
Abstract
Objective
To provide analysis and commentary on Australian state/territory child and adolescent mental health service (CAMHS) expenditure, inpatient and ambulatory structure and key performance indicators.
Method
Data from the Australian Institute of Health and Welfare and the Australian Bureau of Statistics were descriptively analysed.
Results
Between 2015–16 and 2019–20, overall CAMHS expenditure increased by an average annual rate of 3.6%. Per capita expenditure increased at a higher rate than for other subspeciality services. CAMHS admissions had a higher cost per patient day, shorter length of stay, higher readmission rate and lower rates of significant improvement. Adolescents aged 12–17 had high community CAMHS utilisation, based on proportion of population coverage and number of service contacts. CAMHS outpatient outcomes were similar to other age-groups. There were high rates of ‘Mental disorder not otherwise specified’, depression and adjustment/stress-related disorders as principal diagnoses in community CAMHS episodes.
Conclusions
CAMHS inpatient admissions had lower rates of significant improvement and higher 14-day readmission rates than other ages. Australia’s young population had a high outpatient CAMHS contact rate. Evidence-based modelling of CAMHS providers and outcomes may inform future service improvement.
Keywords
Mental health problems are common in Australian children and adolescents.
1
Between 2017 and 2021, the percentage of Australians aged younger than 18 decreased, with the sole exception of the 10–14 age-group (Figure 1).
2
Young people face significant challenges including academic stressors, housing and family instability.
3
In 2013–14, a national survey showed that 13.9% of Australians aged 4–17 had a mental disorder in the preceding 12 months.
4
ADHD was the most common, affecting 7.4% of the young population, followed by anxiety disorders (6.9%), major depressive disorder (2.8%) and conduct disorder (2.1%). A recent meta-analysis found an average of 44% of children and adolescents with mental disorders received services in high-income countries.
