
Abstract
Objective
Older Chinese people in New Zealand underutilise mental health services. Lack of recognition of mental health issues and awareness of available treatment is a potential barrier to accessing care. This study investigated depression literacy in older Chinese people.
Method
A convenience sample of 67 older Chinese people were presented a depression vignette and completed a depression literacy questionnaire.
Results
There was a good rate (71.6%) of depression recognition, but no participant chose taking medication as the best method of help. There was a notable level of stigma among participants.
Conclusion
Older Chinese people would benefit from information regarding mental health conditions and their interventions. Strategies to deliver this information and de-stigmatise mental illness in the Chinese community which incorporate cultural values may be beneficial.
New Zealand is a culturally diverse country with many ethnic groups, including Māori, Pacific, Asian and European. The Asian population is the third largest and fastest growing group, making up 15.1% of the general population. 1 There is also a growing number of older Chinese, who make up 6.4% of older people in New Zealand. 1 This cohort is thought to be a high-risk group for developing mental health problems due to social isolation, language barriers, reliance on family for communication and transport and acculturation issues. 2 The underutilisation of mental health services by Chinese populations has been well-documented in New Zealand,3,4 as well as in other western nations.5,6 Stigmatisation of mental illness in Chinese culture due to influences from Confucianism, Taoism and Buddhism has a significant impact on how individuals and their families seek help for mental illness, which can result in treatment delays. 7 The underutilisation of mental health care by older adults has also been recognised, with Asian older adults accessing services disproportionately less than non-Asian older adults. 8 Chinese older people are an especially vulnerable group due to this intersectionality.
Mental health literacy is defined as ‘the knowledge and beliefs about mental disorders which aid their recognition, management or prevention’. 9 Poor mental health literacy may lead to delayed recognition of symptoms of mental illness, resulting in delayed presentations which can impact on prognosis. Correlates to poorer mental health literacy include older age, and ethnic minority and migrant groups. 10 International research into mental health literacy in older Chinese people is limited. A Canadian study of older Chinese immigrants showed poorer recognition of depression and knowledge of appropriate professional services, compared to their Canadian-born counterparts. 11
There has been no research into mental health literacy of older Chinese people in New Zealand. The aim of this study is to assess depression literacy in older Chinese. Results of the study could provide justification for implementation of culturally appropriate psychoeducation and treatment strategies for this population.
Method
Setting and participants
A convenience sample of participants was recruited from a community organisation that provides weekly social programmes for Chinese older people.
Participants were included if they identified as Chinese; were aged 65 years or above; and provided written informed consent. Ethics approval was obtained from the local university’s Human Participants Ethics Committee. The research was conducted in September 2018.
Data collection
(i) Demographic information: age, gender, ethnicity, marital status, country of birth, number of years living in New Zealand and level of education.
(ii) Jorm’s Mental Health Literacy Questionnaire
9
was used with permission. The questionnaire was modified to that of a written questionnaire which allowed self-administration. The authors, as bilingual clinical researchers, translated the depression vignette (Box 1) and questionnaire to simplified Chinese.
Jenny is 30 years old. She has been feeling unusually sad and miserable for the last few weeks. Even though she is tired all the time, she has trouble sleeping nearly every night. Jenny doesn’t feel like eating and has lost weight. She can’t keep her mind on her work and puts off making decisions. Even day-to-day tasks seem too much for her. This has come to the attention of her boss, who is concerned about Jenny’s lowered productivity.
(iii) The first author attended the community organisation’s weekly programmes to conduct the study. Each participant was given a questionnaire. The questionnaire was also projected on to a screen. The first author and the group coordinator went through each question with the participants as a group. Participants were able to clarify any questions they had.
Data analysis
Data were entered into Statistical Package for Social Sciences version 26. Descriptive statistics, numbers and percentages for categorical variables and means and standard deviations for continuous variables were used to summarise the results.
Results
Demographic information
Participant demographics.
