
Abstract
A viral-induced digital cutaneous exophytic papilloma was diagnosed in a 2-year-old, spayed, female Siberian Husky dog with lameness. Digital pain and lameness persisted after removal of the initial papilloma, and the fifth lateral digit was subsequently amputated. Upon histologic examination of the digit, a de novo digital, cutaneous, inverted, viral papilloma and subungual cyst were diagnosed. The inverted cutaneous papilloma, located at the junction of the digital paw pad and ventral nail, extended focally through the nail into the subungual space, where an expansile cyst was formed. Cellular changes suggestive of papillomavirus infection were present in the epithelium of the original exophytic papilloma, as well as the endophytic mass and subungual cyst. Cytopathic effects included ballooning degeneration of keratinocytes, koilocytosis, irregularity of keratohyalin granules, and margination of nuclear chromatin. Numerous faintly basophilic to eosinophilic intranuclear inclusions measuring 10–15 μm in diameter were present within keratinocytes of the exophytic, endophytic, and subungual cystic lesions. Electron microscopy was performed on tissues from all lesions and revealed numerous 40–45 nm diameter hexagonal virions characteristic of papillomavirus that were arranged in crystalline arrays and dense clusters within affected nuclei.
A 2-year-old, spayed, female Siberian Husky dog presented for lameness of 2 weeks' duration. On physical examination, the only abnormality was a small exophytic mass that was present on the lateral aspect of the distal fifth digit of the right front foot. The mass was surgically removed, placed in 10% neutral buffered formalin, and submitted for histopathologic examination.
Histologically, the mass was composed of variably sized fronds of neoplastic epithelial cells supported by thin stalks of fibrovascular connective tissue extending outward from the surface epithelium. Well-differentiated keratinocytes displayed gradual orderly maturation progressing from the stratum basale outward to the stratum corneum. There was ballooning degeneration of keratinocytes within the stratum granulosum and stratum spinosum, and koilocytosis was observed. Basophilic keratohyalin granules present within the stratum spinosum were enlarged and often densely clumped. Nuclei frequently had marginated chromatin due to centrally located, round to oval, 10–15 μm in diameter, pale, basophilic to eosinophilic, intranuclear inclusions. Histologic features of the mass were consistent with a viral-induced cutaneous exophytic papilloma; however, a definitive cause for the clinical lameness in the dog was not found. The dog was reevaluated approximately 6 weeks later, and the only abnormal finding was pain upon palpation of the fifth digit of the right forelimb. Although the digit (including the nail) appeared grossly normal, the middle and distal phalanges of the digit were amputated due to continued pain and lameness. The excised tissue was preserved in 10% neutral buffered formalin and submitted for histopathologic examination.
Microscopically, a second papilloma was discovered at the junction of the digital pad and the ventral nail of the excised digit. The mass was composed of fronds of squamous epithelial cells that projected inward from the acanthotic surface epithelium. Histologic features of the mass were similar to the exophytic papilloma removed from the same digit, except for the endophytic orientation (Fig. 1) and lack of irregular keratohyalin granules in the stratum granulosum. The squamous epithelium of the inverted papilloma extended focally through the adjacent disrupted ventral nail, forming the lining of an expansile keratin-filled cyst encased within the nail proper (Figs. 1, 2). The cyst lumen contained flakes of laminated keratin, and the epithelium lining the cyst displayed orderly maturation and keratinization of epithelial cells through a sparse granular cell layer. Similar to the exophytic and endophytic lesions from this dog, epithelial cells lining the cyst displayed moderate ballooning degeneration, mild multifocal koilocytosis (Fig. 3), and sparse cytoplasmic keratohyalin granules. Epithelial cells contained numerous lightly basophilic intranuclear inclusions (Fig. 3). Adjacent to the cyst, the distal margins of the third phalanx were disrupted and fragmented with mild loss of cortical and trabecular bone. Moderate infiltrates of neutrophils and macrophages were centered on keratin fragments, and karyorrhectic debris was present between bony trabeculae of the distal third phalanx. The remaining bone trabeculae within this region were lined by osteoclasts, and a few bone fragments were hypereosinophilic and lacked lacunar osteocytes (osteonecrosis). Multifocal periosteal new bone formation was observed on the cortical surface of the remaining bone. Changes within the distal third phalanx were thought to be secondary to pressure-induced osteo-necrosis caused by the expanding subungual cyst. Inflammation was likely secondary to rupture of the cystic mass with release of keratin fragments into the surrounding tissue.
