
Abstract
Active music interventions represent one promising nonpharmacological intervention; however, the effects of these interventions are not well understood. This systematic review and meta-analysis examined the effects of active music interventions on cognitive function and neuropsychiatric symptoms in patients with dementia. Four independent database searches revealed 747 independent studies that were filtered by article type, topic, and relevancy, based on inclusion criteria. Nine randomized controlled trials (RCTs) were selected for inclusion and were assessed for quality using the Cochrane Risk of Bias tool. Results of the meta-analyses revealed those receiving an active music intervention scored significantly higher than controls on the Mini-Mental State Exam and reported fewer neuropsychiatric symptoms as denoted by the Neuropsychiatric Inventory, post-intervention. There is a need for additional RCTs with consistent standardized cognitive measures to compare dosage, duration, and intervention type (e.g., instrumental or vocal) across domains. Future research is necessary to distinguish the benefits of active music interventions on cognitive function and neuropsychiatric symptoms (e.g., agitation, depression) in patients with dementia.
Dementia refers to a group of complex neurodegenerative disorders afflicting 50 million adults worldwide. Such disorders are characterized by progressive cognitive decline resulting in loss of daily functioning (Kirova et al., 2015; World Alzheimer Report, 2019). It is estimated that the number of people who are diagnosed with dementia will increase to 75 million by 2030 (World Health Organization [WHO], 2019). There is a need for effective treatments for both the causes and symptoms of dementia since current pharmaceutical treatments are costly, provide limited relief from symptoms, and often have adverse side effects; for example, anticholinergics are associated with higher hospitalization rates and further cognitive decline (Kalisch Ellett et al., 2014; Schneider et al., 2006). It is therefore necessary to identify nonpharmacological interventions capable of reducing the cognitive deficits and enhancing the quality of life of people with dementia. The purpose of this systematic review and meta-analysis was to assess the effects of randomized controlled trials (RCTs) with active music therapy and other active music interventions on global cognition and neuropsychiatric symptoms in older adults with dementia, compared with standard treatments.
Music is a promising area of study due to its universal appeal and ease of application in therapy programs (Mofredj et al., 2016). In addition, the neural networks required for music processing are complex and may enhance global cognition in dementia (Herholz et al., 2013). Music processing requires the use of both cerebral hemispheres; the right hemisphere is involved in perceiving duration, timbre, tone, and volume of music, while the left hemisphere is important for rhythm, simultaneity, and motor control (Gates & Bradshaw, 1977; Golden et al., 2017). Furthermore, structures for processing music remain intact in late Alzheimer’s disease, suggesting that even patients diagnosed with advanced dementia may respond well to music interventions (Jacobsen et al., 2015).
Music therapy has been defined as the use of musical experiences implemented clinically by a professional music therapist to achieve a goal related to physical, social, and cognitive functioning (Aigen, 2012; Thaut & Hoemberg, 2014). There are two broad types of music therapy, receptive and active (Vink et al., 2004). In receptive music therapy, participants listen to live or recorded music provided by a music therapist. Active music therapy involves participation in music-making via singing, clapping, playing instruments, or movement to music such as dancing. Many therapeutic music programs include both active and receptive components; thus, there is no clear distinction between programs comprising solely active and those using solely receptive music therapy, which can make it difficult to select music listening or performance exercises best suited for participants with dementia. Research in this area could provide information as to the active music therapy programs and interventions that are most beneficial for cognitive performance and neuropsychiatric symptoms, and the stage of dementia at which they are best implemented (Regier et al., 2017). This review focuses on RCTs of active music therapy and music interventions that include singing, playing an instrument, clapping along to music, and any other movement in response to music that does not involve the whole body.
A key strength of music therapy is that interventions are applied at the individual level and tailored to the needs of independent conditions. In addition to music therapy, music interventions, derived from the tradition of music education, include a scalable sequenced curriculum of progressively more difficult exercises with the aim of teaching music and enhancing transfer to cognitive and health outcomes. Results of recent studies with group music interventions have demonstrated promising results (Bugos & Wang, 2022; Dorris et al., 2021). Musical interventions as well as active music therapy programs contribute to musical care, a term suggesting that the interdisciplinary use of music can affect individuals at the micro level, as individuals, the meso level, in groups, and the macro level, in society and through cultures (Sanfilippo et al., 2022; Wood & Clift, 2022). The results of previous meta-analyses of studies of patients with mild cognitive impairment suggest that participating in musical activities may contribute to care in terms of supporting improved cognitive function and psychosocial outcomes (Dorris et al., 2021). However, most meta-analyses focus on patients with dementia listening to music (Garrido et al., 2017, 2018; Li et al., 2015) or do not differentiate between receptive and active music interventions (Chang et al., 2015; van der Steen et al., 2017; Zhang et al., 2017). Some recent reviews have attempted to discriminate between types of music interventions (Lam et al., 2020; McDermott et al., 2019; Moreno-Morales et al., 2020). Yet only the meta-analysis conducted by Dorris et al., (2021) has attempted to determine the effects of active music interventions on cognitive function in patients with dementia, resulting in small effect sizes. While listening to music may reduce stress and anxiety in patients with dementia (Bradt et al., 2013), some research suggests that programs involving active participation in music-making may be more beneficial than music listening alone. In one study, older adults with mild to moderate dementia were enrolled in a 10-week music intervention involving listening or singing, or assigned to a control group, with all participants completing standardized measures of cognition pre- and postintervention (Särkämö et al., 2013). At the end of the intervention, individuals in the singing group demonstrated improved short-term and working memory, with less decline in verbal learning as compared to the music-listening and control groups. Nevertheless, few RCTs have compared music-listening interventions with active music performance interventions or therapy.