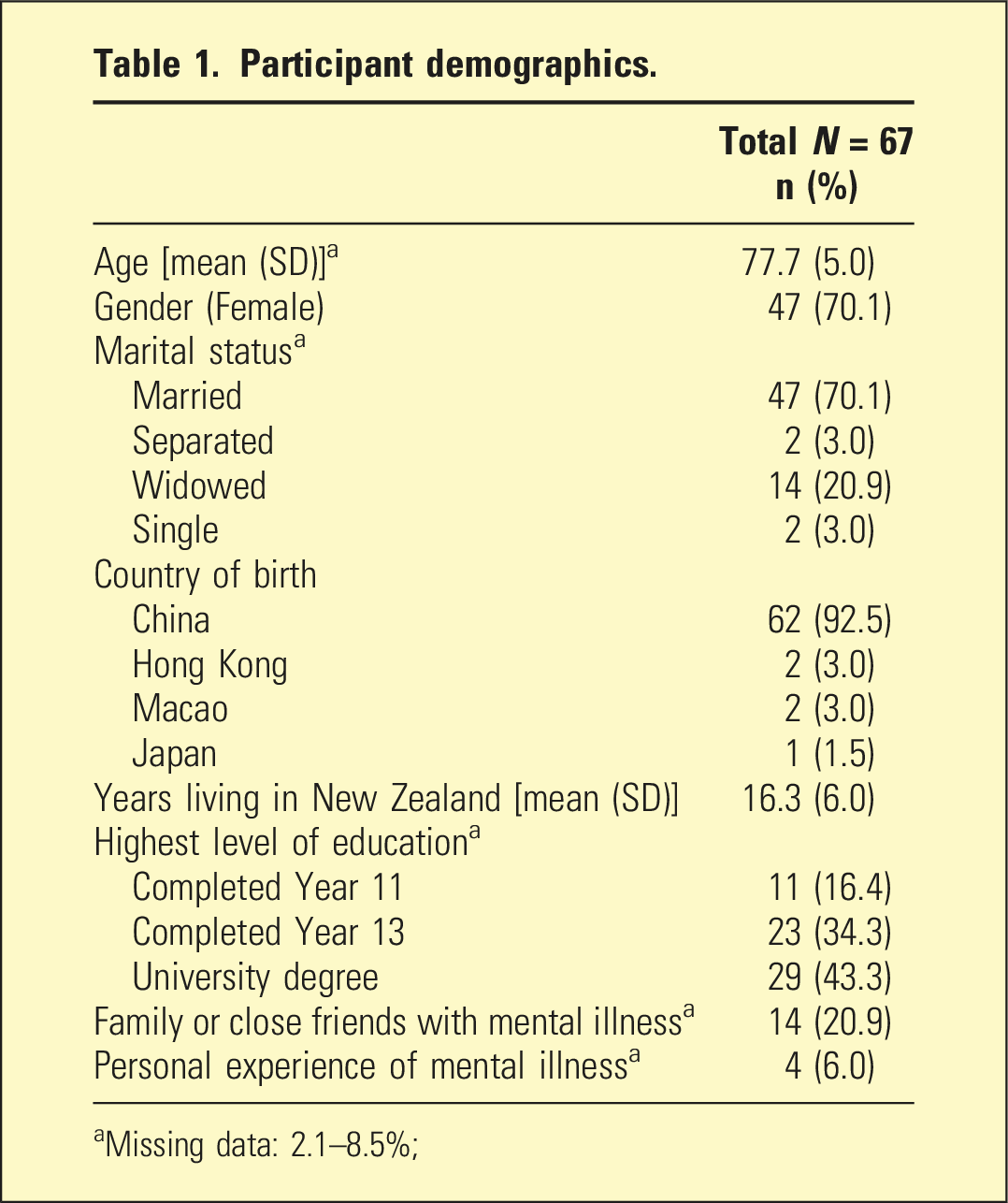
aMissing data: 2.1–8.5%;
Recognition of depression
71.6% of participants identified depression as the diagnosis.