5
In this context, the 2021 National Children’s Mental Health and Wellbeing Strategy (NCMHWS)
1
recommended increased funding for public Australian child and adolescent mental health services (CAMHS). Age of Australian young people as percentage of total Australian population between 2017–2021 and 2017–2021.1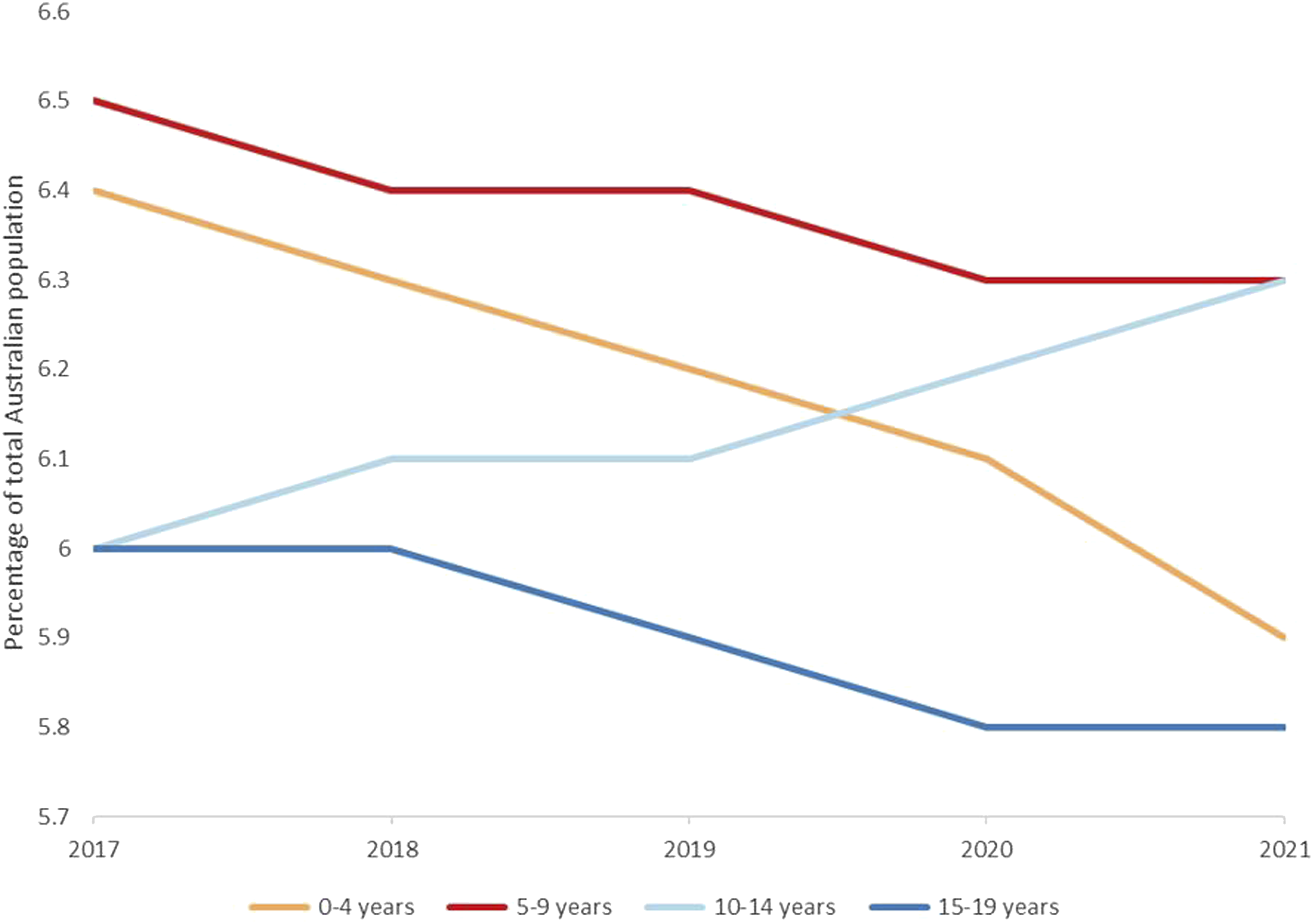
We investigated recent trends for Australian CAMHS inpatient and ambulatory services, expenditure and key performance indicators (KPIs) prior to the NMCHWS. We examined the most recent CAMHS data (2019–20) to establish current services and outcomes. We also examined a 5-year period between 2015–16 and 2019–20, to allow future research to comment on the effect of the NMCHWS on CAMHS structure and outcomes.
Methods
Description of key concepts used to describe mental health services by AIHW
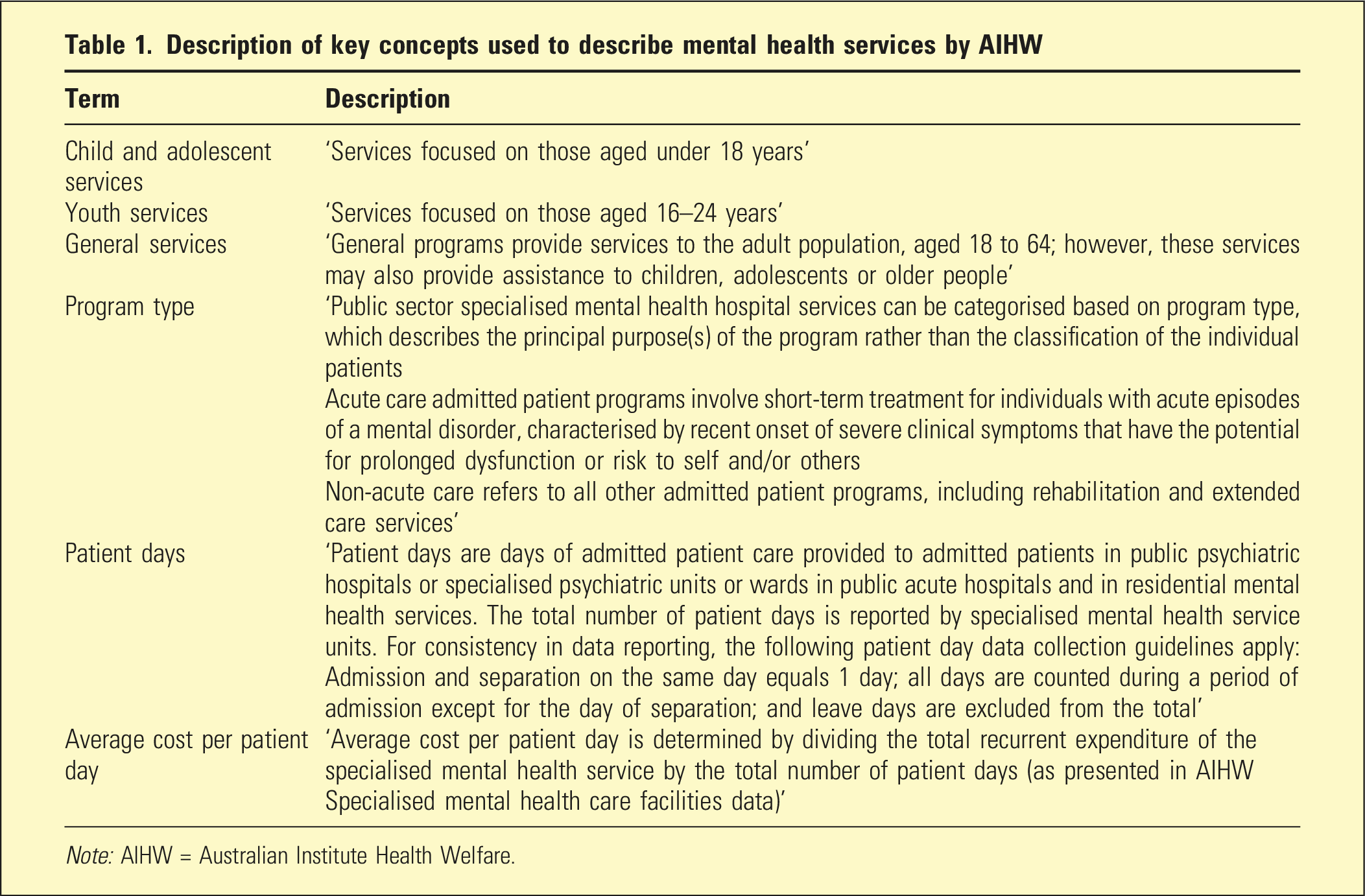
Note: AIHW = Australian Institute Health Welfare.
Results
Expenditure
