
Abstract
Aim: The aim of the study was to evaluate the pharmacological treatment of migraine patients by general practitioners before referral to a neurologist. First, was the pharmacological treatment in accordance with the Dutch College of General Practitioners headache guideline? Second, which migraine characteristics were associated with receiving migraine-specific medication?
Methods: Migraine patients (age ≥18 years) who visited the neurology outpatient clinic for the first time were included. Migraine characteristics and pharmacological status were collected retrospectively for each patient from the general practitioner’s referral letter, hospital record and a headache characteristics questionnaire.
Results: A total of 420 migraine patients were included. Only 18.3% of the patients with two or more migraine attacks per month were using prophylactic medication. Furthermore, only 11.7% of patients with symptoms of nausea and/or vomiting were using anti-emetic medication. More than half of patients (51.7%) were using triptans and were likely to have typical migraine symptoms and a long history of migraine.
Conclusions: Migraine prophylactic medication and anti-emetics are underutilized in the primary care setting for migraine patients in the Netherlands, when compared to the general practitioners guideline. It is important to enhance the knowledge of general practitioners regarding the diagnosis of migraine, and to increase awareness of the headache guideline.
Introduction
Migraine is a common, chronic, neurovascular disorder characterized by headache attacks with or without aura (1). The burden of migraine is high, associated with deteriorated quality of life, lost productivity and great impact on family and social life (2,3).
Despite advances in both acute and prophylactic treatment, community-based studies in several countries have demonstrated that a minority of migraine patients use specific anti-migraine drugs (4,5). There are several reasons why migraine patients do not receive adequate treatment; these can be both patient- and physician-related.
The general practitioner plays an important role in the management of migraine (6). A satisfactory consultation with the general practitioner is important to ensure subsequent effective treatment of migraine (7). However, little is known about how general practitioners actually treat their migraine patients and if the pharmacological treatment is adequate. Studies comparing anti-migraine medication prescription by general practitioners and neurologists demonstrated an increase in the use of triptans and prophylactic treatment after patient consultation with a neurologist (8,9). However, these studies do not tell us how many migraine patients really do need medical treatment.
Various guidelines concerning the treatment of migraine have been established in order to improve the care of migraine patients. In the Netherlands, the Dutch College of General Practitioners provides a clear diagnostic and therapeutic standard for the care of migraine patients (10). To our knowledge, no evaluations have been published on the extent to which guidelines for treatment of migraine are actually used.
The overall aim of this study was to evaluate the pharmacological treatment of migraine patients by general practitioners, before referral to a neurologist. More specifically, the following questions were addressed: (1) to what extent is the pharmacological treatment of migraine patients in accordance with the Dutch College of General Practitioners headache guideline and (2) are there certain migraine or patient characteristics associated with receiving migraine-specific medication from a general practitioner?
Methods
Study setting and patient selection
This study was conducted at a general hospital in the Netherlands. We selected all patients who were registered as having a headache diagnosis according to the DTC-registration (diagnostic-treatment-combination) database in a period of 1.5 years. The DTC was introduced in the Netherlands in 2003, and it functions as a defrayment system for intramural curative and somatic health care. All patients with headache were referred by a general practitioner to the outpatient clinic.
Screening of the hospital records was conducted to identify patients who met the following criteria:
Patients had to be naive patients who visited the neurology outpatient clinic for the first time because of headache. Consultation took place at the outpatient clinic, excluding patients who were seen on the emergency ward or admitted to the hospital for migraine or another reason. Patients had to have a migraine diagnosis according to the criteria of the International Classification of Headache Disorders, second edition (ICHD-II) (i.e. ICHD-II 1.1, 1.2.1, 1.2.2, 1.2.6, 1.6). Patients had to be 18 years of age or older at the time of consultation.
Data collection
Data were collected retrospectively. The hospital records of all patients who met the previously described criteria were examined. Data concerning patient pharmacological status were retrieved from the hospital record and the general practitioner’s referral letter. Data collection was performed by RZ. The type of migraine, according to the ICHD-II criteria, was recorded and checked by a neurologist (JSPB) specializing in headache disorders. Patients visiting the specialized headache outpatient clinic had completed a self-administered questionnaire that included questions about headache characteristics, accompanying symptoms such as photo- and phonophobia, nausea, vomiting, presence of aura symptoms and demographic characteristics. In order to obtain information from patients visiting the regular neurology outpatient clinic, a shortened questionnaire was send to patients who had visited the regular neurology outpatient clinic with migraine. To reach the remaining non-responders, at least two attempts were made by telephone to obtain the missing information.