Best method of help
Talking with friends/family was thought to be the best method of help (28.3%), followed by seeing a general practitioner (22.3%) and a psychologist (16.4%). No participants chose ‘Take medication’ as the best method of help (Figure 1). Best method of help.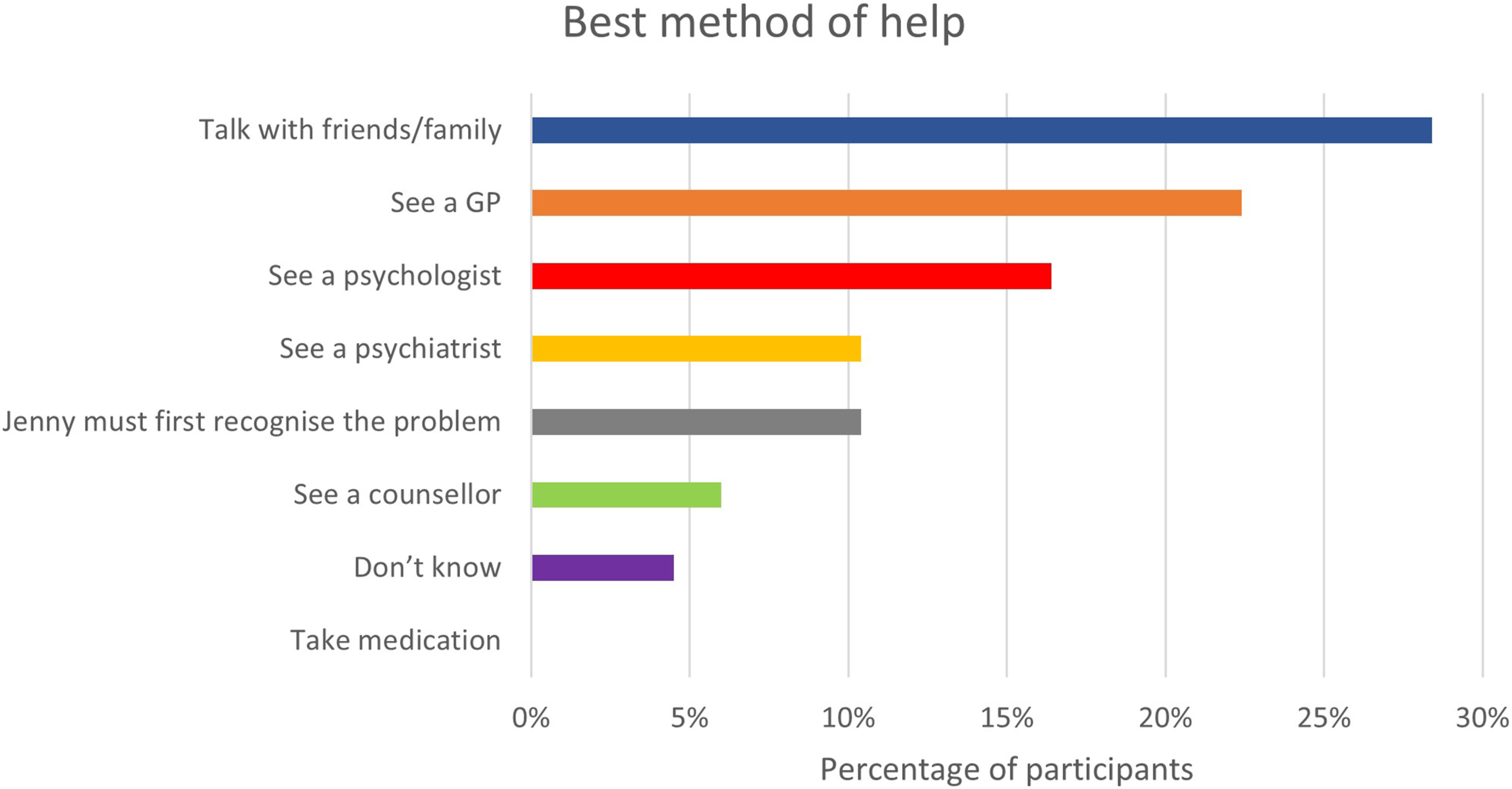
Potential causes of the problem
Potential causes of the vignette character’s problem.
