
Abstract
The current study was designed to determine the changes of the cardiac troponin I (cTnI) expression in blood and tissue during the myocardial degeneration in calves with foot-and-mouth disease (FMD). Seventeen crossbred calves presenting pathological signs for FMD confirmed by viral analysis were studied. A biochemistry panel and immunohistochemistry were performed on 17 diseased calves and 7 calves used as controls. Creatine kinase (CK), CK-myocardial band (CK-MB), aspartate aminotransferase (AST), and lactate dehydrogenase (LDH) activities were analyzed for both groups. Cardiac troponin I levels were measured by a commercially available enzyme-linked immunosorbent assay kit. Mean cTnI (14.8 ± 1.9 ng/ml) concentration and CK (573 ± 407 U/l), CK-MB (238 ± 37 U/l), AST (84 ± 7), and LDH (298 ± 29 U/l) activities were higher in FMD cases compared with controls. Immunohistochemistry revealed loss or depletion of cTnI expression in myocardium of all cases. None of the 7 controls showed loss of cTnI expression. Increased serum cTnI concentration correlated with myocardial injury and loss of cTnI immunolabeling in cardiomyocytes of calves with FMD.
Keywords
Introduction
Foot-and-mouth disease (FMD) is a highly contagious, notifiable disease of cattle, sheep, pigs, goats, and other domestic and wild mammals, and it is one of the most economically important diseases of livestock. 15 In calves, FMD produces high mortality. Often these young calves die suddenly due to acute severe myocardial injury without developing the characteristic blister lesions noted in adult cattle. 2 In fact, many calves die without any clinical signs of the disease. The primary lesions in the young animals in the current study were observed in the heart at necropsy. The myocarditis of young animals is acute, with hyaline degeneration and necrosis of muscle fibers and an intense infiltration of mainly lymphocytes. 2,6,37 The mortality rate is around 5% in mature animals but can run as high as 50% in young animals because of myocardial damage. 6
Cardiac troponin I (cTnI) is one of the subunits in the troponin complex bound to tropomyosin and actin on the thin filaments of striated muscle fibers, 9 and it is 1 of 3 isoforms of troponin known to be present exclusively in cardiac muscle. 4 Its serum concentration elevates after acute myocardial injury because of leakage from the damaged myocardial cells. 29,30 However, during the very early stage of myocarditis, the laboratory markers of myocardial cell damage, such as creatine kinase (CK) and CK-myocardial band (CK-MB) levels are often within the normal range in humans. 36 However, cTnI is now the preferred biochemical parameter in human medicine for assessing myocardial necrosis and myocyte damage, with virtually absolute myocardial tissue specificity as well as higher sensitivity than CK isoenzyme CK-MB, cardiac troponin C, and cardiac troponin T. 3,22 A remarkable homology exists in amino acid sequence between human and animals, and tissue reactivity of cTnI of various species revealed that cTnI can be used in animals. 29 Elevated cTnI has been reported in calves 17 and cattle, 16,29 indicating that elevations in the blood would serve as useful biomarkers of myocardial injury. Cardiac troponin I was also used as a histologic marker for myocardial injuries in humans 33 and dogs. 13 Increased cTnI levels were reported in human acute viral pericarditis cases 20 and in cattle with traumatic pericarditis. 16
The use of cTnI in veterinary medicine is biochemical 14,26,28,32 rather than immunohistochemical. In animals, only a few experimental studies have examined tissue microscopically to visualize the pattern of cTnI loss from the injured myocardium. 13,21 However, in humans, it was suggested that cardiac troponin immunolabeling might be useful to identify myocardial damage. 18
To the authors' knowledge, no study using cTnI immunoreactivity for diagnosis of cardiac injury in ruminants has been performed. However, it was previously suggested that serum cardiac troponin might be used for the diagnosis of myocardial degeneration due to FMD in calves 17 and in cattle with traumatic pericarditis. 16 However, the relationship between viral pericarditis and serum cTnI levels and its in vivo immunohistochemical expression has not been studied in veterinary medicine. The current study was designed to investigate the practical value of using biochemical and histologic assessment of cTnI concentration to detect myocardial degeneration in calves with FMD.
