
Abstract
Congenital lobar emphysema (CLE) and tension pneumothorax (TPT) are rarely reported in dogs. A case of CLE of the right middle lung lobe predisposing to air trapping, alveolar hyperinflation, and pleural rupture resulting in fatal spontaneous TPT in a 6-month-old mixed breed dog is described. The unique alteration of “bloat line” was observed in this case in addition to compressive atelectasis of all other lung lobes and lack of negative pressure within the thoracic cavity, signifying markedly elevated intrathoracic pressure. Bronchial cartilage hypoplasia and bronchiectasis were confirmed microscopically, which likely led to abnormal dynamic collapse of bronchi during expiration, consequentially leading to increased intrapulmonary pressure, bullous emphysema, and pleural rupture resulting in TPT. TPT consequent to CLE may therefore be considered one of the potential causes of sudden death in young dogs without overt clinical illness.
Congenital lobar emphysema (CLE) is a well recognized yet uncommon clinical entity in human infants, which has uncommonly been described in dogs. 1–3,6,7,11,14,17 Tension pneumothorax (TPT) is seldom reported in animals and is a rapidly fatal pathologic condition, characterized by the presence of intrapleural air at higher than atmospheric pressure throughout the entire respiratory cycle. 13 The term spontaneous pneumothorax is used to describe the entry of air into the pleural space without underlying traumatic or iatrogenic causes. 12 Here, we describe a case of CLE predisposing to alveolar hyperinflation and rupture, resulting in fatal spontaneous TPT.
A 6-month-old, female mixed breed dog was submitted for necropsy after having been found dead without any premonitory clinical illness. Slight caudal displacement of the abdominal viscera by a convex protrusion of the diaphragm and lack of negative pressure within the thoracic cavity (on puncturing the diaphragm) were observed on necropsy examination. The right middle lung lobe had multifocal slightly raised, variably sized, irregularly round, thin-walled, translucent, gray-pink, deflated emphysematous bullae measuring up to 2 cm in maximal dimension on the pleural surface (Figs. 1, Figs. 2). On sectioning, the bronchi appeared thin-walled and dilated. Bilaterally and diffusely, all the other lung lobes were dark red, shrunken, and collapsed (Fig. 1). On placing mechanically inflated lungs in a bowl of water, an approximately 3 mmdiameter perforation of the visceral pleura was identified on the medial aspect of the right middle lobe. The mucosal surface of the esophagus cranial to the thoracic inlet was diffusely dark red with abrupt blanching of the segment caudal to the thoracic inlet (“bloat line”). 6 Approximately 10 ml of blood was present within the right thoracic cavity. A tentative gross diagnosis of spontaneous tension pneumothorax resulting from rupture of an emphysematous bulla in the right middle lung lobe was made.
Microscopically, the right middle lung lobe was devoid of or had marked reduction in the amount of bronchial cartilage. When cartilage was present, it was rudimentary and arranged in a disorganized fashion (Fig. 3). Affected bronchi were usually dilated, had small, dispersed smooth muscle bundles and were sometimes lined by cuboidal, instead of normal columnar, epithelial cells. Variably sized cystic to bullous spaces (measuring up to 1.4 cm in greatest dimension) formed by the rupture and confluence of several contiguous alveolar septa replaced most of the pulmonary parenchyma and multifocally distended the visceral pleura. There was expansion of the perivascular spaces, visceral pleura, and the alveolar septa by extensive fibrosis and/or granulation tissue. A few lymphocytes, plasma cells and occasional eosinophils were widely scattered or occurred in small clusters throughout the remaining fibrotic alveolar septa. These microscopic features were interpreted to be consistent with congenital bronchial cartilage hypoplasia and postnatal lobar emphysema.

Right thoracic cavity; the middle lung lobe is emphysematous and partially deflated (*); whereas the right cranial (arrow) and caudal lung lobes are completely deflated and collapsed.
