
Abstract
Objective
This study aimed to describe the social demographics and clinical profile of patients referred to the psychiatry service within the local Queensland metropolitan Aboriginal Medical Service (AMS).
Method
This was a retrospective cohort study of patients referred to the psychiatry service provided at three clinics of a metropolitan AMS, over an 18-month period. Medical records were accessed to determine demographic and diagnostic information.
Results
Diagnostically, 53% of patients had mood/anxiety disorders, 10% psychosis, 23% substance use and 14% with other diagnoses. There was approximately 50% non-attendance rate with no statistical difference between gender and age groups. The highest proportion of non-attenders within age groups was males 45–54 years old. The patients needed to travel an average of 20 km to attend the AMS.
Conclusion
The high non-attendance rates, and proportionately more males within the age group 45–54 years who were more likely to not attend their mental health appointments, suggested a target area for outreach services which have been implemented in the AMS. Some of the recommended solutions included confirming attendance the day prior and supporting with transport. This study highlighted the large distance that Aboriginal and Torres Strait Islander people must travel to access culturally appropriate service.
Aboriginal and Torres Strait Islander peoples (respectfully referred to as Indigenous Australians or Indigenous people) have higher mental health needs than non-Indigenous Australians, but lower access to mental health services. 1 The Fifth National Mental Health and Suicide Prevention Plan laid out Aboriginal and Torres Strait Islander social and emotional wellbeing among important priority areas. 2 The Queensland Health Aboriginal and Torres Strait Islander Mental Health Strategy 2016–2021 focused attention on inter-sectoral collaboration to address the social determinants of mental health problems in Indigenous Australians. 3
The social and emotional wellbeing of Indigenous Australians is impacted by historical policies such as dispossession and stolen generations, as well as ongoing marginalisation. 4 There is evidence that approximately one third of adults experience high levels of psychological distress. 5 Queensland’s Indigenous people carry 32% higher than expected burden of disease compared to non-Indigenous people. 6 Anxiety and depression were found to be the largest diagnostic group within mental disorders, followed by schizophrenia and substance use disorders. 6
Isaacs et al. (2010) emphasised the need for more region-specific research to assist with identifying local communities mental health needs. 7 This research study was conducted in an Aboriginal Medical Service (AMS) in a metropolitan region of Queensland. The local public mental health service provides onsite psychiatry input through General Practice (GP) liaison psychiatry service, which includes direct clinical assessments by a psychiatry registrar under supervision of a part-time psychiatrist, phone support and case-conferences with the GP’s.
Study objectives
To describe the social demographics and clinical profile of patients referred to the psychiatry service provided at the AMS; and to determine the distance travelled to access these health centres.
Methodology
This retrospective cohort study focused on patients referred to the psychiatry service provided at three clinics of the AMS, in a Queensland metropolitan area, over an 18-month period. Adults referred to the psychiatry service were identified through the appointment diary in Medical Director software.
The medical notes entered by the GP liaison psychiatry service were reviewed retrospectively to determine the DSM-5 diagnosis of those who were assessed. Mapping of home postcode was done, using GPS satellite mapping software, against the clinic where individuals attended to determine the approximate distance travelled. The distance was approximated using postcode to further protect the identity and personal information of study participants who were all de-identified. Numbers of patients, and their age group, that were referred by the GPs for additional mental health input were generated by the AMS practice managers from the Medical Director software and not directly identified. This protocol was developed in consultation with AMS managers and Indigenous members of the social and emotional wellbeing team.
Data analysis
Analyses were performed using STATA statistical software. Chi squared analyses were performed for gender and age comparing attendance. A two-sample Wilcoxon rank-sum (Mann–Whitney) test was performed to account for the skewed age range data and adjusted for variance. Logistic regression models were used to determine predictors of non-attendance controlled for gender, age and employment status as independent variables against the outcomes ‘seen’ versus ‘did not attend’ (DNA) clinic appointments.
