
Abstract
Objective
The northern suburbs of Adelaide, South Australia, are characterised by marked socio-economic disadvantage. Through private practice agreements, psychiatrists employed by this region’s public health service accept referrals from General Practitioners (GPs) to undertake Medicare-Benefits-Scheme Item 291 Psychiatric Assessments (MBS-291s). This study reports the clinical characteristics of people in this region who received an assessment under this initiative.
Method
Data was collected from 169 consumers aged 18–65 years, who attended MBS-291s with one psychiatrist between 2017 and 2021. Data included demographics, diagnoses, comorbidities, management challenges, engagement with other services, and the psychiatrist’s recommendations.
Results
Of 169 consumers, 32% were aged 18–25. Mood (37%) and trauma-related (36%) disorders predominated. Psychiatric comorbidity was common (37% had ≥2 diagnoses). Adverse experiences were reported by 92%, including psychological abuse (60%) and suicidality (51%). Medication recommendations were provided in 99% of cases, alongside psychotherapy (75%), referrals to other services (88%), and lifestyle recommendations (70%).
Conclusions
This study highlights the complex clinical and psychosocial characteristics of those referred for MBS-291s in the northern suburbs of Adelaide, South Australia. We discuss the range of specialist recommendations and comment on the value and sustainability of providing these assessments in the Australian healthcare context.
Keywords
The 2020–2021 National Study of Mental Health and Wellbeing provides a stark perspective on the impact of mental illness (MI) in Australia, with MI being identified as the leading cause of healthy years of life lost due to disability. 1 Over two in five Australians aged 16–85 years (8.6 million) had experienced a MI at some time in their life, with 17% experiencing an Anxiety Disorder, 8% an Affective Disorder, and 3% a Substance Use Disorder in the preceding 12 months. Rates were especially high in young people, with 40% of 16–24 year-olds having a previously diagnosed mental illness which they continued to experience symptoms of in the preceding 12 months.
The annual national expenditure associated with MI in Australia in 2020–21 amounted to ∼$12.2 billion, an annual average increase of 3% since 2017–18. 2 During this period, the largest components of spending were community mental health (MH) care services ($2.8 billion). Locally, in the Adelaide Primary Health Network in 2018 there were 13,177 hospitalisations and 17,981 Emergency Department presentations for MH-related issues, with 33% of those being linked to anxiety-related disorders and 22% to substance-related disorders. 3 There were 54,289 MH Treatment Plans prepared by GPs statewide. 4 Overall, in the 2018–19 calendar year 176,623 people in South Australia accessed MBS-subsidised MH-related services.
Social determinants of health are central to health outcomes and the emergence of MI. 5 Food and housing insecurity, being in a minority group, gender inequality, social exclusion, financial or occupational disadvantage, education or healthcare access, physical illness, adverse experiences, and the quality of relationships have all been shown to significantly impact MH. 6 Social determinants are often entangled in cycles of disadvantage which predispose individuals to MI, creating further barriers to health and livelihood, and perpetuating intergenerational adverse determinants of health. Public policy addressing both social determinants and established MI are crucial to addressing the MH needs of the population. 7
This study was undertaken in the northern metropolitan Adelaide region, a region characterised by socio-economic disadvantage with high incidences of unemployment, developmental and cultural trauma, and many of the social determinants mentioned above. The northern metropolitan Adelaide region is observed to have a Socio-Economic Indexes for Areas (SEIFA) index in the 1st quintile, with 6 of the population health areas in the region being ranked amongst the 10% most disadvantaged population health areas nationally.3,8 The northern region is noted to have an Index of Relative Socio-economic Disadvantage (IRSD) score of 945, compared to the national set average of 1000, and the central and southern region scores of 1024 and 1007, respectively. 8 Correlating with this, compared to the Adelaide Public Health Network (PHN) average rate of psychological distress (13%), the rates in the Local Government Areas (LGAs) of Playford (22%) and Salisbury (18%) were markedly higher. 9 Both LGAs are within the catchment of focus in this study.
Through private practice arrangements with the Community MH Team (CMHT) servicing this region, consultant psychiatrists have been receiving increasing numbers of referrals for MBS-291s. Since their introduction in 2006, MBS-291s have offered GPs and consumers specialist psychiatric advice whilst the GP remains their primary MH treatment provider. 10 These assessments involve a comprehensive interview, diagnostic formulation, and therapeutic advice to inform GPs for the ensuing 12-month period. The MBS-291s currently have set fees of $523.40, with Medicare covering 85% of this cost.