Gross and microscopic lesions in the emphysematous right middle lung lobe were in conformity with previous descriptions of CLE in dogs. 1–3 , 6 , 7 , 11 , 14 , 17 Bronchial cartilage aplasia, hypoplasia, or dysplasia has been demonstrated as the underlying cause of CLE in all the prevailing reports of this condition in dogs. To date, CLE has been reported in Pekingese, 14 , 17 Shih Tzu, Jack Russell Terrier 6 and English Springer Spaniel 3 puppies, young Chow Chow, 7 Schipperke 16 and Pomeranian 11 dogs, an adult Pekingese, 2 and 2 senile Afghan hounds. 1 CLE results in respiratory compromise in 2 ways. First, entrapment of air in the affected lung lobe results in enlargement of the lobe causing compression of the remaining lobes. 10 Second, increased expiratory intra-alveolar pressure in the affected lung lobe result in progressive emphysema, 6 , 8 subsequently leading to development of subpleural blebs or bullae that could rupture and discharge air into the pleural space (spontaneous pneumothorax) that is rapidly fatal. In addition to CLE, reported causes of spontaneous pneumothorax in dogs include pulmonary abscesses, neoplasia, dirofilariasis, bacterial pneumonia, bullous emphysema, or pulmonary blebs. 12 Gross or microscopic lesions specific to non-CLE causes of spontaneous pneumothorax were not observed in this dog.
The most likely pathophysiology in this case is as follows. Laxity of the right middle lung lobe bronchus caused by cartilage hypoplasia permitted abnormal dynamic collapse of the bronchus during expiration, while the negative pressure prevailing