Results
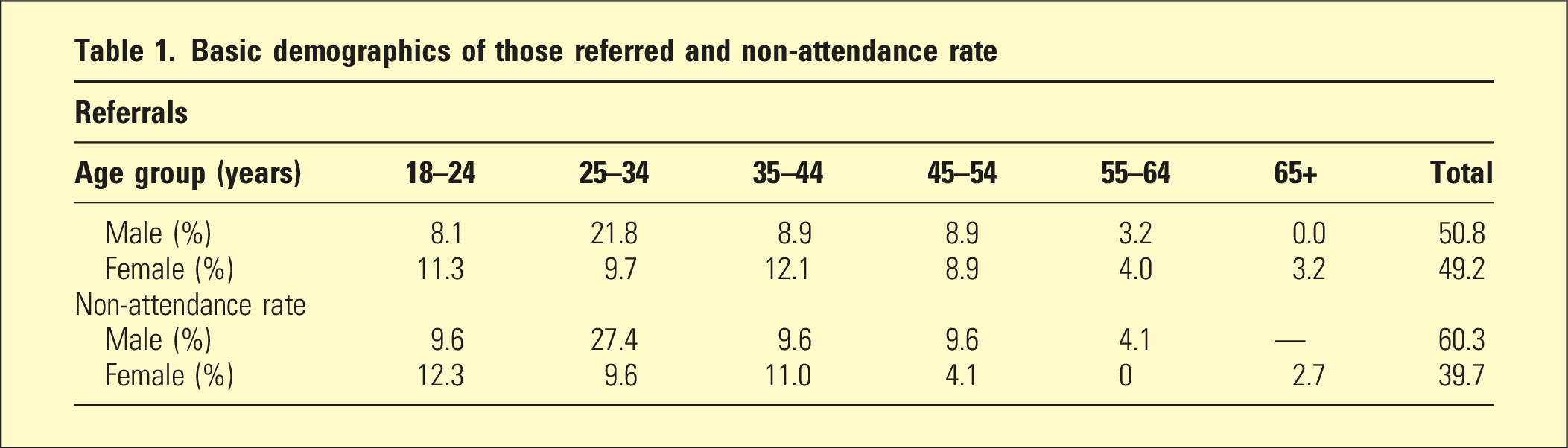
Basic demographics of those referred and non-attendance rate
Number of Aboriginal and Torres Strait Islander people in the catchment area of one AMS clinic (potential patients) and the number and proportion of those who are patients seen by the service
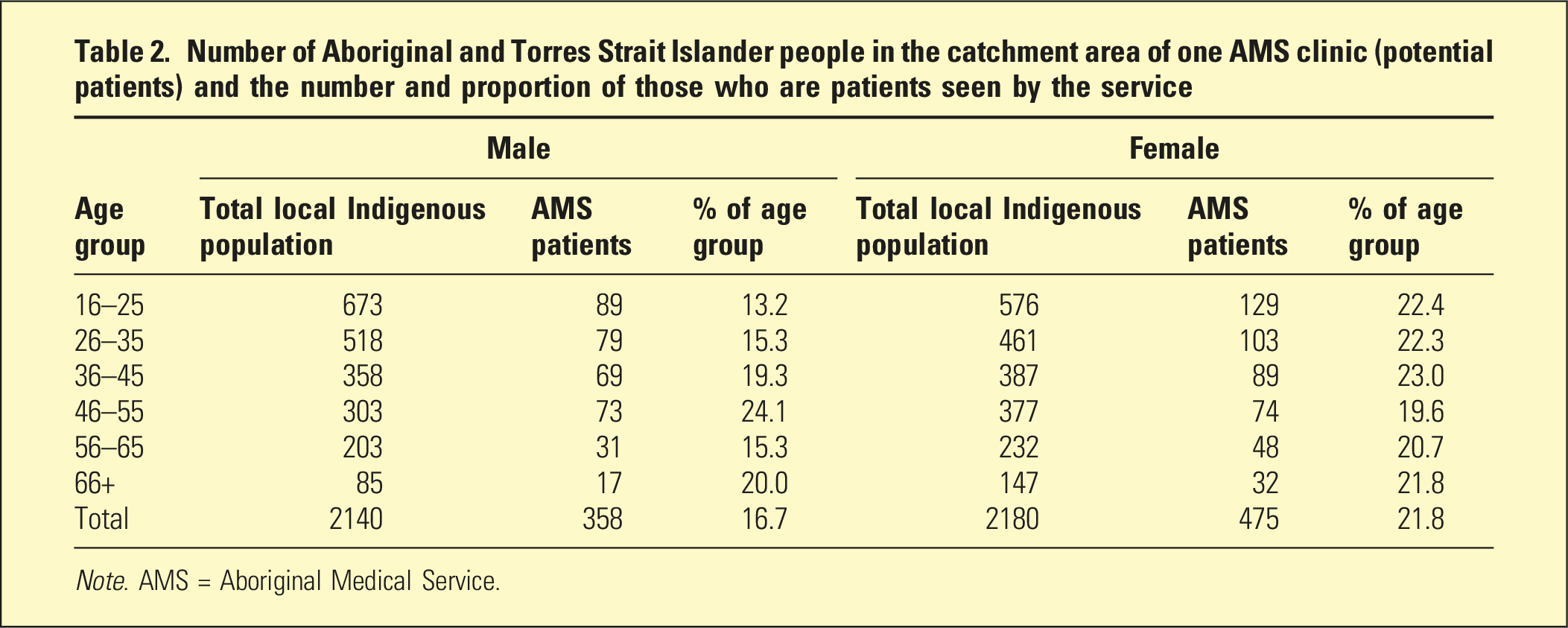
Note. AMS = Aboriginal Medical Service.
