
Abstract
Keywords
It is widely acknowledged that the health of Aboriginal Australians is poor when compared with non-Aboriginal Australians, and worse than their indigenous counterparts in New Zealand, Canada and the USA [1, 2]. It has been suggested that life expectancy for indigenous Australians is ‘100 years behind those for non-indigenous people’ [3]. The poor health of Aboriginal Australians has been attributed to sociosomatic illness arising from factors such as dispossession, disadvantage, forced separation of children from parents and communities, and legislation. Hospital inpatient and mortality data suggest that Aboriginal and Torres Strait Islander people were more likely to be hospitalized for ‘mental and behavioural disorders’ than the general population [4]. Mortality associated with mental disorder, particularly that related to psychoactive substance use, was more common among indigenous Australians [4].
High rates of mental disorder have consistently been found in prisoner populations [5–9]. A recent review of >60 prison mental health surveys found that inmates were more likely than the general population to have a psychotic illness, major depression, and personality disorder [6]. We recently identified high levels of mental disorder among New South Wales (NSW) prisoners (46%), substance use disorder (55%) and personality disorder (41%) [5, 10]. Mental disorders were higher in women than men, and more prevalent among those screened at the time of reception into the prison system compared with those already serving a sentence. Simpson et al. found similar levels of mental illness between indigenous New Zealand (Maori), Pacific Islander, and European prisoners [11].
Prisoner populations in Australia are continuing to rise, with a 43% increase between 1994 and 2004 [12]. In 2004, Indigenous people were 11-fold more likely to be imprisoned than non-Indigenous people. Although around 2% of the general population are Aboriginal, >19% of men and 30% of women in full-time custody are indigenous [13].
The 1991 Royal Commission into Aboriginal Deaths in Custody (RCIADIC) highlighted the plight of indigenous prisoners in Australia and made more than 300 recommendations regarding social, health and judicial issues [14]. The recommendations concerning mental health were focused mainly on suicide risk following incarceration. Despite the concerns expressed by the RCIADIC, there have been remarkably few publications on the mental health of Aboriginal people in custody. Given the stark facts regarding indigenous over-incarceration together with the high prevalence of mental disorder among prisoners, it is important that the mental health needs of Aboriginal people in custody be clearly identified and addressed.
As part of a review by Justice Health of the Aboriginal Health Strategic Plan, we were asked to provide information on the physical and mental health status of Aboriginal prisoners in custody to inform this process [15]. The mental health findings used in that review form the basis for this article. We compare the 1 month and 12 month ICD-10 prevalence estimates of mental illness in Aboriginal and non-Aboriginal prisoners in NSW.
Methods
Setting
The survey was conducted at 29 correctional centres across NSW.
Sample
The sample consisted of two groups: (i) reception prisoners (those coming into prison following a court appearance); and (ii) sentenced prisoners (those who were already convicted and serving a prison sentence at the time of the study).
The reception group consisted of a consecutive sample of prisoners admitted into the State's correctional system over a 4 month period in 2001 and assessed within 24 h of admission into prison (n = 953). Details of this study have been described elsewhere [10]. Male reception prisoners were assessed primarily at the State's main remand facility in the Sydney metropolitan area, which processes around 80% of new admissions to the correctional system. Three small rural sites were also used. Women were assessed at the State's main reception centre for women in Sydney. The sample was screened consecutively whenever possible.
The sentenced sample consisted of inmates recruited into the 2001 NSW Inmate Health Survey [9]. Out of a total of 914 inmates (approx. 10% of all men and 34% of all women in full-time custody) who participated in the 2001 NSW Inmate Health Survey, 557 (61%) were available and consented to further mental health assessment. The response rate to the 2001 Inmate Health Survey was 85%. The Inmate Health Survey sample was stratified by sex, age, and Aboriginality and is described elsewhere [9]. Participants were approached several weeks after the main health survey and invited to undertake further mental health screening.