Materials and methods
Animal material
The current study involved 17 calves with clinically diagnosed FMD during a disease outbreak between January and July 2006 and 7 healthy control animals. Cases were submitted to the Department of Pathology, Faculty of Veterinary Medicine, University of Kafkas (Kars, Turkey) for pathological examination. Samples collected from cases were also submitted to the Foot and Mouth Disease Institute (Ankara, Turkey) for disease confirmation and serotyping. Control animals were obtained from a slaughterhouse where blood samples were collected before slaughter and heart tissue was taken after slaughter. Control animals were not age matched, but all controls were under 1 year of age, ranging from 6 months to 11 months.
Necropsy and histopathology
Necropsy was performed in all cases that died of FMD. Myocardial tissue specimens were collected from the interventricular, the right and left atrial, and ventricular parts of the hearts. All tissue specimens were divided into 3 equal parts. Samples were taken from these parts for a total of 15 samples per case. Tissue samples taken from heart were fixed in 10% buffered formalin. Selected blocks were processed and embedded in paraffin. Sections (4-6 μm) were then cut from each block for histologic examination and immunolabeling.
Serum biochemistry
Blood samples were collected from diseased calves before necropsy and control calves before slaughter and centrifuged at 800 × g for 10 min. Serum samples were harvested and then stored at −20°C until analyses. Serum CK, CK-MB, aspartate aminotransferase (AST), and lactate dehydrogenase (LDH) activities were determined on a spectrophotometer a using commercial kits. b
Cardiac troponin I analyses
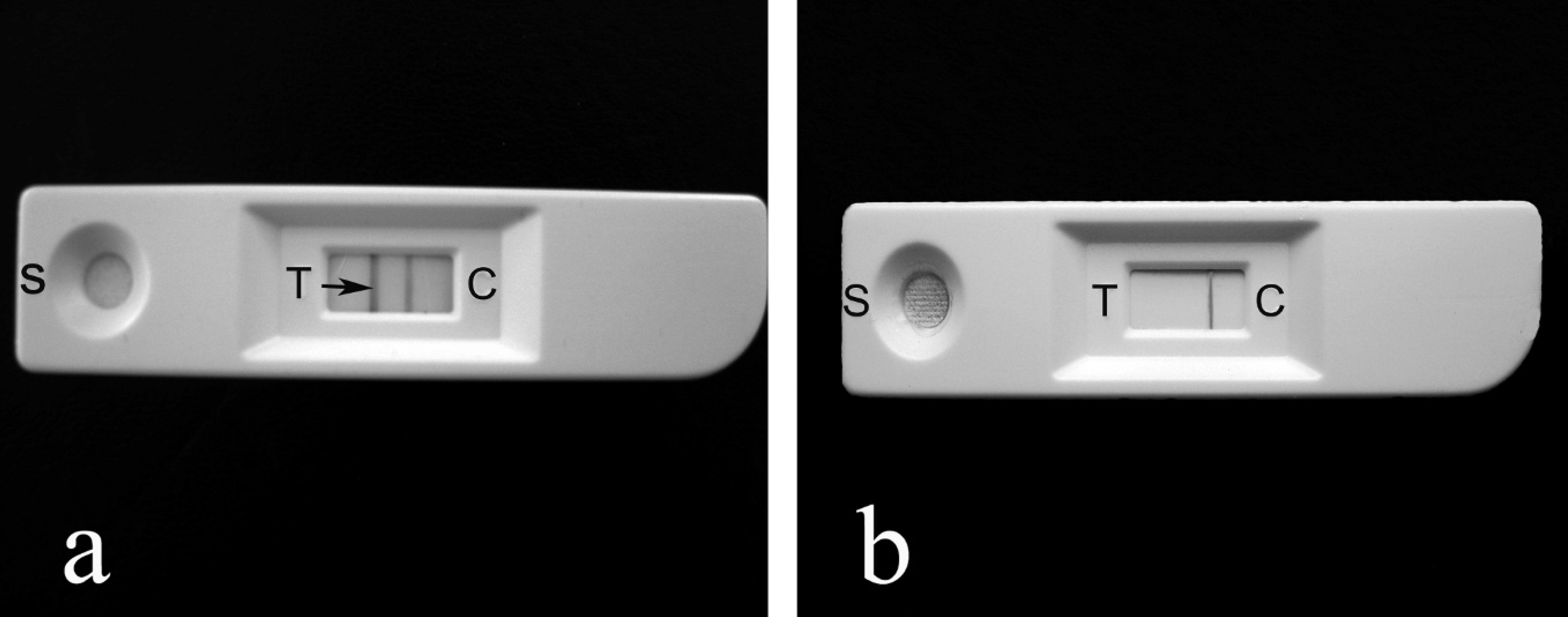
Serum cTnI reactivity was determined using a rapid assay, Card-I Kit Combo Test, c following the manufacturer's instructions. Results were recorded as positive when 2 red-brown lines appeared in the chamber within 15–20 min of the test and negative when 1 line was observed. A commercially available enzyme-linked immunosorbent assay (ELISA) kit d was used to determine cTnI concentration in all animals. The ELISA was performed and the results were calculated (ng/ml) following the manufacturer's instructions.
Immunohistochemistry
Sections from all tissue samples were cut to 4–6 μm and processed for immunohistochemical examination by a streptavidin-biotin-peroxidase complex (ABC) method. Tissue sections were placed on 3-amino-propyltrieyhoxysilanecoated e slides, dewaxed, and hydrated. Antigen retrieval was facilitated by heating in citrate buffer (pH 6.0) for 10 min in a microwave oven with a power of 800 watts. The slides were