The total non-attendance rate across all age groups was 60.3% for males, compared to 39.7% for females. The highest proportion of non-attenders within age group were males within the 45–54 years group at 63.6%. Males had higher non-attendance rates across most age groups.
Chi2 statistical analysis showed a significant difference between males and females, (Chi2 = 0.014; Fisher’s exact = 0.011) in the 25–34 age group only. A two-sample t-test was conducted for those who attended versus DNA by age; and a Mann–Whitney U test was conducted to account for the skewed distribution of the data. Both tests found that the difference in the data between those who attended versus DNA by age was not statistically significant (Pr([T] > [t]) = 0.2226 (t-test) and Pr > [z] 0.2297 (Mann–Whitney U test)).
Linear regression models did not find any statistically significant predictors of non-attendance between age groups when males and females were grouped. When disaggregated by both age group and gender, linear regression did not show either to be a predictor of non-attendance with a 95% CI of −0.2 to 0.09, p value 0.4, except for females aged 55–64 years, where 100% of those referred attended their appointments.
Approximately 20% of the total local Indigenous population in one AMS clinic catchment attended the service, thereby adequately representing the local population as shown in Table 2.
Regarding employment status, the greatest proportion (51%) of patients were found to be receiving a Centrelink benefit, including Newstart payment, Disability Support Pension and family payments. A total of 26% were employed, 9% were retired or dependent on others and 2% were students. About 12% of patients had no confirmed employment status listed in the data system.
Employment status of those referred, diagnostic groups and distance travelled of those seen
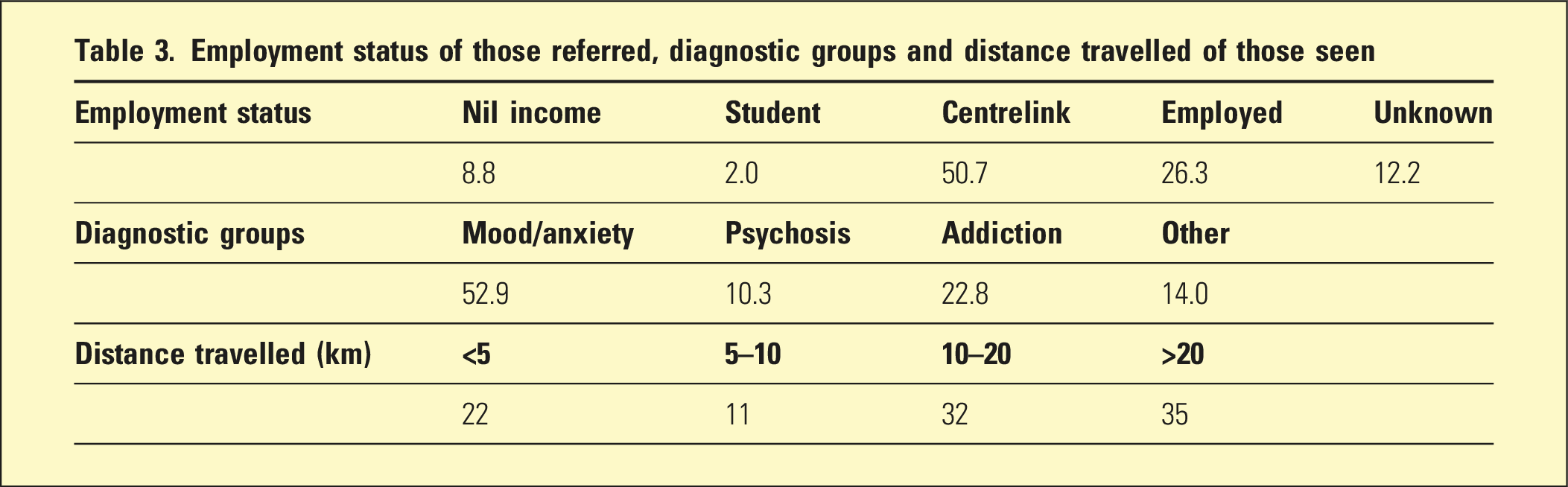
Distance travelled from home post code to the AMS clinic by those who attended, shown in Table 3, suggests that Indigenous Australians had to travel a significant distance to attend a culturally appropriate setting for a mental health service within a metropolitan area with 67% of patients travelling more than 10 km and 35% of patients travelling more than 20 km. The average distance travelled was 20 km.