Assessment
Screening for mental disorder in both the reception and sentenced groups was undertaken using the Composite International Diagnostic Interview-Auto (CIDI-A) and a number of other screening measures incorporated into the programme such as the Kessler Psychological Distress Scale (K-10) and a psychosis screener [16, 17]. The psychosis screener assessed for symptoms of psychosis occurring in the past 12 months only [18].
The interview was the same as used in the Australian National Survey of Mental Health and Wellbeing (NSMHWB) [19]. The programme yields 12 month and 1 month diagnoses for both International Classification of Diseases-Version 10 and DSM IV [20].
Mental health nurses working in the correctional health system screened the reception prisoners while both forensic psychology masters’ students and Justice Health nurses conducted the assessments on the sentenced sample.
Ethics
Ethics approval was granted by the Corrections Health Service, and the Department of Corrective Service's Human Research and Ethics Committees.
Statistical methods
Data from the CIDI were imported into SPSS version 11 (SPSS Inc., Chicago, IL, USA) and scored using a programme developed by staff at the Clinical Research Unit for Affective Disorders, Sydney. For the purpose of this study, ‘any mental illness’ refers to psychotic symptoms in the past 12 months, and any ICD-10 affective or anxiety disorder in the previous 12 months. Summary statistics were calculated using SPSS version 12 (SPSS).
Results
Demographic and offending characteristics
Aboriginal men were slightly younger than non-Aboriginal men (28.9 years vs 31.0 years), more likely to be living in a married or de-facto relationship, have a prior history of juvenile detention, and have a greater number of previous adult incarcerations (Table 1). Similarly, Aboriginal women were younger than