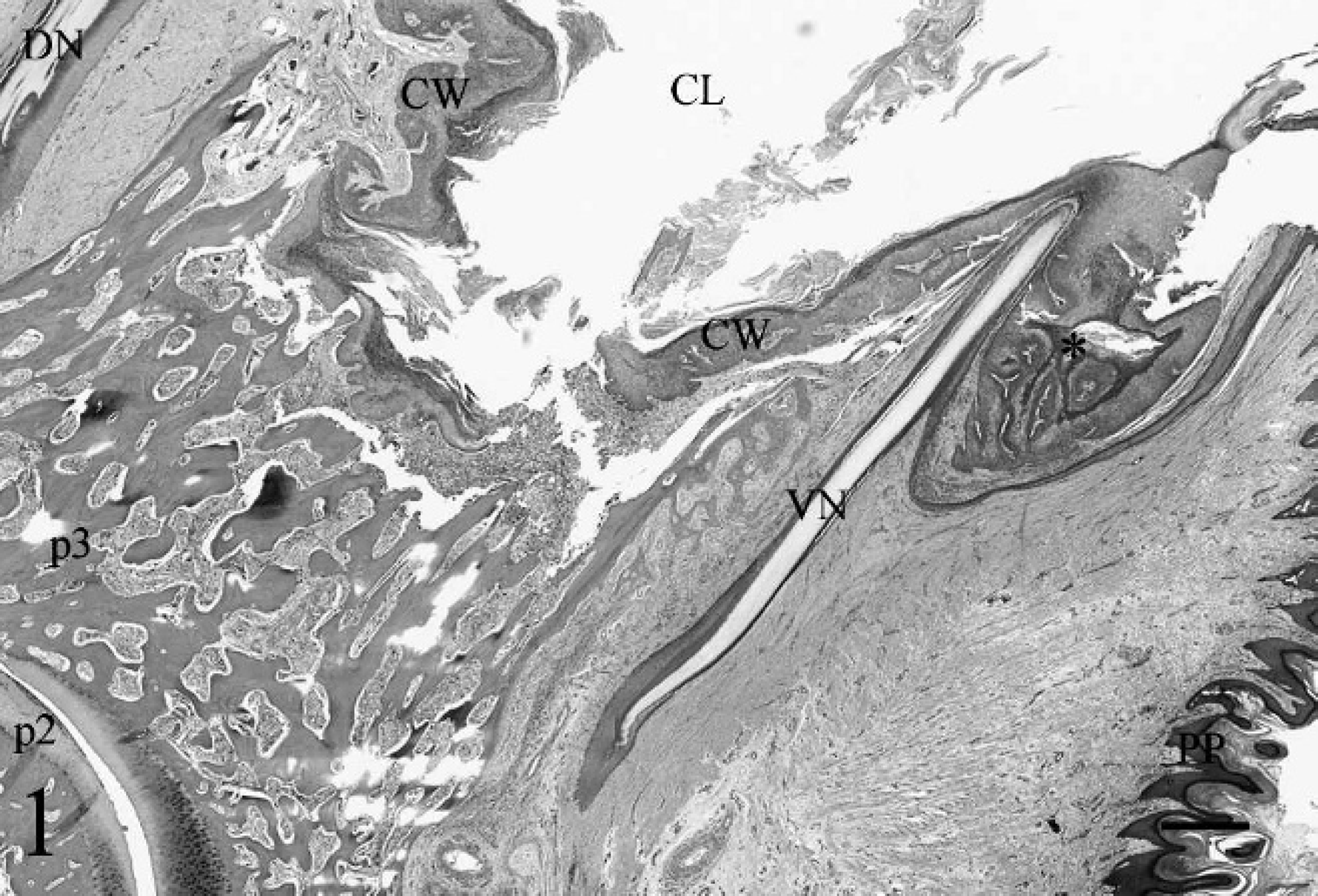
Midsagittal section of the lateral digit. Epithelium of the inverted cutaneous papilloma (*) extends through the ventral nail (VN) into the subungual space, forming an expansile cyst wall (CW). The cyst lumen (CL) contains fragments of laminated keratin. The distal interphalangeal joint is present in the bottom left corner. DN = dorsal nail; p2 = articular surface of distal second phalanx; p3 = bone of third phalanx; PP = paw pad. Hematoxylin and eosin. Bar = 1 mm.