then dipped in freshly prepared absolute methanol containing hydrogen peroxide 3% vol/vol for 15 min to quench endogenous peroxidase activity. Sections were treated with goat anti-cTnI (1:100; C–19: sc-8118) f for 60 min. After washing with phosphate buffered solution (PBS), the slides were incubated rabbit anti-goat immunoglobulin G diluted at 1:300 in PBS for 30 min at room temperature. Sections were then incubated with ABC g diluted at 1:300 in Tris-buffered solution for 30 min at room temperature. After washing with PBS, the slides were treated for 5 min at room temperature with 3,3′-diaminobenzidine tetrahydrochloride g (DAB) in PBS (0.5 mg DAB/ml) containing hydrogen peroxide 30% vol/vol. Finally, sections were counterstained with Mayer's hematoxylin, dehydrated, and mounted.
Normal heart myocardium obtained from healthy control animals was sampled and trimmed identically to the clinical cases served as positive control. In addition, each slide had its own built-in negative and positive controls: arteries within the myocardium were expected to be negative for cTnI and Purkinje fibers were positive for cTnI. An additional negative control for immunolabeling procedure consisted of replacing primary antisera with saline.
Scoring of cTnI immunolabeling results and statistical analysis
The percentage of the total area of the cTnI-positive cardiomyocytes, including cells with decreased labeling, was assessed semiquantitatively under a light microscope with 10X ocular grids and a 40X objective. Mean percentage of total area of labeled myocytes in 10 fields of each section was calculated, and this was repeated for 15 sections of heart from each calf. The final mean value was accepted as the immunolabeling score for each animal. Consistency was maintained by evaluating similar regions of heart from case to case. The mean immunolabeling score determined for each animal was also explored in statistical analyses. Seven slaughterhouse control cattle were included in the statistical comparison. For the statistical analysis, differences between the groups were tested by analysis of variance and Duncan test using SPSS for Windows (version 10.0). h Data were presented as mean ± standard deviations, and P values less than 0.05 were considered significant.
Rapid cardiac troponin I (cTnI) assay kit.
Results
Calves attended by the authors (HME, MC, EU, and EG) were comatose. Raised heart and respiratory rates and murmur were determined on auscultation. Adult cattle had typical lesions of FMD on the mouth, feet, and teats on the same farms where study material was obtained. Results obtained from Foot and Mouth Disease Institute revealed Aphthovirus (family Picornaviridae) serotype A 22.