non-Aboriginal women (27.0 years vs 31.2 years), more likely to have been in juvenile detention, and have a greater number of prior adult incarcerations.
Subject characteristics
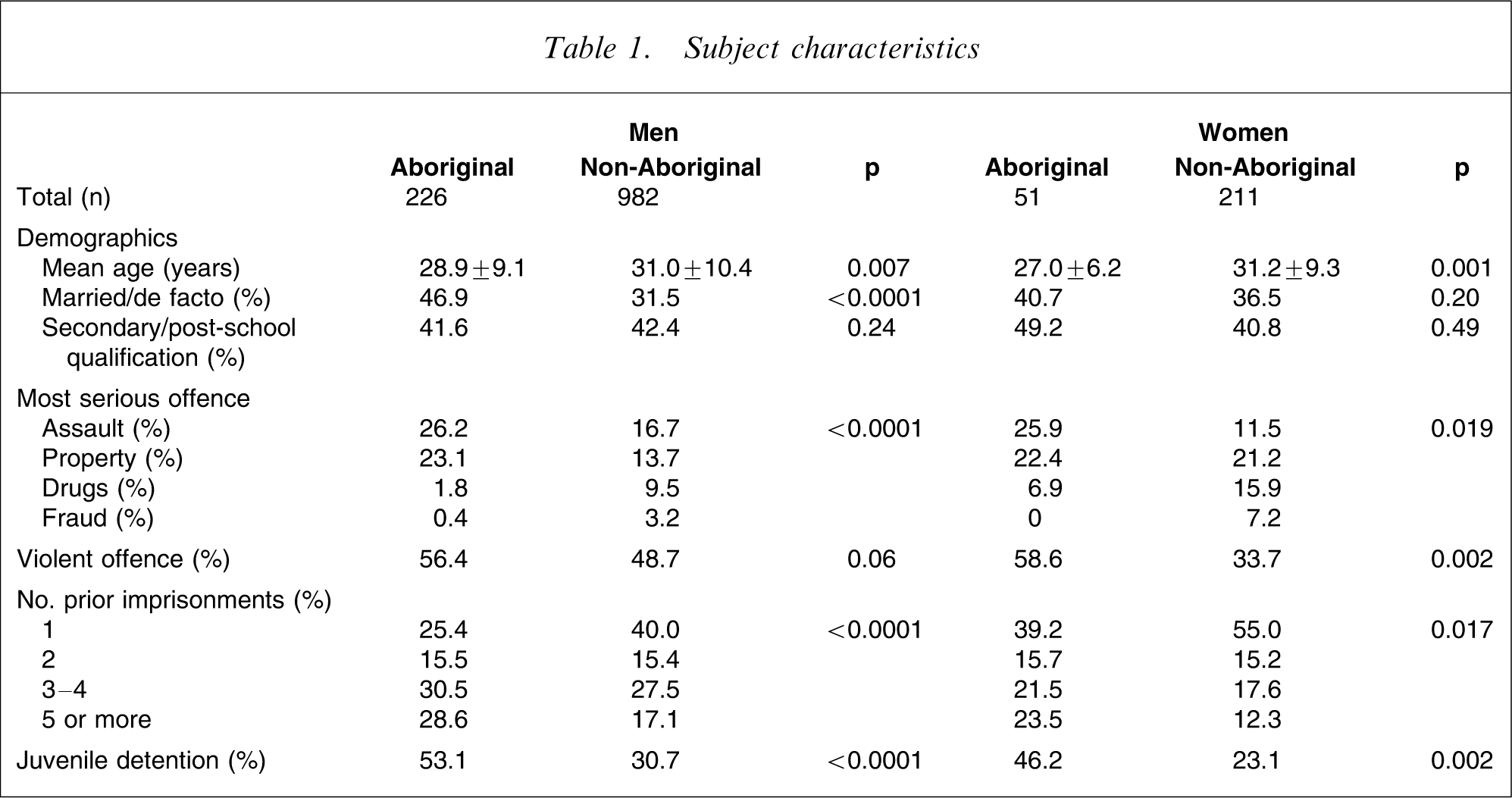
Aboriginal men and women were more likely to have been convicted of a violent offence (murder, assault, robbery) while non-Aboriginal men and women were more likely to have been incarcerated for a drugs-related offence.
Mental disorder
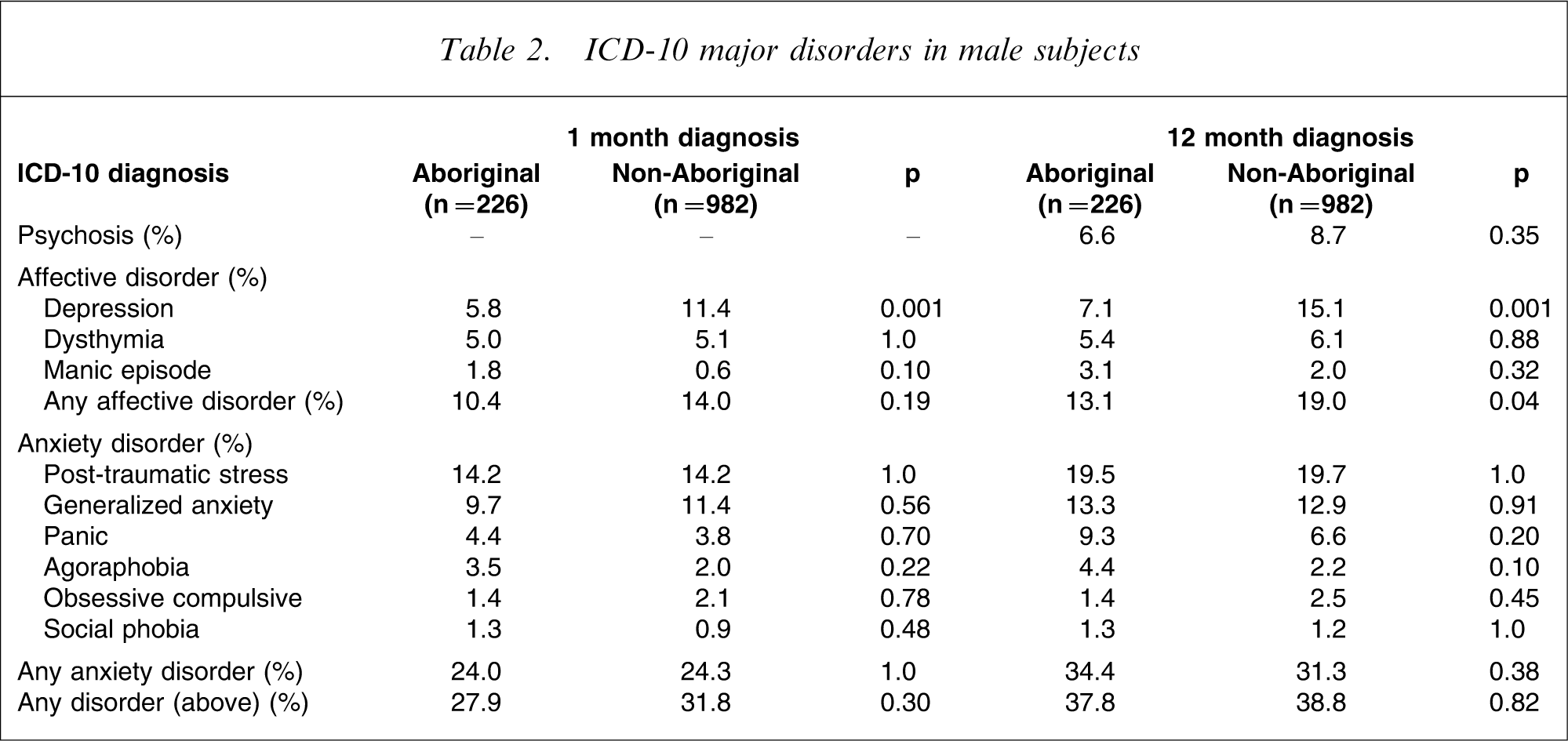
In men, both the 1 month and 12 month prevalence of depression was significantly lower in the Aboriginal group compared with non-Aboriginal prisoners (Table 2). Otherwise, no differences were identified between Aboriginal and non-Aboriginal men in either the 1 month and 12 month prevalence of affective and anxiety disorder, and psychosis.
ICD-10 major disorders in male subjects
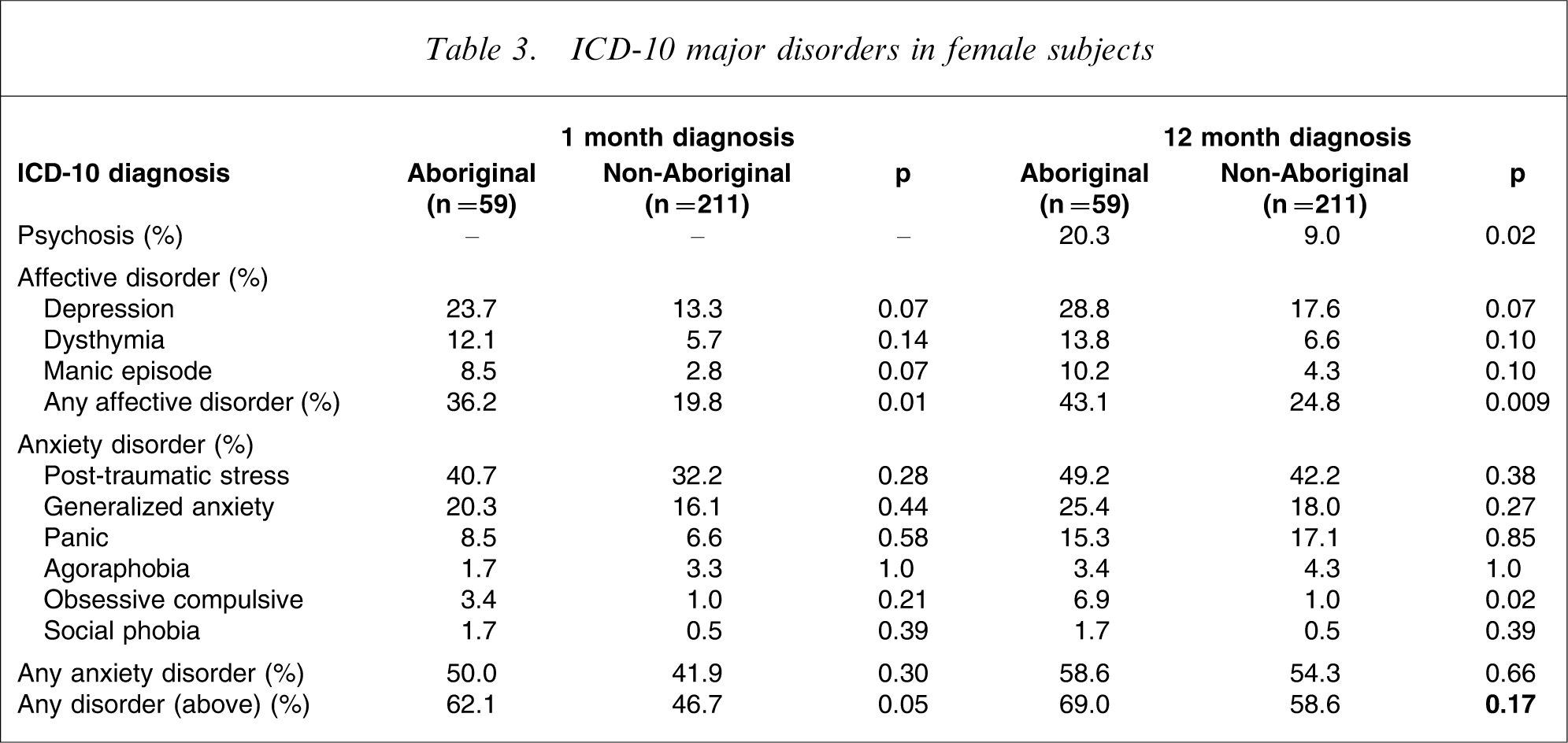