Discussion
This study found that the rate of referrals for mental health disorders among Indigenous Australians was the highest in adults aged 25–34 years. Referrals over 50 years showed a significant decline in numbers, with no males over the age of 65, which may reflect shortened life expectancy of Indigenous Australians and unmet needs of health services for older males. There were high rates of non-attendance across both genders and age groups, and males were less likely to attend their appointments than females.
These results indicate the need for targeted outreach programs utilising kinship structures within the community, aimed at making culturally appropriate contact with Indigenous population, especially men to provide education around mental health and encourage attendance. Other solutions could be reception confirming attendance the day prior to the appointment and the clinic staff assisting with transport if required. Previous studies have also stressed the importance of the social and emotional wellbeing model which recognises the importance of connection to land, culture, spirituality, ancestry, family and community for Indigenous Australians. 9
This study found that 10% of Indigenous patients seen had a diagnosis of psychosis and chose to be managed by their GP as opposed to attending a mainstream tertiary medical service. Supporting GPs and Aboriginal Medical Services is essential to ensure adequate treatment for these serious mental disorders. Indigenous Australians have a higher incidence of suicide than non-Indigenous people and are also less likely to engage with mental health services. 10 It is important to develop partnerships between specialist services and primary care services to improve support for patients in the community.
Hepworth et al. (2015) reported that feelings of ‘shame’ and stigma about mental health conditions among Indigenous Australians lead to avoidance of mental health services located in a designated mental health building. 11 Integration of mental health services within the medical service in the same building led to increased engagement. 11 The fact that Indigenous people chose to travel an average of 20 km to access culturally appropriate services is a clear indication of their preference for AMS, rather than mainstream GP or tertiary care mental health services. Potential strategies to improve engagement of Indigenous Australians include improving access to culturally appropriate mental health services, engagement of Indigenous mental health professionals and improved cultural awareness and competency of non-Indigenous staff through appropriate training and support.11,12 In addition, involvement of families and Indigenous elders to incorporate cultural perspectives and values and an Aboriginal and Torres Strait Islander multidisciplinary outreach team helps in development of trust and the breaking down of stigma. 13
Further localised studies may assist to understand predictors for poor attendance of appointments and may also help elucidate target areas for communication and outreach from the Indigenous Social and Emotional Wellbeing Team. Such research could assist to reduce shame and stigma in the metropolitan setting and ultimately contribute to ‘closing the gap’.
Limitations and strengths
This study has a few limitations. First, diagnostic information was not collected from patients who did not attend their appointments, thereby not allowing the diagnoses to be analysed as a predictor of non-attendance. Although the data were collected over an 18-month period, the sample size remained relatively small. Some demographic information such as employment status and home address could not be confirmed as current. Finally, the distance travelled was estimated via post code using a GPS mapping program, which may introduce some error as some postcodes cover a large area and the mapping program utilised the central point to estimate distance. These limitations should be balanced with the study strengths, for example, the sample comprised 20% of the total local population, medical records of every patient were manually reviewed and the study was devised in consultation with Indigenous members of AMS. To our knowledge, this is the first study which has calculated the average distance travelled by Indigenous Australians in a metropolitan area to access culturally appropriate mental health services and illustrates scope for further research into the causes and predictors for non-attendance.
Conclusion
This retrospective cohort study found that the most common diagnoses of patients seen by a mental health service at a metropolitan AMS were mood/anxiety disorders, followed by substance use disorders and psychotic disorders. High rates of non-attendance of appointments were found, the reasons for which need to be investigated through further research. Indigenous Australians chose to travel a large distance to access the service, which depicts their preference for culturally appropriate services at the AMS rather than mainstream GP clinics or tertiary mental health services which may have been geographically closer. This study therefore may identify a high unmet need for culturally appropriate services for Indigenous Australians in a metropolitan region, a fact which is often not highlighted as much as accessibility issues in regional/rural Australia.
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Author note
In this article, we may respectfully refer to Aboriginal and Torres Strait Islander Peoples as Indigenous Australians or Indigenous people(s).