
Abstract
One in five people experience clinically relevant mental health problems before the age of 25 years. Furthermore, in Australia, one in seven children are reported to experience a mental health disorder. Consequently, there has been a steady increase in demand for mental health services for children and young people, and this has been compounded by the COVID-19 pandemic. Unfortunately, currently many children and young people with mental health difficulties are not accessing appropriate and/or timely care, with individuals and families finding it increasingly difficult to access and navigate suitable services. In part, this is related to the fragmented and isolated manner in which child mental health services are operating. To address the current issues in access to appropriate child and adolescent mental health care in Australia, a novel Integrated Continuum of Connect and Care model is proposed to integrate relevant services along a tiered care pathway. The aim of this model is to facilitate timely access to mental health services that meet the specific needs of each child/young person and their family. This model will function within co-located service hubs that integrate health care through a comprehensive assessment followed by a link up to relevant services. The Integrated Continuum of Connect and Care has the potential to pave the way for unifying the fragmented child and youth mental health system in Australia.
Most mental health conditions (MHCs) start before the age of 25 (Colizzi et al., 2020) and continue into adulthood (World Health Organisation (WHO), 2014). However, Australia’s mental health system has been struggling to provide adequate level of care to children and adolescents early in life and early in illness. The Royal Commission into Victoria’s Mental Health System (2021) highlighted that demand for services has outpaced supply, a factor further compounded by the COVID-19 pandemic (Tedja et al., 2022). There is also a ‘missing middle’, of those with MHCs that are ‘too severe’ for primary care but not ‘severe enough’ for specialist services, that are finding it particularly hard to access and navigate suitable services. Furthermore, children under 12 years of age and with psychosocial difficulties who often require an array of services spanning various agencies and sectors (e.g. mental health, physical health, education and juvenile justice), are particularly finding that the system is unresponsive to their needs (Royal Commission into Victoria’s Mental Health System, 2021). Indeed, connecting services can be an additional challenge (Australian Medical Association, 2018). An integrated system comprising clinical services coordinated effectively including through digital platforms, with wrap around care comprising education and social care services is critically needed. This article will review the current state of the child and adolescent mental health care system in Australia and reflect on how best to assist children and adolescents with MHCs to access the right care at the right place and time.
Fragmented, isolated and discontinuous care as a contributory factor
There are a number of factors that have contributed to the fragmented nature of services, including different funding sources, structural, geographic, socio-economic and cultural factors. This has resulted in an array of services across settings such as private, government-led federal and state and non-government organisations (NGOs; Mental Health Australia, 2020). While a range of services across settings can help meet a broad range of needs, it can also result in duplication and poorly co-ordinated and inequitable service distribution. This worsens inequity in access to services with an ‘inverse care law’, where families with greater disadvantage who are at higher developmental risk, and therefore could potentially benefit most from intervention, are less likely, and indeed less able, to seek and access help early and engage in services (Eapen et al., 2017). Furthermore, as the number of service providers required by families with complex needs increases, the intersections between services and service coordination also becomes challenging (Koren et al., 1997).
Comprehensive assessment, referral pathways and models of care
One of the first ports of call in ensuring that children are receiving the support most suited to their needs is the assessment process facilitating early and accurate identification of MHCs. In line with this, the Australian Department of Health has established the National Initial Assessment and Referral (IAR) for Mental Healthcare Guidance to assist General Practitioners, intake teams, providers of initial assessments and Primary Health Networks to operationalise the factors clinicians need to consider when determining which services are most appropriate for those seeking mental health assistance (Australian Government Department of Health, 2019). This tool draws on all information available, including clinical interviews and information gathered from the person’s family, referrers and other sources with four primary domains – symptoms severity and distress, risk of harm, functioning and impact of co-existing conditions. It also has four contextual domains – treatment and recovery history, social and environmental stressors, family and other supports and engagement and motivation. Based on the assessment, the tool uses a five-level schema to conceptualise the complexity of the MHCs of the person, providing a framework to guide the referral process, with the following levels: level 1 – self management; level 2 – low intensity services; level 3 – moderate intensity services; level 4 – high intensity services and level 5 – specialist and acute services. Such an assessment can guide clinicians in determining the most appropriate level of support for a child and family in their care.