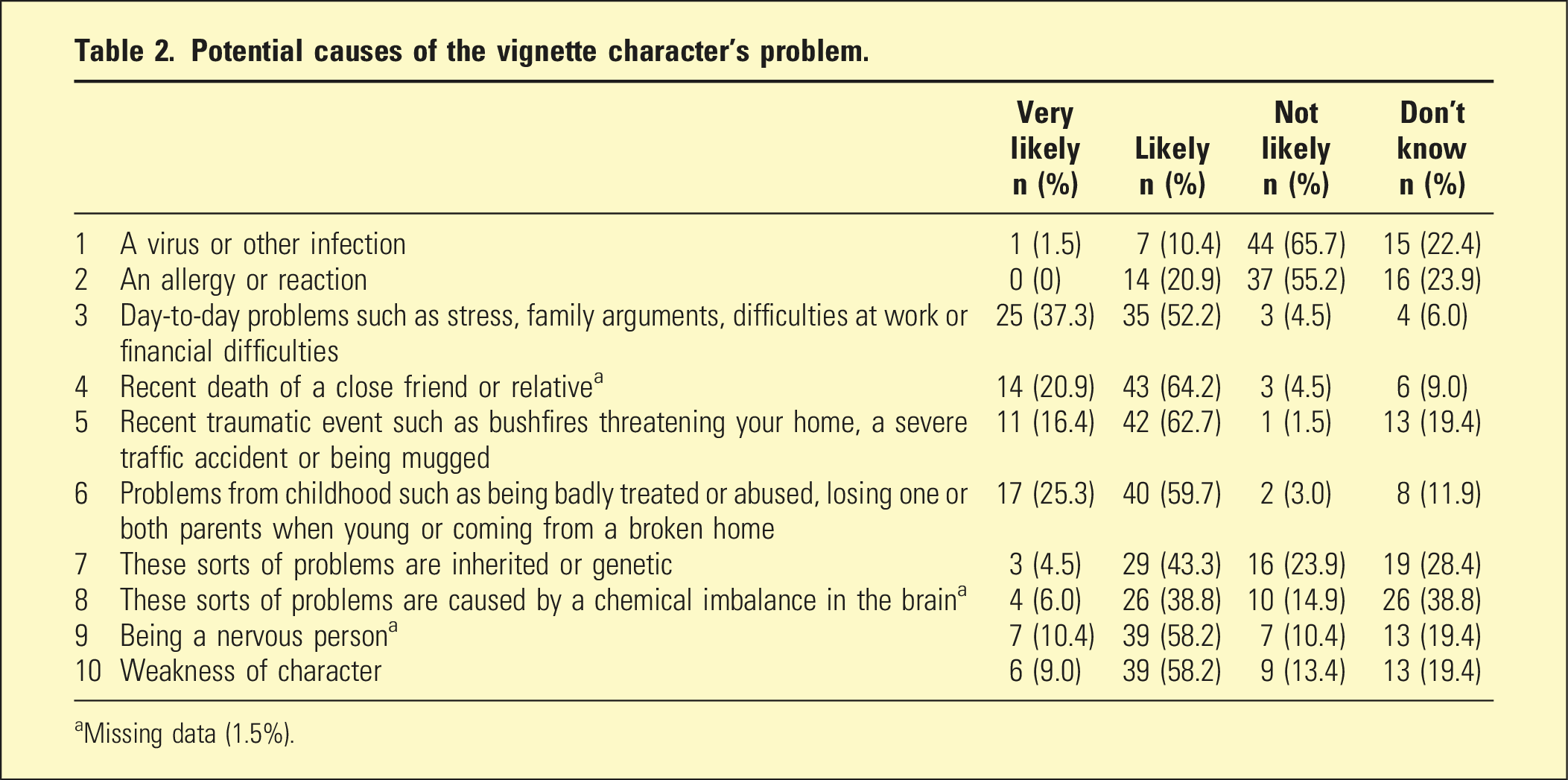
aMissing data (1.5%).