A few studies have attempted to elucidate the benefits of receptive music therapy as opposed to active music therapy, or vice versa. An RCT comparing the effects of receptive and active music therapy on participants with major depressive disorder found that receptive music therapy achieved its peak therapeutic effect faster, but active music therapy had a greater average therapeutic effect (Atiwannapat et al., 2016). The results of a recent systematic review found that receptive music therapy is more effective than interactive music therapy for reducing agitation, behavioral problems, and anxiety in older adults with dementia (Tsoi et al., 2018). In contrast, a subgroup analysis reported in another recent systematic review suggested that there is a beneficial effect of active music therapy on cognition in people with dementia (Fusar-Poli et al., 2018). However, this subgroup analysis was performed using just three studies, and we aimed to investigate this claim further in a rigorous analysis of existing and novel literature.
Research examining the effects of active music interventions on cognition and executive functions in older adults without cognitive impairment may inform future efforts to help those with dementia. Older adults who completed 6 months of individualized piano training outperformed no-treatment controls on measures of working memory and executive functions (Bugos et al., 2007). Data showed that some areas of executive functions such as perceptual speed and visual scanning were maintained after a 3-month delay period. The researchers suggested that the benefits may be attributed to overcoming the sensorimotor challenges of bimanual coordination, task novelty, and progressive difficulty. In a subsequent study, older adults showed improved visual scanning and working memory following a 16-week piano- or percussion-training intervention as compared to a music-listening program (Bugos, 2019).
In another study, adults who completed a 4-month program of group piano training showed increases in measures of cognitive control and well-being (Seinfeld et al., 2013). Older adults who completed a 10-day intensive piano-training intervention experienced an increase in verbal fluency (Bugos & Kochar, 2017). Other types of music interventions involving activities such as drumming have been shown to increase working memory in healthy adults (Degé & Kerkovius, 2018) and participants with Huntington’s disease (Metzler-Baddeley et al., 2014). A recent scoping review of 11 publications, many of which were correlational studies comparing associations between the cognitive performance of healthy older adult musicians and nonmusicians, suggested that playing music has positive outcomes for cognition (Schneider et al., 2019). Collectively, these studies provide evidence to support the role of music interventions for enhanced executive function in healthy adults. Music programs may be a viable and sustainable intervention for clinical populations.
Although studies have suggested cognitive benefits from music interventions for older adults, few studies have involved clinical populations. Recent RCTs have produced mixed results. Some demonstrate promise in improving cognitive function (Biasutti & Mangiacotti, 2018; Chen & Pei, 2018), while the findings of others are limited by therapist availability, sample size, session scheduling, and treatment adherence (Wang et al., 2018). There is thus a need for a systematic review and meta-analysis of RCTs to increase the power of these studies and more rigorously assess the effect of active music interventions on cognitive function in older adults with dementia. Specifically, we asked if interventions involving active participation in music-making affect cognitive outcomes in older adults with dementia to a greater extent than no-music interventions
Our secondary purpose was to evaluate the effect of music interventions on neuropsychiatric symptoms in older adults with dementia. Neuropsychiatric symptoms in Alzheimer’s disease include psychosis such as delusions and hallucinations; mood disorders such as depression, anxiety, and apathy; behavioral symptoms such as irritability, agitation, and aggression; and other syndromes such as sleep disorders, eating disorders, and prefrontal syndromes (Lyketsos et al., 2011). Neuropsychiatric symptoms are prevalent among those with dementia. In one study, over 80% of 362 participants with dementia who were surveyed reported experiencing at least one neuropsychiatric symptom since the onset of the disease (Lyketsos et al., 2002). Additionally, research has suggested that the presence of neuropsychiatric symptoms predicts cognitive decline in dementia. A longitudinal study of participants with frontotemporal dementia and Alzheimer’s disease found that neuropsychiatric symptoms in the early stages of the disease had a direct impact on the subsequent course of the disease (Santacruz Escudero et al., 2019). Evidence reported in the literature suggests that music interventions may improve neuropsychiatric symptoms in older adults with dementia, and this meta-analysis aimed to further evaluate the effects of active music interventions on neuropsychiatric symptoms (Gallego & Garcia, 2017; Schroeder et al., 2018).