within the pleural space tended to keep the airway open during inspiration, thereby creating a valvular obstruction. This valvular obstruction led to increased expiratory intra-alveolar pressure, air trapping, hyperinflation, and rupture of alveolar septa and visceral pleura. Because the tissue in the mediastinum is extremely scanty in the dog 5 making it vulnerable to pressure, the pressure gradient could not be maintained between the 2 pleural spaces. 9 This resulted in unilaterally introduced air spreading bilaterally. 15 Lacking therapeutic intervention, the rapidly expanding pleural air mass compressed thoracic structures causing proportional hemodynamic and respiratory compromise that rapidly became life-threatening. Proposed specific mechanisms causing death in cases of TPT, based on experimental evidence in animal models include 1) development of significant hypoxemia before cardiovascular collapse, 13 2) direct mechanical compressive effect on ipsilateral lung lobes causing substantial reduction in pulmonary and bronchial arterial blood flow, 4 as well as air transit and, 3) obstruction of venous return to caval-atrial junction secondary to mediastinal shift with consequent cardiovascular collapse and a precipitous fall in cardiac output. 9
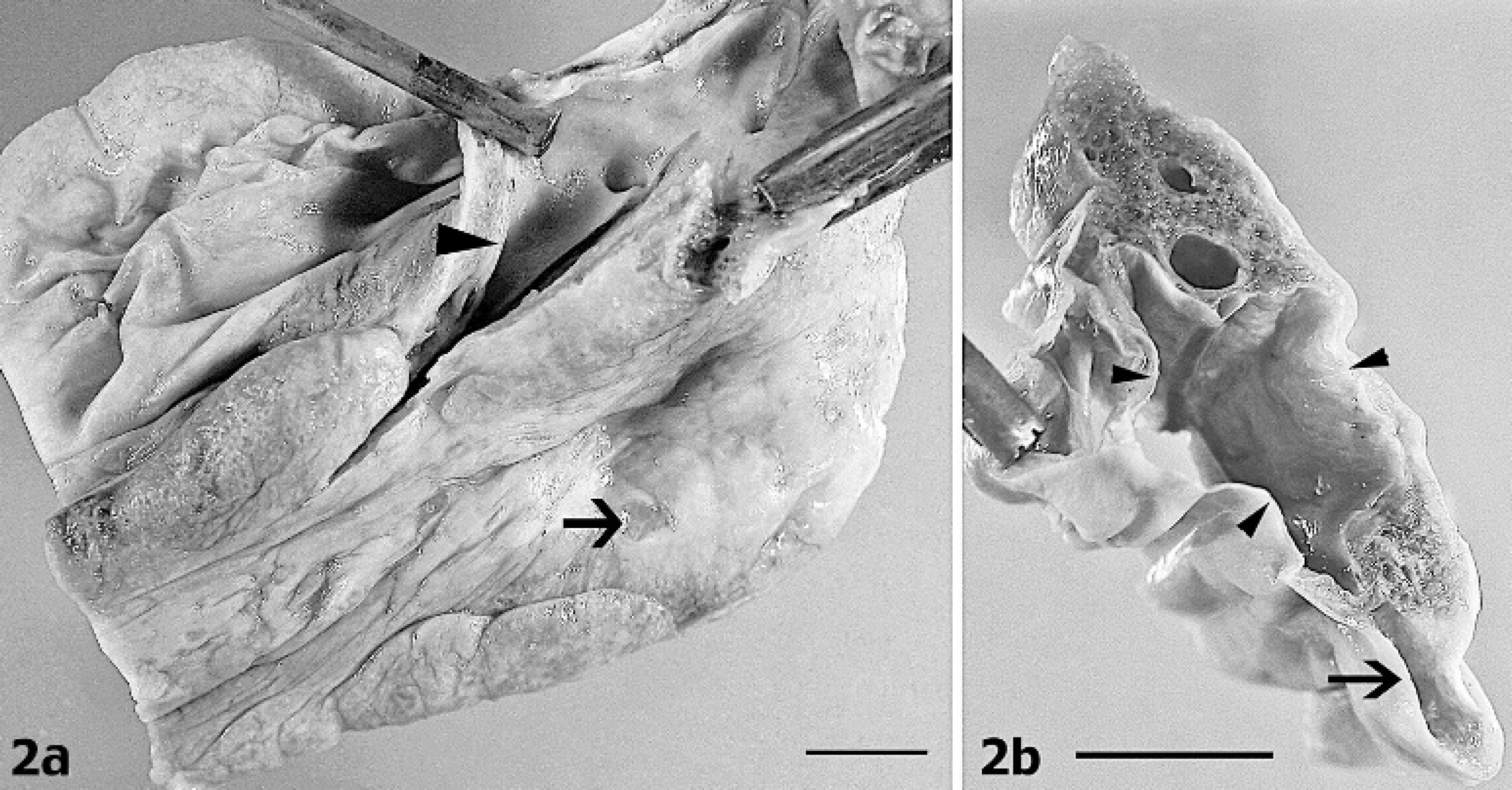
Proximal portion of the right cranial lung lobe (formalin fixed specimen); medial aspect
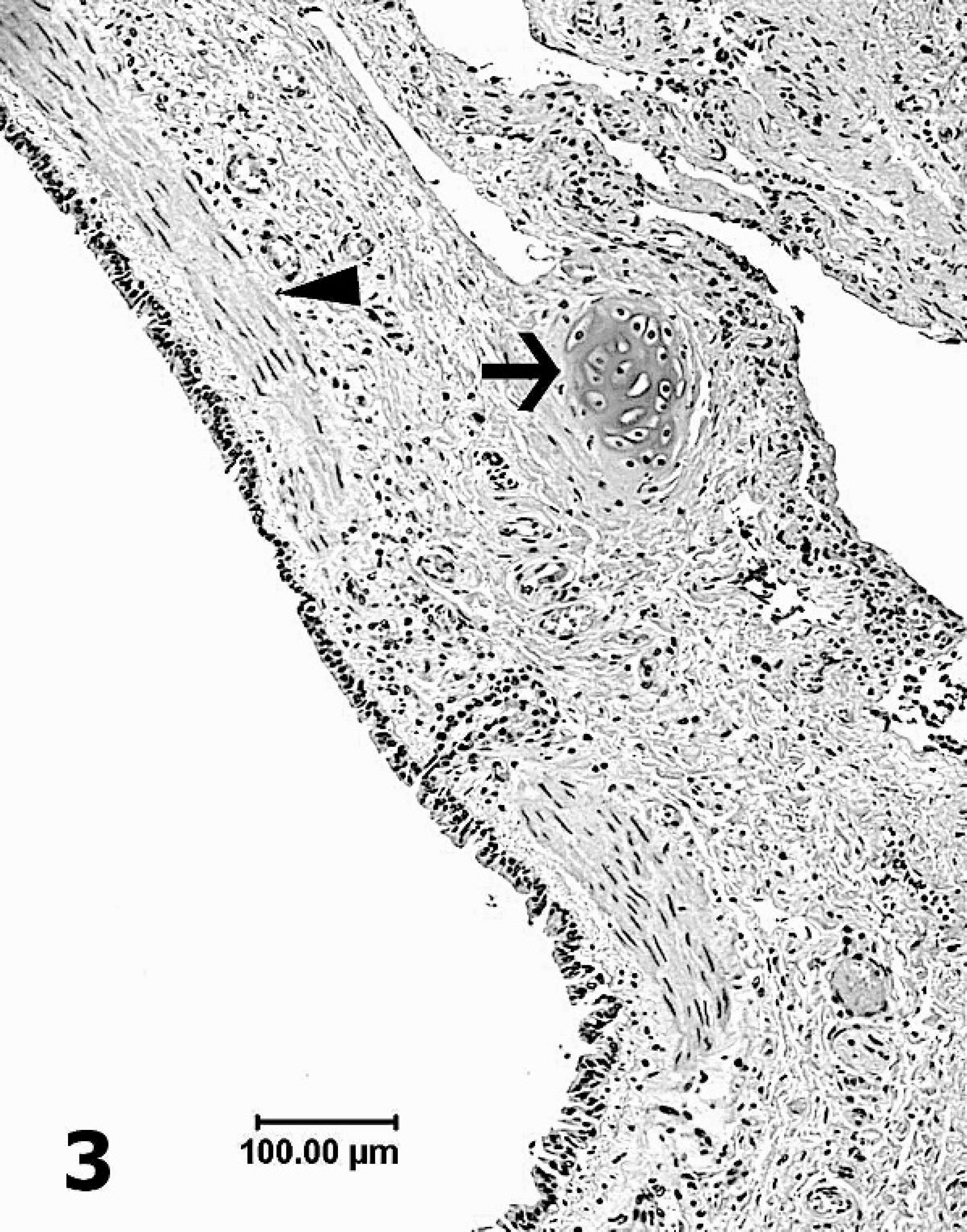
Photomicrograph of a portion of dilated bronchus in cross section showing remnants of cartilage oriented in an irregular fashion (arrow) and thin, dispersed smooth muscle bundles (arrow head).