Rating of pharmacological and non-pharmacological treatments
The majority of participants viewed antidepressants as helpful (72.7%).
Rating of pharmacological and non-pharmacological treatments.
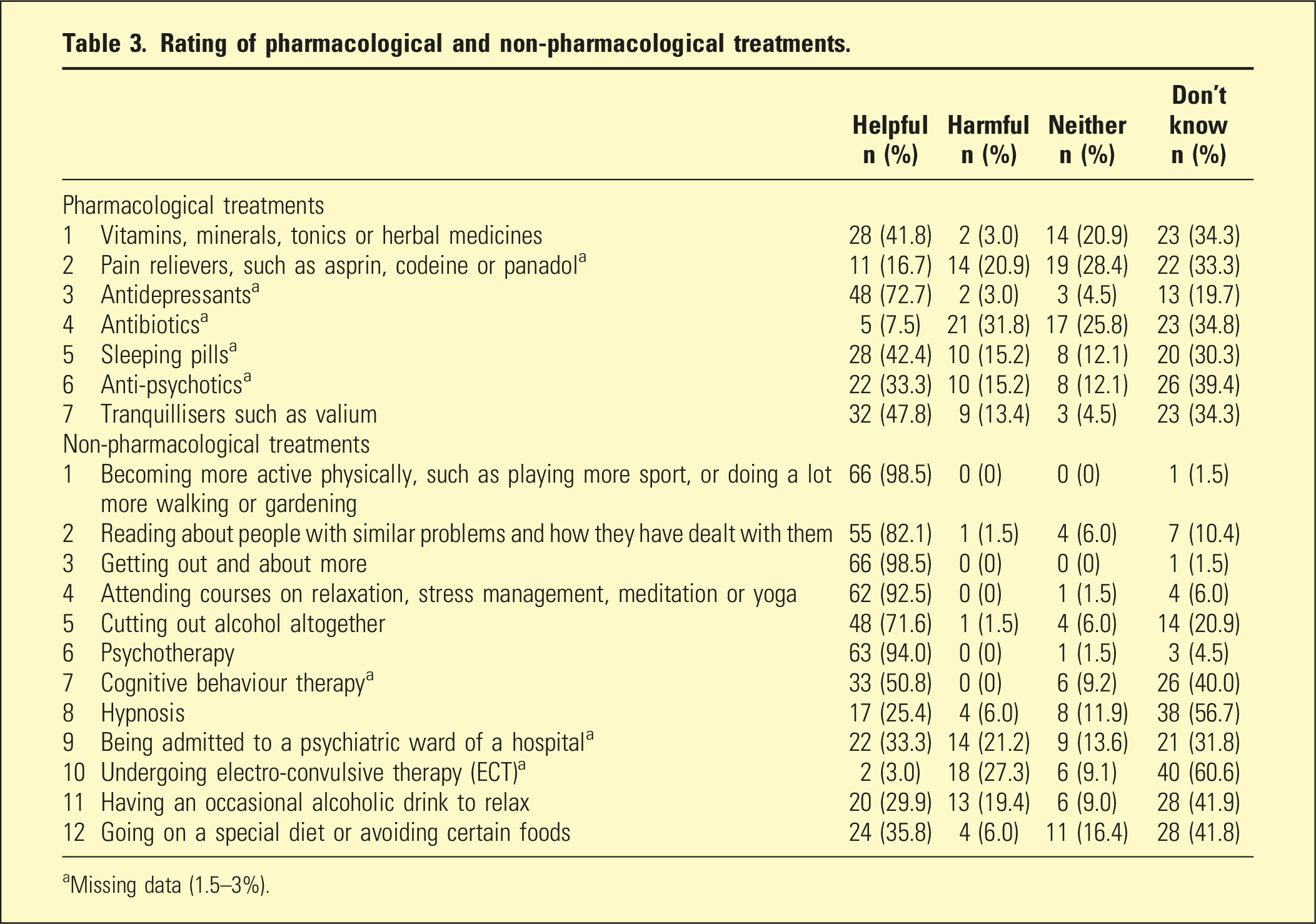
aMissing data (1.5–3%).