Methods
Systematic review
A comprehensive search of the literature in PubMed, Embase, Web of Science, and Cochrane Central was performed in May 2019 in accordance with the Preferred Method Items for Systematic Review and Meta-Analyses (PRISMA) statement (see Figure 1). Since our research focused on the extent to which interventions involving active participation in music-making affect cognitive outcomes in older adults with dementia, as opposed to no-music interventions, a predetermined set of 20 search terms was used for each database, using a combination of the terms “music,” “cognition,” “executive function,” “Alzheimer’s disease,” “dementia,” and “cognitive impairment,” and combinations of these terms. The inclusion of search terms focusing on a clinical diagnosis of dementia or Alzheimer’s disease was necessary as “music therapy,” “music intervention,” or “music” on its own would not produce relevant research on active music therapy or interventions for patients with dementia. All searches were performed from the inception of the database with no time restriction and were filtered for RCTs when possible. Supplementary searches were performed by entering the same search terms into Google Scholar to identify other studies that might have fitted the inclusion criteria. All searches were restricted to the English language. Search results were imported into EndNote X9.3.2.
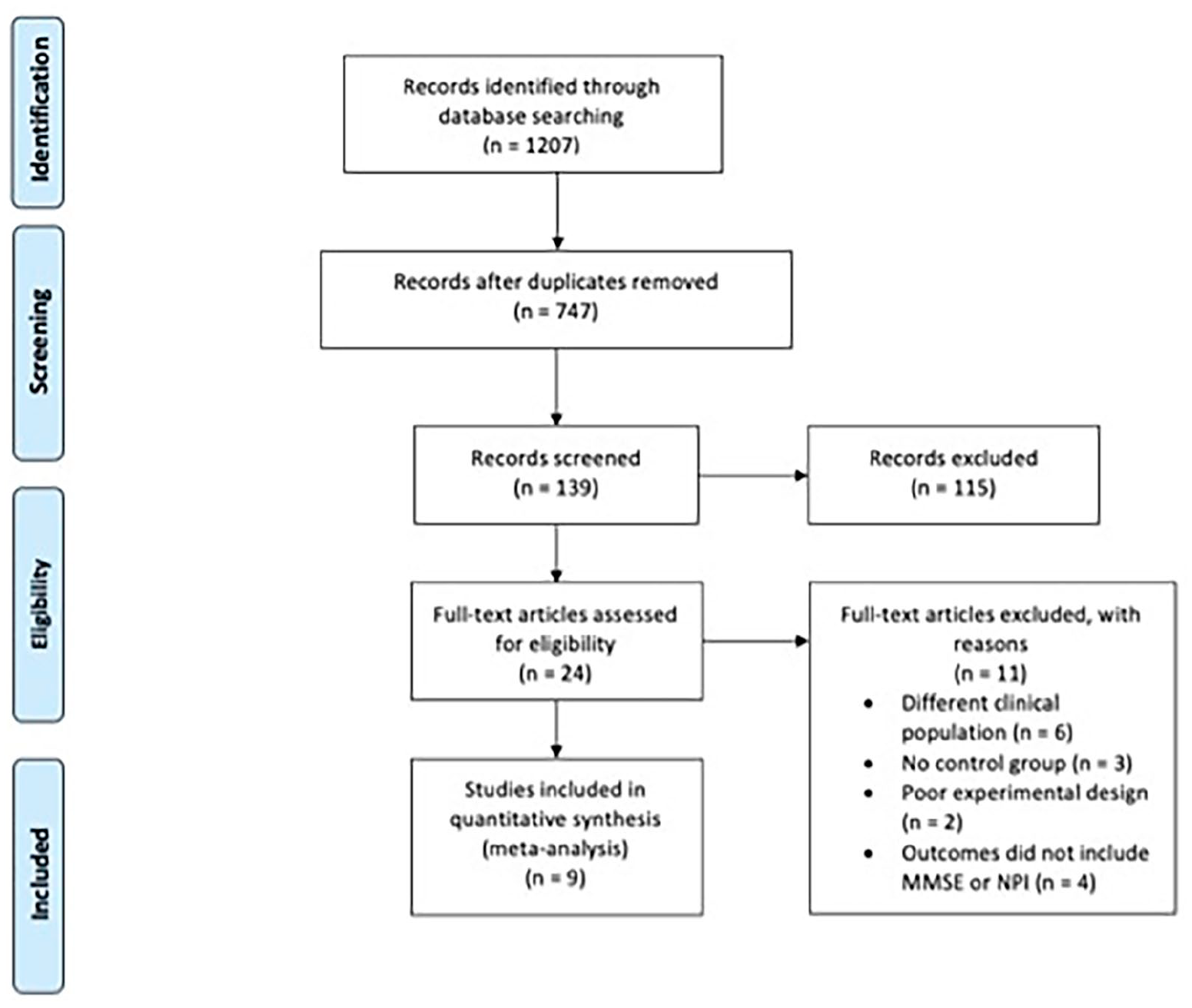
PRISMA flow diagram.