There is little literature reporting on the effectiveness and personal or economic benefit of MBS-291s, nor the characteristics of those referred. More than a decade ago, Williams et al. (2011) found general trends towards an improvement in MH following an MBS-291; however, there is no information about the characteristics of those referred nor the recommendations made. 11 More data is needed to understand whether this approach to psychiatric care best meets the needs of the Australian population in a cost-effective manner.
The aim of this study was to identify the clinical characteristics of consumers referred from the northern metropolitan Adelaide region for MBS-291s in the 2017–21 period. Secondary aims included raising awareness of the unique challenges faced by this cohort and enhancing understanding of the predictors associated with the need for specialist psychiatric input to support GPs.
Methods
Study design
A quantitative approach with a descriptive observational design was employed to investigate the characteristics of consumers referred for MBS-291s by their GPs to a psychiatrist in the Northern CMHT, Adelaide, during the period 2017–2021. Data was collected from the psychiatrist’s reports and included demographics, prior diagnoses and engagement with services, comorbidities, management challenges, and the psychiatrist’s recommendations.
Participants
A total of 169 MBS-291 reports were collected from one consultant psychiatrist’s clinic. Consumers were aged 18 years or older and were living in the Northern Adelaide Local Health Network (NALHN) catchment in South Australia.
Data collection and analysis
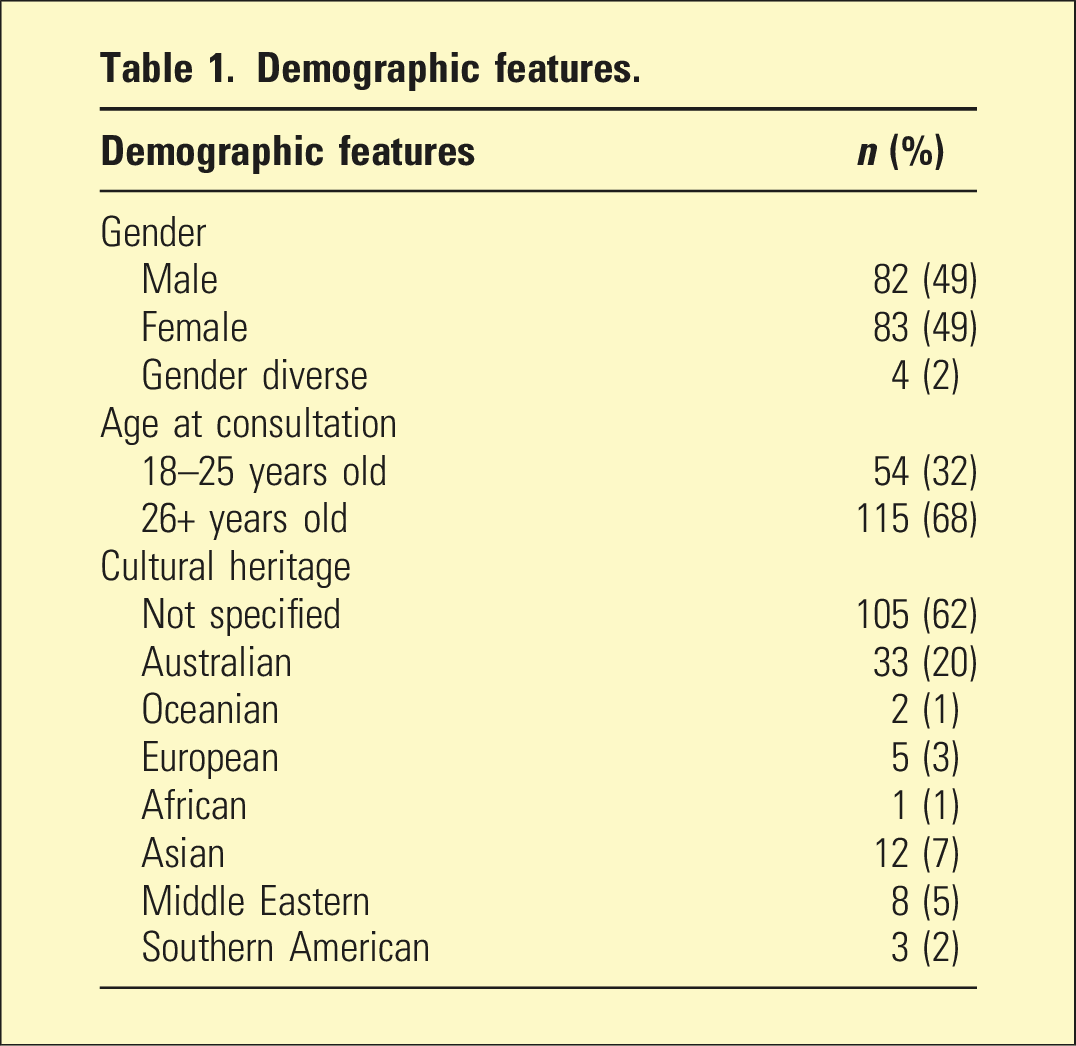
Demographic features.