Perceptions of people like the vignette character
Perceptions of people like the vignette character.
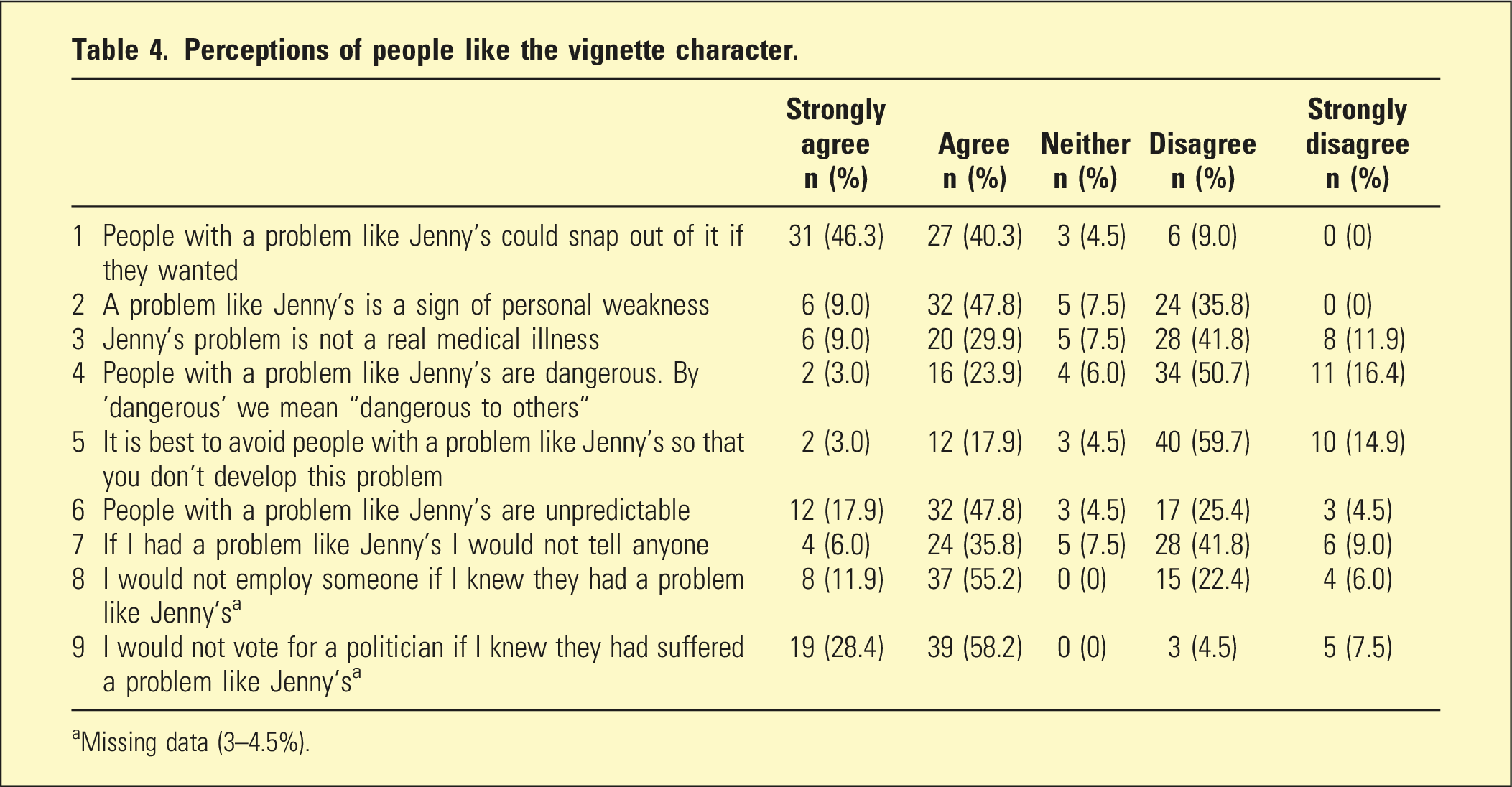
aMissing data (3–4.5%).
