
Abstract
A 13-year-old female spayed Domestic Shorthair cat presented with a history of right-sided mucopurulent nasal discharge for 18 months. Computed tomography revealed a mass within the right nasal cavity and the right frontal sinus. The animal was euthanized, and a postmortem examination was performed. On macroscopic examination, the right nasal cavity and the right frontal sinus were partially occluded by a soft whitish mass. Microscopically, the mass was composed of well-differentiated plasma cells that were immunopositive for immunoglobulin G and lambda light chains. These findings were consistent with a mature-type sinonasal plasmacytoma. In addition, there was right-sided mucopurulent rhinitis and sinusitis caused by a Pasteurella infection, which probably developed secondary to the sinonasal plasmacytoma. To the authors’ knowledge, this is the first report of a sinonasal plasmacytoma in a cat. The present communication shows that feline sinonasal plasmacytomas should be included in the differential diagnosis for tumors located in the upper respiratory tract of cats.
Plasma cell tumors are formed by a monoclonal proliferation of plasma cells, which are terminally differentiated cells in the B-lymphocyte lineage. In domestic animals, plasma cell tumors are most commonly reported in dogs, less frequently in cats, and rarely in other species. 6 Neoplastic plasma cell proliferations include multiple myeloma (MM), solitary osseous plasmacytoma (SOP, synonym: solitary myeloma), and extramedullary plasmacytoma (EMP). 17 Neoplastic plasma cells of MM are located in the bone marrow cavity of multiple skeletal sites and often in other organs, such as the spleen, liver, and lymph nodes. 6 Extramedullary plasmacytomas are primary plasma cell tumors located in the skin, mucosa-associated sites, and other organs. In dogs, EMPs usually are solitary masses and affect middle-aged to old dogs. They are most frequently observed in the skin, oral cavity, and anorectal mucosa. 4,13 Individual cases of canine EMP have been reported in other locations, such as the lungs, spleen, kidney, vertebral canal, and brain. 6 Canine cutaneous and oral EMP are usually benign tumors with uncommon local recurrence and very rare metastases. 4,6,13 In contrast, EMPs in locations other than the skin and oral cavity frequently metastasize to regional lymph nodes. 6 Similar to dogs, 6 most feline plasma cell tumors are described in older animals with an average age of 8 to 9 years. 6,9,17 The estimated incidence of MM in cats is much lower than in dogs, in which these tumors account for about 8% of all hematopoietic neoplasms. 17 Considering the limited number of reported cases, feline EMPs appear to be rare tumors. They are most commonly described in the skin of a variety of body areas. 9 Other reported locations for feline EMPs include the oral cavity, 9 gastric mucosa, 19 retroperitoneal space, 10 globe, 11 liver, 8 and cerebrum. 5 To the best of the authors’ knowledge, primary sinonasal plasmacytoma has not been previously reported in cats, dogs, or other domestic animals. In people, however, primary EMPs are most commonly located in the upper respiratory and digestive tract, with the nasal cavity and nasopharynx as predilection sites. 15
The present communication describes a sinonasal plasmacytoma in a 13-year-old female spayed Domestic Shorthair cat. The cat had been sneezing for several months and had a right-sided mucopurulent nasal discharge of 18 months’ duration. On presentation, clinical signs were limited to right-sided nasal discharge and stridor nasalis. A complete blood cell count was within normal limits. Serum biochemical analysis showed no significant alterations. Creatine kinase activity was mildly elevated, which was most probably caused by restraint of the animal during venipuncture. All other parameters, including globulins and serum calcium, were within normal limits. In detail, in the 2 examined serum samples, the following concentrations of total protein, albumin, and globulins were measured: total protein 75.8 and 72.3 g/1 (reference range 61–80 g/1), albumin 32.6 and 31.3 g/1 (reference range 28–42 g/1), globulins 43.2 and 41.0 g/1 (reference range 25–46 g/1).
A computed tomographic examination revealed increased density within the right nasal chamber with loss of turbinate detail, extension into the nasopharynx, and increased density within the right frontal sinus compatible with extension of the disease into the frontal sinus (Fig. 1). Rhinoscopy confirmed the presence of a proliferative mass within the right nasal cavity. An initial biopsy, which was taken from the intranasal mass by endoscopy, showed the presence of dense plasma cell infiltrates admixed with respiratory epithelium, nasal glands, and fragments of bone. Plasma cells were mildly anisocytotic with rare mitotic figures. Because of the presence of the dense plasma cellular infiltrate and lack of other inflammatory cells, plasmacytoma was suspected. The cat was euthanized and submitted for a complete postmortem examination.
