
Abstract
Objective
To investigate the role of telehealth in youth psychiatry during and after the pandemic in Australia.
Methods
We analysed Medicare Benefits Schedule (MBS) item number data for psychiatry services provided to patients aged 0–24 years, from 2017 to 2022. We analysed total services (in-person and telehealth) from 2017 to 2022, determining provision before and during the pandemic. We also analysed changes to use of each modality during the pandemic. Finally, we calculated the use of each modality in 2022, when COVID-19 restrictions had eased.
Results
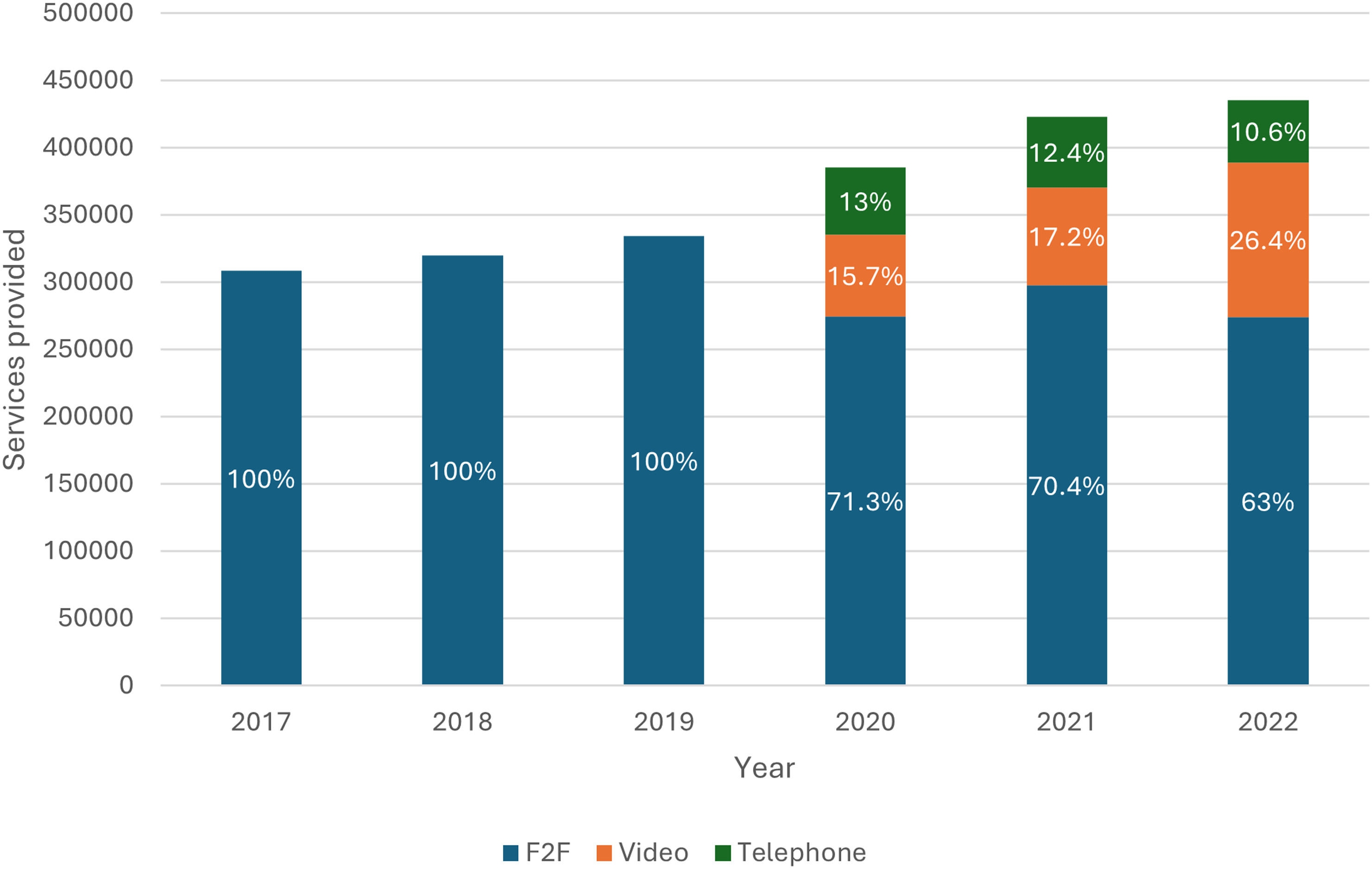
Youth psychiatry service provision steadily increased prior to the pandemic (2017–2019). Larger increases were seen during the pandemic, with 15.3% increase between 2019 and 2020, and 9.7% increase between 2020 and 2021. After the introduction of telepsychiatry MBS item numbers, in-person services decreased from 71.3% to 63% between 2020 and 2022. Video-telepsychiatry increased from 15.7% to 26.4% between 2020 and 2022, and telephone-telepsychiatry decreased from 13% to 10.6%. In 2022, most consultations were in-person, but video-telepsychiatry was higher than ever despite fewer COVID-19 restrictions.
Conclusions
Telepsychiatry was well-received by young people during the pandemic and should remain an option to improve access to youth psychiatry in post-pandemic times.