The second critical aspect is that young people with complex presentations are most effectively managed through integrated and multidisciplinary services (Colizzi et al., 2020). In this regard, social determinants of health are emerging as key factors that need due consideration and hence models that integrate health care with social care using a ‘wraparound process’ are increasingly receiving attention. This process involves developing, implementing and monitoring holistic care including attention to social determinants of health. Here a social worker or a service navigator facilitates the process for the four phases of engagement, plan development, implementation and transition from service. A meta-analysis examining the efficacy of such a system found medium-sized effects for costs, residential outcomes and school functioning, while small effects were found for mental health symptoms (Olson et al., 2021).
A third critical factor in effective health care models is managing the supply and demand gap in the availability of mental health specialists, and a model of care that can assist young people presenting with MHCs and their families to access mental health care through integrated services (Dillon-Naftolin et al., 2017). The goal here is to address limitations in the current care system by building capacity and confidence in primary and community care providers through facilitating partnerships with mental health specialists for delivering mental health care. Indeed, a number of studies have demonstrated positive effects for integrated care models (see Asarnow et al., 2015; Kolko et al., 2014; Richardson et al., 2014).
Resource constraints in scale and skill sets
Worldwide, many young people do not access treatments and there is a gap between prevalence and treatment rates such that only 25%–35% of affected children and adolescents access treatment (O’Brien et al., 2016). In Australia, it is reported that, of those with a severe mental health disorder over a 12-month period, only 27% had seen a psychiatrist (Commonwealth of Australia, 2015) suggesting a continuing significant unmet need for specialist Child and Adolescent Mental Health Services (CAMHS) for these young people. Furthermore, the gap between availability of specialist mental health professionals catering for young people’s MHCs and the demand for these services has been widening. As an example, Mulraney et al. (2020) noted an average wait time of 41 days for psychiatrists and 34 for psychologists in Victoria and South Australia between March and May 2019. Furthermore, for individuals who do receive help this is often delayed or insufficient in frequency or duration (Tully et al., 2019). This issue is particularly problematic for those living in rural and remote Australia, with a recent Senate Community Affairs References Committee inquiry finding that those living in rural and remote Australia access mental health care at a much lower rate than those in metropolitan areas (Commonwealth of Australia, 2018). This has been further worsened by the Covid-19-related increase in child and adolescent mental health presentations in the Emergency Department and admissions (Hu et al., 2022). Hence, despite the development of effective treatments, traditional models of care are not meeting the psychiatric needs of young people, which in turn is increasing the overall burden of mental illness across the lifespan (Dillon-Naftolin et al., 2017). Reducing barriers to help-seeking, such as out of pocket expenses and prolonged waiting times is critical for effective service delivery (Reardon et al., 2020). Therefore, it is imperative that alternate models of care are identified and implemented that includes capacity building at all service levels. There are various ways in which such skills building can be structured. A method that would be particularly suitable to the Australian context, where there is a significant gap in the availability of child and adolescent mental health specialists, is that of a ‘community of practice’ model. Here, a multidisciplinary team of mental health professionals, including a child and adolescent psychiatrist, consult on cases identified by primary or secondary care physicians or other health professionals. One such example of capacity building is a telehealth Project Extension for Community Healthcare Outcomes (ECHO) model established for primary care physicians in rural areas to have access to consultation with specialist physicians located in urban settings (Carrol et al., 2016). This could also be used to support primary health physicians working with children with MHCs in urban areas through case-consultation with specialists. Indeed, the Project ECHO model has already been implemented to bridge service gaps in the provision of adequate support for mental health needs in Australia and overseas (e.g. Chand et al., 2014; Moss et al., 2021). Extending such programmes to provide primary and secondary care providers (e.g. GPs, general paediatricians, school psychologists) the opportunity for consultation and capacity building with child and adolescent mental health specialists could be operationalised via a Community of Practice (CoP) programme. In this programme, community-based health professionals have opportunities for case-based discussion via a multidisciplinary specialist panel using an online conferencing platform. The aim of such a programme is to provide primary (e.g. general practitioner [GP]) and secondary (e.g. Paediatricians) care providers with pragmatic, timely and actionable advice that can be implemented by the practitioner to allow them to manage their patients themselves. Following the panel discussion, a management plan will be constructed, and used to consider recommendations and care facilitation as needed. Such a model will provide a means by which to mitigate the current gap in the availability of child and adolescent mental health professionals/services. This interdisciplinary collaborative model (examples include COMPASS in Victoria and Mind Link in NSW; personal communication) can help overcome the current structural barriers to integrated care while also providing equitable access to quality care for young people with complex MHCs.