Psychiatric diagnoses
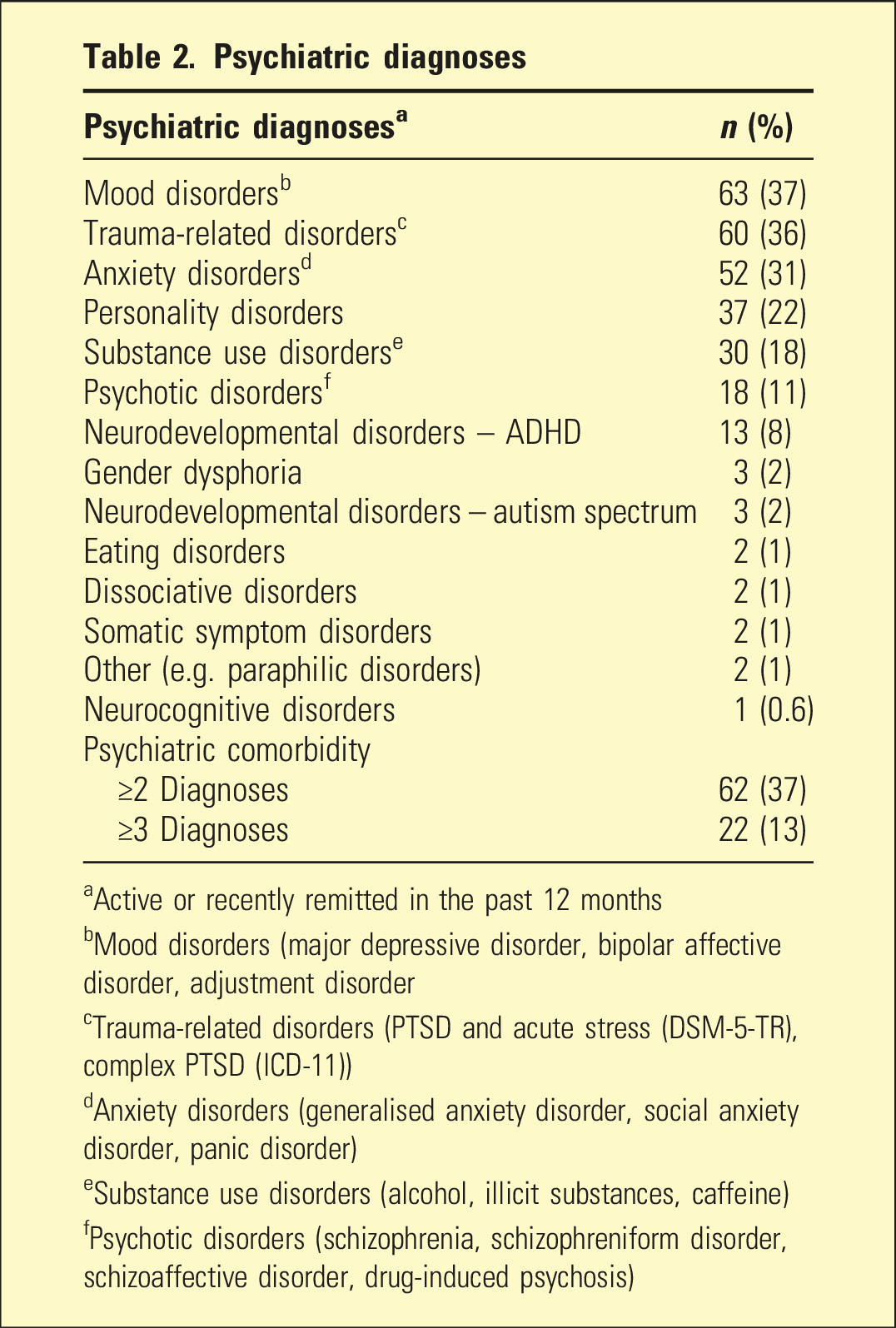
aActive or recently remitted in the past 12 months
bMood disorders (major depressive disorder, bipolar affective disorder, adjustment disorder
cTrauma-related disorders (PTSD and acute stress (DSM-5-TR), complex PTSD (ICD-11))
dAnxiety disorders (generalised anxiety disorder, social anxiety disorder, panic disorder)