In March 2020, new Medicare Benefits Schedule (MBS) telehealth items were introduced to facilitate private psychiatric service provision during the COVID-19 pandemic and could be provided via videoconference or telephone. Video-telehealth items were previously available in rural and remote areas, but the new items are now accessible to both rural and metropolitan patients. In January 2022, pre-pandemic telehealth items were removed, and most telephone-telehealth items were subsequently ceased in July, but video-telehealth items introduced during the pandemic were retained. 1
Although research has shown a positive uptake of telehealth psychiatry in Australia,2–4 there is less information on the adoption of telepsychiatry by young people (aged 0–24 years), despite declining mental health over the previous two decades. This demographic is of interest as the COVID-19 pandemic has left young people particularly vulnerable to psychological distress, due to social isolation, loss of structured activities and peer relationships and a lack of control over their situations.5–10
Missed appointments and high dropout rates undermine youth assessments and therapy, partly due to practical consideration such as travel to appointments. 11 Research shows that telehealth has a higher attendance rate and is more accessible to those unable to commute or miss school and work to attend consultations.3,12 Telehealth has been found to be as effective as in-person mental health services.12,13 Telehealth could thus be an important method of increasing accessibility and meeting the high demands for youth psychiatric services. While young people are often comfortable with digital platforms, concerns about privacy and access to internet and technology can be barriers to accessing telehealth services. 14
We analysed how the pandemic and new telehealth MBS item numbers have changed treatment modalities usage in youth psychiatry from 2020 to 2022. We also investigated the role of telehealth modalities in 2022, in the context of improving pandemic conditions, that is, fewer lockdowns and shorter isolation periods.
Methods
We extracted annual MBS-Item Service data from the Services Australia Medicare Item by Patient Demographic Reports (https://medicarestatistics.humanservices.gov.au/statistics/mbs_item.jsp) for psychiatry practice office-based in-person consultations from January 2017 to December 2022 and equivalent video- and telephone-telehealth consultations from March 2020 to December 2022. In a purpose-built Excel spreadsheet, we combined the data for male and female patients aged 0–24 years and analysed the data for totals and percentages. Although data for telehealth items are separated into the age groups 0–4, 5–14 and 15–24 years, in-person items are only available in a single age group of 0–24 years. In order to compare telehealth and in-person items, we chose to combine the telehealth data and analyse the 0–24 years age group as a whole. In doing so, our analysis combines Child and Adolescent Mental Health Services (CAMHS) with the more traditional definition of youth psychiatry services provided to 12–25 years. To analyse the change in total services provided annually from 2017 to 2022, we compared data from each year to the previous year and calculated percentage change. To analyse the change in in-person consultations at the onset and throughout the pandemic, we used 2019 data as a baseline comparator, as this was the closest proximate year before the pandemic. To analyse the change in video- and telephone-telehealth consultations during the pandemic, we used 2020 data as a baseline comparator, as this was the first year of telehealth item numbers. Finally, we calculated the percentage of services provided in 2022 via each modality.
Results
Overall findings
Total MBS services of all modalities provided each year from 2017 to 2022 and percentage change each year.
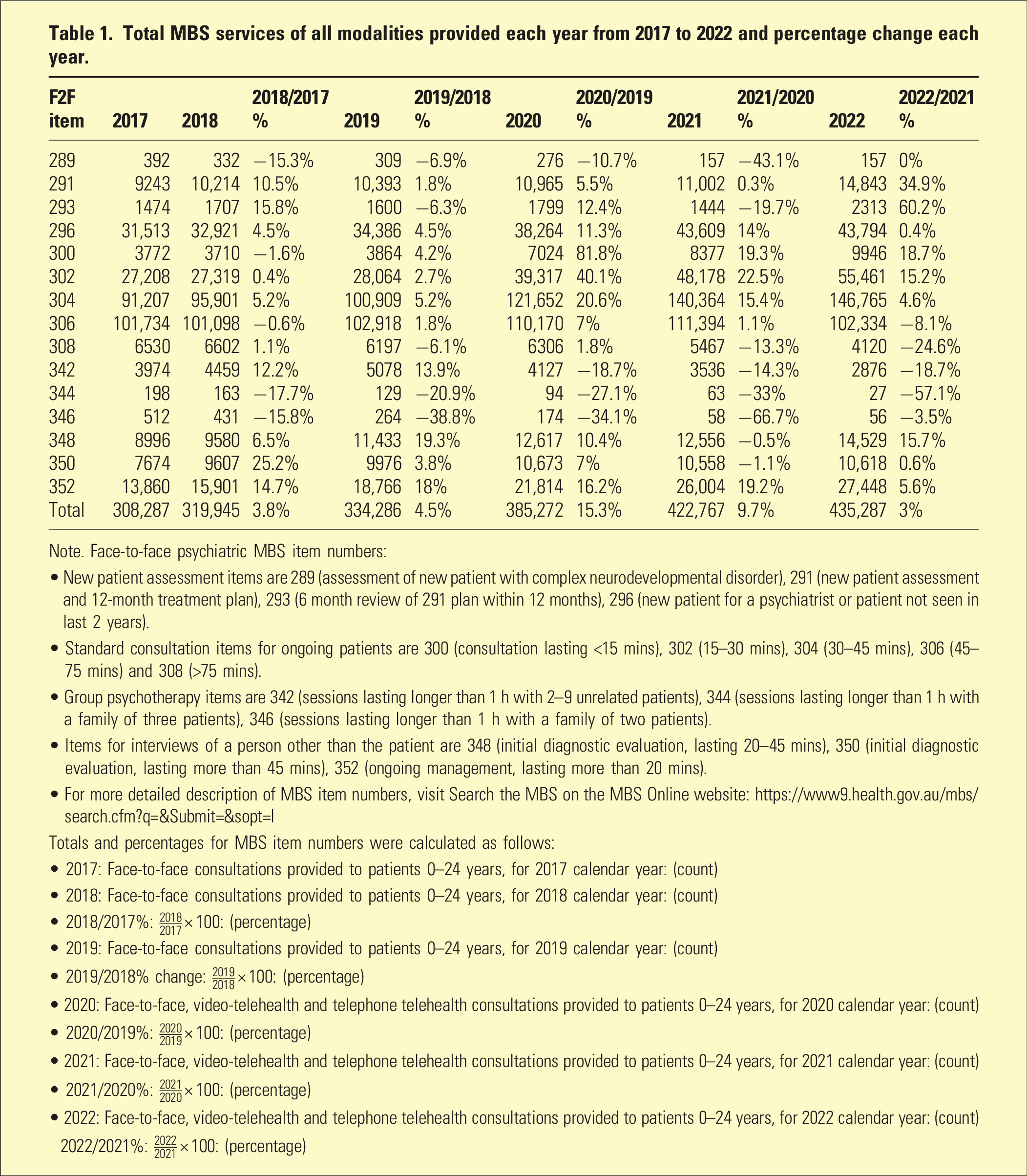
Note. Face-to-face psychiatric MBS item numbers:
• New patient assessment items are 289 (assessment of new patient with complex neurodevelopmental disorder), 291 (new patient assessment and 12-month treatment plan), 293 (6 month review of 291 plan within 12 months), 296 (new patient for a psychiatrist or patient not seen in last 2 years).
