
Abstract
Objective:
SPARX is a computerized cognitive behavioral therapy self-help program for adolescent depression that is freely available in New Zealand. At registration, users identify themselves as either male, female, intersex, or transgender. We aimed to describe the mental health of adolescent intersex users.
Method:
A secondary analysis of SPARX usage data over 5 years.
Results:
Of the 8922 adolescents users, 0.6% (n = 50) identified as intersex. Based on Patient Health Questionnaire 9 – modified for Adolescents (PHQ-A) results, 78.3% of intersex users had high levels of depression and/or self-harm and suicidal ideation. The mean PHQ-A scores for intersex users were significantly higher than for males and females (p < .001). As only three intersex users completed SPARX Level 4 or more (of the seven-level program), we were unable to meaningfully investigate any reductions in their depressive symptoms over time.
Conclusions:
There is a dearth of empirical data on the mental health of intersex adolescents. These results suggest that intersex adolescents seeking help from an online resource have high mental health needs compared with other young people, possibly because they defer seeking help.
Intersex people are individuals born with biological or physical sex characteristics (e.g. sexual anatomy and hormonal variations) that are more diverse than those stereotypically associated with male or female bodies. 1 Unfortunately, stigmatizing and pathologizing practices are often an issue in relation to variations of sex characteristics (VSC), 1 including the persistent use of problematic terminology, which includes the term “Disorders of Sex Development.” 2 In contrast to viewing VSC or diverse sex development as especially rare medical conditions, it is increasingly being argued that intersex be viewed as an ordinary aspect of human bodily diversity. 3 Data are not available to establish the exact proportion of intersex people in the overall population, but it has been estimated that ‘genital anomalies’ occur in approximately 1 in 4500 births. 4 However, only a small fraction of people with VSC will “. . .require [an] extensive multidisciplinary assessment” (p. 159) to formally confirm diverse sex development. 5 For some people, VSC will be apparent prenatally or at birth, 6 while for others VSC will emerge later in life, often at puberty. 1
Diverse sex development is thought to have particular implications for an intersex person’s mental well-being due to a range of factors often related to traumatic medical assessments and interventions, the potential secrecy and sense of shame related to the stigmatization of VSC, and the possible challenges that can be associated with managing one’s bodily difference.1,3 A recent systematic review exploring the mental health of intersex people found that 16 (out of 18) studies in the field reported elevated rates of mental health problems. 7 The remaining two studies involved research conducted with adolescents; neither study found an increase in psychological distress when intersex adolescents were compared to a matched control group using standardized assessments. 7
In New Zealand, rates of youth suicide are elevated compared with other high-income countries, although rates of depression in adolescents are on par with many other countries. 8 Unfortunately, access to evidence-based psychotherapies such as cognitive behavioural therapy (CBT) is problematic for this age group. 8 In response to this, a gamified CBT intervention for adolescent depression called SPARX (www.sparx.org.nz) was developed (for further details, see [9]) and shown to be at least as good as treatment as usual in primary care settings. 9 Since April 2014, SPARX has been made freely available online as a self-help tool in New Zealand, funded by the Ministry of Health. The intervention has been actively promoted by the Ministry of Health (via its webpages) as well as by practitioners, including those from community organizations such as ITANZ (Intersex Trust Aotearoa New Zealand). SPARX includes tracking of a user’s mood via an embedded version of the Patient Health Questionnaire 9 – modified for Adolescents (PHQ-A) 10 at Levels 1, 4, and 7 (from a total of seven levels). Telephone, web-based, and email support can be accessed via the program’s website, and automated messages suggest seeking professional help for those reporting severe depression or self-harm. Adolescent users of SPARX are asked a single sex/gender question at registration, which involves selecting only one of the following: male, female, intersex, or transgender (the results pertaining to the 207 transgender users of SPARX are reported elsewhere 11 ). The objective of this study was to explore the mental health of adolescents identifying as intersex who were seeking online help for their depression. We were only able to investigate baseline/Level 1 data, due to very low SPARX completion rates for intersex users.