Total CAMHS expenditure increased by an average annual rate of 3.6% between 2015–16 and 2019–20. Acute CAMHS expenditure increased by an average annual rate of 4.5%, whereas expenditure on non-acute CAMHS, including rehabilitation and extended care services, decreased by 4.9% during this time period. Per capita expenditure on Australian CAMHS increased at an average annual rate of 2.2% between 2015-16 and 2019–20, which was higher than the 1.1% increase for general adult and the 1% decrease for older persons services. This was less than the increases of 3.6% and 13% for forensic and youth services, respectively (Figure 2). Average annual change (%) in per capita Australian public mental health service expenditure between 2015–16 and 2019–20 by service target population.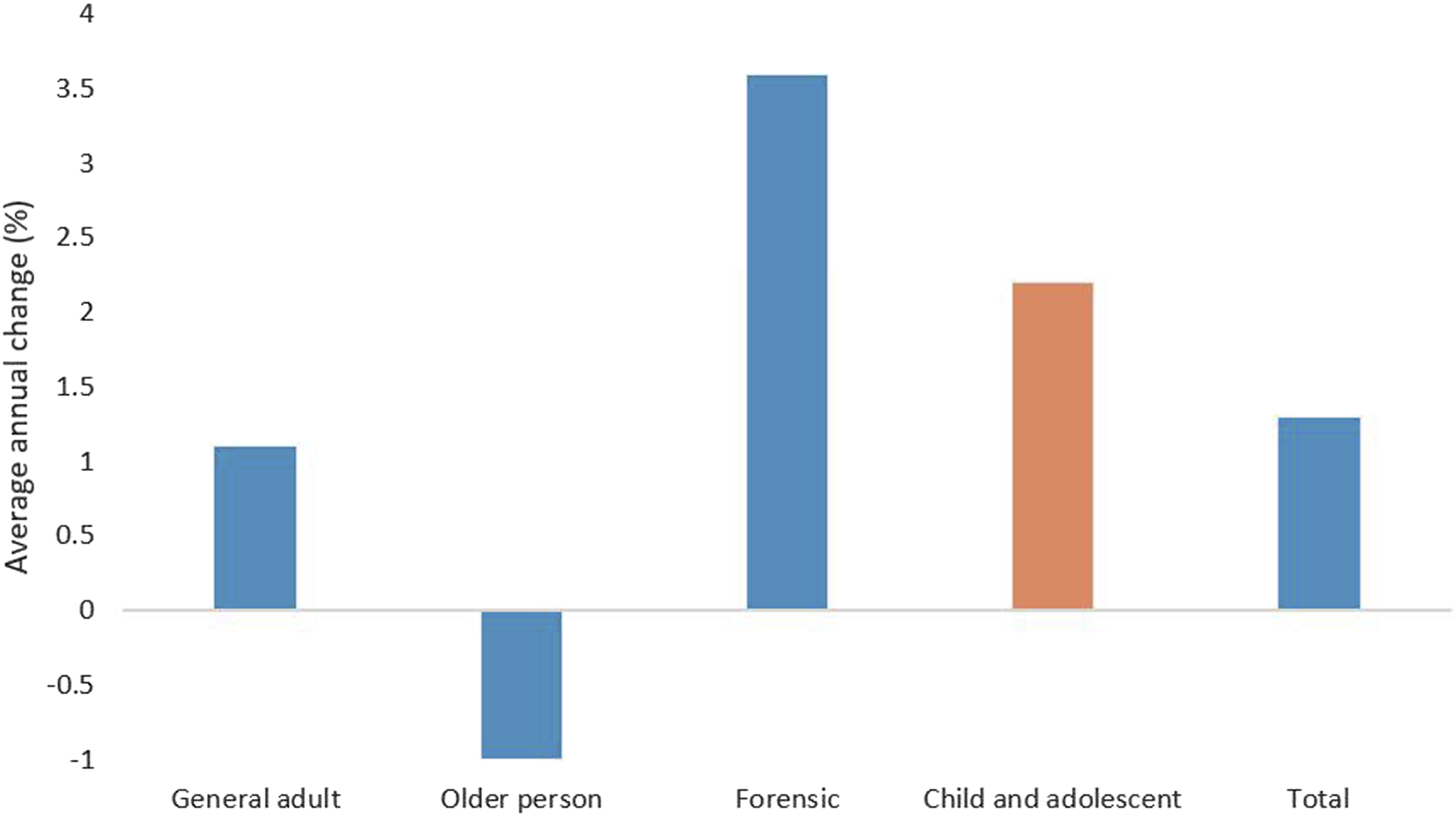
Inpatient
Australian public hospital psychiatric bed numbers per 100,000 population by service target population over time
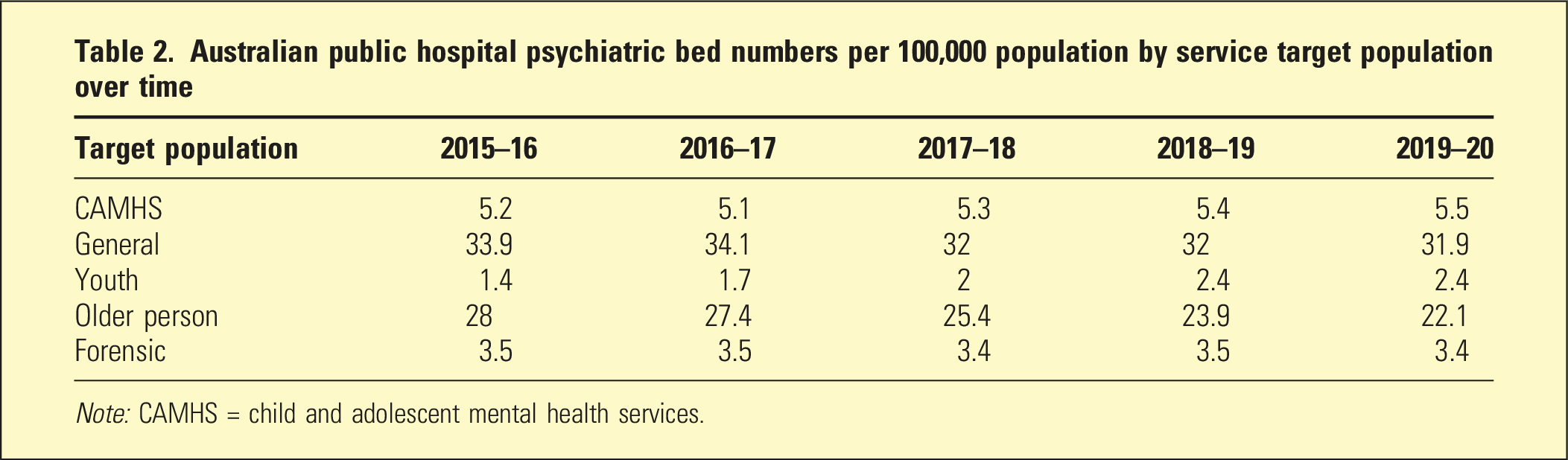
Note: CAMHS = child and adolescent mental health services.