Outcomes framework
It is important for mental health services to have specific goals in relation to mental health outcomes. Specifically, the impact of MHCs reaches beyond symptom severity alone. This is particularly evident when mental ill-health can impact a number of aspects of life, including education, social relationships and employment (Iorfino et al., 2019). Thus, it is important to consider broad outcomes of service provision, as opposed to a narrow focus on clinical symptoms. As an example, Iorfino et al. (2021) propose five domains that make up an outcomes framework that captures the specific needs of young people presenting with MHCs: social and occupational function, self-harm, suicidal thoughts and behaviours, substance misuse, physical health and illness type, stage and trajectory. A focus on outcomes relevant to the social and emotional wellbeing of young people, allows for a broader consideration of the patient’s needs, as well as a broader scope by which to measure efficacy of service provision. Finally, the Productivity Commission report (2020) has recommended continuity of care and co-ordination between services as critical elements in service delivery.
Taking into consideration these factors, we propose an Integrated Continuum of Connect and Care (I-CCC) model to achieve this (Figure 1). Such a model aims to integrate services along a tiered care pathway and facilitate timely access to services commensurate with needs. Within this model, co-located service hubs that integrate a comprehensive assessment framework by appropriately trained professionals with matching services according to the level of need could promote service co-ordination across different healthcare providers and education, social services, disability support and so on. As engagement with some of the most vulnerable families can be challenging, evidence-based strategies to improve service engagement is also critical using the I-CCC principles of a ‘no wrong door’ entry to services, a ‘triage and review’ system with a quick link up and a ‘warm handover’ to ensure uptake of recommendations through service co-ordination and system navigation. This will also include pregnant women and preschool children in the ‘first 2000 days’ of life offering the earliest opportunity to positively influence the long-term trajectory of the child. The model is intended to address the current fragmentation of mental health provision through offering a seamless care pathway starting with an in-person or digital ‘front door’ entry and assessment using the IAR framework followed by a tiered model of care (see Figure 2). Following triage, those deemed suitable for online support will be offered options for online resources and/or programmes as required, such as those referred to in the Head to Health Kids National Service Model (Australian Government Department of Health, 2022). Children whose needs are deemed to be at levels 3 or above on the IAR and with complex psychosocial needs will be assigned a service navigator (Tier 4), to ensure that the young person and their family can access relevant supports (see Honisett et al. (2022) for evidence regarding improved health outcomes as a result of hub-based case management]. The presence of an appropriately trained assessment team as well as a social worker to support complex social care needs via service navigation in the I-CCC model will allow for efficient use of resources, including intake processes and provision of better targeted referrals, thereby mitigating current issues of poor continuity of care and after-care identified in specialist CAMHS teams (Government of Western Australia, 2022). These services will be offered in close collaboration with specialist services, out of home care, non-government services, early learning/education providers and priority population focussed services such as Aboriginal and Out of Home Care services and will include pharmacological and non-pharmacological interventions, trauma informed services, allied health and disability support, developmental and physical health services, parenting/family services and so on. Those at Level 5 of the IAR will need referral to emergency department, in-patient and specialised services (e.g. eating disorders, suicide, drug and alcohol, forensic services). There will also be provisions for the service navigator to facilitate a step-up or step-down between mild- to high-intensity services depending on the changing needs of the young person. Moderate-high intensity services (Tier 3) could be offered to those at Levels 3–4 while those assessed as Levels 1–2 on the IAR could be referred to low-intensity services depending on their needs (Tier 2). According to the Australian Institute of Health and Welfare (2021) report on the impact of mental illness, among young people aged 12–17 years old with mental health disorders, the severity of the impact was mild for 44%, moderate for 33% and severe for 23%. Therefore, it is expected that approximately 44% of young people with mental illness will be offered Tier 2 services, while the remainder will be offered either Tier 3 or 4 services. The key point to note, however, is the current resource constraints that would prevent seamless referral, which the model will address by efficient triage and referral to appropriate services, service navigation for complex cases and community of practice that will increase the capacity of primary/secondary care providers to respond to MHCs.