eSubstance use disorders (alcohol, illicit substances, caffeine)
fPsychotic disorders (schizophrenia, schizophreniform disorder, schizoaffective disorder, drug-induced psychosis)
Associated Factors
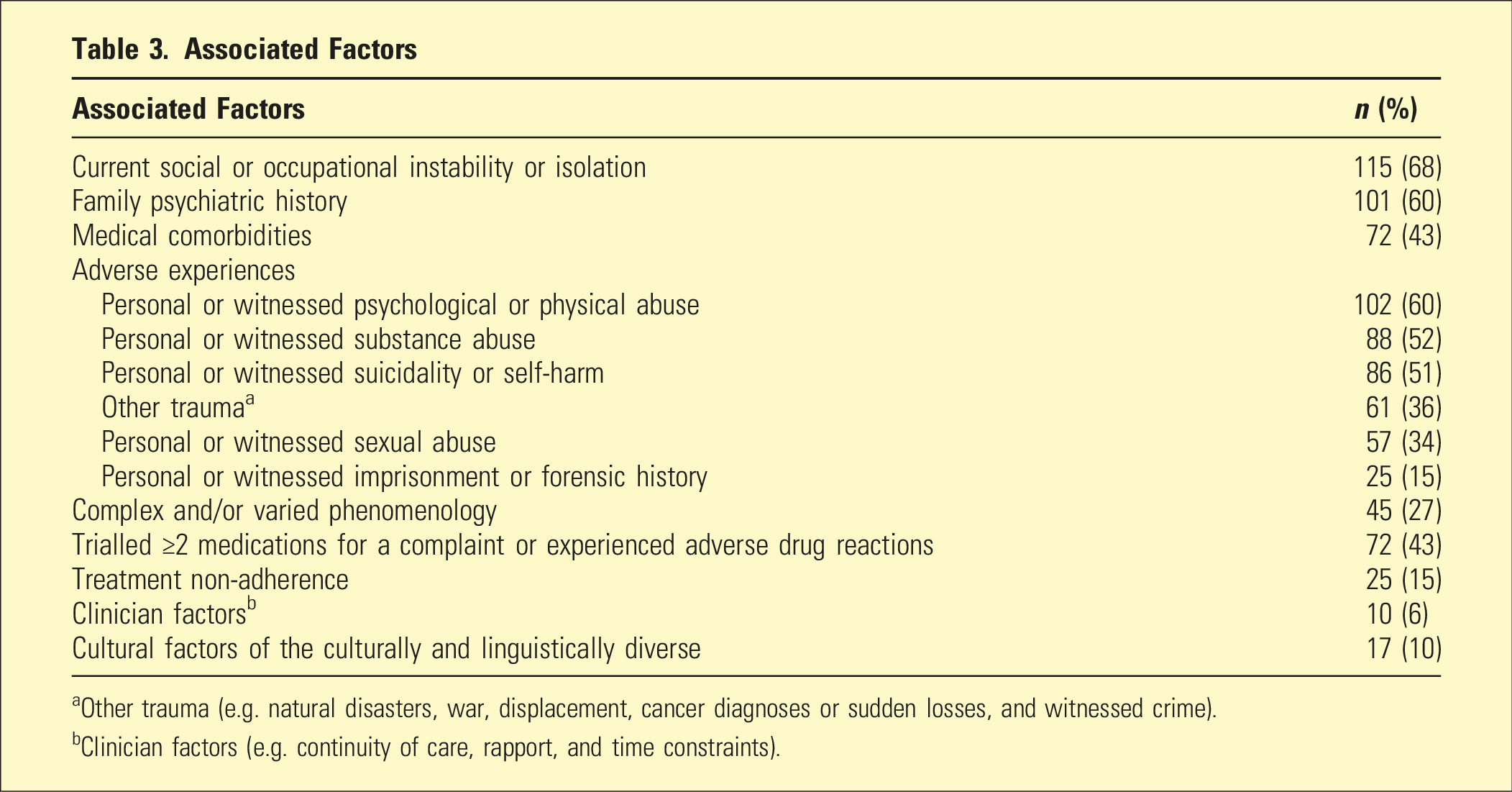
aOther trauma (e.g. natural disasters, war, displacement, cancer diagnoses or sudden losses, and witnessed crime).
bClinician factors (e.g. continuity of care, rapport, and time constraints).