The number of Australian public hospital CAMHS beds increased by an average annual rate of 3% between 2015–16 and 2019–20, a rate higher than general adult (−0.2%), older persons (−2.6%) and forensic (1.3%), but less than youth (15.2%) beds (Figure 3). Average annual change (%) in per capita Australian public hospital mental health bed numbers by target population between 2015–16 and 2019–20.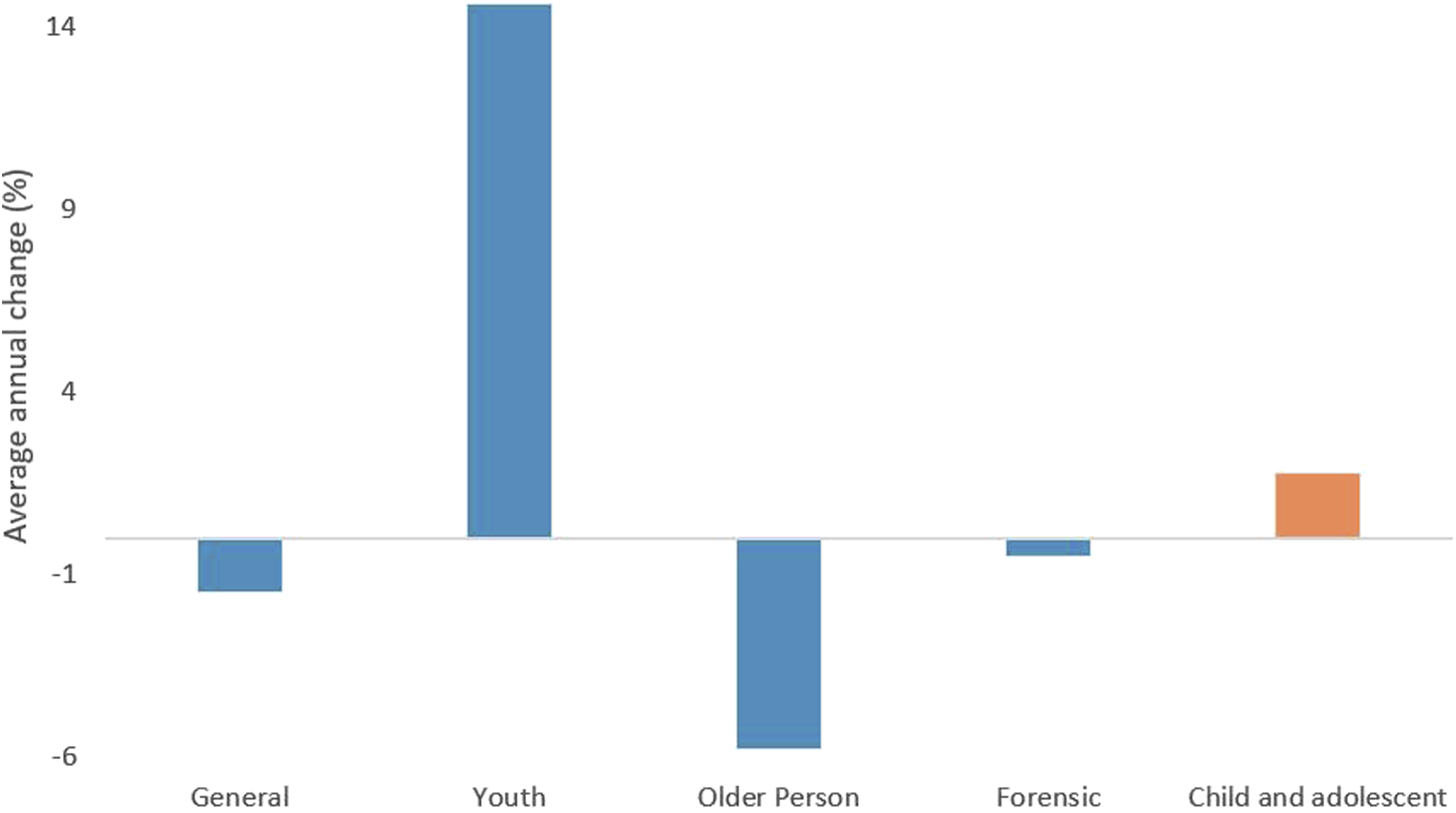
Ambulatory/community
Children aged 0–4-year-olds (0.2%) and 5–11-year-olds (1%) had the lowest and second lowest proportion of total population seen by community MHS, respectively, whilst adolescents aged between 12–17 had the highest proportion of (3.4%) across all age-groups.