Aboriginal women were more likely than non-Aboriginal women to screen positive for symptoms of psychosis in the prior 12 months and have a higher prevalence of affective disorder (1 month and 12 month; Table 3). They were also more likely to be depressed than non-Aboriginal women, but this was not significant. Interestingly, Aboriginal women were more likely to have a diagnosis of obsessive–compulsive disorder in the prior 12 months (Table 3).
ICD-10 major disorders in female subjects
Kessler psychological distress scale
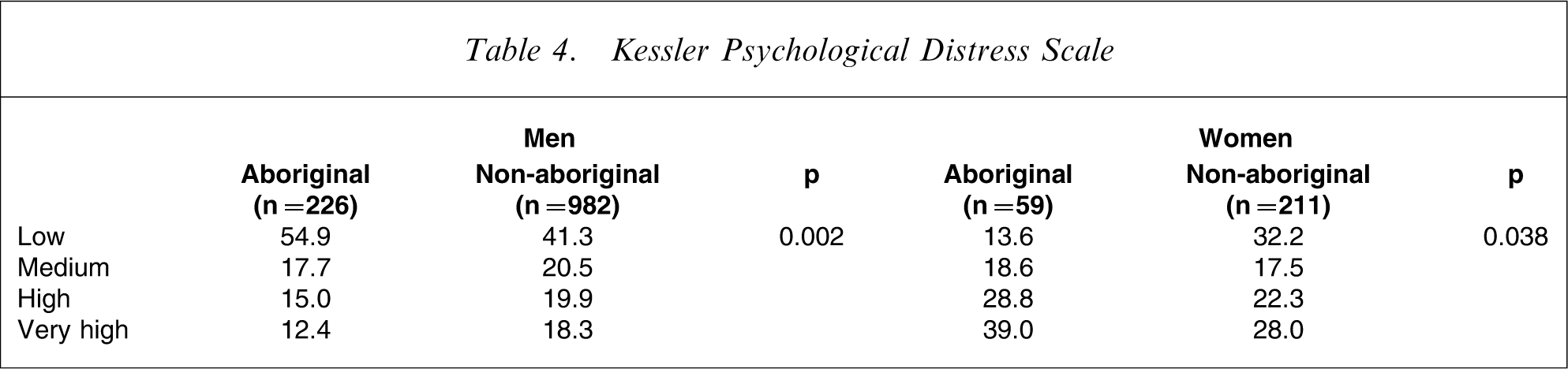
Aboriginal women were more likely than non-Aboriginal women to be classified as having high or very high psychological distress, which concurs with the higher prevalence of mental disorder detected using the CIDI. However, the reverse pattern was found in men: non-Aboriginal men were more likely to be classified as having high or very high psychological distress scores (Table 4).