• Standard consultation items for ongoing patients are 300 (consultation lasting <15 mins), 302 (15–30 mins), 304 (30–45 mins), 306 (45–75 mins) and 308 (>75 mins).
• Group psychotherapy items are 342 (sessions lasting longer than 1 h with 2–9 unrelated patients), 344 (sessions lasting longer than 1 h with a family of three patients), 346 (sessions lasting longer than 1 h with a family of two patients).
• Items for interviews of a person other than the patient are 348 (initial diagnostic evaluation, lasting 20–45 mins), 350 (initial diagnostic evaluation, lasting more than 45 mins), 352 (ongoing management, lasting more than 20 mins).
• For more detailed description of MBS item numbers, visit Search the MBS on the MBS Online website: https://www9.health.gov.au/mbs/search.cfm?q=&Submit=&sopt=I
Totals and percentages for MBS item numbers were calculated as follows:
• 2017: Face-to-face consultations provided to patients 0–24 years, for 2017 calendar year: (count)
• 2018: Face-to-face consultations provided to patients 0–24 years, for 2018 calendar year: (count)
• 2018/2017%:
• 2019: Face-to-face consultations provided to patients 0–24 years, for 2019 calendar year: (count)
• 2019/2018% change:
• 2020: Face-to-face, video-telehealth and telephone telehealth consultations provided to patients 0–24 years, for 2020 calendar year: (count)
• 2020/2019%:
• 2021: Face-to-face, video-telehealth and telephone telehealth consultations provided to patients 0–24 years, for 2021 calendar year: (count)
• 2021/2020%:
• 2022: Face-to-face, video-telehealth and telephone telehealth consultations provided to patients 0–24 years, for 2022 calendar year: (count)
2022/2021%:
Psychiatric MBS services provide by modality from 2017 to 2022.
MBS Services provided each year per modality from 2020 to 2022.
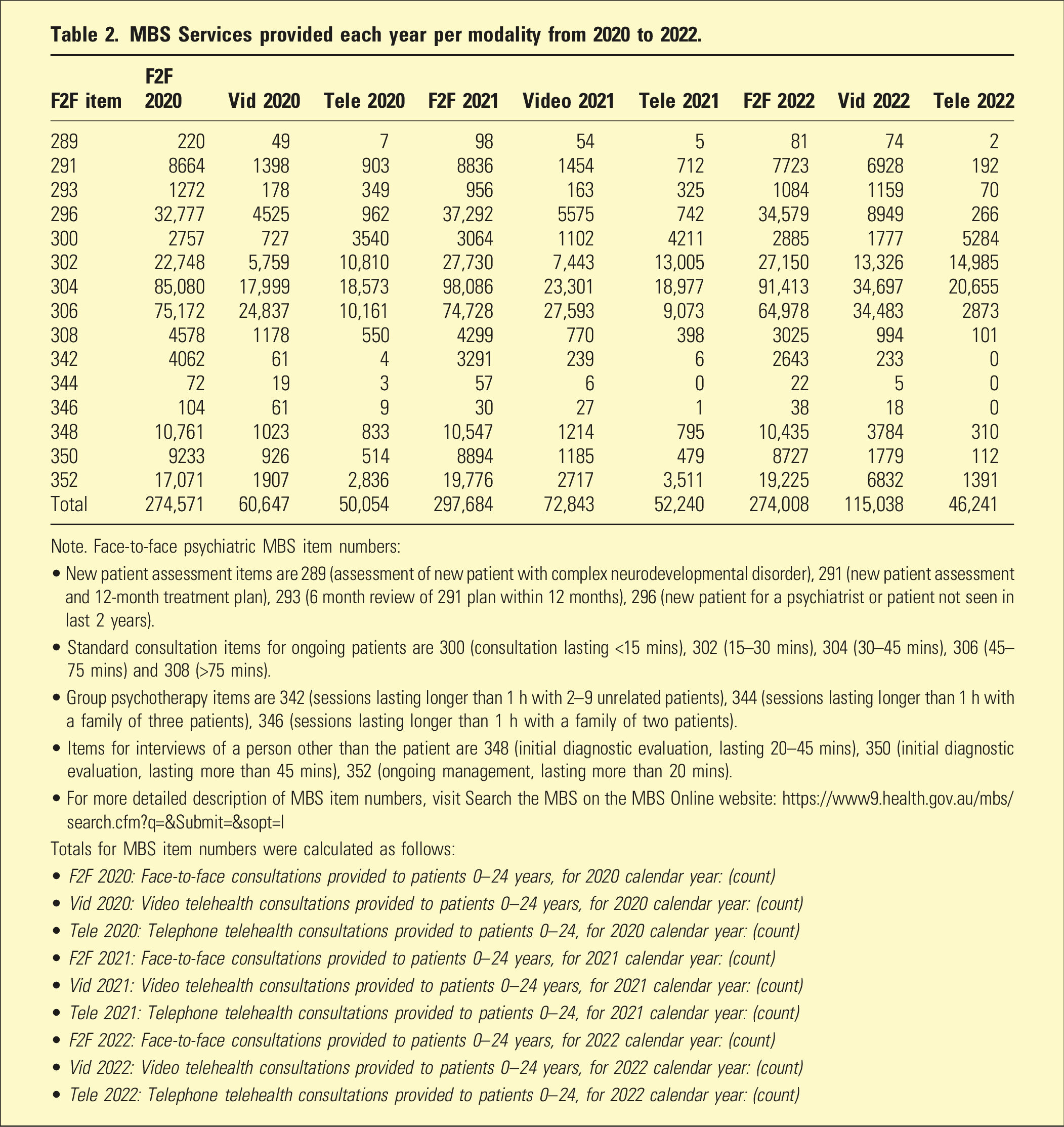
Note. Face-to-face psychiatric MBS item numbers:
• New patient assessment items are 289 (assessment of new patient with complex neurodevelopmental disorder), 291 (new patient assessment and 12-month treatment plan), 293 (6 month review of 291 plan within 12 months), 296 (new patient for a psychiatrist or patient not seen in last 2 years).
