
Abstract
Background
Some antipsychotic drugs elevate prolactin, and hyperprolactinaemia is associated with an increased risk of breast cancer. Women with schizophrenia have an increased incidence of breast cancer, but also multiple risk factors for the condition.
Method
This paper will critically review recent epidemiological studies concerning antipsychotics and breast cancer from a psychiatric perspective.
Results
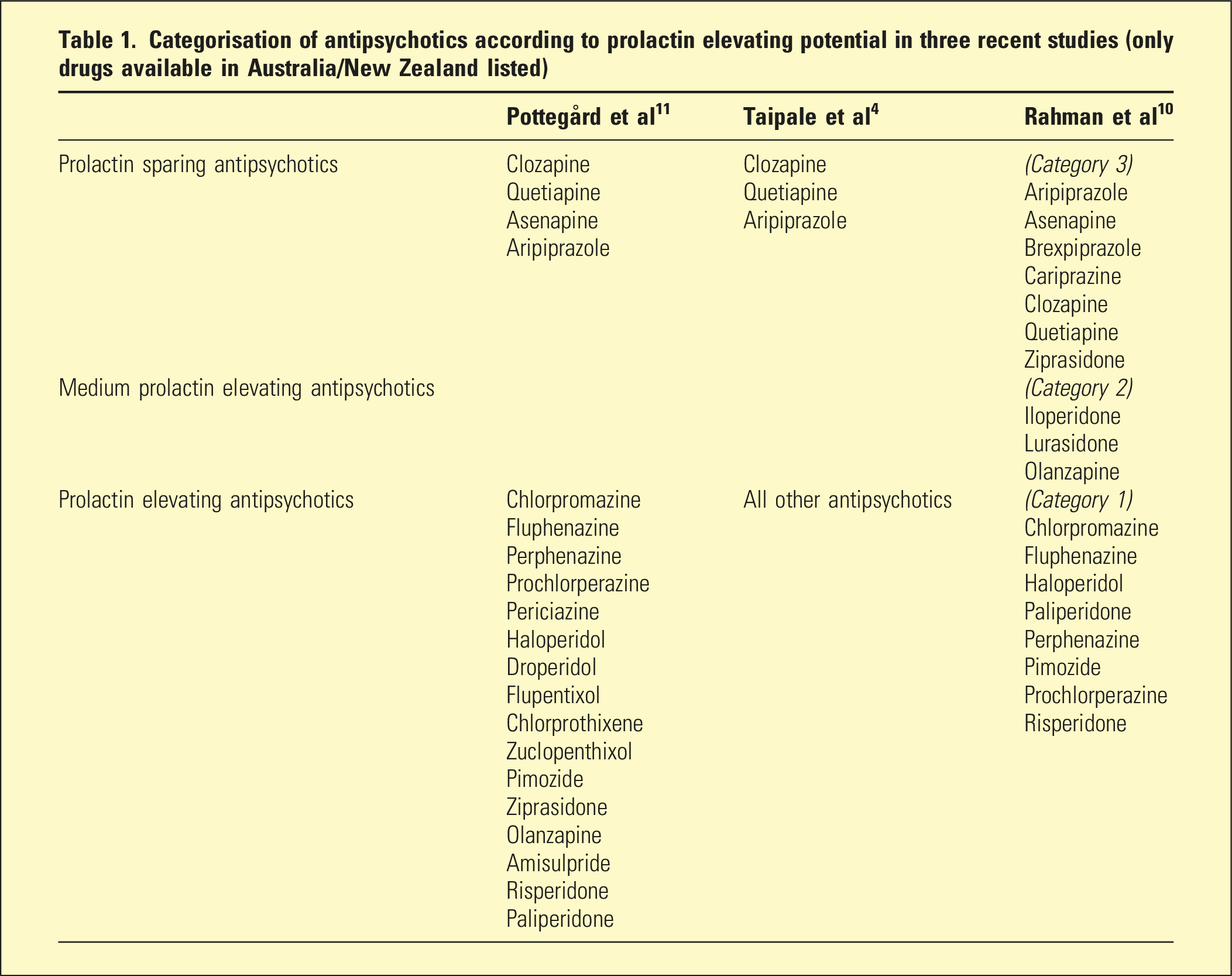
Two recent epidemiological studies have found an association between use of prolactin-elevating antipsychotics and breast cancer in women with schizophrenia and other psychotic disorders. Prolactin-elevating drugs include paliperidone, risperidone, amisulpride and haloperidol, whilst prolactin-sparing antipsychotics included aripiprazole, brexpiprazole, cariprazine and quetiapine. In the two studies, estimated increased risks of breast cancer were disconcertingly high (up to 62%), but a third recent study found only a weak dose-response association. There are extensive methodological complications in this research, including the extent to which studies measure other risk factors for breast cancer and disagreement about the extent of prolactin elevation by some antipsychotics.