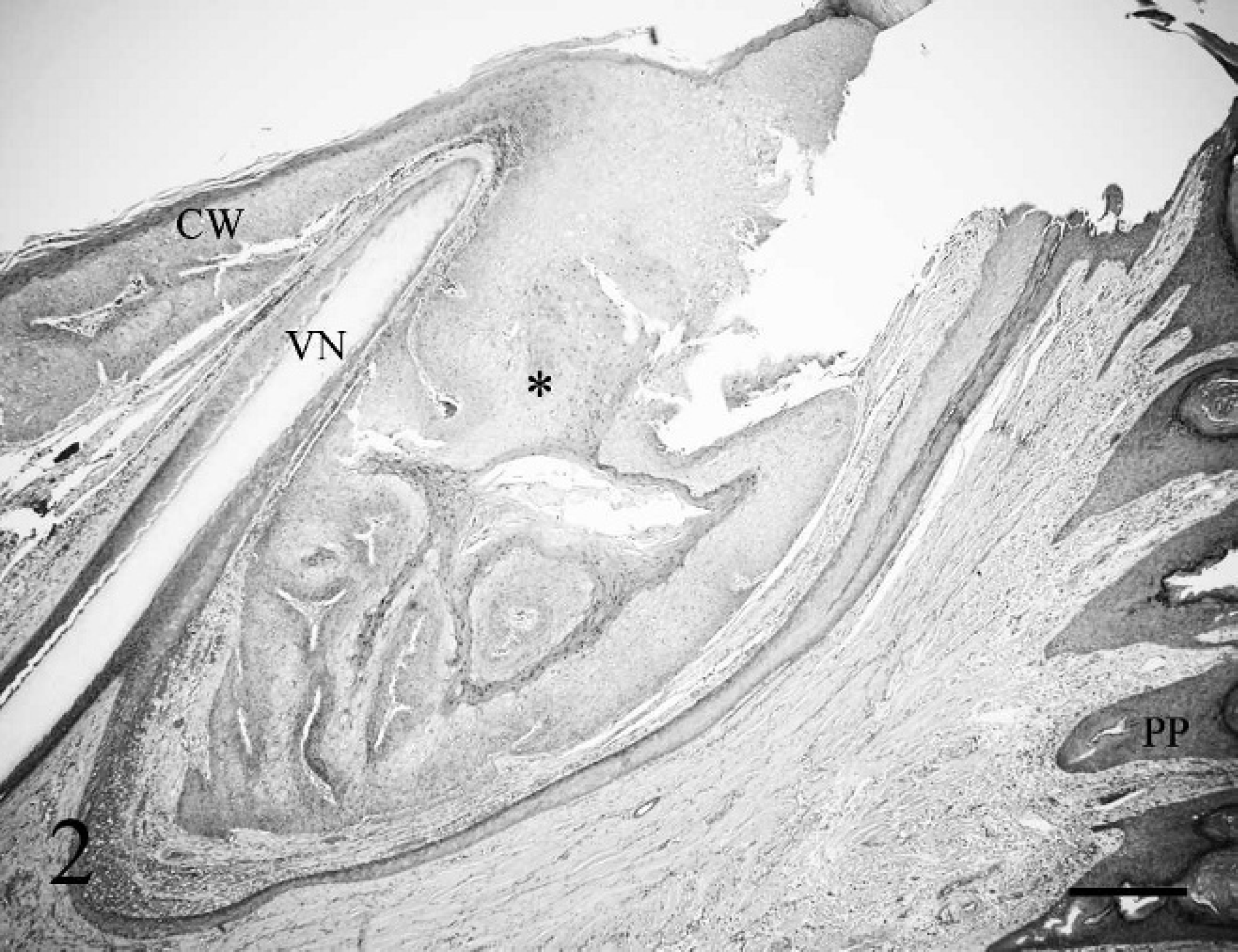
Well-organized stratified squamous epithelium of an inverted papilloma (*) extends through the disrupted ventral nail (VN) into the subungual space, forming the cyst wall (CW). PP = paw pad. Hematoxylin and eosin. Bar = 500 μm.