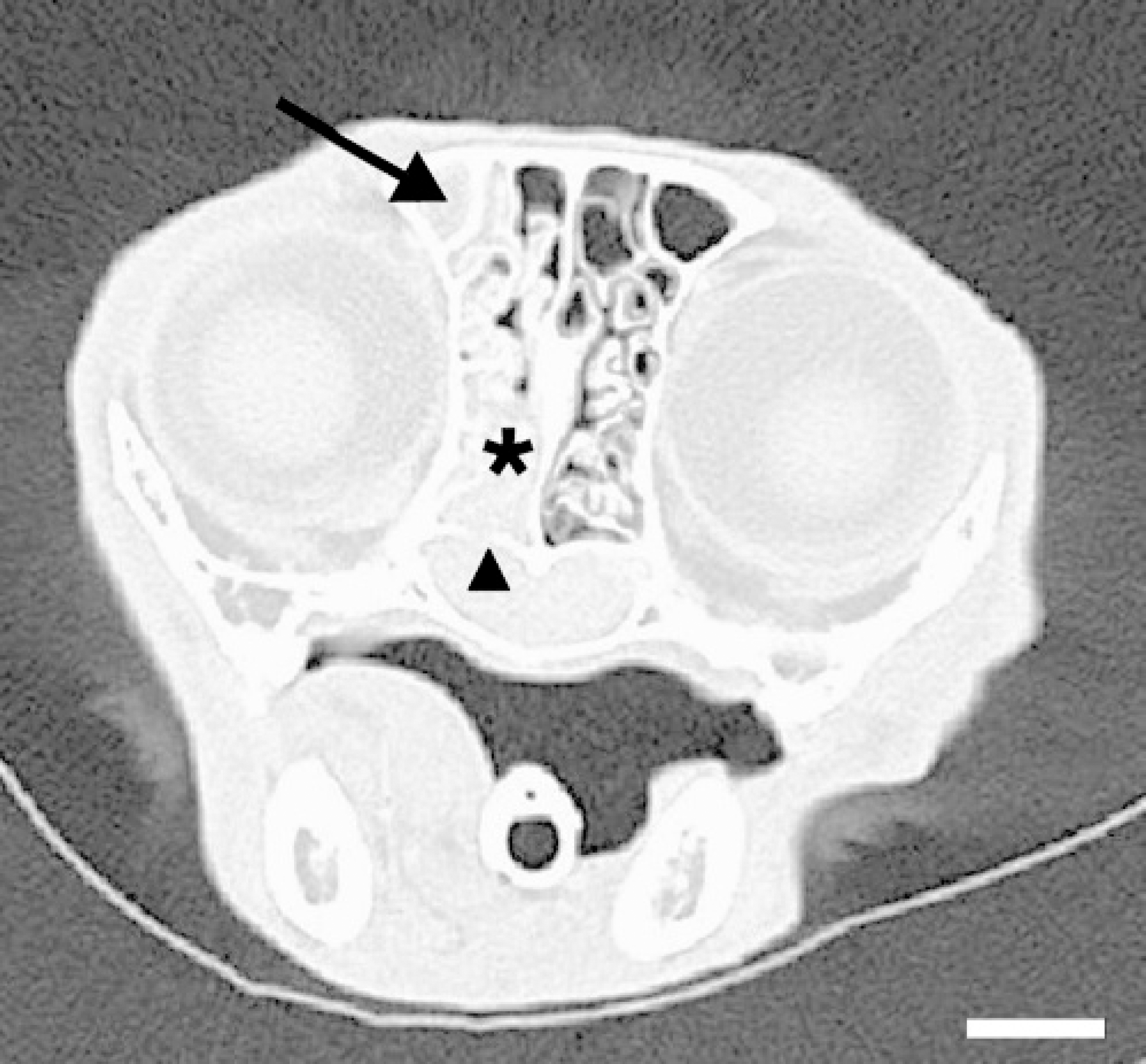
Transverse postcontrast computed tomographic image (window level: −200; window width: 2,000) at the level of the ethmoid turbinates. There was soft-tissue density in the right frontal sinus (arrow), in the right nasal cavity with turbinate destruction (asterisk), and within the nasopharynx with evident bone destruction (arrowhead). Bar = 1 cm.