Definitions/classifications
Migraine diagnosis was made according to the ICHD-II (11). Besides migraine, other types of primary headaches were recorded. If patients had more than one type of headache besides migraine headache, migraine was considered their primary headache if this was the main reason for consultation with a neurologist. To determine if medication overuse was present, the revised criteria for medication overuse (ICHD-II 8.2) were used.
Dutch College of General Practitioners headache guideline
In the Netherlands, the Dutch College of General Practitioners provides general practitioners with clear diagnostic and therapeutic guidelines for different diseases and disorders. In 2004, the most recent headache guideline was published (10). The headache guideline provides diagnostic criteria based on the ICHD-II and therapeutic guidelines for the different primary headache disorders. Migraine treatment is divided into acute treatment of migraine headache and prophylactic treatment (see Figure 1).
Schematic representation of the pharmacological treatment of migraine patients as recommended in the Dutch College of General Practitioners headache guideline.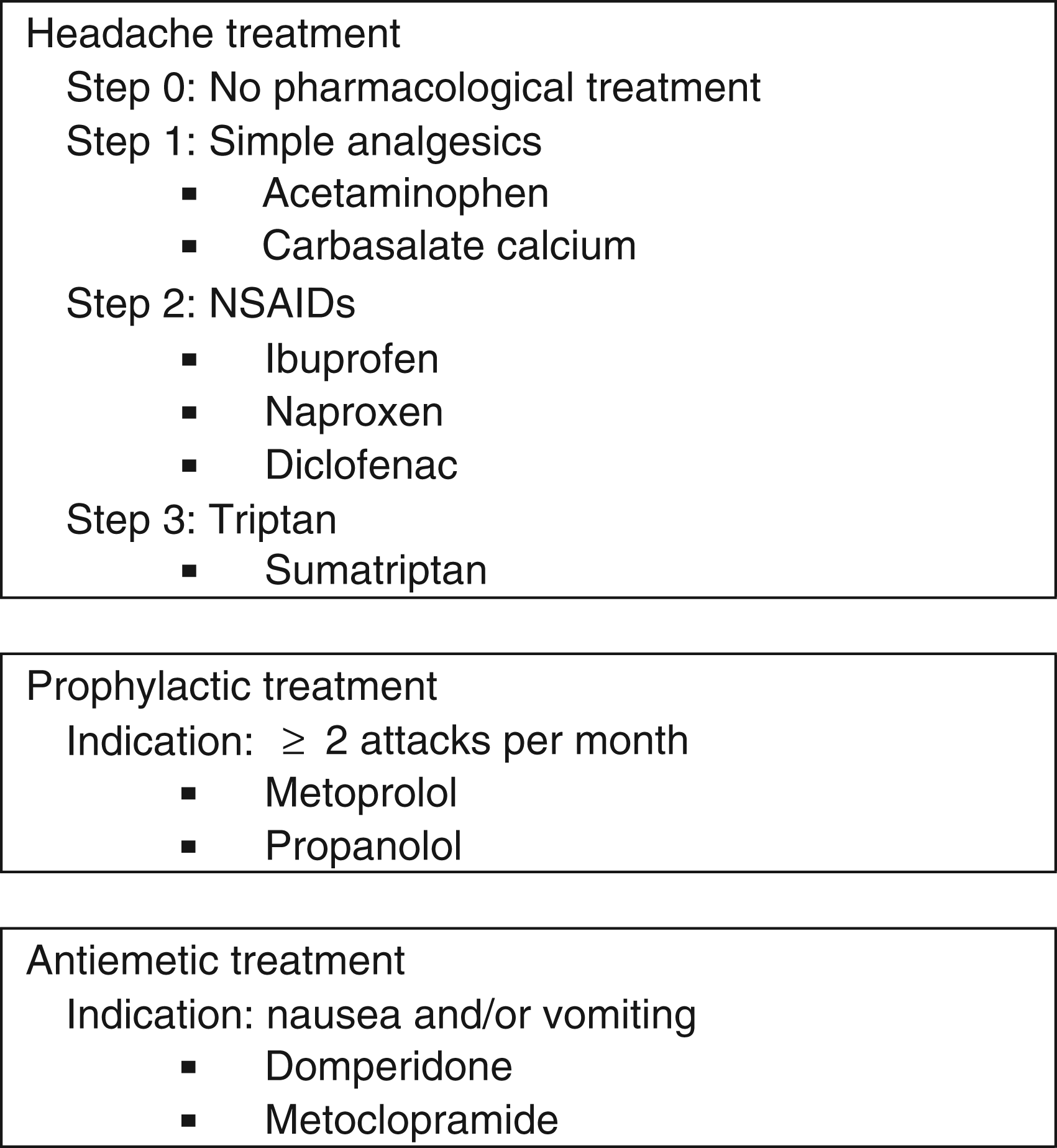
Acute headache treatment is based on stepped care. In step 1, a simple analgesic is recommended; in step 2, a non-steroidal anti-inflammatory drug (NSAID); and in step 3, a triptan. Anti-emetic medication is advised when nausea and/or vomiting is reported by the patient. Migraine prophylactic treatment is indicated when a patient has two or more migraine attacks per month (see Figure 1).