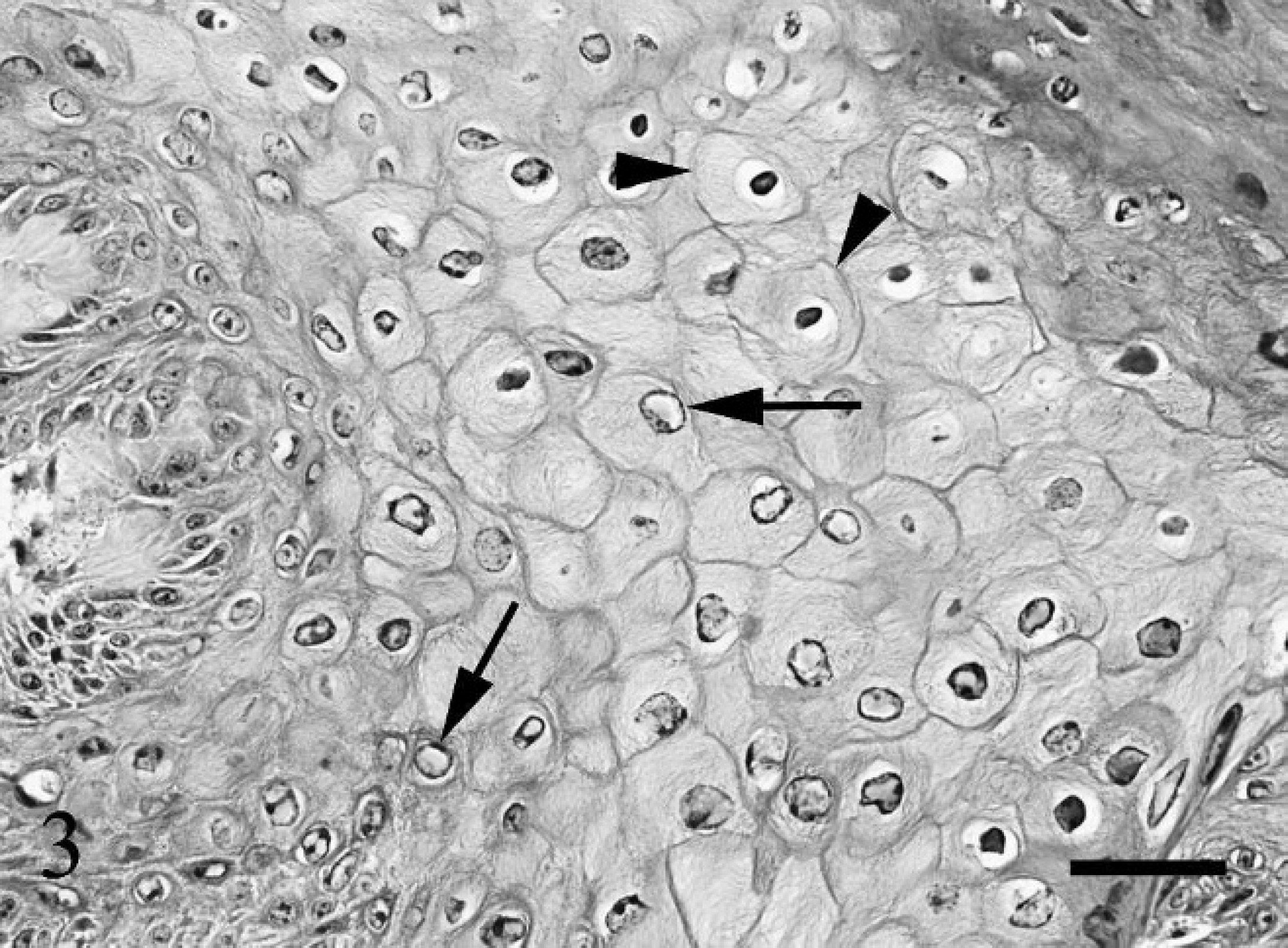
Keratinocytes in the stratified squamous epithelium of the subungual cyst wall contain numerous faintly eosinophilic to basophilic intranuclear inclusions (arrows) that measure 10–15 μm in diameter. Koilocytosis (arrowheads) is also present. Hematoxylin and eosin. Bar = 75 μm.
To confirm the suspicion of papillomavirus infection, electron microscopy was performed on the exophytic papilloma and the epithelial lining of the subungual cyst. Numerous particles characteristic of papillomavirus virions were present within affected nuclei. Virus particles had hexagonal outlines, measured approximately 40–45 nm in diameter, and were commonly aggregated into distinct crystalline arrays within the nucleoplasm or arranged in dense clumps (Fig. 4). Less frequently, virions were scattered within the cytoplasm of affected cells.