Children under 12 years had a low community CAMHS contact rate per 1000 population in 2019–20, with 15.7 contacts for 0–4-year-olds, and 129.5 for 5–11-year-olds. This increased for adolescents, with 12–17-year-olds having a rate of 673.5-per-1000 population, the highest of all recorded age-groups. Between 2015–16 and 2019–20, the community CAMHS contact rate for 12–17 years increased by 4.9%, a larger average annual change than for 5–11 years (0.1%) and 0–4 years (−0.9%) or any other age-group.
2019–20 Five most commonly reported principal diagnosis for Australian community CAMHS contacts by age-group
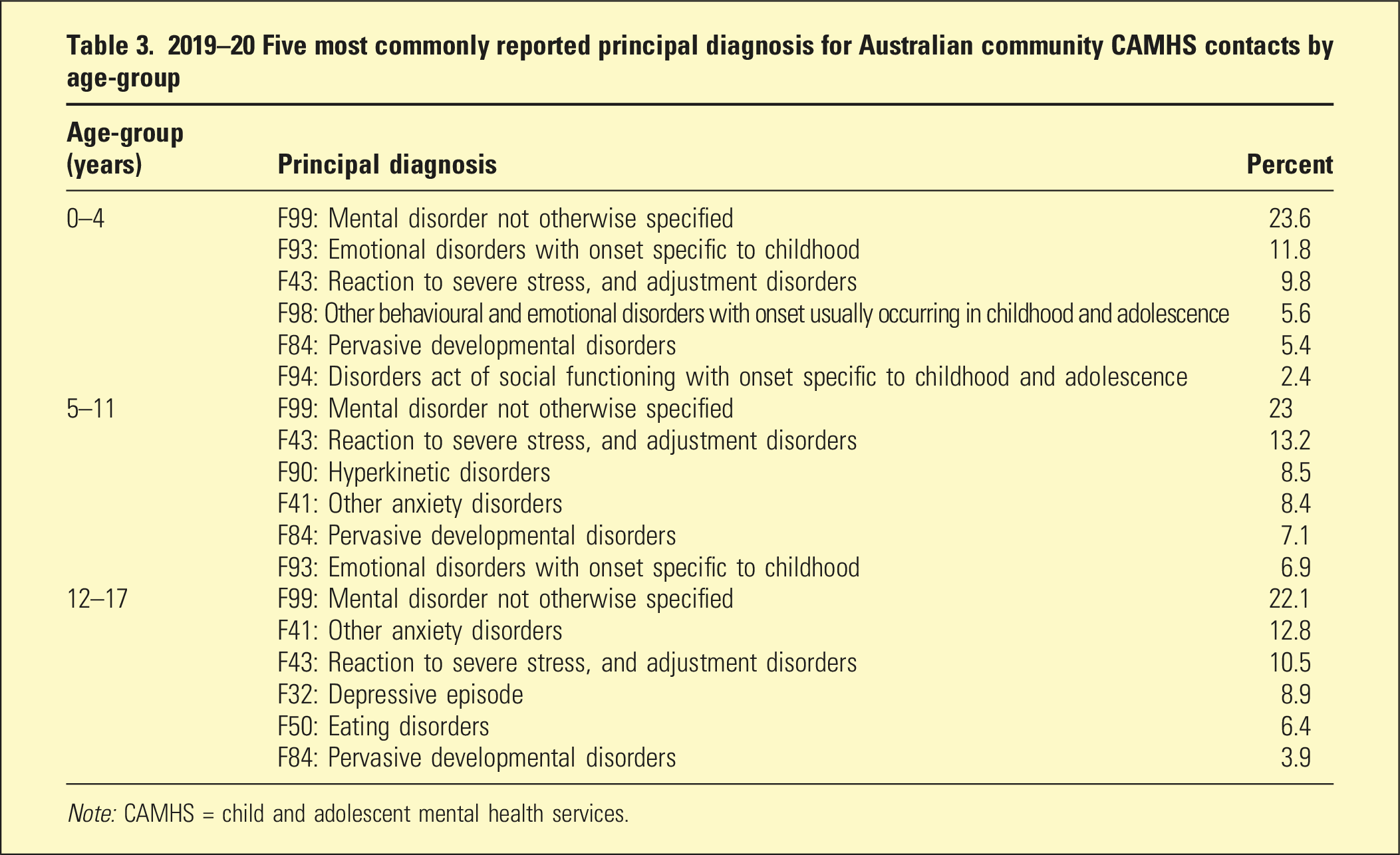
Note: CAMHS = child and adolescent mental health services.