Discussion
The rate of depression recognition in this sample was much higher than another cohort of Chinese older immigrants in Canada in which the recognition rate was only 11.3%. 11 Several factors may explain this difference. The participants in this cohort had a much higher level of education compared to the Canadian study. Higher education levels are associated with better mental health literacy. 10 Methodological differences between the two studies may also have contributed. This study used a self-administered questionnaire with a list of problems to choose from which may have prompted participants to respond with depression. In comparison, interviews were conducted in the Canadian study and participants were asked to identify the condition without any cues. Cueing older adults with mental health labels has been shown to improve mental health literacy. 12 Acculturation was another factor considered given the participants have lived in New Zealand for a relatively long length of time (mean years of living in New Zealand being 16.3). However, the Canadian participants had also lived in Canada for a long period (mean duration of residence in Canada being 21.5 years). It was therefore difficult to attribute the higher rate of depression recognition to acculturation given the process of acculturation can be varied and wide-ranging between different individuals, groups and generations. 13 The age of the vignette character may also have impacted on the recognition rate. Studies have shown that participants are more likely to recognise depressive symptoms when the character is younger compared to older. 12
It was noted that no participant chose medication as the best method of help. This finding is consistent with other parts of the questionnaire, with the vast majority rating ‘being more physically active’ and ‘getting out and about’ as helpful interventions. It was also notable that psychosocial causes such as ‘day-to-day problems’ and ‘problems from childhood’ were rated more highly as potential causes of depression than biological factors such as ‘chemical imbalance in brain’. This may explain the higher rating for non-pharmacological interventions. The results suggest older Chinese people may be more open to non-pharmacological interventions that incorporate physical and social activity such as behavioural activation and exercise. Another consideration is the difficulty for lay respondents to discern the clinical information in the vignette to identify medication as a recommended treatment, given this is a task undertaken by medical professionals. Participants may not have the confidence or knowledge to choose medication as the best method of help.
There was a notable level of stigmatisation in the responses which is likely an impact of underlying cultural beliefs, resulting in negative perceptions of people with mental illness. There may be a place for interventions that address this stigmatisation which targets cultural factors and traditional views, with a focus on older people.
There are several limitations. Firstly, this study used a small convenient sample of older Chinese living in New Zealand which may impact generalisability. Secondly, the translation of the vignette and questionnaire to simplified Chinese did not include a back translation, which may impact on its accuracy and validity. Thirdly, the vignette methodology is limited in potentially not being representative of real-life situations. In real life, individuals can gain more information about symptoms in others and are able to monitor changes over time. A vignette would not be able to capture this information. 14 Lastly, consideration needs to be given to the issue that in using this vignette with a depression diagnosis, a Western view of health is potentially being imposed on this ethnic group. Qualitative studies may add more to knowledge around this cohort’s understanding of mental health issues and be better placed to take into consideration relevant cultural factors. Future research can also include comparing mental health literacy across New Zealand’s main ethnic groups.
Conclusion
This study found high levels of depression recognition in a sample of highly-educated older Chinese, but highlighted deficits in knowledge of some treatment options, and the presence of stigmatising attitudes towards mental illness. Interventions to increase knowledge of mental health issues in older Chinese populations should consider the stigma of mental illness and the cultural values that influence Chinese people’s perception of mental illness.
Supplemental Material
Supplemental Material - Depression literacy in older Chinese people in New Zealand
Supplemental Material for Depression literacy in older Chinese people in New Zealand by Helen Lowe and Gary Cheung in Australasian Psychiatry
Footnotes
Ethical approval
Ethics approval was obtained from the University of Auckland Human Participants Ethics Committee (reference 021551).
Acknowledgements
We would like to thank the participants and Sandy Nip, coordinator at the Chinese Positive Ageing Trust, Auckland, New Zealand.
Informed consent
Informed consent was obtained from all participants in the study.
Correction (September 2023):
Supplementary-material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.