At gross examination, the right nasal cavity contained a grayish soft mass that measured approximately 3 − 0.75 − 0.5 cm. The intranasal mass partially replaced the nasal and ethmoidal conchae and occluded the nasal and ethmoidal meatuses. The right frontal sinus was filled by a whitish soft mass and opaque mucinous material (Fig. 2).
The cranial lobe of the left lungs had multifocal small, mildly depressed red areas. Other tissues and organs were unremarkable on macroscopic examination. A swab from the mucinous material of the right frontal sinus and a sample of lung tissue were cultured for aerobic and anaerobic bacteria. Selected tissue samples of all organs were fixed in 10% neutral buffered formalin, processed by routine methods followed by paraffin embedding, sectioned, and stained with hematoxylin and eosin. A Congo red stain was applied to sections from the sinonasal mass.
Within the affected areas of the right nasal cavity and the right frontal sinus, the subepithelial fibrous connective tissue was markedly expanded by sheets of densely packed plasma cells that were separated by fine fibrovascular tissue septae. Sheets of plasma cells effaced nasal glands and formed raised masses, which partially occluded lumens of the nasal and ethmoidal meatuses (Fig. 3A). More than 95% of the plasma cells were well differentiated (mature-type plasma cells). These cells were ovoid with a singular eccentric-located nucleus with clumped chromatin and a moderate amount of amphophilic cytoplasm with often a distinct perinuclear halo. About 10% of these plasma cells contained intracytoplasmic Russell bodies (Mott cells). Less than 5% of the plasma cells were mildly enlarged, round to polygonal cells. Most of the mildly enlarged cells contained a singular vesicular nucleus. Binucleate cells were rarely noted (Fig. 3B). The mitotic rate averaged less than 1 mitotic figure per 40− power field. Conchal bone, which was surrounded by plasma cells, was often fragmented into bony trabeculae, which were lined by osteoblasts and scattered osteoclasts (osteolysis and remodeling of bone). The remaining nasal mucosa of the right nasal cavity was mildly edematous and infiltrated by a moderate number of plasma cells, including some Mott cells, lymphocytes, and scattered neutrophils. The lumens of the right nasal cavity and the right frontal sinus were plugged by proteinaceous and mucinous material containing numerous neutrophils and scattered macrophages (Fig 3A). The Congo red stain for amyloid deposition in the sinonasal mass was negative.
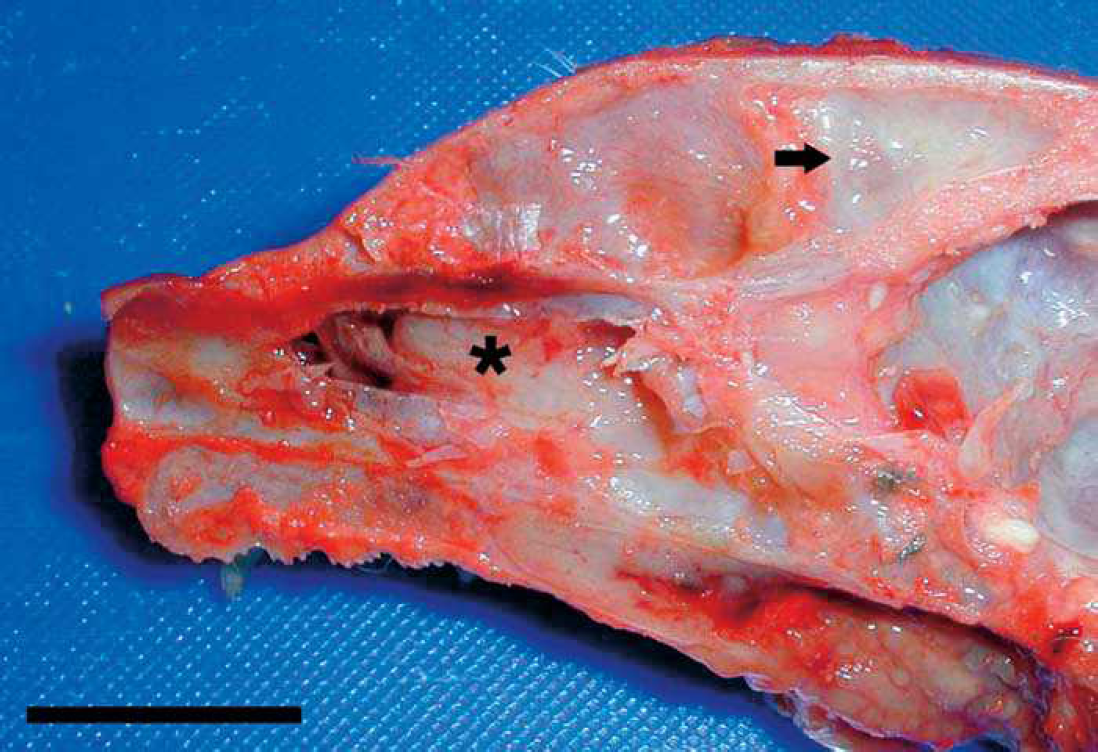
Length section through the head with partially removed nasal septum. Caudal and middle aspects of the right nasal cavity contained a whitish soft mass (asterisk). The right frontal sinus was partially occluded by similar whitish tissue and contained mucoidmaterial (arrow). Bar = 2 cm.