• Standard consultation items for ongoing patients are 300 (consultation lasting <15 mins), 302 (15–30 mins), 304 (30–45 mins), 306 (45–75 mins) and 308 (>75 mins).
• Group psychotherapy items are 342 (sessions lasting longer than 1 h with 2–9 unrelated patients), 344 (sessions lasting longer than 1 h with a family of three patients), 346 (sessions lasting longer than 1 h with a family of two patients).
• Items for interviews of a person other than the patient are 348 (initial diagnostic evaluation, lasting 20–45 mins), 350 (initial diagnostic evaluation, lasting more than 45 mins), 352 (ongoing management, lasting more than 20 mins).
• For more detailed description of MBS item numbers, visit Search the MBS on the MBS Online website: https://www9.health.gov.au/mbs/search.cfm?q=&Submit=&sopt=I
Totals for MBS item numbers were calculated as follows:
• F2F 2020: Face-to-face consultations provided to patients 0–24 years, for 2020 calendar year: (count)
• Vid 2020: Video telehealth consultations provided to patients 0–24 years, for 2020 calendar year: (count)
• Tele 2020: Telephone telehealth consultations provided to patients 0–24, for 2020 calendar year: (count)
• F2F 2021: Face-to-face consultations provided to patients 0–24 years, for 2021 calendar year: (count)
• Vid 2021: Video telehealth consultations provided to patients 0–24 years, for 2021 calendar year: (count)
• Tele 2021: Telephone telehealth consultations provided to patients 0–24, for 2021 calendar year: (count)
• F2F 2022: Face-to-face consultations provided to patients 0–24 years, for 2022 calendar year: (count)
• Vid 2022: Video telehealth consultations provided to patients 0–24 years, for 2022 calendar year: (count)
• Tele 2022: Telephone telehealth consultations provided to patients 0–24, for 2022 calendar year: (count)
Percentage change in number of MBS services provided per modality.
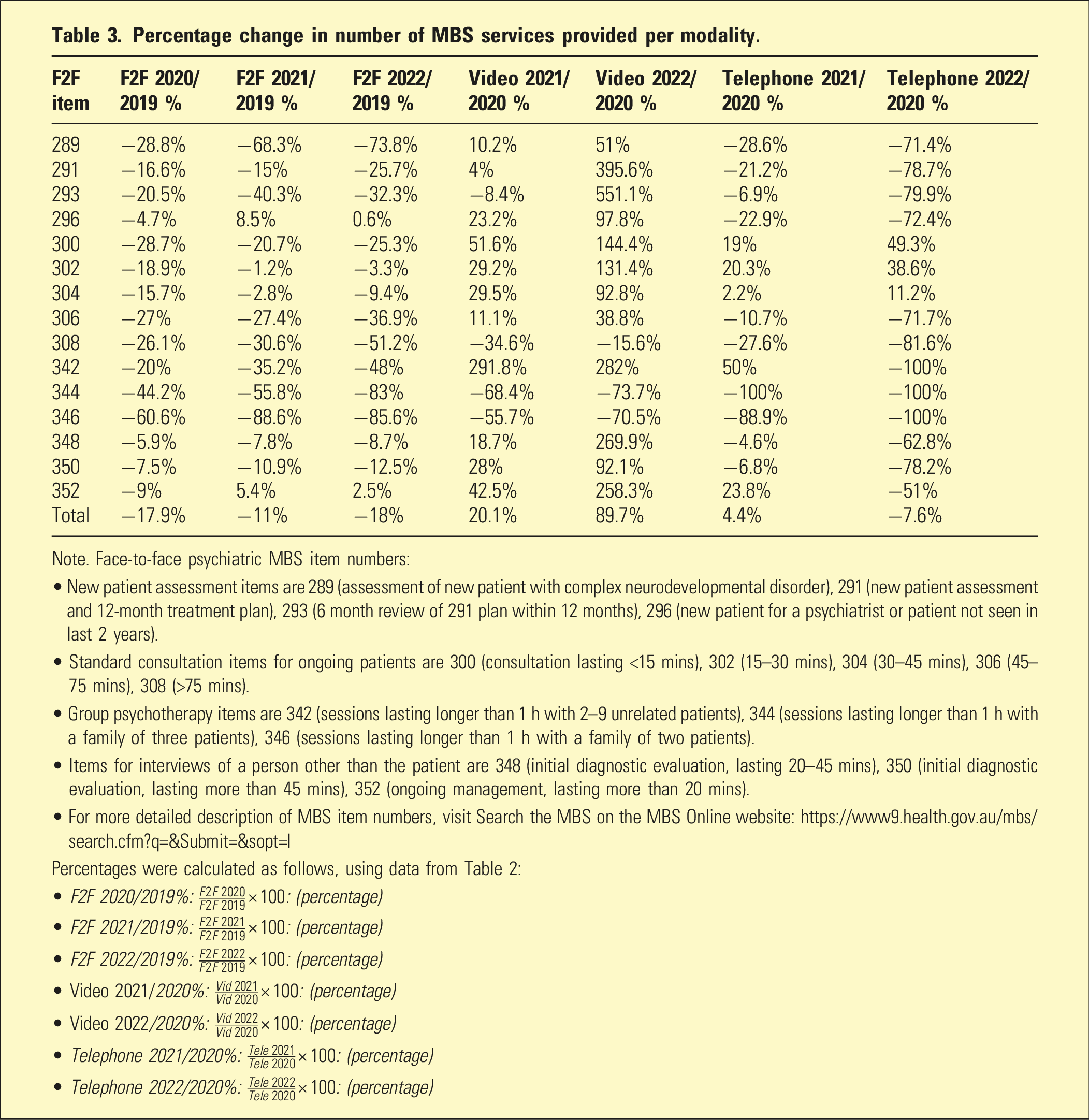
Note. Face-to-face psychiatric MBS item numbers:
• New patient assessment items are 289 (assessment of new patient with complex neurodevelopmental disorder), 291 (new patient assessment and 12-month treatment plan), 293 (6 month review of 291 plan within 12 months), 296 (new patient for a psychiatrist or patient not seen in last 2 years).