Biochemistry
The rapid cTnI assay kit revealed that all cases were positive as indicated by the 2 colored lines appearing in the test window; controls were negative (Fig. 1a, 1b). The concentration of cTnI and activities of CK, CK-MB, AST, and LDH are given in Table 1.
Gross pathological findings
Control heart tissues did not reveal any gross lesions. The pericardial sac of calves with FMD contained up to 50 ml of fluid and fibrin. The atria and coronary vessels were hyperemic. Occasionally, the pericardial surface was rough. The myocardium was soft and flaccid in consistency, containing white or grayish stripes or spots (like “stripes on a tiger”). The lesions were widespread in the subepicardial muscle and particularly frequent near the base of the heart. Lesion diameter was variable and ranged from 5 to 20 mm.
Histopathological findings
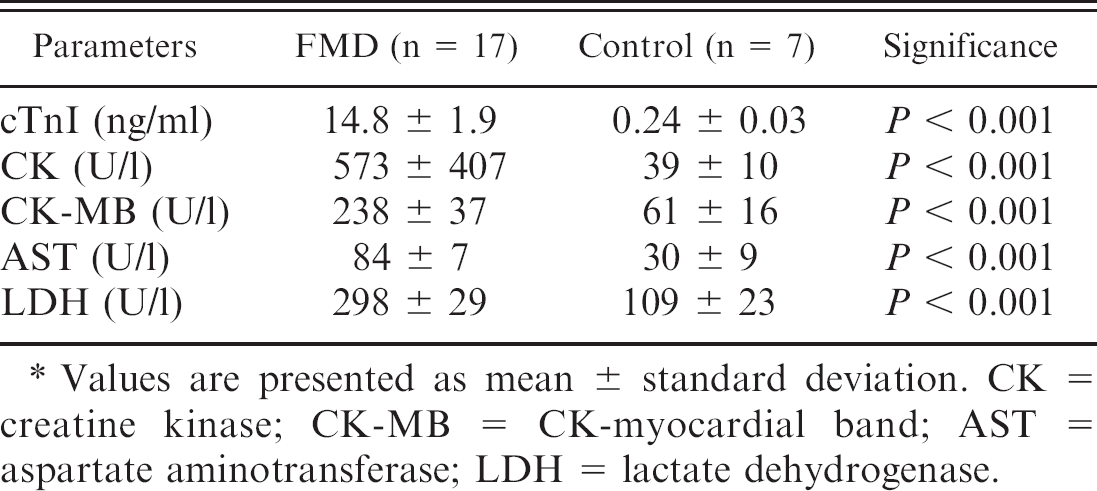
Although degenerative lesions were not present in the control calves, affected hearts from calves with FMD exhibited severe hyaline degeneration, necrosis, mineralization of occasional myocardial fibers, and marked interstitial aggregations of inflammatory cells (mainly mononuclear and some neutrophils). The ventricular myocardium was most markedly affected, but some auricular muscle fibers had also undergone degenerative changes. Myocardial degeneration and necrosis occurred both focally, in and near inflammatory areas, and diffusely, involving large areas through which inflammatory foci were scattered (Fig. 2a, 2b). Degenerative muscle fiber cells were swollen, and the cross striations disappeared. Cardiac myocyte nuclei within the foci of myocarditis were hyperchromatic, pyknotic, or karyorrhectic. With development of necrosis, the nuclei disappeared and muscle fibers disintegrated into irregular masses of eosinophilic amorphous and granular debris. In these areas, some of the macrophages that invaded the damaged fibers contained large eosinophilic granules of necrotic debris within their cytoplasm. Fine mineral granules were scattered indiscriminately among the necrotic contents of some fibers. A focal acute vasculitis affected a few small vessels.
Serum cardiac troponin I (cTnI) concentration and biochemical changes in enzymatic activities in foot-and-mouth disease (FMD) cases and healthy calves.*
Values are presented as mean ± standard deviation. CK = creatine kinase; CK-MB = CK-myocardial band; AST = aspartate aminotransferase; LDH = lactate dehydrogenase.