Methods
We carried out an analysis of the first 5 years of SPARX data using baseline/Level 1 PHQ-A scores. All data were based on self-report and any person with a New Zealand Internet Protocol/IP address was able to register. Adolescents (12–19 years old) were categorized as having “high depression scores and/or self-harm and suicidal ideation” if they had a baseline PHQ-A total score in the “moderately severe depression” or “severe depression” range and/or a baseline PHQ-A self-harm and suicidal ideation score indicating medium or above risk. Chi-square tests for independence were used to compare participants for categorical data. For continuous data, participants were compared with a one-way between-groups ANOVA. Statistical analyses were performed using IBM SPSS Statistics version 24. This study was approved by the New Zealand Health and Disability Ethics Committee, Reference: 15/NTB/183.
Results
Two-thirds of SPARX users identified as female (n = 5968), almost one-third identified as male (n = 2904), and 0.6% (n = 50) identified as intersex. Female users were more likely to be aged between 16 and 19 years (p < .001). The largest single ethnic group was New Zealand European, but less than half of intersex adolescents (n = 21) were New Zealand European (p < .001) (Table 1).
Demographics
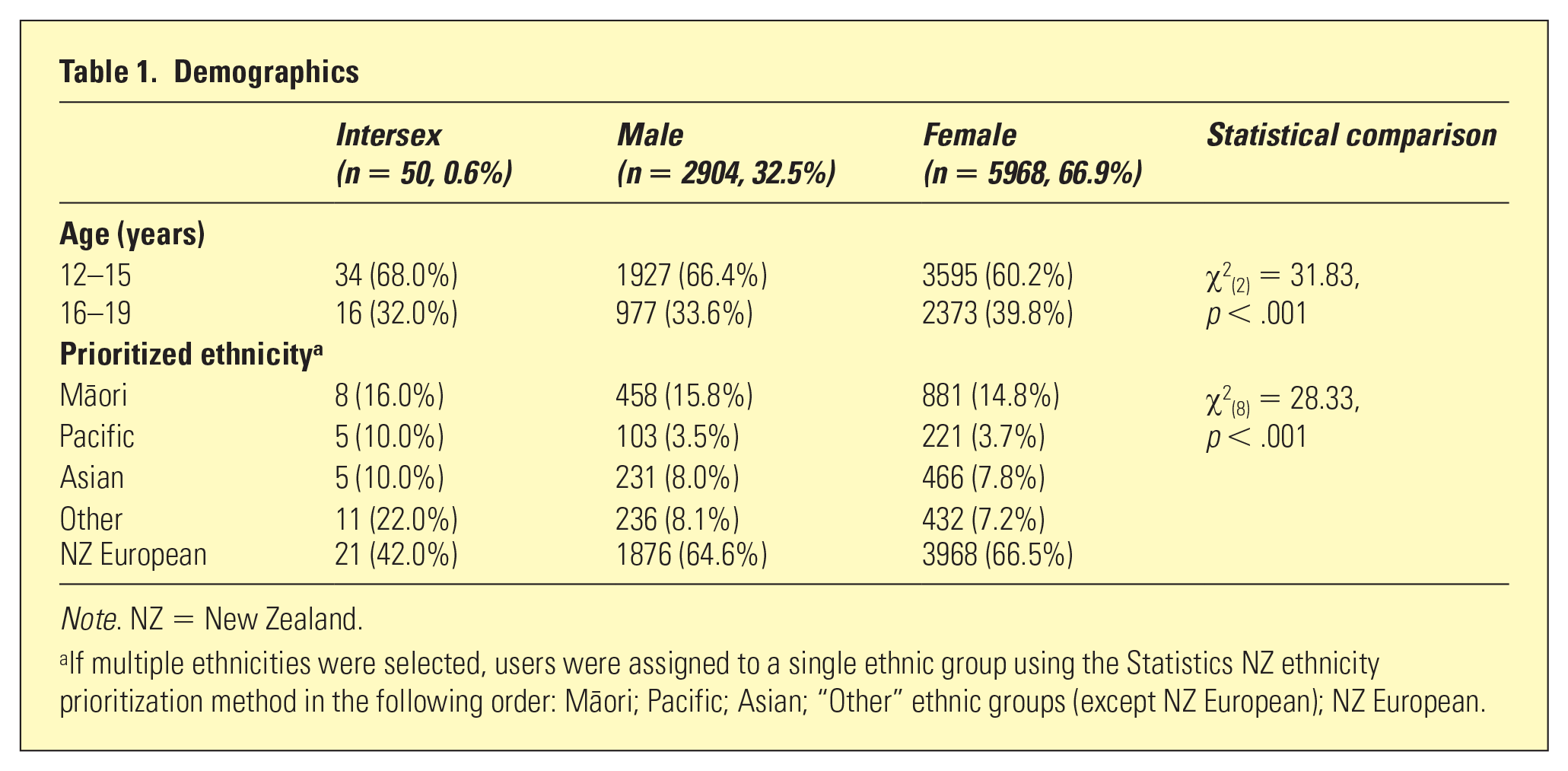
Note. NZ = New Zealand.