• Standard consultation items for ongoing patients are 300 (consultation lasting <15 mins), 302 (15–30 mins), 304 (30–45 mins), 306 (45–75 mins), 308 (>75 mins).
• Group psychotherapy items are 342 (sessions lasting longer than 1 h with 2–9 unrelated patients), 344 (sessions lasting longer than 1 h with a family of three patients), 346 (sessions lasting longer than 1 h with a family of two patients).
• Items for interviews of a person other than the patient are 348 (initial diagnostic evaluation, lasting 20–45 mins), 350 (initial diagnostic evaluation, lasting more than 45 mins), 352 (ongoing management, lasting more than 20 mins).
• For more detailed description of MBS item numbers, visit Search the MBS on the MBS Online website: https://www9.health.gov.au/mbs/search.cfm?q=&Submit=&sopt=I
Percentages were calculated as follows, using data from Table 2:
• F2F 2020/2019%:
• F2F 2021/2019%:
• F2F 2022/2019%:
• Video 2021/2020%:
• Video 2022/2020%:
• Telephone 2021/2020%:
• Telephone 2022/2020%:
By contrast, the number of video-telehealth consultations consistently increased throughout the pandemic, as did their percentage of total services (Tables 2 and 3 and Figure 1). In 2020, video-telehealth services accounted for 15.7% of total services. In the following year, there were 20.1% more video-telehealth services than 2020, accounting for 17.2% of total services for that year. In 2022, video-telehealth services were at their highest, with 89.7% more occasions of service than 2020 and accounting for 26.4% of total services provided that year.
However, the number of telephone-telehealth consultations decreased overall during the pandemic (Tables 2 and 3 and Figure 1). In 2020, telephone-telehealth consultations accounted for 13% of total services. In 2021, the number of telephone-telehealth services increased by 4.4% compared to 2020, but the proportion of total services provided in that year decreased to 12.4%. In 2022, the number of telephone-telehealth services decreased by 7.6% compared to 2020 and only accounted for 10.6% of total services provided that year.
COVID-19 MBS-item modality usage
For ease of reference, we refer to all MBS services using the equivalent in-person item number. Descriptions of each service are available in the Table 1 notes. Further information about MBS item numbers can be found on the Medicare Benefits Schedule website (https://www9.health.gov.au/mbs/search.cfm).
New patient assessments (289, 291, 293 and 296)
In-person new patient consultations declined at the onset of the pandemic, decreasing by 4.7–28.8% in 2020 compared to 2019 (Table 3). This decline continued throughout the pandemic for items 289, 291 and 293, decreasing by between 15% and 68.3% in 2021, and 25.7% to 73.8% in 2022. In-person new patient consultations increased for item 296 by 8.5% in 2021 and 0.6% in 2022, compared to 2019.
Video-telehealth new patient consultations increased during the pandemic for items 289, 291 and 296 by between 4% and 23.2% in 2021 and 51% to 395.6% in 2022, compared with 2020. Item 293 video-telehealth consultations decreased by 8.4% in 2021 compared to 2020, but this was followed by an increase of 551.1% in 2022.
Telephone-telehealth consultations decreased for all new patient item numbers, with 2021 services being from 6.9% to 28.6% less than 2020 and 2022 services being between 71.4% and 79.9% less than 2020.
Standard ongoing consultations (300, 302, 304, 306 and 308)
In-person ongoing consultations decreased at the onset of the pandemic by between 5.9% and 28.7% in 2020 compared to 2019 (Table 3). This decline continued for all ongoing consultations, decreasing by between 1.2% and 30.6% in 2021 and from 3.4% to 51.2% in 2022 compared to 2019.
Video-telehealth usage increased throughout the pandemic for ongoing consultations under 75 min (items 300, 302, 304 and 306), increasing by 11.1–51.6% in 2021 and 38.8–144.4% in 2022, compared with 2020. The greatest increases were seen for consultations lasting less than 15 min (item 300). Video consultations longer than 75 min (item 308) decreased by 34.6% in 2021 and 15.6% in 2022, compared to 2020.
Telephone-telehealth usage increased for ongoing consultations under 45 min (items 300, 302 and 304) by between 2.2% and 20.3% in 2021 and from 11.2 to 49.3% in 2022, compared to 2020. These telephone items were the three retained after the 2022 telehealth adjustments, while other telephone items were ceased in June 2022. 1 Telephone-telehealth ongoing consultations lasting 45–75 minutes decreased by 10.7% in 2021 and 71.7% in 2022, compared to 2020. Telephone-telehealth consultations lasting more than 75 min decreased the most by 27.6% in 2021 and 81.6% in 2022, compared to 2020.
Group psychotherapy (342, 344 and 346)
In-person group psychotherapy decreased throughout the pandemic by between 20% and 60.6% in 2020, from 35.2% to 88.6% in 2021 and 48–85.6% in 2022, compared to 2019 (Table 3).
Use of video-telehealth for group psychotherapy with 2–9 patients or more than three family members (item 342) increased throughout the pandemic, with a 291.8% increase in 2021 and 282% increase in 2022 compared to 2020. For group psychotherapy with three family members (item 344) and with two family members (item 346), video-telehealth usage decreased by 68.4% and 55.7%, respectively, in 2021, and 73.7% and 70.5%, respectively, in 2022, compared to 2020.