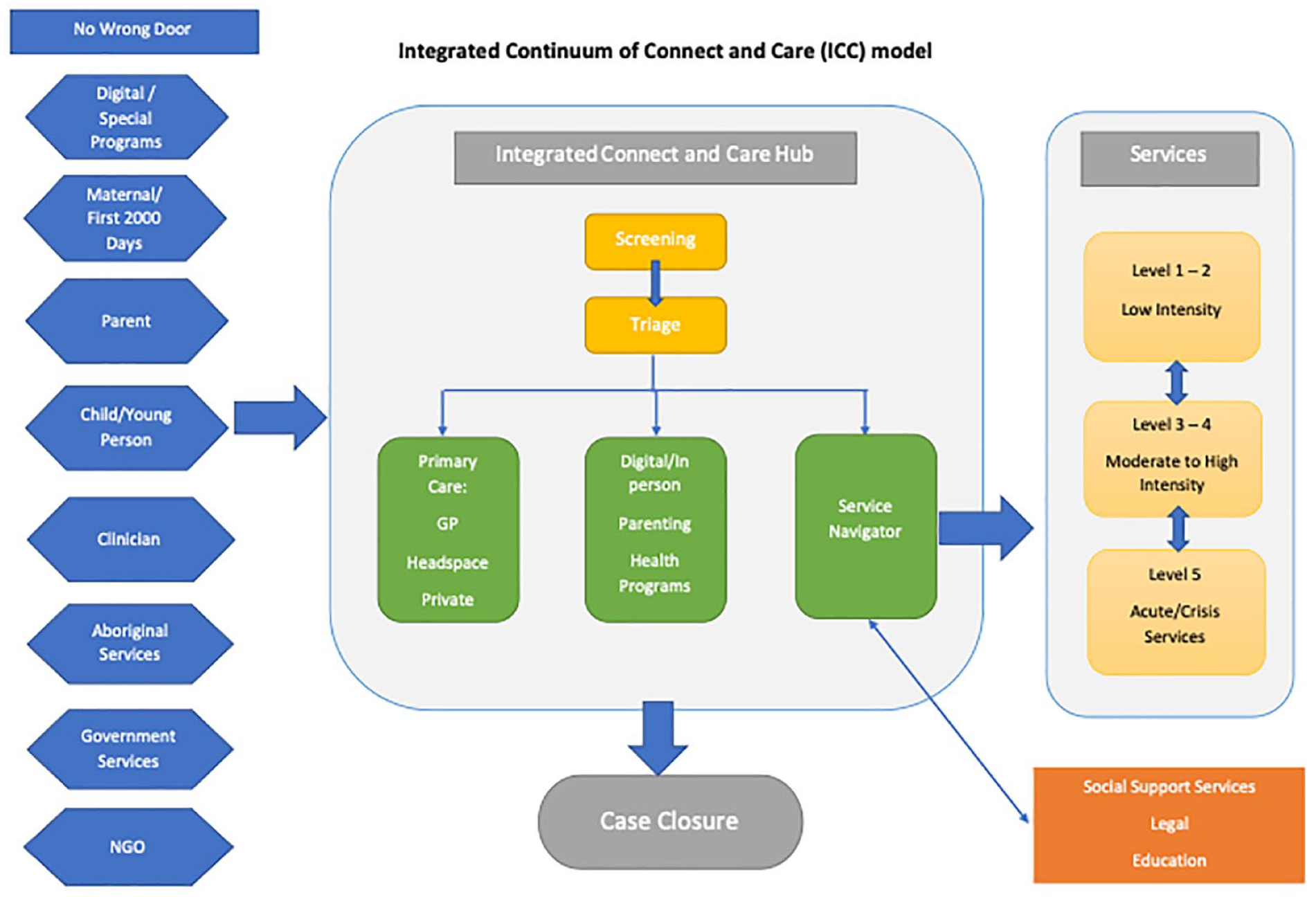
Schematic of Integrated Connect and Care Model. In this model, families enter the Head to Health hub through a range of pathways, including an electronic platform used to monitor child development (Watch Me Grow-Electronic), or through various service providers (with a no wrong-door policy). In the Integrated Care and Connect Hub, parents and children/youth will be screened and referred to a specific care pathway based on their