If multiple ethnicities were selected, users were assigned to a single ethnic group using the Statistics NZ ethnicity prioritization method in the following order: Ma¯ori; Pacific; Asian; “Other” ethnic groups (except NZ European); NZ European.
More than three-quarters of intersex users reported high depression scores and/or self-harm and suicidal ideation (n = 36), and they were significantly more likely to report this compared to males and females (χ2(2) = 278.38, p < .001). Moreover, the mean PHQ-A score for intersex users was significantly higher than the means for both males and females (F(1,45.5) = 21.78, p < .001) (Table 2).
PHQ-A scores
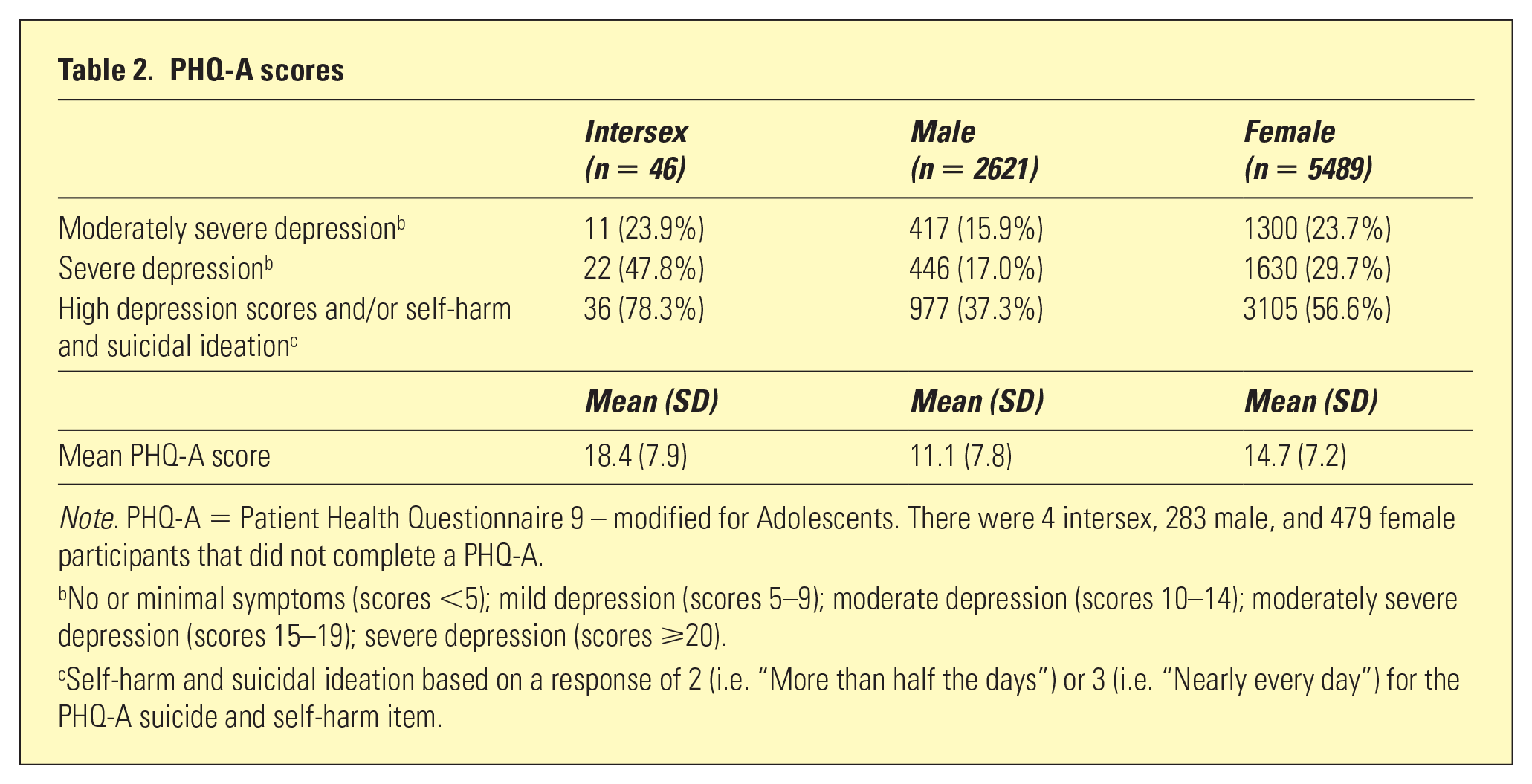
Note. PHQ-A = Patient Health Questionnaire 9 – modified for Adolescents. There were 4 intersex, 283 male, and 479 female participants that did not complete a PHQ-A.
No or minimal symptoms (scores <5); mild depression (scores 5–9); moderate depression (scores 10–14); moderately severe depression (scores 15–19); severe depression (scores ⩾20).
Self-harm and suicidal ideation based on a response of 2 (i.e. “More than half the days”) or 3 (i.e. “Nearly every day”) for the PHQ-A suicide and self-harm item.
Discussion
In this community sample of adolescents registering for SPARX, those who identified as intersex were ethnically diverse and reported higher levels of depression than users who identified as male or female. As only three intersex users completed SPARX Level 4 (or more), we were unable to meaningfully investigate any reductions in their depressive symptoms over time. The utility of a “mainstream” intervention like SPARX for this population, therefore, remains to be investigated. That all responses in this study are based on self-report is a limitation of this research. In particular, the single sex/gender item was restrictive, as users could only select “Male,” “Female,” “Transgender,” or “Intersex.” No further options were available (e.g. gender queer or non-binary), and users were not permitted to select more than one response. Therefore, intersex users were unable to identify in more than one way, such as being intersex and also identifying as male or female, as many intersex adolescents