Telephone-telehealth use for item 342 increased in 2021 by 50% compared to 2020. For item 344, telephone-telehealth consultations were not used. For item 346, telephone-telehealth consultations decreased by 88.9% in 2021 compared to 2020. In 2022, no telephone-telehealth consultations were used for group psychotherapy.
Consultations with a person other than the patient (348, 350 and 352)
All in-person consultations with a person other than the patient declined 5.9% to 9.0% in 2020 compared to 2019 (Table 3). This decrease continued throughout the pandemic for in-person consultations with a person other than the patient to assist with initial diagnostic evaluation (items 348 and 350), decreasing by from 7.8% to 10.9% in 2021 and 8.7% to 12.5% in 2022, compared with 2019. In-person consultations with a person other than the patient for ongoing patient management (item 352) increased in 2021 by 5.4% and by 2.5% in 2022, compared with 2019.
All video-telehealth consultations with a person other than the patient increased throughout the pandemic, by between 18.7% and 2.5% in 2021 and from 92.1% to 269.9% in 2022, compared with 2019.
Telephone-telehealth usage for items 348 and 350 decreased throughout the pandemic, by between 4.6% and 6.8% in 2021 and 62.8% to 78.2% in 2022, compared to 2020. Item 352 telephone-telehealth usage increased in 2021 by 23.8% compared to 2019 but then decreased by 51% in 2022 compared to 2019.
2022 MBS-item modality usage
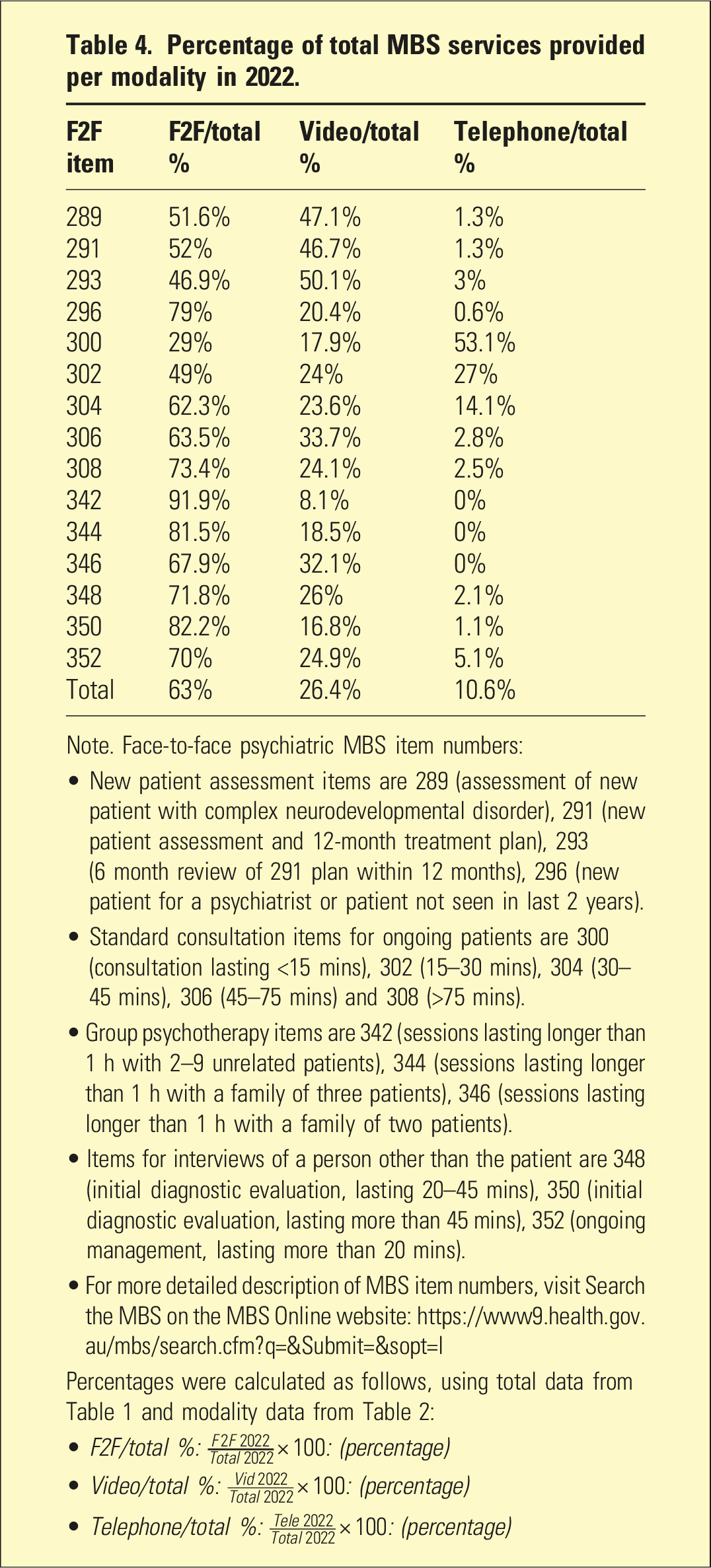
Percentage of total MBS services provided per modality in 2022.
Note. Face-to-face psychiatric MBS item numbers:
• New patient assessment items are 289 (assessment of new patient with complex neurodevelopmental disorder), 291 (new patient assessment and 12-month treatment plan), 293 (6 month review of 291 plan within 12 months), 296 (new patient for a psychiatrist or patient not seen in last 2 years).
• Standard consultation items for ongoing patients are 300 (consultation lasting <15 mins), 302 (15–30 mins), 304 (30–45 mins), 306 (45–75 mins) and 308 (>75 mins).
• Group psychotherapy items are 342 (sessions lasting longer than 1 h with 2–9 unrelated patients), 344 (sessions lasting longer than 1 h with a family of three patients), 346 (sessions lasting longer than 1 h with a family of two patients).