Congestion of esophagus cranial to the thoracic inlet with abrupt blanching of the caudal portion (similar to “bloat line” in ruminants) observed in this case was likely a consequence of elevated intrathoracic pressure, compression of intrathoracic veins and subsequent venous distention cranial to the thoracic inlet. Bloat or tympany in ruminants is characterized by overdistention of the forestomachs by gases produced during fermentation. Abdominal distention and compression of the diaphragm resulting in significantly elevated intra-abdominal/intrathoracic pressure coupled with reduced venous return to the heart is considered the cause of death in affected animals. Increased intra-abdominal/intrathoracic pressure causes generalized congestion of tissues cranial to the thoracic inlet. A sharp line of demarcation between the blanched distal esophagus and the congested proximal esophagus at the thoracic inlet, often referred to as the “bloat line,” is considered the most reliable postmortem indicator of antemortem bloat in ruminants. 6
To the authors' knowledge, no report prevails in veterinary literature describing rupture of pleural bullae as the cause of fatal spontaneous TPT in any animal species. Thus, CLE and consequent spontaneous TPT should be considered among the differential diagnoses in young dogs with acute onset of respiratory distress or in acute deaths without significant premonitory clinical signs.
Acknowledgements. The authors thank Dr. Ingeborg Langohr for her critical review of this manuscript.