Myocarditis caused by foot-and-mouth disease.
Immunohistochemistry
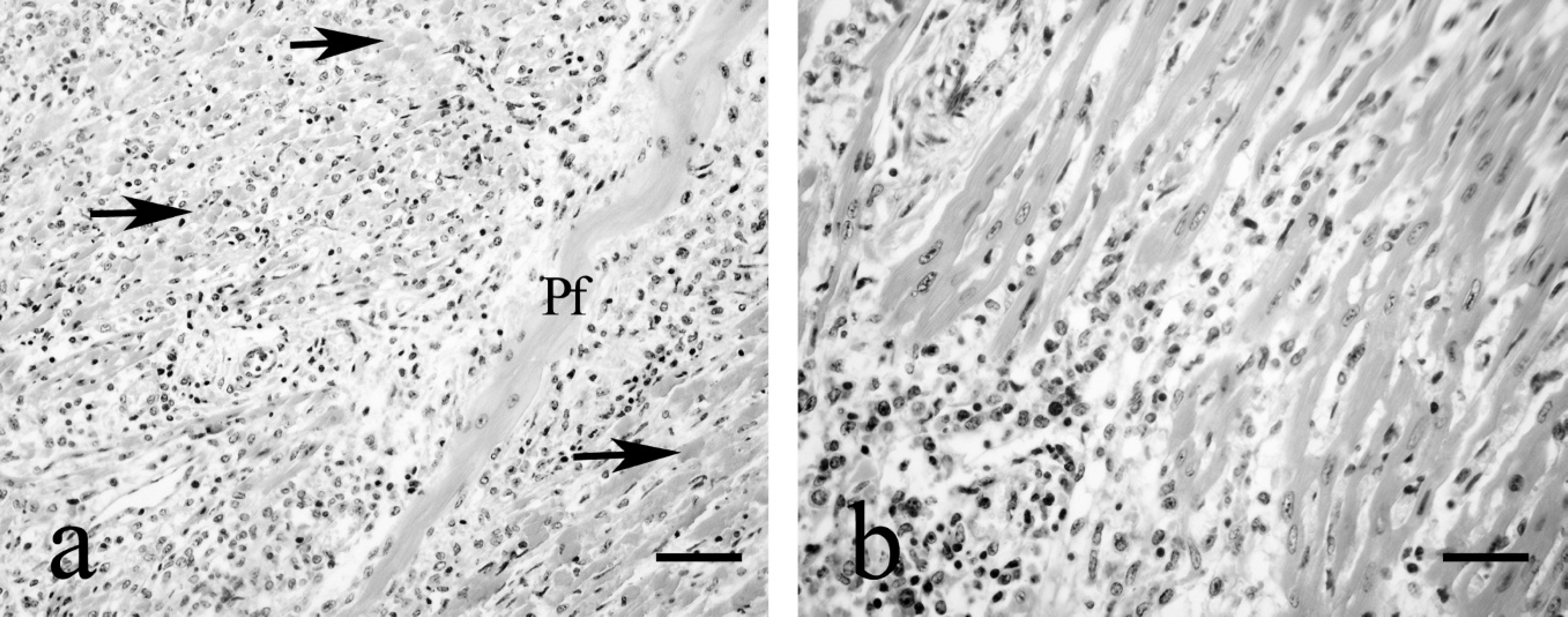
The immunohistochemical investigation of the samples revealed a marked depletion of the cTnI in all the hearts of calves with FMD (Fig. 3a–e). In normal myocardium from a slaughterhouse control animal, strong and diffuse cytoplasmic cTnI immunoreactivity was observed in the cardiac myocytes (Fig. 3f). No other components of cardiac wall expressed cTnI reactivity. There was a statistically significant difference (P < 0.001) between control hearts and hearts with FMD for the immunolabeling analysis score despite the fact that the evaluation method used significantly underestimated the magnitude of the loss of cTnI immunolabel from cardiomyocytes. The semiquantitative assessment of cTnI immunolabeling and the statistical differences in the cardiac muscle of calves with FMD and control calves are summarized in Figure 4.