Kessler Psychological Distress Scale
Suicide and Self-harm
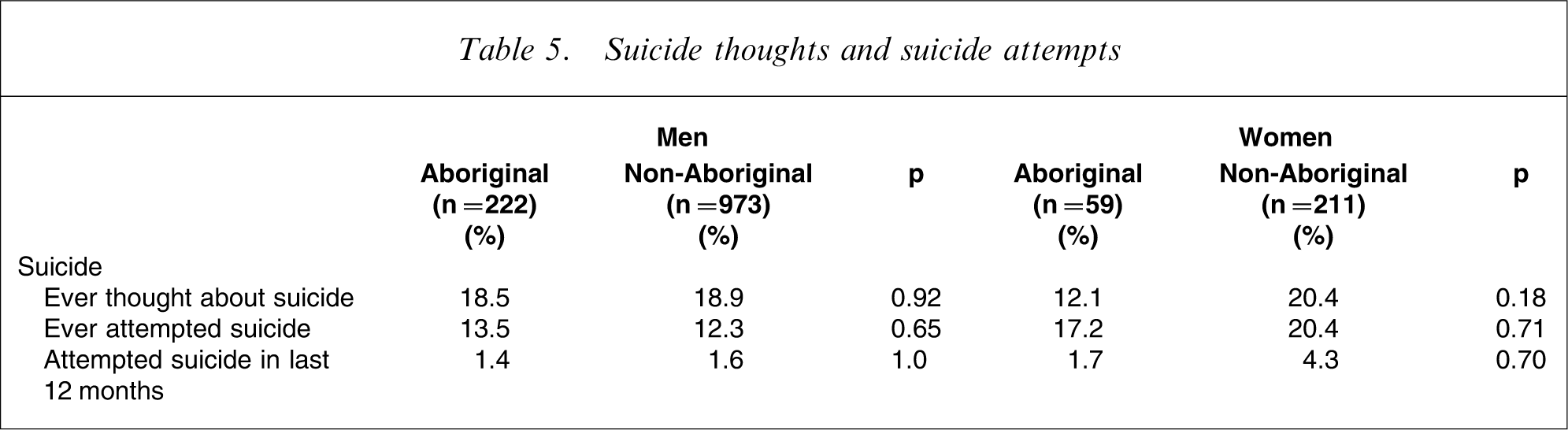
Suicidal thoughts and attempts (lifetime and prior 12 months) occurred with similar frequency in both Aboriginal and non-Aboriginal men and woman (Table 5).
Suicide thoughts and suicide attempts
Discussion
This is the first study to compare in detail the mental health of Aboriginal and non-Aboriginal offenders in Australia. We found few differences in the prevalence of mental illness between Aboriginal and non-Aboriginal male prisoners in NSW apart from depression and psychological distress, which was higher in the latter group. Suicidal thoughts and behaviour were similar in the two groups. Our findings agree with those of Simpson et al., who found similar levels of mental illness between indigenous (Maori) and non-indigenous prisoners, but higher rates of current depression among men of European descent compared with indigenous men [11].
Aboriginal women prisoners were more likely than their non-Aboriginal counterparts to be diagnosed with psychosis, depression, and obsessive–compulsive disorder. Given that our previous work found that prisoners had significantly higher levels of mental illness and psychological distress than the community, this finding suggests that Aboriginal women prisoners are one of the most psychologically vulnerable groups in the community [21].
The general absence of differences in the mental health status between Aboriginal and non-Aboriginal prisoners, particularly among men, is noteworthy. Prisoner populations, both Aboriginal and non-Aboriginal, have backgrounds characterized by sociodemographic disadvantage (poor educational attainment, abuse and neglect, unemployment, parental incarceration). With disadvantage comes an increased vulnerability for poor physical and mental health, regardless of ethnicity. This could explain the lack of significant differences between indigenous and non-indigenous prisoners. This finding is similar to that found in the New Zealand prisoner population [11].