• Items for interviews of a person other than the patient are 348 (initial diagnostic evaluation, lasting 20–45 mins), 350 (initial diagnostic evaluation, lasting more than 45 mins), 352 (ongoing management, lasting more than 20 mins).
• For more detailed description of MBS item numbers, visit Search the MBS on the MBS Online website: https://www9.health.gov.au/mbs/search.cfm?q=&Submit=&sopt=I
Percentages were calculated as follows, using total data from Table 1 and modality data from Table 2:
• F2F/total %:
• Video/total %:
• Telephone/total %:
New patient assessments (289, 291, 293 and 296)
For items 289, 291 and 296, the majority of consultations were in-person in 2022, between 51.6% and 79% (Table 4 and Figure 2). Video-telehealth consultations accounted for 20.4–47.1%. For item 293, 50.1% of consultations were conducted via video-telehealth and 46.9% were in-person. Telephone-telehealth only accounted for 0.6–3% of all new patient consultations. Psychiatric MBS services provided in 2022 by modality.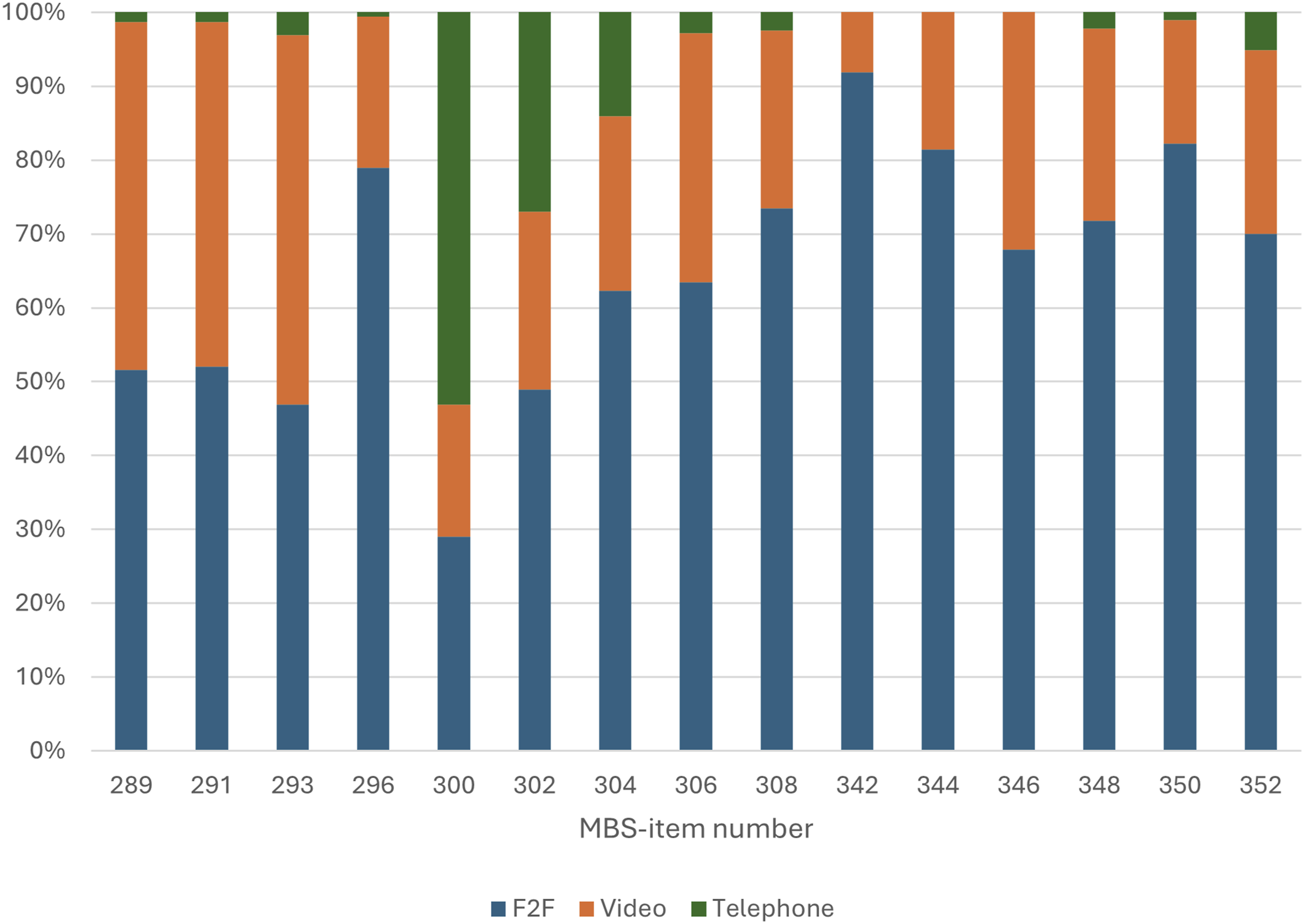
Standard ongoing consultations (300, 302, 304, 306 and 308)
In-person modality was used for 62.3–73.4% of ongoing consultations lasting more than 30 min (items 304, 306 and 308). Consultations shorter than 30 min (items 300 and 302) used in-person modality for between 29% and 49%. Video-telehealth consultations accounted for 17.9% to 33.7% of all ongoing consultations. Telephone-telehealth was used in 53.1% of consultations lasting less than 15 min (item 300), 14.1% to 27% of consultations lasting between 15 and 45 min (items 302 and 304) and 2.5% to 2.8% for consultations lasting more than 45 min (items 306 and 308).
Group psychotherapy (342, 344 and 346)
In-person modality was used for the 67.9% to 92% of group psychotherapy in 2022. Video-telehealth accounted for between 8.1% and 32.1%, while telephone-telehealth was not used at all.
Consultations with a person other than the patient (348, 350 and 352)
In-person modality accounted for between 70% and 82.2% of consultations with a person other than the patient. Video-telehealth accounted for between 16.8% and 26% of consultations, while telephone-telehealth accounted for 1.1–5.1%.