In all 17 calves with FMD, significantly decreased immunoreactivity occurred in cardiac muscle cells, particularly myocytes with microscopic features of degeneration and necrosis. Total loss of immunolabeling was seen in areas with severe degeneration and necrosis. Loss of cTnI tended to be greater at the center of these regions rather than the periphery (Fig. 3a). Loss of cTnI immunolabeling was also identified, even in the absence of histologic proof of myonecrosis or degeneration. Some of the hematoxylin and eosin (HE)-stained sections of these samples showed only subtle hypereosinophilia. Interstitial aggregations of inflammatory cells (mainly mononuclear and some neutrophils) were negative for cTnI. However, some of the neutrophils and macrophages containing necrotic substance within their cytoplasm exhibited intense cytoplasmic cTnI immunoreactivity (Fig. 3e).
Discussion
Serum cardiac troponins are the earliest appearing biochemical markers during myocardial damage. 7,11,31 The unique aspect of cTnI being 100% tissue specific for the heart 9 makes it an excellent marker to serve as a biochemical and immunohistochemical tool for detecting myocardial injury. The continuing cellular release and clearance of cTnI account for its excellent diagnostic sensitivity.
Serum cTnI concentrations increase in several types of myocardial injury because of leakage from the damaged myocardial cells. 1 Measurement of cTnI in various animal species serves as a useful biomarker of myocardial injury. 29,30 In humans, release of cTnI from the heart into the systemic circulation in acute pericarditis is representative of inflammatory myocardial cell damage. 10 Studies in humans with acute myocardial infarction have shown that cTnI peaks on average within 11 hr and persists for around 100 hr. 8,20 Cardiac troponin I concentration in a cow with idiopathic pericarditis was reported as 0.89 ng/mL, and values of 5 healthy cattle ranged from 0 to 0.04 ng/mL in the same study. 21 In the current study, significantly elevated cTnI levels ranged from 11.7 to 16.4 ng/ml in FMD cases; the mean cTnI concentration was 0.24 ng/ml in healthy calves.
Cardiac troponin I (cTnI) immunoreactivity in the heart of calves with foot-and-mouth disease. Marked depletion (panels a–e) of the cTnI compared with control (panel f). Avidin-biotin-peroxidase complex method.