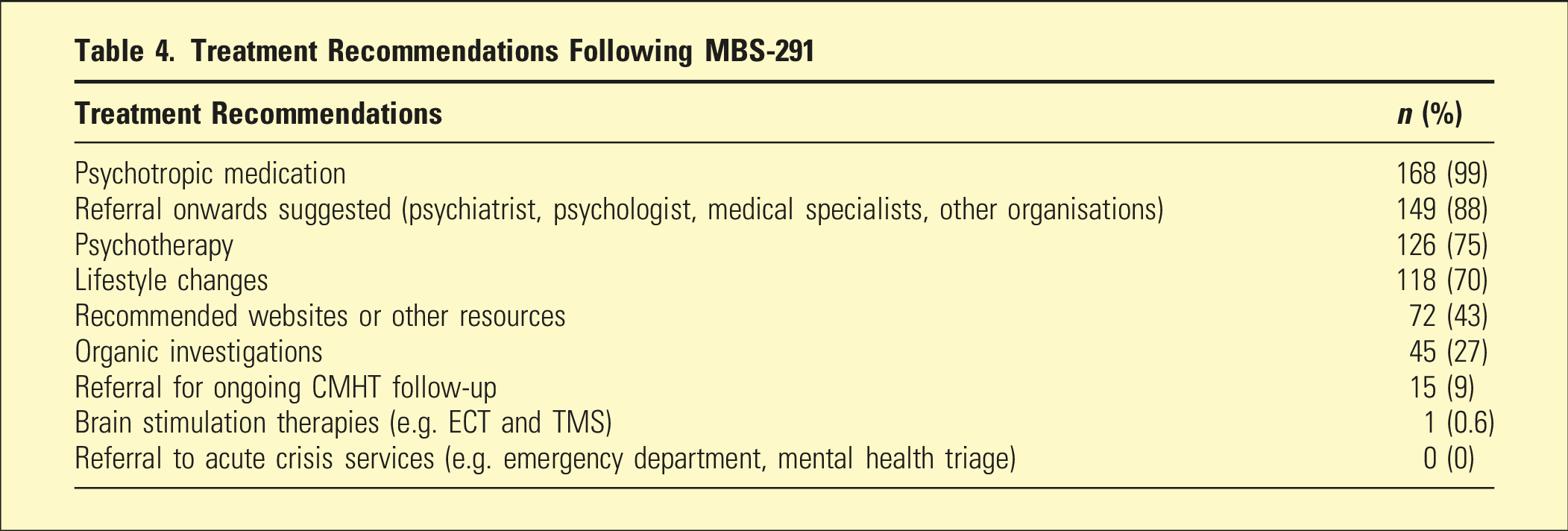
Treatment Recommendations Following MBS-291
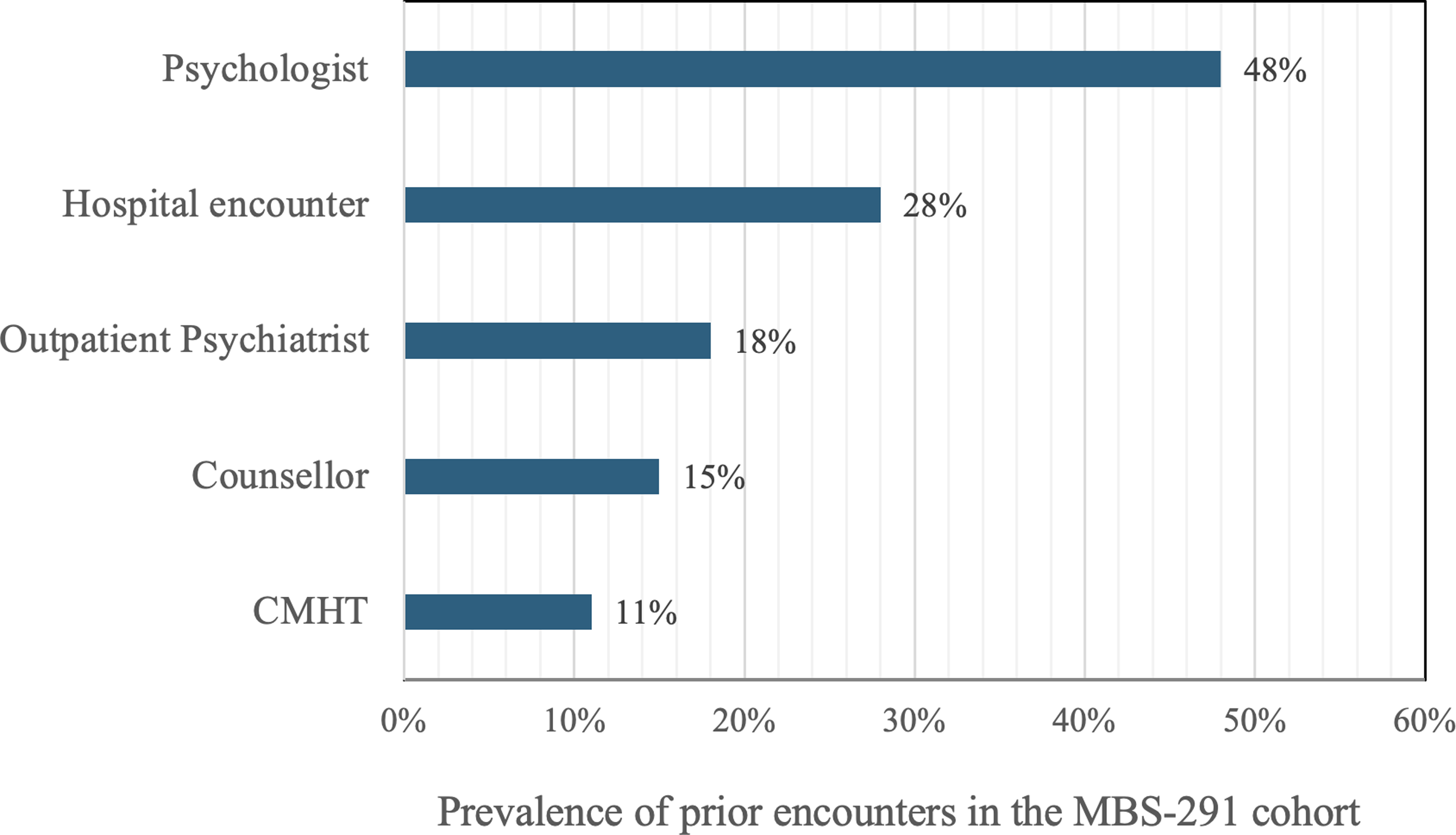
Graph 1: Engagement with other services prior to MBS-291.
Results
To reflect the current structure of adult MH services, consumers were grouped into younger adults, aged 18–25 (32%), and older adults, aged 26+ (68%). Cultural heritage was clearly documented for 38% of participants and was unspecified for most consumers (62%) (Table 1). No consumers were recorded as being of Aboriginal or Torres Strait Islander background.
Diagnoses (active or recently in remission) were observed across 14 categories (Table 2), with a total of 288 diagnoses across the sample. Mood disorders (37%) and trauma-related disorders (36%) were most prevalent with Anxiety Disorders (31%) and Personality Disorders (22%) closely following. Psychiatric comorbidity was common, with ≥2 diagnoses occurring in 37% of the group and ≥3 diagnoses in 13% of the group.
Other complicating associated factors were grouped into 9 domains (Table 3). Notably, 68% of consumers reported current social or occupational instability or isolation, and 60% reported a family psychiatric history. Medical comorbidities were found in 43% of consumers. Adverse experiences were further divided into 6 sub-categories and had been either experienced personally or witnessed by the consumer. The most common adverse experiences were exposure to psychological or physical abuse (60%) and exposure to substance abuse (52%). Personal or witnessed self-harm and suicidality was found in over half of the population (51%). A third (34%) of consumers had witnessed or personally experienced sexual abuse, and 36% had experienced other trauma. Overall, 92% of consumers reported adverse experiences. Complex phenomenology, treatment non-engagement, clinician factors, and barriers related to culturally and linguistically diverse (CALD) backgrounds further complicated many cases. Treatment resistance (defined as trialling ≥2 medications for a condition) and adverse drug reactions were found in 43% of cases.
Consumer engagement with other services prior to the MBS-291 is summarised in Graph 1. Almost half (48%) of the consumers had seen a psychologist at least once prior to assessment and 28% had contact with a hospital for an MH-related concern. In addition, 18% of consumers had seen an outpatient psychiatrist prior to assessment, and 11% had previously engaged with a CMHT.