Postmortem bone marrow samples obtained from both proximal femoral metaphyses had a cellularity within normal limits with approximately equal amounts of hematopoietic precursor cells and adipose connective tissue. Adequate numbers of erythroid and myeloid elements were present. Erythroid late stages predominated. Within the myeloid line, the storage pool was depleted with a reduced number of band and segmented neutrophils. Megakaryocytes were adequate in number and maturation.
Suppurative bronchiolitis was found in the left cranial lung lobe. Additional microscopic findings included moderate alveolar pulmonary edema, mild multifocal interstitial lymphoplasmacytic nephritis, pancreatic islet cell amyloidosis, and mild mineralization at the cortical-medullary junction of the adrenal glands. A swab of the mucoid material of the right frontal sinus yielded heavy growth of Pasteurella species.
The sinonasal mass was regarded as a plasmacytoma due to the presence of a space-occupying mass composed exclusively of plasma cells. In addition, there was a concurrent infection with Pasteurella spp. that caused a mucopurulent rhinitis and sinusitis and mild suppurative bronchiolitis likely resulting from extension of upper respiratory tract infection to the lungs. The mild depletion of neutrophils in the bone marrow maturation and storage pool developed likely secondary to the sinonasal Pasteurellosis. To confirm the presence of a monoclonal plasma cell proliferation, sections of the sinonasal mass were evaluated by immuno-histochemistry for detection of kappa light chains, lambda light chains, immunoglobulin G (IgG), IgA, and IgM. Within the sinonasal mass, about 60% of the plasma cells showed mild to marked intracytoplasmic immunolabeling for IgG and lambda light chains. Immunostaining for detection of IgA, IgM, and kappa light chains was negative (Fig. 4). Results of immunohistochemistry confirmed the presence of a monoclonal population of plasma cells producing IgG and lambda light chains. Monoclonal proliferation is a feature of plasma cell tumors.
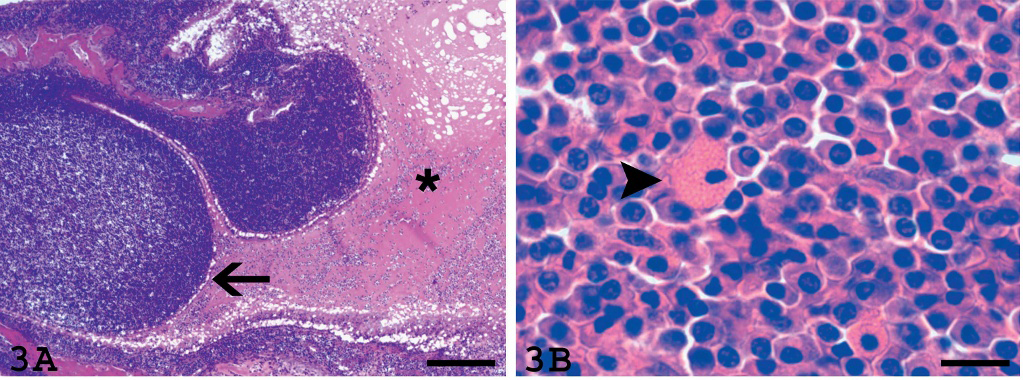
Light microscopy, right nasal cavity, plasmacytoma.