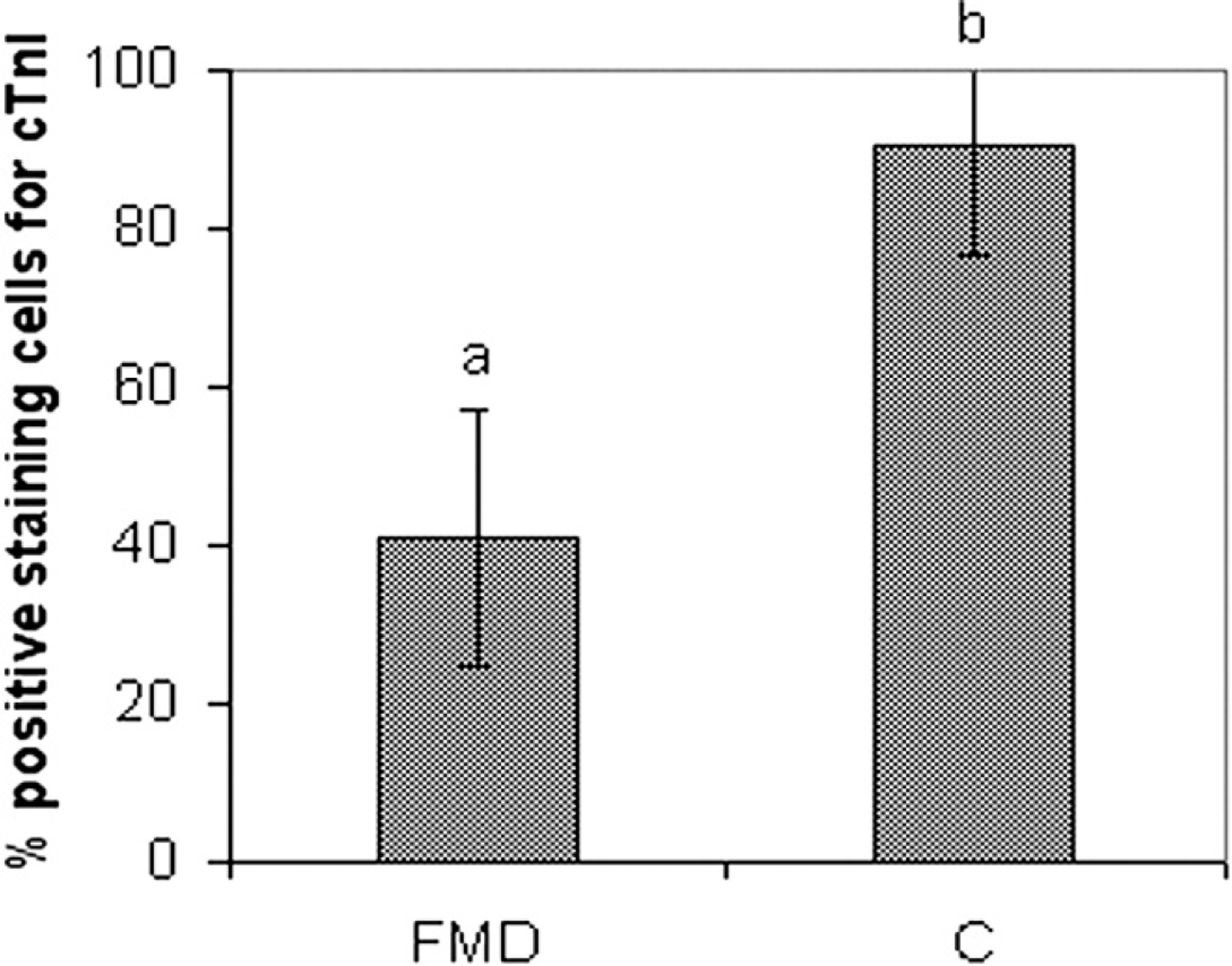
Semiquantitative analysis of cardiac troponin I (cTnI) immunolabeling results. FMD = foot-and-mouth disease; C = control. Values are presented as mean ± standard deviation.
Comparison of the histologic and biochemical data revealed an inverse correlation between histologic score values and the serum concentration of the markers. Immunohistochemistry of all 17 FMD cases showed well-defined areas with significant reduction or total loss of cTnI expression, indicating the presence of myocardial cellular degeneration. Elevated CK, CK-MB, LDH, and AST activities and cTnI concentration in FMD-induced myocarditis supported the immunohistochemical findings. Similar results were reported for humans with viral pericarditis. 20 Furthermore, a previous study 34 demonstrated that in dogs, increases in serum troponins occurred in parallel with loss of troponins from the ischemic myocardium. In rats, alterations in cTnI occurred with severe left ventricular remodeling. 35
It was reported that the serum cardiac troponin concentration was an earlier marker of myocardial injury after virus infection than was the histologic finding of inflammation. 25 The increase of serum cTnI and reduction or loss of cTnI expression in tissue are roughly related to disease severity, probably reflecting the extent of inflammatory and degenerative changes of the myocardium. In humans, maintenance of high serum concentrations of cTnI was considered an indication of a poor prognosis in advanced heart failure. 19 Also in humans, the definitive diagnosis of myocarditis has to be established by the demonstration of myocytolysis and lymphocytic infiltrates in the endomyocardial biopsies, 5 and acute myocarditis was histologically diagnosed in only 10% of the patients with clinically suspected myocarditis. 27
It was suggested that cardiac troponin immunolabeling might be useful for identifying myocardial necrosis in human autopsy hearts. 18,33 Similarly, an experimental dog model of myocardial infarction revealed that loss of tissue cTnI could be seen in infarcts as early as 30 min, even before histologic evidence of necrosis appeared. 13 These results show that immunolabeling for cTnI was more sensitive than routine HE staining for the recognition of peracute myocardial necrosis in both experimental animals and humans.