will. 12 Furthermore, participants were not asked whether they had received any formal confirmation of their intersex status, so we note that intersex status in this study was by self-identification. Strengths of this study include the use of a psychometrically sound assessment 10 and the large-scale “real world” context of this research. This study has two main implications. First, intersex adolescents with high mental health needs are accessing a “mainstream” tool like SPARX, but their treatment completion rates are disappointingly low. Second, given that intersex adolescents have demonstrated that they will access digital interventions, are geographically spread throughout New Zealand, have unique psychosocial needs,1,2,13 and so few intersex users advanced past SPARX Level 4, digital health tools specifically for intersex adolescents are likely to be valuable. Peer support and advocacy groups have previously been highlighted as being particularly important (e.g. in New Zealand www.ianz.org.nz),1,3 but further research that builds on earlier support work is warranted in advancing digital tools for this population.
Footnotes
Acknowledgements
We would like to thank all the adolescent participants who used the SPARX program and the staff at the National Institute for Health Innovation (NIHI) at the University of Auckland who supported this study, specifically Professor Chris Bullen (Director, NIHI) and Karen Carter (General Manager, NIHI). We would like to thank Mani Bruce Mitchell (Executive Director), Dr. Rogena Sterling (Co-Chairperson), and Jelly O’Shea (Communications and Projects Manager) from ITANZ (Intersex Trust Aotearoa New Zealand) for their feedback on earlier drafts of this paper. We would like to thank the Ministry of Health for funding the development and deployment of SPARX in New Zealand. Finally, we would like to thank Cure Kids who provided funding for SM and KS.
Disclosure
The intellectual property for SPARX is held by UniServices at the University of Auckland. Any proceeds from licensing or selling SPARX outside of New Zealand will be shared in part with UniServices and ML, TF, SM, MS, and KS.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article