Rate per 1000 population of principal diagnosis of community MHS contacts in 2019–20 by age-group and disorder type
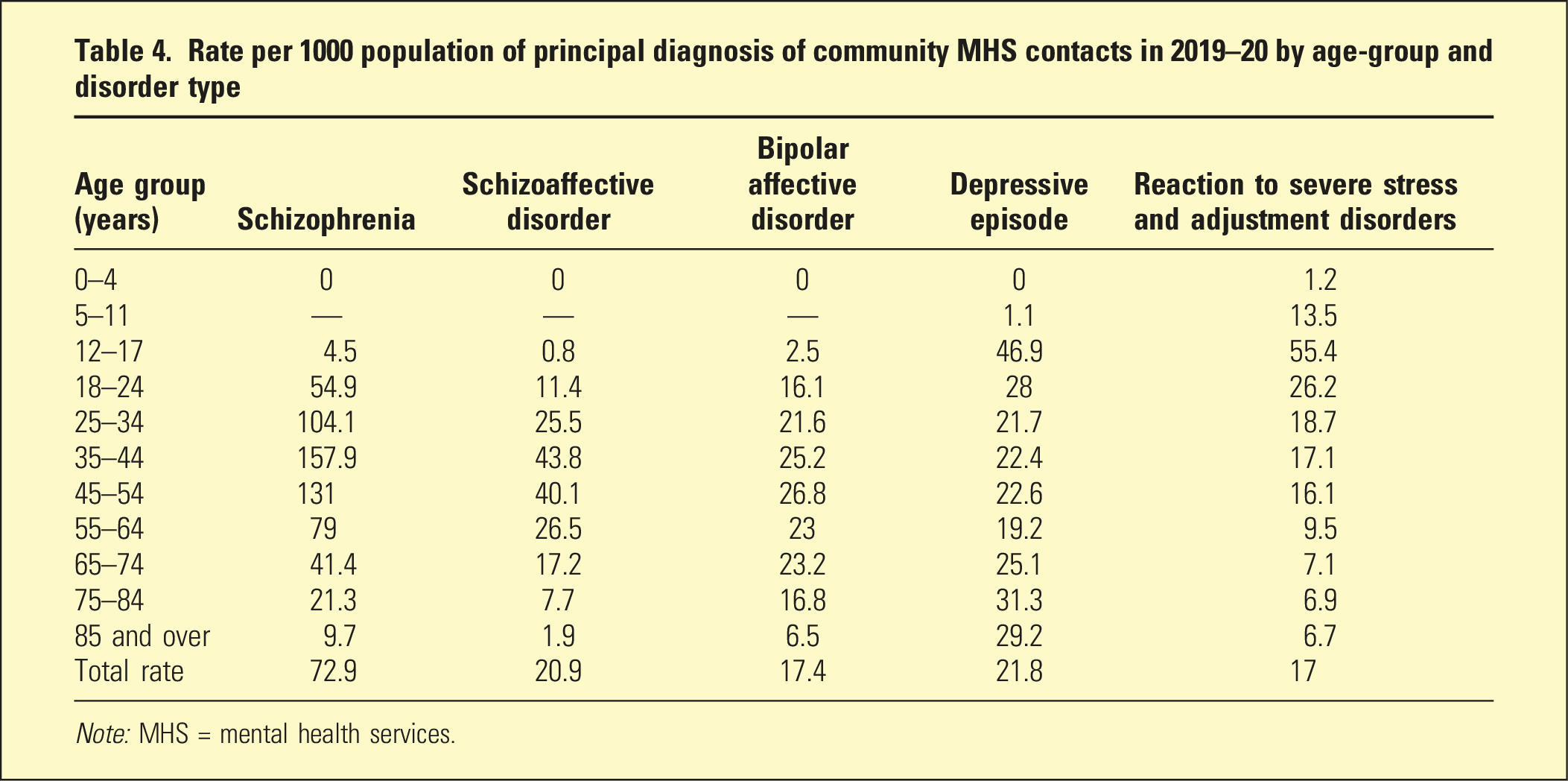
Note: MHS = mental health services.