needs, this may include support in the Integrated Care and Connect Hub itself as well as linkages with external services including a combination of primary, secondary and tertiary care. This model of care can be adapted to fit specific communities, including rural and remote communities, with services tailored to suit the needs of the community that the hub services.
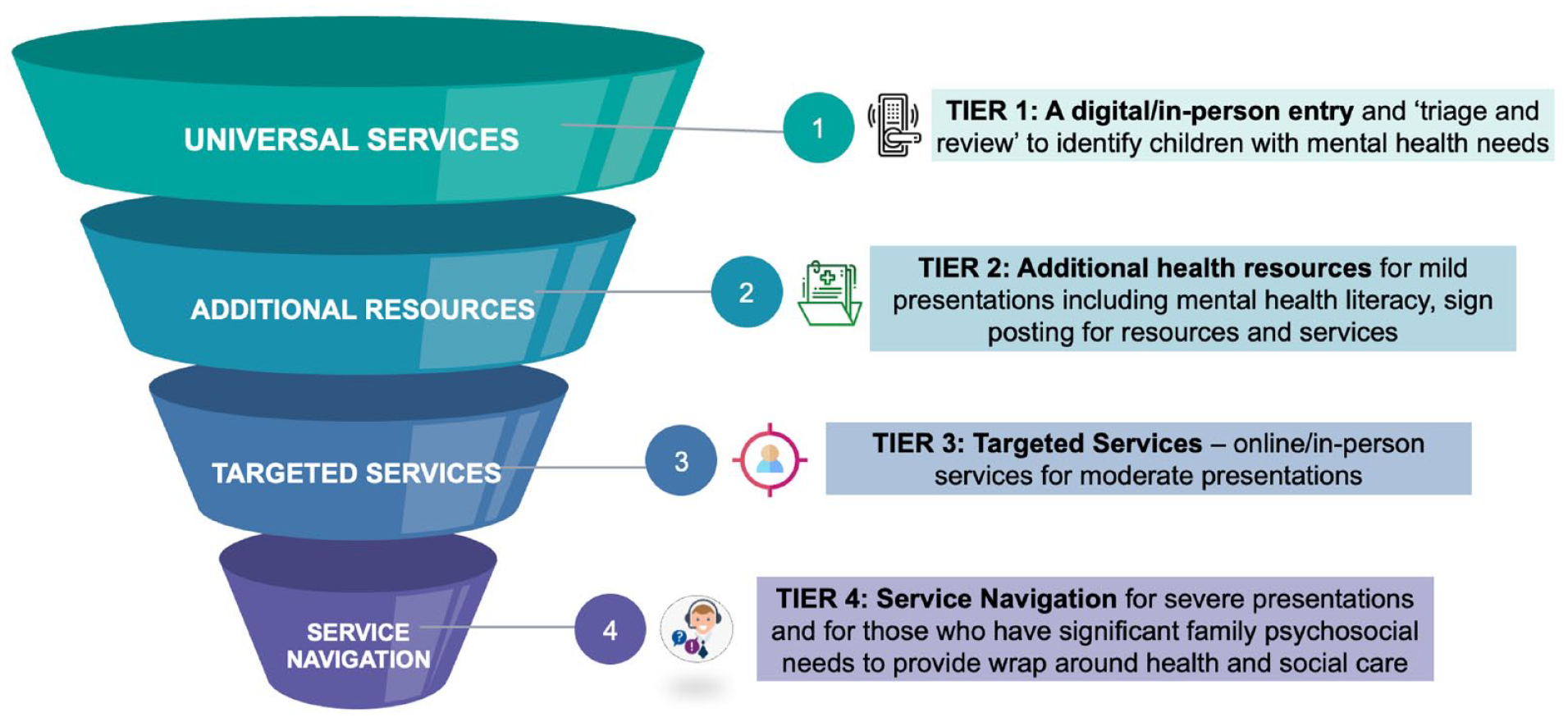
Tiered model of care: Integrated Continuum of Connect and Care (I-CCC).