Immunohistochemistry.
This case indicates that plasmacytoma must be included as a differential diagnosis for sinonasal tumors in cats. Reported sinonasal tumors in cats are most frequently squamous cell carcinoma of the planum nasale, adenocarcinoma, lymphoma, and less commonly other tumors (e.g., chrondrosarcoma, olfactory neuroblastoma). 18
The main differential diagnoses for accumulation of well-differentiated plasma cells admixed with Mott cells in tissues are neoplastic and non-neoplastic plasma cell proliferation. In the upper respiratory tract, reactive plasma cell proliferation can be observed in lymphoplas-macytic rhinitis and plasma cell granuloma (synonym: inflammatory pseudotumor). Aggregates of reactive plasma cells are polyclonal and commonly found in tissues together with other inflammatory cells. Plasma cell granulomas form masses composed of plasma cells, other inflammatory cells, and (myo)fibroblasts. 12 In humans, plasma cell granulomas develop at various locations, including the upper respiratory tract. 12 To the authors’ knowledge, plasma cell granulomas have not been described in the respiratory tract of dogs and cats.
The confirmation of plasma cell neoplasia is obtained by demonstration of monoclonality; for this purpose immuno-histochemical detection of immunoglobulin and light chain restriction is commonly used. 9,13,14 There is a physiological predominance of lambda light chains in immunoglobulins of dogs and cats, 1 which is reflected by the predominance of lambda light chain restriction in canine and feline EMPs. 4,9,13 Only a few cases of feline and canine EMPs with kappa light chain expression have been reported. 5,7,13
Although most mucocutaneous plasmacytomas are primary EMP, 14 underlying MM must be ruled out. In animals, the diagnosis of MM is based on the presence of at least 2 of the following 4 criteria: 1) radiographic detection of osteolysis, 2) bone marrow plasmacytosis, 3) monoclonal gammopathy on serum electrophoresis, 4) Bence-Jones (immunoglobulin light chains) proteinuria. 3 Osteolysis is commonly observed with MM in humans 16 and dogs, 3 but it is considered rare in cats with MM. 3,17 Whereas within the bone marrow less than 5% of individualized plasma cells are considered within normal limits, more than 15 to 20% of bone marrow plasma cells are observed with MM. 3 In addition, animals with MM often show systemic signs of disease, such as depression, anorexia, weight loss, hypercalcemia, hyperviscosity syndrome, immunodeficiency, and renal failure. 6,17 Although radiographic evaluation of the skeleton and serum, urine electrophoresis, and antemortem aspiration of bone marrow were not performed in the present case, there was no suspicion of the presence of MM because of the lack of systemic disease, absence of hyperglobulinemia and hypercalcemia, and failure to detect disseminated plasma cell neoplasia or an increased number of plasma cells within the bone marrow histologically. Similar to MMs 2 and EMPs 15 in humans, canine and feline EMPs have been classified in mature, hyaline, cleaved, asynchronous, and blastic types. 4,9,13 The tumors were assigned to a particular class if more than 50% of the neoplastic plasma cells had the cytomorphological features of the respective tumor subtype. 4 In the present case, the tumor was consistent with a mature-type plasmacytoma. The presence of Russell bodies in mature-type plasmacytomas has been previously reported. 4,11 Human plasmacytomas have been graded based on their respective subtype: mature-type plasma cells are of low-grade malignancy, whereas blastic plasmacytomas are regarded as high grade. 2,15 Retrospective studies on canine EMP failed to reveal any significant correlation between plasmacytoma subtypes and proliferation index 13 and prognosis. 4 A similar study on EMP of cats has not been done, probably because of the low incidence of feline EMP.
To the authors’ knowledge, the present communication is the first description of an extramedullary sinonasal plasmacytoma in a cat. Although feline sinonasal plasmacytomas must be regarded as very rare, they should be included in the differential diagnosis for tumors located in the upper respiratory tract of cats.
Acknowledgements. The authors are grateful to Professor Alun Williams (Royal Veterinary College, London, United Kingdom) for critical review of the manuscript and Professor Brian Summers (Royal Veterinary College, London, United Kingdom) for helpful discussion of the case. We thank members of the Department of Pathology and Infectious Diseases at The Royal Veterinary College for the excellent technical support and acknowledge Joy Cramer and Casey Morgan (Cornell University, Ithaca, New York) for performing the light chain immunohistochemistry.