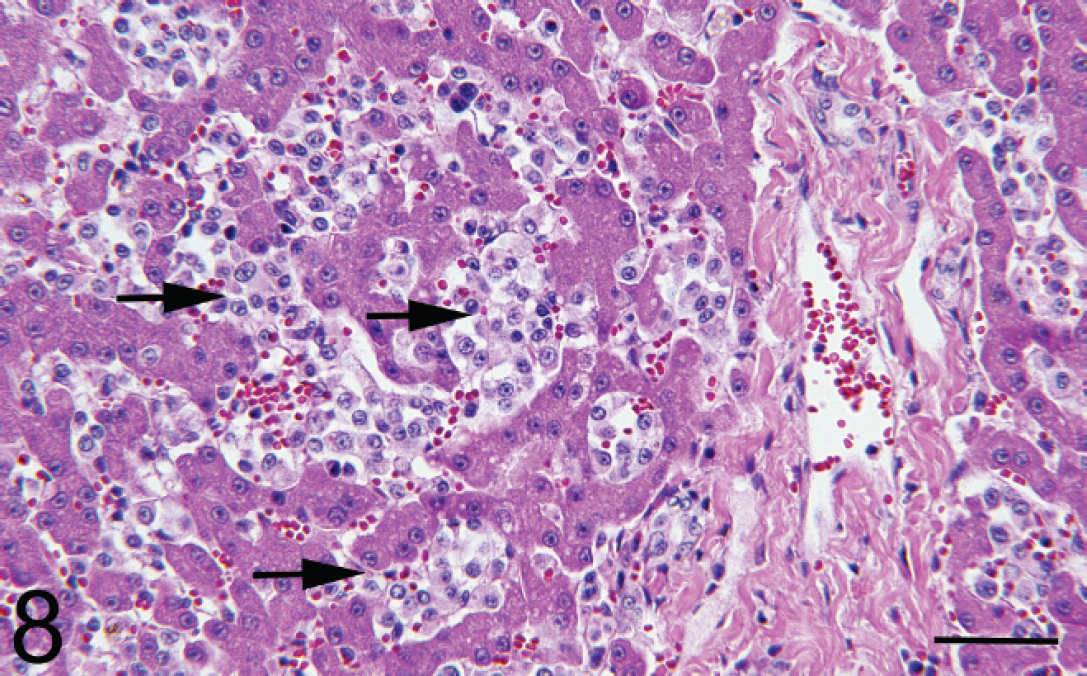
Neoplastic mast cells expand the hepatic sinusoids (arrows). Hematoxylin and eosin stain. Bar = 100 μm.
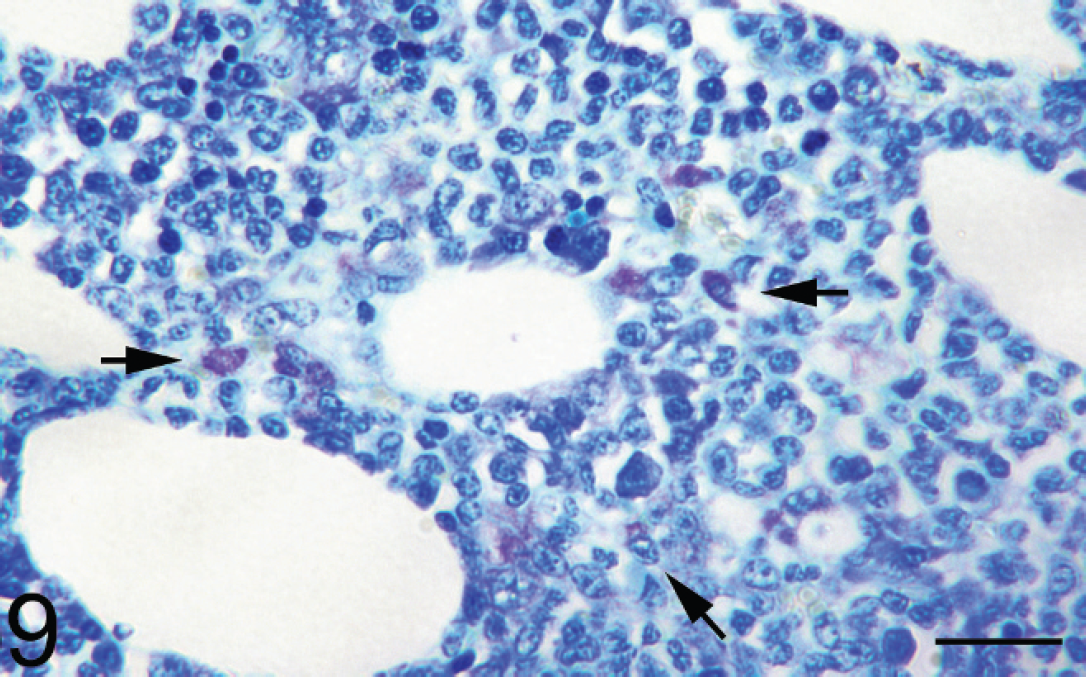
Neoplastic mast cells with metachromatic cytoplasmic granules infiltrate the bone marrow (arrows). Giemsa stain. Bar = 75 μm.
for c-KIT, confirming mast cell origin. Both epitheliotropic lymphoma and progressive feline histiocytosis are associated with a poor prognosis. Epitheliotropic lymphoma and progressive feline histiocytosis are slowly progressive, indolent neoplasms with metastasis late in the course of disease despite aggressive chemotherapeutic and immunomodulatory treatments. 1,10 Because epitheliotropic MCTs have not been described, there is no information on prognosis within the veterinary literature. The cat described in the present report survived 6 months from initial examination by the referring veterinarian before being humanely euthanatized. During that time, the cat progressed from having small isolated skin lesions to disseminated disease with visceral involvement.