The lesion in this dog has similarities to digital lesions reported in other dogs, particularly nail bed epithelial inclusion cyst and nail bed inverted squamous papilloma. 5 Benign nail bed inclusion cysts are analogous to follicular cysts of infundibular origin, occur infrequently in the subungual region in dogs, and are most likely a result of trauma and subsequent embedment of portions of cuticular epidermis or nail bed epithelium in subjacent connective tissue. Nail bed inclusion cysts are non-neoplastic and have not been reported in association with papillomavirus infection; however, these lesions may rarely transform into squamous cell carcinoma. 5 Distinguishing features in the lesion in the current case include viral cytopathic effects, nuclear viral inclusions observed within epithelial cells lining the cyst, and the continuity of the cyst with the cutaneous papilloma.
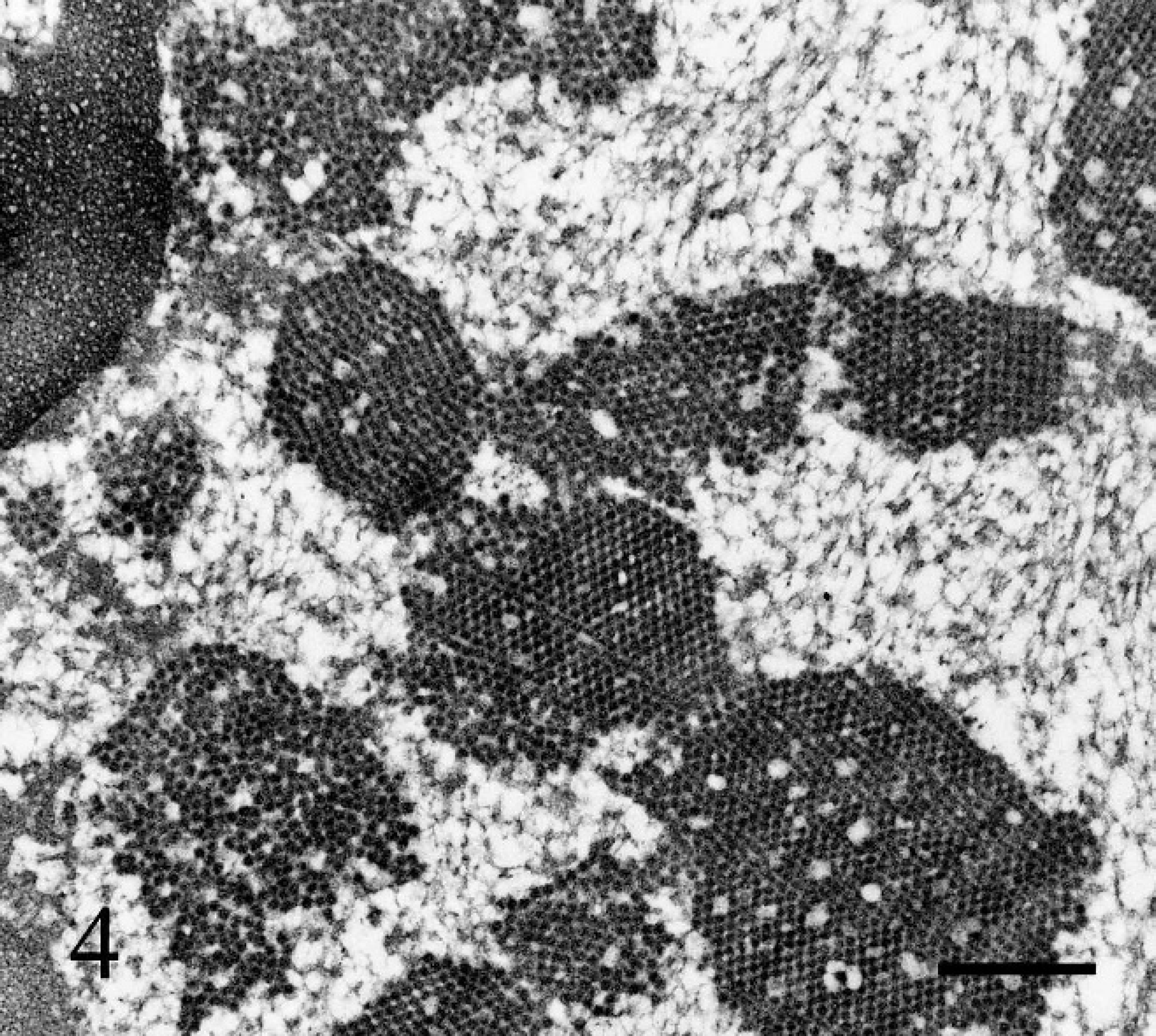
Numerous hexagonal, 40–45 nm in diameter, viral particles consistent with canine papillomavirus virions are arranged in crystalline arrays and dense clusters within the nucleoplasm of an affected keratinocyte. Electron micrograph. Bar = 500 nm.