Conclusion
Although causation between prolactin elevating antipsychotics and breast cancer in women has not been demonstrated, recent epidemiological reports are worrying. For women on antipsychotics, informed consent should ideally include discussion of breast cancer concerns within the wider context of treatment benefits and risks.
Antipsychotics medications elevate prolactin by blocking the action of dopamine (which inhibits prolactin secretion) via dopamine D2 receptors on the surface of pituitary lactotrophs which reside outside the blood–brain barrier. 1 The effect of antipsychotics is affected by factors including penetration and affinity, but may be so transient with some antipsychotics such as clozapine and quetiapine, that routine tests fail to detect any prolactin elevation. 2 With partial dopamine agonist antipsychotics (aripiprazole, brexpiprazole, cariprazine), effects on prolactin depend on ambient dopamine concentrations, so that at times prolactin can be reduced from baseline as a consequence of drug action. 2 Paliperidone (the first metabolite of risperidone) causes more hyperprolactinaemia than any other antipsychotic (followed in descending order by risperidone, amisulpride and haloperidol). 3
Breast cancer occurs about 25% more frequently in women with schizophrenia than the general female population. 4 Although hyperprolactinaemia is known to increase breast cancer risk in women,5,6 evidence concerning an association between prolactin-elevating antipsychotics (PEAPs) and breast cancer has been unclear. In 2002, a retrospective study of 108,108 women about half of whom had been treated with antipsychotics of all types, found that use of antipsychotics was associated with a 16% increase in risk of breast cancer, with the greatest risk for higher cumulative doses. 7 Other older studies were either negative or equivocal.2,8
A comprehensive 2015 review of the evidence concluded that antipsychotic-induced prolactin elevation was less important for development of breast cancer than risk factors of nulliparity, obesity, diabetes, alcohol, smoking and inactivity. 8 A further 2017 population study of 88,923 women in Taiwan, those who had been treated with risperidone, paliperidone or amisulpride had a 1.94-fold increased risk of breast cancer; however, the study did not control for other risk factors for breast cancer. 9
Since 2018, three large epidemiological studies have been published which examine the risk of breast cancer in women with schizophrenia treated with PEAPs 4 and in women with a range of diagnoses treated with PEAPs.10,11 This paper will briefly and critically review these three epidemiological studies published in the last 5 years and the implications for clinical psychiatric practice.
The evidence
In 2018, a case-control study from the Danish Cancer Registry identified 60,360 women diagnosed with breast cancer between 2000 and 2015, and age-matched each case with 10 female population controls. 11 Parity, obesity and substance use were not controlled. Pottegard et al. 11 reported no overall associations for first- and second-generation antipsychotic classes nor for antipsychotics identified as prolactin-sparing antipsychotics (PSAPs) or PEAPs. A weak association with long term first generation PEAPs was present, and a weak dose–response pattern was seen with cumulative antipsychotic dose exposure to second generation PEAPs. However, the categorization of PEAPs included olanzapine and ziprasidone, while PSAPs included asenapine (which causes higher prolactin elevation than both olanzapine and ziprasidone 3 ), which weakens the comparison. Associations between antipsychotic use and breast cancer were seen for oestrogen receptor-positive and non-localized cancers.