Well-differentiated cutaneous MCTs in cats are typically benign, and complete excision is usually curative. 6,7,24,29 In the current case, there was moderate anisocytosis, the mitotic rate was low, and uninucleated or multinucleated neoplastic giant cells were not observed, which is most consistent with the well-differentiated form of MCTs in cats. However, cats with a single cutaneous MCT were shown to have longer survival times compared with those with multiple (5 or more) cutaneous MCTs. 19,25 The presence of multiple neoplasms in the present case favored a guarded prognosis.
Another dermatologic entity, known as urticaria pigmentosa, is characterized by dermal perivascular to interstitial infiltrates of mast cells. Urticaria pigmentosa has been reported in Sphinx, Himalayan, and Devon Rex cats. 27 Grossly, urticaria pigmentosa is characterized by small multifocal, red, slightly raised areas. The gross appearance of urticaria pigmentosa is strikingly different compared with the large, exophytic dermal nodules reported in the present case. Histologically, the mast cells in cases of urticaria pigmentosa do not form discrete dermal nodules and instead form an inflammatory perivascular to interstitial pattern within the skin. Again, this is very different from the neoplasms described in the present case.
The nomenclature used for MCTs in cats is highly variable and includes mast cell leukemia, systemic mastocytosis, disseminated cutaneous MCTs/mastocytosis, and mastocytoma. Mast cell leukemia is used to describe a neoplasm of mast cell origin characterized by mastocytemia and is used interchangeably with systemic mastocytosis in some of the veterinary literature. 3,14,18,28 Systemic mastocytosis is used to describe neoplastic mast cells that infiltrate multiple visceral organs, particularly the spleen. 2,18 Bone marrow involvement is common with systemic mastocytosis, and a variable mastocytemia can be seen. 3,18,28 Disseminated cutaneous MCTs and diffuse cutaneous mastocytosis are used interchangeably and refer to multiple, cutaneous MCTs. 5,8 A mastocytoma is reserved to describe a single benign cutaneous MCT. 15 In the current case, the distribution of the lesions had features of both disseminated cutaneous MCTs and systemic mastocytosis, with cutaneous epitheliotropism being a unique feature.
It is extremely rare for cats with disseminated cutaneous MCTs to have involvement of other organ systems. 5,8 In previous reports, visceral metastasis was limited to the pancreas and lymph nodes. 5,8 Similarly, cats with systemic mastocytosis have not been reported to have cutaneous involvement. In the current case, the cat had multiple dermal MCTs with extensive visceral involvement. It is impossible to determine whether the neoplasm originated from the skin or visceral organs in the current case. The cat originally presented with a few dermal nodules and was otherwise clinically healthy. Clinical signs of anorexia and vomiting developed later in the course of disease. This suggests that visceral involvement likely followed the development of the cutaneous neoplasms. The pattern of visceral involvement appears to be vascular oriented, suggesting spread from a solid tumor, such as within the skin, to other organs. Because blood work was not performed, a mastocytemia could not be documented.
The gross appearance of the skin lesions in the present case resembles that in a previous report of disseminated cutaneous MCTs in a cat. 8 In that report, the neoplastic cells were poorly differentiated and the dermal mast cells lacked cytoplasmic granules, which is in stark contrast to the case presented here, in which metachromatic granules were well demonstrated with special stains in the original skin biopsy. In the previous report, the cat was euthanized due to anorexia, lethargy, and poor prognosis. On necropsy of that cat, neoplastic mast cells were noted within the peripheral lymph nodes and within the pancreas. Epitheliotropism was not reported in the previous case.
Another case of disseminated cutaneous mastocytosis has been reported in a cat with small miliary lesions along the skin. 5 The cat was euthanized due to unresponsive and intense pruritis. On histologic examination of tissues from that cat, neoplastic mast cells had distinct cytoplasmic granules and multinucleated cells were common. Mast cell infiltration was limited to the dermis and the peripheral lymph nodes. Involvement of other organs and epitheliotropism were not documented.
To the authors’ knowledge, this is the first report to document disseminated cutaneous MCTs with epitheliotropism and systemic mastocytosis in a domestic cat. Mast cell tumors have not been previously reported to exhibit epitheliotropism in any species. The cause for the neoplastic mast cell epitheliotropism in the present case is not known. It is possible that regional cytokine release results in mast cell infiltration of the overlying epidermis.
Based on the findings in this case, a MCT should be considered on the list of differential diagnoses for cutaneous epitheliotropic round-cell neoplasms in cats. Although the present report only discusses a single case, the prognosis should be guarded in cats with disseminated epitheliotropic cutaneous MCTs, given the lack of response to clinical treatment and disease progression in this case. Cats with disseminated cutaneous MCTs should be evaluated for involvement of other organ systems.
Acknowledgements. The authors thank Brian Olson and the histology staff at the Oklahoma Animal Disease Diagnostic Laboratory for their technical assistance.
Footnotes
a.
Qiagen Inc., Valencia, CA.