The establishment of the Head to Health Kids Hubs (15 across the country; Federal Budget; Australian Government Department of Health, 2022) jointly by state and federal government offers a unique opportunity to implement the I-CCC model. Each hub comes with a multidisciplinary staff establishment that will allow innovative service provision including a hub and spoke model. This will allow for ‘digital front door’ and ‘community of practice’ functions, as well as comprehensive assessment and formulation, which in itself could provide therapeutic benefits, particularly when underpinned by principles of motivational interviewing (Dean et al., 2016) and trauma-informed and also strengths-based approaches such as the HOPE framework (Burstein et al., 2021). Furthermore, the use of single-session therapy (Young et al., 2012) will allow engagement and focussed immediate support while waiting for further referrals. The linkages will be critical including all mental health providers in the community (headspace, private and NGOs), thereby providing a ‘warm handover’ and seamless continuity of care. It will be important to co-develop, implement and evaluate the I-CCC model with Aboriginal representatives while implementing in specific contexts, and as new versions are created. It should also be noted that while the I-CCC model shares some aspects of other tiered models of care (e.g. the National Health Services’s (NHS) tiered model of Mental Health Care; Healthy Young Minds in Herts, 2022), this model is unique in that it allows for coordination of care via co-located service hubs with referrals as per level of need. This model will address a number of the Royal Commission into Victoria’s Mental Health System (2021) recommendations for young people via a responsive service system with integrated support comprising comprehensive assessment and matching therapeutic services, wellbeing supports, care co-ordination and continuity of care.
This I-CCC model will have a strong focus on tracking outcomes including identifying those who are not improving so as to link them in with intensive or potentially more suitable forms of care. The model will also have telehealth options for reaching geographically disadvantaged communities. This will also ensure that those living in rural and remote communities have access to ‘timely, affordable and quality health services’ (National Strategic Framework for Rural and Remote Health (Australian Government Department of Health, 2016). The performance of the I-CCC will be measured using implementation indicators of Patient Reported Experiences Measures (PREMS) and Patient Reported Outcome Measures (PROMS) as well as administrative data on the rate of referrals accepted from primary to secondary/specialist care.
There is a need to enhance universal services including increasing mental health literacy and reducing stigma alongside bridging the gap between the supply and demand for services via technological innovations and CoP models. The I-CCC model will offer seamless opportunities for step up and transition to specialised services and step down to less intensity services leveraging the CoP network. Finally, care coordination and integration across all levels of care is critical (Iorfino et al., 2021), with smart IT system platforms used for effective data sharing and tracking outcomes. This will ensure measurement-based care, so that those not improving are identified in a timely manner for appropriate action.
Overall, the I-CCC model can pave the way for unifying the fragmented service system in collaboration with health (GPs, paediatricians, psychologists), education and social-care sectors. Provision of coordinated care to children and families along a continuum from primary to specialised services using the principle of ‘proportionate universalism’, i.e., universal services plus targeted care commensurate with needs, is expected to ensure that young people can access timely and appropriate support, allowing them to thrive and reduce the long-term burden of mental illness.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.