Recommendations following MBS-291s are summarised in Table 4. Almost all (99%) of assessments included recommendations regarding psychotropic medications, including commencement, cessation, or titration. No consumers were referred to acute crisis services, 15 were recommended for CMHT follow-up, 126 for psychotherapy, and 149 for engagement with other services.
Discussion
This study highlights the complex clinical and psychosocial characteristics of those referred for MBS-291s in the northern metropolitan Adelaide region. As our cohort was specific and risk-selected without prior studies available for direct comparison of findings, the discussion of key observations is contextualised by the Adelaide PHN Needs Assessment Report (2019–2022).
Whilst prevalence rates of diagnoses between this cohort and the general population cannot be compared, the distribution of predominating diagnoses is of interest. In the MBS-291 cohort, 37% had a diagnosed mood disorder, 36% had trauma-related disorders, and 31% had anxiety disorders, compared with the general population where the prevalence of anxiety disorders (17%) was much higher than mood disorders (8%), and PTSD (6%). 1 Interestingly, the Bettering the Evaluation and Care of Health (BEACH) survey identified 12% of GP encounters to involve consumers diagnosed with depression, and 6% with anxiety disorders, with less data available for trauma-related disorders. 14 The high prevalence of trauma-related disorders in the MBS-291 cohort aligns with regional data from the Adelaide PHN Needs Assessment Report pertaining to social disadvantage and psychological distress. 9
The Adverse Childhood Experiences (ACE) study identified a strong link between childhood trauma and negative social and health outcomes and correlated the number of ACEs with the severity of negative outcomes. 15 The categorisation of adverse experiences in this study of MBS-291s was informed by the ACE study, with similar observations regarding the impact of adverse experiences on case complexity. Comparable data from primary care is limited, with the BEACH survey data indicating limited documentation and under-recognition of the role of childhood adversity in case complexity. 14 Given the once-off nature of MBS-291s, these may not capture more insidious adverse experiences, for example, misattunement and attachment disruption.
The impact of personal or witnessed psychological or physical abuse on 60% of consumers in this study cannot be understated. Both psychological and physical abuse culminate in feelings of worthlessness, emotional dysregulation, anxiety, and suicidal ideation, with the AIHW finding abuse and neglect to be associated with anxiety disorders in 27% of cases, suicide and self-inflicted injuries in 26%, and depressive disorders in 20%. 16
National data offer insights into case complexity of the 52% of consumers in this study who reported personal or witnessed substance abuse. The interplay between substance use and MI is dynamic and comorbid, with one often exacerbating or predisposing to the other. 17 In Australia, 46% of those with Substance Use Disorder (SUD) have been found to also meet the criteria for anxiety or affective disorders, and in doing so experience greater combined disease severity and poorer outcomes. 18 Those with comorbid SUDs and other MIs have also been found to have higher mortality rates. 19
Distinct themes in cases of suicide have been previously identified through lived experience surveys and parallel the themes identified in our cohort. 20 Those in our cohort who reported personal or witnessed suicidality or self-harm (51%) were also likely to have encountered ACEs of abuse, trauma, family conflict, bereavement, discrimination, or substance use problems. 20 The interaction of these social determinants and individual factors often generate complex life stressors which when experienced concurrently with psychological distress are often temporally related to suicide attempts. In Australia, psychosocial risk factors are common, being identified in 67% of suicide cases. 21
Current literature points to personal or witnessed sexual abuse as having far-reaching and multilayered consequences. The Australian Longitudinal Study on Women’s Health (ALSWH) offers further insights into the experiences of the 57 consumers in this study who reported personal or witnessed sexual abuse from psychological, physical, and economic perspectives. 22 The ALSWH identified that women with experience of sexual violence (compared to those without) had higher rates of illicit substance use (30%) and a higher likelihood of being diagnosed or treated for depression (39–62%) or anxiety (50%).
Social and occupational instability both provoke and perpetuate cycles of intergenerational disadvantage. Such instability was noted as a significant factor for 68% of our consumers. Food access, housing security, social integration, access to education and healthcare, and physical illness were all relevant factors and are potentially modifiable with infrastructural development. 5
The rates of engagement with other services prior to the MBS-291 were of interest, particularly the identified discrepancy between the rate of hospital encounters (28%) with the rate of outpatient psychiatry follow-up (18%) was of interest. While this data was not captured, it could be postulated that these consumers were linked with private psychologists (50%), counsellors (15%), or a CMHT (11%) in lieu of a psychiatrist on discharge. A possible alternative is that there was discontinuity in specialised care, wherein with the consumers’ GPs became their primary MH support; this is pertinent in considering the need for additional support to GPs.