In 2021, Taipale et al. 4 reported a methodologically rigorous study of 30,785 women with schizophrenia, of whom 1069 had developed breast cancer over 17 years. Each case was compared to five controls examining duration of antipsychotic exposure, antipsychotic type and other breast cancer risk factors. PSAPs (clozapine, quetiapine, aripiprazole) were compared to all other antipsychotics. There was no increased cancer risk if exposure to PEAPs was less than 5 years, but longer exposure was associated with increased risk of breast cancer (OR 1.56 or a 37% increase in overall odds); exposure to higher cumulative PEAP dose was also associated with higher risk for cumulative daily dose greater than 1000 DDD (equivalent to risperidone 5 mg/day for 2.74 years). Risk of lobular adenocarcinoma with long-term use of PEAPs was higher than that of ductal adenocarcinoma.
Categorisation of antipsychotics according to prolactin elevating potential in three recent studies (only drugs available in Australia/New Zealand listed)
Discussion
The recent publications of Taipale et al. 4 and Rahman et al. 10 which report associations between antipsychotic medications and breast cancer are concerning. Women with schizophrenia have a higher rate of breast cancer, 12 have lower rates of breast cancer screening13,14 and a higher mortality from breast cancer. 15 Discerning the contribution of antipsychotic medication is an important consideration for any clinician prescribing for women with schizophrenia and other psychotic disorders.
The variation in results from recent studies may reflect methodological factors, such as the classification of antipsychotics and the extent to which confounding factors were controlled. Importantly, differences in liability for hyperprolactinaemia between antipsychotics may affect the findings. The studies showed an inconsistent approach to classification (Table 1), which makes comparisons of the studies more difficult. In studies where PEAPs were limited to those with very high propensity (such as in the Taipale study 4 ), the association with breast cancer appeared stronger, and the effect appeared more pronounced with longer treatment.
The studies involved retrospective analyses of large cohorts and registries but differed in methodology. Rahman et al. 10 used an observational cohort study of administrative claims data for comparison and was limited to women under 65 years, whereas Taipale et al. 4 and Pottegard et al. 11 used case-control analyses of nation-wide registry data from Finland and Denmark, respectively, which were gathered over several decades. Although the methodology of Taipale et al. 4 was generally strong, the use of an odds ratio in a case-control sample has been criticised as not being generalisable to the general population of women with schizophrenia. 16
While some studies controlled for confounding factors for breast cancer (such as Taipale et al.), 4 other studies did not. Key factors that may affect breast cancer development in women with schizophrenia include alcohol use, diabetes, nulliparity, not breast feeding, inactivity, obesity and smoking; other risk factors for women more generally include family history, early menarche, late menopause, hormone manipulation and the presence of risk-related genes. 8 Other factors complicating the interpretation of the studies considered in this paper arise out of technical issues concerning prolactin, including the circadian variation in prolactin concentrations and potential normalisation after long term use of PEAPs. 2
If the findings of Taipale et al. 4 are accurate, the lifetime risk of breast cancer for women who use a PEAP for over 5 years may increase from 12% to 16%. In Australia, this would potentially represent an excess of approximately 1,388 cases of breast cancer in women with psychosis (based a psychosis prevalence of 3.5 per 1000 and 2021 ABS estimation of 9.9 million adult women in Australia). Whilst a possible association of PEAPs and breast cancer is concerning, it does not provide evidence of causation and needs to be weighed against the association of antipsychotic treatment with overall lower mortality in schizophrenia. 17
On the basis of these studies, clinicians and their patients should ideally discuss the individual patient’s breast cancer risk factors and may consider the relative merits of using PSAPs. Prescribing choices regarding antipsychotic drugs continue to require a balancing of considerations, including efficacy, other side effects and risks and personal preference.
Conclusion
Recent studies have not proven causation between treatment with PEAPs and breast cancer, but some of the findings are disquieting. In this context, collaborative and informed decision making regarding antipsychotic medication options should now include a discussion of the potential risks for women taking prolactin-elevating medications, alongside routine discussions of the relative risks of individual antipsychotics weighted against the known benefits of effective treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article. This research was supported by the Pratt Foundation.