Statistical analysis
Baseline characteristics were reported as mean ± SD (standard deviation) or absolute numbers with percentages. In order to assess which patient and headache characteristics were associated with migraine-specific treatment at the time of consultation, we compared patient and headache characteristic between groups with and without triptan use, with and without prophylactic medication use and with and without anti-emetic medication use. Differences in means were tested with independent samples t-tests. Differences in proportions were tested using χ2-tests. Data analyses were performed using SPSS 17.0 (SPSS Inc., IBM, USA). P values <0.05 were considered statistically significant.
Results
Study population
Baseline characteristics, headache diagnosis according to ICHD-II diagnostic classification (11) and migraine characteristics (n = 420).

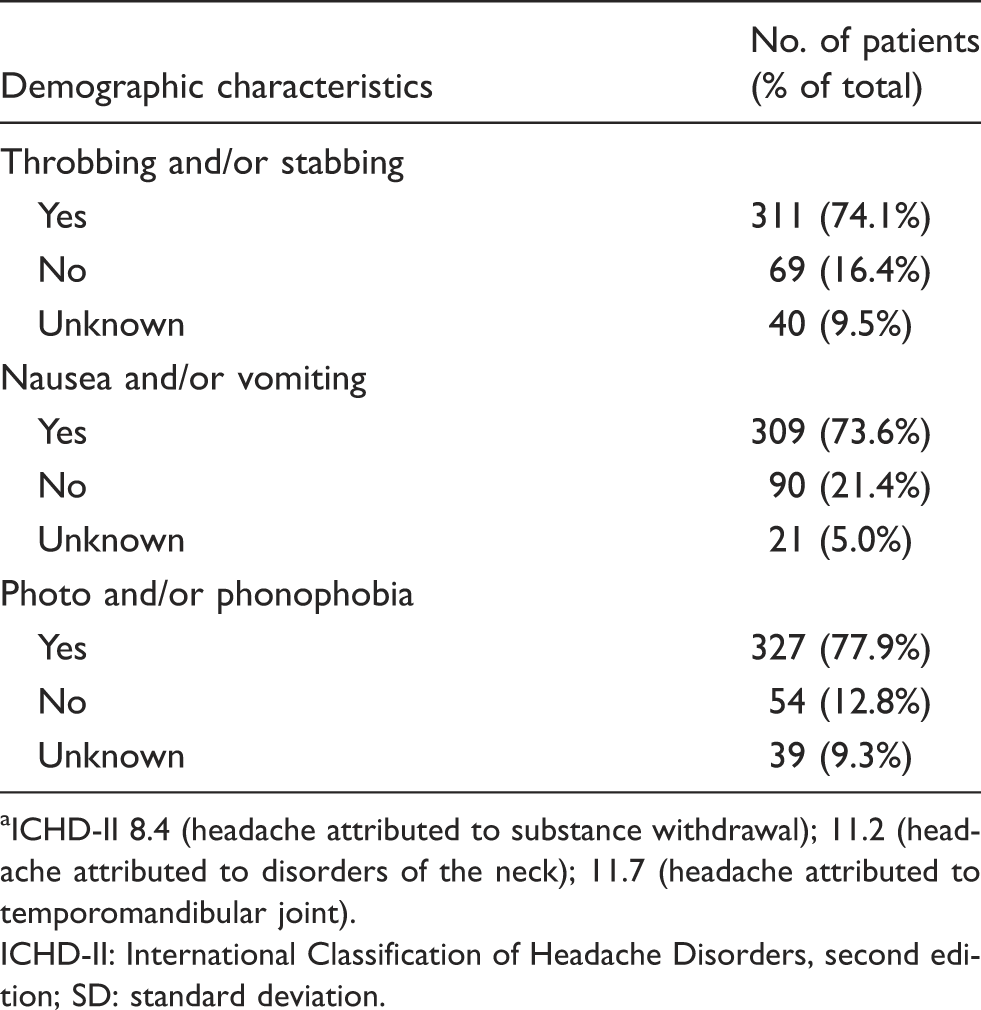
ICHD-II 8.4 (headache attributed to substance withdrawal); 11.2 (headache attributed to disorders of the neck); 11.7 (headache attributed to temporomandibular joint).