In the present study, Aboriginal and non-Aboriginal prisoners differed with regard to criminographic and demographic factors. They had more prior periods of incarceration in juvenile detention centre and adult prisons and were more likely to be incarcerated for a violent crime [22, 23].
While these data provide a broad overview of mental illness in Aboriginal inmates, more research is required to understand the culturally specific needs of the Aboriginal prisoners with a mental illness. For example, the cultural mechanisms underlying mental disorders in the Aboriginal population may differ from non-Aboriginal populations and impact on which treatment approaches are likely to be effective. It is possible that psychological and emotional distress is expressed in a culturally determined manner such that the screening instrument was insensitive. However, experienced mental health clinicians who administered the CIDI, were directed to be clinically sensitive to mental illness symptoms within this population group and the study used a number of indigenous interviewers who did not report comprehension difficulties regarding the individual items used to generate the diagnosis. Feedback provided by the interviewers was that Aboriginal participants comprehended the questions. This does not preclude the possibility of variation in cultural expression of mental illness.
There has been little research with regard to obsessive–compulsive disorder among indigenous populations. It is possible that this may be a spurious finding possibly relating to the nature of the questions. This requires further examination.
Post-traumatic stress disorder was more than twice as common in women than men, which reflects the relative difference between the sexes in the community (2% in men and 4% in women) [24]. However, the prevalence did not differ significantly between indigenous and non-indigenous prisoners. The high rates of both 12 month and current post-traumatic stress disorder probably reflect the social milieu common to this population. It is ironic that the community perceives prisoners as ‘traumatizers’, but they are a highly traumatized group.
Many Aboriginal people return from prison to isolated and outlying geographic areas with limited access to psychiatric services. Pre-release planning for those returning to isolated areas needs to take the lack of adequate mental health resources as well us cultural needs into consideration. Although we do not advocate incarceration as a treatment option, contact with the criminal justice system is an opportunity for initiating contact with mental health services. It is important that this opportunity is realized, particularly for those in areas with poor access to health services.
Suicide and self-harm receives considerable attention within correctional populations. While prisoners are at an increased risk of suicide compared with the general population, a recent NSW study found the risk of death from suicide to be higher among non-indigenous prisoners [25]. We found no difference between the indigenous and non-indigenous inmates in terms of either suicidal ideation or suicide attempts.
Scores on the K-10 for Aboriginal women were broadly consistent with the diagnostic information generated by the CIDI, indicating a degree of consistency between the two measures. This also suggests that the K-10 may be a valid instrument to use in Aboriginal populations.
Despite the minimal difference in the prevalence of mental disorder between Aboriginal and non-Aboriginal prisoners, the demand for mental health care in the NSW prisoner population, per capita, significantly exceeds that of the general population and demands multidisciplinary and culturally appropriate treatment interventions.
Given the significance of mental illness in prisoner populations it is essential that reliable indicators be collected to monitor trends in mental disorder, and to evaluate the effectiveness of interventions and diversion programmes aimed at deflecting those with a mental illness away from prison and into treatment. The development of mental health indicators at both the State and national level for prisoner populations would enable the effectiveness of these programmes to be monitored in both Aboriginal and non-Aboriginal populations. They would also serve to call attention to the extraordinarily high level of mental disorder in prisons and ensure equitable resource allocation.
Footnotes
Acknowledgements
We wish to thank the nurse interviewers for their determination: David Cain, Dale Owens, Chris Muller, Lee Trevathan, Michael Harris, Alison Lee, Peter Sadler, Rebecca Gibson, and Eli Baxter. We wish to thank the NSW Department of Corrective Services for providing custodial staff to assist with retrieving inmates, particularly Mr Brian Kelly from the MRRC, and Ms Lee Downes from Mulawa. We also wish to thank all the participants for their valuable contribution to this project.