In the present study, heterogenous loss of cTnI was seen in the degenerated myocardium. There was a great deal of variability in intensity of residual staining for cTnI within the degenerative areas. Heterogeneous loss of immunolabeling occurred in dog hearts with experimental myocardial ischemia. 13 This variability of the immunolabeling was based on heterogeneous distribution of flow within the ischemic tissue with necrosis occurring faster in some parts of the myocardium than others. 13 This variability of immunolabeling intensity was attributed to heterogeneous distribution of blood flow within the ischemic tissue that resulted in differing rates of onset and progression of cardiac necrosis. In some necrotic cardiomyocytes, decreased immunohistochemical labeling for cTnI could be due to loss of immunoreactivity, to some unknown degree, due to the in situ degradation of this protein rather than release of the immunogenically intact protein fragment from the injured cell.
It was well established that cardiac troponins are cleared from blood faster than CK-MB, but concentrations stay elevated longer. 23 Because 94% of troponins are bound in the structure of myofibrilla, and 6% are dissolved in cytosol, 24 in cases of severe cell damage the proportion that is dissolved in the cytosol can immediately be released into blood by diffusion. In contrast, the major proportion of troponins can only be released after proteolytic disintegration. This delayed release from the injured cell is the reason for the relatively long period during which increased troponin concentration is detectable in serum, although the fragments continue to be subjected to proteolytic disintegration within the blood stream. 24 These findings indicate continued, delayed release of troponins from necrotic myocytes. 13 A previous study 13 suggested that the sustained elevation of cardiac troponin in the blood resulted from ongoing release during infarct development.
In the current study, the loss of immunolabeling paralleled histologic evidence of injured myocytes in the tissue. Depletion or loss of cTnI immunolabeling was pronounced at the center rather than the periphery of the lesions. However, an earlier study 13 observed greater loss at the periphery of an infarct than at its center in an experimental dog myocardial ischemia model. The authors of that study suggested that the phenomenon was possibly due to greater antegrade and retrograde flow at the periphery of the infarct with washout of proteins from necrotic myocardium. 12,13 The authors 13 further suggested that greater depletion of cardiac troponin occurring at the periphery of the infarct, particularly with reperfusion, represents a manifestation of this washout. However, the opposite finding in the present study was likely related to the different pathogenesis involved in viral myocarditis that resulted in a diffuse pattern of myocardial degeneration and necrosis. The positive immunolabeling of the periphery of the lesions might have resulted solely from the limited damage of the myocytes.
In conclusion, the present study demonstrates that elevated serum cTnI levels can potentially provide solid evidence for myocardial injury during FMD in calves, and serum cTnI concentrations are well correlated with depletion or loss of tissue cTnI expression. Measurement of serum cTnI is highly sensitive and specific for cardiac myocyte injury in calves with FMD and may be an important first step toward the design of new methods to diagnose FMD-induced myocarditis. In animals with clinically suspected myocarditis, measurement of cTnI is a very sensitive way of demonstrating myocardial cell damage. Furthermore, it is suggested that evaluation of immunohistochemical expression of cTnI represents a highly sensitive marker of myocardial degeneration and necrosis.
Acknowledgements
The authors wish to thank the Foot and Mouth Disease Institute (Ankara, Turkey) and Vet. Med. Rahsan Koç for assistance with this research.
Footnotes
a.
UV-1201 Spectrophotometer, Shimadzu Corp., Japan.
b.
IBL, Hamburg, Germany.
c.
AboaTech, Turku, Finland.
d.
CARD-I-KIT ELISA cTnI, Labmaster Oy, Turku, Finland.
e.
Sigma-Aldrich, St. Louis, MO.
f.
Santa Cruz Biotechnology Inc., Santa Cruz, CA.
g.
Dako North America Inc., Carpinteria, CA.
h.
SPSS Inc., Chicago, IL.