ICHD-II: International Classification of Headache Disorders, second edition; SD: standard deviation.
Migraine treatment and the general practitioners headache guideline
Treatment of migraine patients at the time of consultation with a neurologist (present) and present and pharmacological history combined (present and history), compared to the general practitioners headache guideline. a

p values in bold indicate significant differences (p < 0.05) using a χ2 test.
Percentage of patients with an indication for prophylactic or anti-emetic treatment, respectively.
Percentage of patients without an indication for prophylactic or anti-emetic treatment, respectively.
Over-the-counter analgesic use was not well documented in the referral letter or the hospital record in 68 cases. At least 92.3% of patients had at any time used non-opioid analgesics to treat their migraine attack. Only a few patients reported the use of opioids (n = 27; 6.4%), of which the majority were combination preparations like acetaminophen with codeine (n = 19; 4,5%) with only a small number of single opioids (n = 4; 1.0%). Ergotamines are hardly prescribed anymore in the Netherlands; only one patient had recently used ergotamines to treat a migraine attack, whereas 20 patients (4.8%) had used ergotamines at any time in their medical history.
A small number of patients had at any time in their medical history used anti-emetic medication (n = 58), and an even smaller number of patients still used anti-emetic medication at the moment of consultation with a neurologist (n = 38).
The majority of patients (n = 309) reported nausea or vomiting during the migraine attacks; of these patients, 36 were using anti-emetic treatment. An additional 18 patients with nausea or vomiting had been using anti-emetics in the past.
Seventy-seven patients were using migraine prophylactic medication at the time of consultation. A large number of patients (n = 81) previously used prophylactic medication but stopped using them. Of the patients still using prophylactic medication at the time of consultation, 27.3% had previously tried another prophylactic drug. A frequency of two or more migraine attacks per month was reported by 295 patients; 54 of these patients were using prophylactic treatment at the time of consultation with a neurologist.
Migraine characteristics and association with medication use
Baseline (migraine) characteristics of patients and the association with medication use (triptan, prophylactic medication and anti-emetics) at the time of consultation with a neurologist (n = 420). a

p values in bold indicate significant differences (p < 0.05), using independent-sample t-test and χ2 appropriately; p values uncorrected for multiple testing.
Prophylactic medication was less likely to be prescribed to patients with probable migraine. The number of migraine years was associated with prophylactic medication use; patients with a long migraine history were more likely to use prophylactic medication. No other specific migraine characteristics, not even migraine frequency, were associated with prescription of prophylactic medication by a general practitioner.
Prescription of anti-emetic medication was only associated with nausea and/or vomiting and not with any other migraine characteristics.
Discussion
The current retrospective study reports on the pharmacological treatment by general practitioners of 420 patients with migraine. We compared the pharmacological status of these patients to the advice given in the general practitioners guideline for headache diagnosis and treatment. Evident from our study is an underuse of prophylactic and anti-emetic treatment when compared with the general practitioners headache guideline.
The proportion of patients who were using preventive therapy at the moment of consultation with a neurologist was 18.3%. In the general practitioners headache guideline, a frequency of two or more migraine attacks per month is considered an indication for migraine prophylactic treatment. At the time of consultation, 73.6% of patients met the criteria for starting migraine prophylactic medication. However, only 18.3% of these patients were actually using prophylactic medication. These strict criteria are admittedly somewhat arbitrary, because in practice the decision to prescribe preventive medication depends on many factors other than migraine frequency alone. There are several explanations as to why patients with a migraine frequency of two or more attacks did not use prophylactic treatment after visiting the general practitioner; it could be that the patients were afraid of the side effects or that the migraine did not influence the daily activities of the patient because of very effective acute treatment. However, prophylactic drugs were more frequently prescribed to the subgroup of triptan users, indicating that a triptan alone possibly was not effective enough in a subgroup of migraine patients. Unfortunately, we have no information about patient satisfaction or treatment efficacy.