Discussion
Total MBS psychiatry service provision increased between 2017 and 2022. Although this trend existed prior to the pandemic, the largest increases of 15.3% and 9.7% were seen from 2019 to 20 and 2020–21, respectively. Research into Australian youth mental health suggests that while youth mental health was already deteriorating prior to COVID-19, psychological distress increased during the pandemic, reflecting the global trend of worsening youth mental health.5–8,10
The increase in total services provided may also be in part due to telehealth overcoming barriers to accessing psychiatry, thereby addressing high unmet demand amongst young people that existed prior to the pandemic. Research suggested that telehealth improved accessibility for paediatric patients who were otherwise under-served due to barriers like distance, commute and time away from school. 12 The therapeutic alliance between practitioners and patients was maintained at a high level when services were provided online. 12 Other research found that transitions to telehealth at the beginning of the pandemic led to a decrease in the total number of youth mental health services provided, but attendance rates increased and patients reported high levels of satisfaction. 13 These are significant findings for youth psychiatry, given the high rates of missed appointments and dropping out of in-person youth services.
Since telehealth item numbers were introduced, the proportion of consultations provided in-person has decreased from 71.3% in 2020 to 63% in 2022. Video-telehealth increased from 15.7% in 2020 to 26.4% in 2022. Telephone-telehealth decreased from 13% in 2020 to 10.6% in 2022, attributable to the cessation of most telephone items in June 2022. 1 The steady decrease in in-person and increase in video-telehealth services indicates that young patients may prefer video-telehealth, aligning with evidence that telepsychiatry has been well-received by young patients. 12 This is congruent with evidence that in-person psychiatric service provision to patients of all ages decreased despite increased total consultations, since the introduction of the new telehealth items. 15
Several psychiatric services did not follow the above trend. Standard ongoing consultations lasting more than 75 min (item 308) decreased across all modalities. Standard ongoing consultations lasting less than 45 min (items 300, 302 and 304) were the services for which telephone-telehealth items were retained and showed an increase in telephone-telehealth usage of 11.2–49.3% from 2020 to 2022. This suggests that telephone-telehealth is valuable for shorter consultations, as has been seen in previous research on adult psychiatry. 3
Group psychotherapy decreased prior to and during the pandemic. Despite this, video-telehealth usage increased by 282% from 2020 to 2022 for group psychotherapy with 2–9 patients or more than three family members (item 342). In intensive outpatient programs, videoconference group therapy showed equal efficacy as in-person delivery in improving symptoms of depression, anxiety and stress. 16 Similarly, online group therapy for veterans in the United States has been successful, with high satisfaction rates as well as higher enrolment and attendance rates than in-person groups. 17 Other research identified that connections between group participants was reduced in online therapy; however, the researchers concluded that the convenience and higher attendance rates for online therapy made this trade-off acceptable. 18
The majority of psychiatric services were provided in-person in 2022, with the exceptions of new patient consultations reviewing a 12-month plan (item 293) and standard ongoing consultations lasting less than 30 min (items 300 and 302). The lower usage of in-person consultations for items 300 and 302 are likely due to the retention of telephone items for services in 2022. 1 However, despite fewer COVID-19 restrictions in Australia in 2022, telehealth and particularly video-telehealth grew in usage for most services.
The pandemic increased rates of psychological distress and mental illness in young people globally, due to the unique stressors of lockdowns, isolation from peers and increased COVID-related media exposure.5–9,19 This distress may possibly have ongoing effects on young people in post-pandemic times. 20 The MBS should therefore address the increased demand for psychiatric services and improve accessibility of services by maintaining telehealth item numbers. 12
Telepsychiatry may not be suitable for all patients. In-person services are likely more appropriate for patients at high risk of self-harm, or those with hearing and vision impairments. 21 Furthermore, patients with less motivation to receive treatment and therefore higher likelihood of discontinuation when receiving telepsychiatry services may benefit more from in-person psychiatry. 22 Conversely, telepsychiatry may be particularly suitable for young patients who prefer being in their own environments, such as those with autism spectrum disorder and social anxiety. 23 In some cases of anxiety, telepsychiatry may provide clinicians the opportunity to observe a patient in their home environment and coach the patient through managing environmental triggers of anxiety. 24
We have underestimated the demand for psychiatry services by limiting our analysis to MBS subsidised services, as state public health services may not bill the MBS. Estimating the severity of COVID-19 restrictions would have been useful to understand the demand for telehealth services during the pandemic, however this was beyond the scope of this study. Another limitation of the data analysis is that we did not provide population adjusted rates of MBS item usage.
Future research should investigate the quality of telepsychiatry provided to young patients and the barriers to accessing telepsychiatry for Australian youth, as well as access equality across geographical areas and socioeconomic statuses. Future research could also compare MBS item usage between gender groups and between ages 0–14 and 15–24 years. This would provide more information on how acceptability of telehealth varies within the Australian youth population. Moreover, our research focused on psychiatric services, but future research could investigate the use of telehealth for allied health psychological services, particularly as these may be more accessible to Australian youth than psychiatry.
Conclusion
Based on the findings that young people have used video-telehealth during and after the pandemic, we advise that telepsychiatry should remain an option to improve access for patients aged 0–24 in post-pandemic times. This is not to suggest that video-telehealth has or should completely replace in-person consultations, which remain the major proportion of total consultations. However, our findings do suggest that video-telepsychiatry is a viable option for many young people, so MBS items should continue to reflect this situation in post-pandemic times.
Footnotes
ORCID iDs
Ethical considerations
No ethics approval or consent was required as this paper does not involve research with humans or animals.
Author contributions
All authors have satisfied: Substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; Drafting the work or revising it critically for important intellectual content; Final approval of the version to be published; and Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: LW, SK, TB, SA and JCLL are editorial staff of the journal and were not involved in editorial handling or review of the paper, which is independently peer-reviewed. It represents the views of the authors, not the journal.