Interestingly, there was an observed contrast between treatment guidelines and trends in the MBS-291 recommendations. With mood (37%), trauma-related (36%), anxiety (31%), and personality disorders (22%) being of highest prevalence in this group, it was expected that psychotherapeutic recommendations would be provided more frequently than advice on pharmacotherapy, in accordance to current RANZCP management guidelines. 23 However, medication advice was provided to almost all consumers, while only three-fourths of consumers were advised of specific psychotherapy recommendations. There are several possible explanations for this, the most pertinent being that data captured pharmacotherapy advice not only for new medicines but also for deprescribing and dose adjustment of already prescribed psychotropics. This is unsurprising given the BEACH survey findings, whereby medication recommendations in General Practice remained the most common form of management for MH problems (64%), followed by counselling or other clinical treatments (45%). 14 Symptom severity may also drive the demand for pharmacological advice, as may referrer and consumer expectations. Resource unavailability for psychotherapeutic interventions may also drive prescribing trends. Even prior to the COVID-19 pandemic there were notable service demands, particularly in Private Psychology. According to the Australian Association of Psychologists Private Practice survey (2022), there have since been further increases in the demand for their services, first by 77% in 2021, and a further 63% in 2022. Concerningly, by the end of 2022 38% of psychologists were unable to see new clients. 24
This study has several limitations. First, the broader applicability of findings to the Australian population due to the sample selection. Not only was this a small sample size, but the cohort only represented a subset of the population during 2017–2021. There also may not be broad applicability to the local context as the sample did not proportionately capture minority groups who were linked to dedicated services; both First Nations and Gender Diverse populations were underrepresented compared to national rates of engagement with MH services.16,25 The timing of this data collection does not capture the impacts of COVID-19. 26
Additionally, this study considers the assessments of only one psychiatrist in this region, with this therefore also limiting generalisability. While this homogeneity may be a strength, the modest scope of this project should be acknowledged. Given this was a retrospective review of reports following comprehensive assessments, in-depth analysis is limited when compared to the use of transcripts. In future research, it would be worthwhile to delineate the impacts of personal versus witnessed adverse experiences.
With limited studies on MBS-291s to date, a major strength of this study has been its novel contributions of local and national relevance in a crucial time where MBS items are being closely evaluated. 11 While the study provides insights into the NALHN catchment, the findings speak to a wider narrative of the breadth and impact of social determinants and adverse experiences in health, and in turn the increase in demands on GPs and CMHTs.
Further research to compare this study’s findings with another LHN catchment may offer further insights into regional factors contributing to case complexity. Further research into MBS-291s with data from the COVID-19 period, and subsequent to this, is also recommended. 26 Larger-scale studies are also needed of MBS-291s in the Youth and the Older Persons Mental Health Services, and for Aboriginal or Torres Strait Islander People and Gender Diverse groups.
This study prompts a multitude of enquiries around the value of MBS-291s to GPs, consumers, and the broader healthcare system. It would be worthwhile exploring these questions using surveys and questionnaires to explore GP, consumer, and psychiatrist views. Other stakeholders would also have valuable insights, notably Non-Government Organisations, Peer Support Workers, Psychologists, and the Specialist Training Colleges for General Practice and Psychiatry. Further enquiry will also inform the need for more GP education and support, and the development of primary prevention programs focussing on the social determinants of health.27,28
Conclusion
This study explored the characteristics of consumers referred by GPs for MBS-291s in a defined catchment region (northern metropolitan Adelaide, South Australia). Consumers displayed high incidences of trauma and were disproportionately affected by psychiatric morbidity compared to the general population. Trends in recommendations were also observed. Further research is needed into understanding the unique challenges of other LHNs as well as the perspectives of consumers, GPs, and psychiatrists, to more effectively utilise MBS-291s when supporting vulnerable consumers.
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethical approval was obtained from theCentral Adelaide Local Health Network Human Research Ethics Committee (HREC/18/CALHN/347) and the Northern Adelaide Local Health Network Human Research Ethics Committee (SSA/18/NALHN/159).
Data Availability Statement
The raw data set is available upon request.