Use of preventive treatment clearly varies per country. In a French-population-based study, only 6% of migraine patients with a migraine frequency of two or more attacks per month were using prophylactic treatment (12). In the American Migraine Prevalence and Prevention (AMPP) study, a panel of experts advised or would consider preventive treatment in 38.8% of studied patients. However, in the AMPP only 12% of the patients actually used preventive medication (2). Patients in our clinically based study had, on average, a higher frequency of migraine attacks compared to those in the AMPP, which may explain the higher rate of prophylactic users in our study. In the AMPP, patients using preventive treatment were more likely to be female, older in age, have unilateral and extremely severe pain, associated symptoms (e.g. phonophobia), migraine with aura, a high frequency of attacks and a lower quality of life (high disability) (13). In our population, the use of prophylactic treatment was only associated with having migraines for many years and migraine with or without aura.
A study on migraine prophylactic treatment in the Netherlands between 1994 and 1998 found that the overall incidence of initiation of migraine prophylactic therapy following the use of abortive migraine drugs was 6.0% per year and fell considerably during the five-year study period. Only 12% of the study population had commenced prophylactic therapy during the five-year observation period (14). In another publication from this same study, the investigators demonstrated that patients commencing migraine prophylactic treatment for the first time had used these drugs for a relatively short period of time. More than half of the study population had discontinued migraine prophylaxis within three months after commencing this form of treatment. Approximately 15% had continued treatment for more than two years (15). This phenomenon is also seen in our study: more than half of the patients who had used prophylactic medications stopped using them.
Anti-emetic drugs can relieve complaints of nausea or vomiting and can also provide significant reduction in migraine pain (16). Anti-emetic treatment was used in only 17% of the 309 patients with nausea or vomiting. Patients using anti-emetic treatment were, as to be expected, more likely to have nausea or vomiting. In a Canadian study, 606 migraine patients referred to neurologists specializing in headache showed that only 7.6% used anti-emetic drugs before referral, and almost 19% after consultation. However, the study did not clearly state which patients had an indication for treatment with anti-emetics (8). It seems that nausea and vomiting in migraine patients are undertreated phenomena, although guidelines recommend the prescription of anti-emetics.
In contrast to the underprescription of anti-emetics, triptans were prescribed in 51.7% of the patients by the general practitioner, which is a rather high percentage when compared to similar studies in other countries. An Italian study reported that only 9.1% of patients were using triptans prescribed by their general practitioners (9), and a population-based survey in France revealed that 8% of migraine patients treated their attacks with triptans (12). A Dutch study collecting data from community pharmacy records on triptan and ergotamine use found that 13% of migraine patients were treated with migraine-specific medication (4). A possible explanation for the large number of patients using triptans in our study are that triptans are covered by health insurance in the Netherlands, and that patients in our clinic-based cohort had a higher frequency of migraine.
A number of factors may explain why migraine patients do not receive adequate preventive and anti-emetic treatment. It is well established that lack of consultation for headache is a major contributing factor (5,7). But even if migraineurs seek medical care, they often do not receive the appropriate diagnosis by a physician (17). It may be that it is difficult for a general practitioner to diagnose migraine; especially if the patients are lacking some of the typical migraine symptoms, for example, unilateral headache, or if there is a concomitant headache disorder present (18). In our study, concomitant headache disorders had no direct influence on the patient’s getting migraine-specific treatment. However, our study showed that patients with the typical migraine symptoms were more likely to receive migraine-specific treatment. Another physician-related explanation may be that the general practitioners have no knowledge of the existence of the headache guideline. Our study shows that only half of the patients reach the last step of recommended stepwise care for acute migraine treatment and a small number of patients with an indication for prophylactic or anti-emetic treatment are receiving such treatment.
Some limitations of our study have to be addressed. The patients studied were from a selected population of migraine patients who were referred to the neurology outpatient clinic. These patients are more likely to have moderate-to-severe migraine with a high migraine frequency, and may be difficult to treat for general practitioners. Furthermore, due to the retrospective study design, information may be incomplete—in particular, analgesic medication bought over the counter is likely to be underreported. In our study, we only investigated the Dutch general practitioners headache guideline; the guidelines for treating migraine can differ from country to country.
To summarize, our study shows that the general practitioners headache guideline is not well implemented as regards migraine care, especially regarding the prescription of anti-emetic and prophylactic treatment. To improve the treatment of migraine by general practitioners, it is important to enhance their knowledge regarding diagnosing migraine and to emphasize that patients with migraine, but lacking typical migraine symptoms, also deserve adequate treatment. Episodic migraine, and even moreso, chronic migraine, are associated with a decreased quality of life (19). Therefore, increasing awareness of the existence of headache guideline among general practitioners is essential for adequate treatment. This will enhance the quality of life of migraine patients, and will, we would hope, reduce unnecessary burden of illness of migraine patients who are currently undertreated.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflicts of interest
The authors report no conflict of interest.