Most recent outcome measures
In 2019–20, 57.7% of Australian public CAMHS patients reported significant improvement after an admission, which was less than the 72.2% for the total population. CAMHS admissions had higher rates of no improvement after an inpatient episode (32.8%), compared to all ages (22.9%). The average length of stay (LOS) for CAMHS inpatient episodes was 8.8 days, compared to 11.7 days for general adult and 35.1 for older persons admissions. CAMHS had a 21-day public hospital readmission rate of 19.5%, higher than older persons (7.6%), forensic (13.2%), general adult (14.9%), but less than youth (22.6%) services. The average cost per acute admitted patient day was AUD$2553 for CAMHS, higher than the AUD$1342 for general adults, AUD$1444 for forensic-patients and AUD$1158 for older persons.
52.4% of CAMHS patients reported significant improvement after a completed ambulatory episode in 2019–20, compared to 50.7% for all ages. CAMHS also had rate of significant deterioration after a completed outpatient episode of 5.7%, in comparison with 6.4% for all ages.
Discussion
Despite a decrease in the proportion of Australians aged less than 18 years, per capita CAMHS expenditure increased at a relatively higher rate in comparison to all other MHS. Our descriptive analysis shows that inpatient CAMHS had the highest cost per patient day, with a lower rate of significant improvement, and a higher rate of no improvement after an episode.
These findings could be due to increased complexity in treating young people, for example, managing familial discord. 7 Perhaps young people are receiving longer admissions for conditions that do not necessarily respond well to inpatient treatment, such as mental distress from personality related factors, abnormal illness behaviour, bullying and child protection issues around placement. This requires further research as to the reasons for these possible care effectiveness shortfalls.
CAMHS had relatively low per capita bed numbers and LOS compared to other populations, possibly due to lower rates of more serious mental illnesses and higher rates of conditions that do not require prolonged inpatient care. Young people may have greater at home family/carer support compared to some other age-groups, perhaps reducing the requirement for inpatient care.
Australians aged 12–17 had relatively high outpatient MHS utilisation (proportion of total population seen and service contacts), and rates of depression and adjustment/stress-related disorders. The cause of this is likely multifactorial, with social media and smartphones 8 implicated as having a negative effect on youth mental health. Certain scenarios common in CAMHS such as weight-monitoring in anorexia nervosa require frequent contact and so may artificially inflate the contact rate. Perhaps the trend to broader, and less well-defined mental health and illness concepts, 9 as well as prominent youth mental health advocacy are also factors in these extremely high service utilisation rates. Broadly the high contact rates could also possibly relate to a small proportion of adolescents being seen at high frequency, inflating total contact rates for this age-group.
MD-NOS was the most common outpatient principal diagnosis for all age-groups. This may be due to increased diagnostic complexity in young persons, limitations in diagnostic manuals and/or a reluctance to diagnose due to fear of inducing stigma. 10
Limitations
Australia has many health services with differing structure and AIHW data may not accurately represent regional MHS funding and utilisation. Headspace consumers access MBS reimbursements, but there’s no reported data available from AIHW or other sources.
Adolescents cared for by other providers such as paediatric, general adult or youth mental health services were not reported. Adolescent inpatients are possibly being cared for in other settings, such as within youth mental health, paediatric or general psychiatric wards and so were not captured in the AIHW data. Further studies should examine workforce, models of care and other data collected by the Australian Mental Health Outcomes Collection Network. It would also be useful for the AIHW to provide a nomogram of service contact rates to determine if the high contact rates in CAMHS could be related to a small number of consumers being seen at extremely high frequency.
Future
We recommend evidence-based modelling of Australian CAMHS, as well as organisations such as headspace, and the private sector, to inform policy and system reform. 11 Advocacy should be focused on how effective, outcome-based, services can be implemented. Collection of real-time, real-world data could inform CAMHS how to better improve outcomes. 12
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.