Nail bed inverted squamous papillomas have been described in dogs, 5 but these neoplasms are also histologically distinct from the present case. Nail bed inverted squamous papillomas are thought to arise from the germinative epithelium of the nail and are characterized by a subungual cup-shaped mass filled with compact keratin. The wall of the cup is composed of a thick layer of squamous epithelial cells that forms delicate conical or papillary projections extending centrally into the keratin core. These histologic features were not present in the current case. Squamous nail bed papillomas in dogs are often associated with abnormal claws, broken or absent nails, and destruction of the third phalanx. Important distinguishing features observed in the current case that are not present in cases of nail bed inverted squamous papilloma include a clinically normal claw, continuity of the cyst with the cutaneous papilloma, and prominent viral inclusions. 5
A single case of multiple cutaneous digital papillomas in a dog has been reported. 2 As in the present case, the lesions reported in the young Beagle were thought to have originated from the skin adjacent to the digital pads rather than from nail bed epithelium. The lesion in the current case had 2 distinguishing features from that of the Beagle 2 : 1) local extension into the subungual space with cyst formation and 2) the presence of viral cytopathic effects.
In a recent review of benign and malignant canine digital neoplasms that resulted in amputation, a single inverted papilloma was diagnosed out of a total of 297 cases, revealing the infrequency of this tumor in this anatomic location. 7 An important differential diagnosis in the present case was squamous cell carcinoma, given the apparent extension of this cutaneous endophytic papilloma through the nail into the subungual space. Squamous cell carcinoma has been reported to be the most common histologic diagnosis in amputated canine digits. 7 Squamous cell carcinomas are composed of moderately to well-differentiated squamous epithelial cells, and invasion of adjacent digital bone is frequently a prominent feature of these neoplasms. 5 There was evidence in the present case of extension of the cutaneous mass into the subungual space; however, epithelial cells lining the subungual cystic portion of the mass displayed orderly maturation and minimal cellular atypia. In addition, neoplastic cell invasion was not present beneath the subepithelial basement membrane.
The present case is atypical of canine papillomavirus infection. Papillomaviruses are small, double-stranded DNA viruses that infect a wide variety of animal species. 4 These viruses are epitheliotropic and tissue specific, affect a wide variety of species, and can be grouped into viruses that affect cutaneous sites and viruses that affect mucosal sites. 6 In dogs, 2 genetically distinct papillomavirus types and several variations of papillomavirus-associated syndromes have been reported. 4 Classical viral-induced exophytic cutaneous papillomas in dogs are uncommon, usually occur on haired skin, and often spontaneously regress over time. Cutaneous inverted papilloma, first described 1988, 1 is a rare endophytic variant that is also associated with papillomavirus but typically does not undergo spontaneous regression. 3,4 Canine oral papilloma is another well-described benign lesion that occurs as single or multiple exophytic masses of the oral mucosa. Canine oral papilloma is also generally associated with papillomavirus; however, in situ hybridization suggests that these lesions are induced by a papillomavirus that is distinct from the virus that induces canine cutaneous papillomas. 1
Endophytic and exophytic cutaneous papillomas in dogs are considered benign lesions that may spontaneously regress and lack local invasion. The source of viral exposure and the mechanism of nail bed invasion in this case are undetermined. It is suspected that the lesion originated in the digital skin as cutaneous papillomas, and extension into the subungual space was potentially aided by damage to the nail. Clinical lameness was likely associated with pain caused by the expanding subungual cyst and pyogranulomatous inflammation subsequent to rupture of the cyst wall with release of keratin into the surrounding tissue. Pressure-induced bone lysis by subungual cyst expansion and mild periosteal bone proliferation have been reported in association with subungual inclusion cysts. 5
Acknowledgements. The authors thank Judy Stasko, National Animal Disease Center, Ames, IA, for her expertise with electron microscopy.