Inclusion and exclusion criteria
Studies were considered for inclusion if they met the following criteria: (1) they were peer-reviewed RCTs; (2) participants had a standard diagnosis of dementia or Alzheimer’s disease by a medical professional prior to the intervention period; (3) the music intervention included a component that required active participation, such as singing, drumming, clapping but did not include movement to music or multimodal interventions; and (4) primary or secondary outcomes were assessed using standardized measures of cognitive function or neuropsychiatric symptoms. Studies were excluded if they used multimodal interventions or movement to music and if they consisted primarily of listening passively to music, as none of these activities reflect active musical engagement. Studies were excluded if patients had early-onset dementia as we were primarily interested in identifying studies that included older adults (65+). Studies were not excluded based on the type of control group. Therefore, some studies included an active control group in which participants engaged in an alternative form of therapy and others included a passive control group in which participants received standard treatment. All studies included a control with some sort of cognitive stimulation (e.g., social stimulation, lyric reading, neuroeducation).
Outcome measures
The primary outcome measured was cognitive function. Cognitive function was defined as the higher-order processing required to carry out specific tasks, such as memory, attention, language, and visuospatial skills. We considered outcome measurements broadly, then chose those that had been used in a sufficient number of studies for the meta-analysis to be conducted with adequate power. Cognition was therefore measured using a commonly used assessment, the Mini-Mental State Examination (MMSE; Folstein et al., 1975). This is a questionnaire used in clinical settings to evaluate cognitive domains, including visuospatial skills, language, concentration, working memory and recall, and orientation. It takes 5–10 min to administer and has a maximum score of 30; scores of less than 24 indicate cognitive impairment. The MMSE has been shown to be useful for screening patients with cognitive decline and aiding in the diagnosis of dementia. In a recent study, the sensitivity of the test was reported to be .85 (95% confidence interval [CI] = [.74, .92]) and the specificity was .90 (95% CI = [.82, .95]; Creavin et al., 2016).
A secondary outcome was neuropsychiatric symptoms measured by the neuropsychiatric index (NPI; Cummings, 1997). Measures to assess neuropsychiatric outcomes varied widely across studies, with several studies found to be using country-specific measures. However, the NPI is a commonly used questionnaire completed by caregivers to quantify the severity of psychosocial symptoms, including hyperactivity, affect, apathy, and psychosis on a scale from 1 to 12. Test–retest reliability on the NPI was reported as r = .79 for frequency (p = .0001) and a fairly good level of r = .86 for severity (p = .0001; Connor et al., 2008). One advantage of the NPI is its ability to distinguish between different dementia-related symptoms as well as the common symptoms of Alzheimer’s disease, such as euphoria and disinhibition in frontotemporal dementia.
Data extraction and quality assessments
Two evaluators (L.L. and J.A.B.) independently assessed the studies to check that they met the inclusion and exclusion criteria and for risk of bias (RoB), assessed using the Cochrane Collaboration’s RoB tool (Higgins & Green, 2011). Discrepancies were resolved in conjunction with the third author (M.R.T.) via consensus. The results of the RoB evaluation are found in Figure 2. Most of the studies were of intermediate quality as methods were reported in insufficient detail and the randomization process—a crucial component of the Cochrane RoB tool—was poorly described. For instance, though every study mentioned blinding, only two studies indicated allocation concealment. However, RoB appeared to be low overall for the meta-analysis because the reporting of data was of high quality. Algorithms were conducted on data submitted in seven areas: random sequence generation, allocation concealment, anonymization of participants, anonymization of outcome assessments, incomplete outcome data, selective reporting, and other biases. Similarly, data were abstracted from all studies that met the inclusion criteria using a pilot-tested data-abstraction form (formulae to calculate the standardized mean difference) by two of the investigators (L.C. and L.L.) independently. Disagreements were resolved through discussion or consultation with the first author (J.A.B.). The US National Institutes for Health quality assessment tool for controlled-intervention studies was used to assess the quality of the trials (14 items ranked 0, 1, or not applicable, with 1 representing adequate quality).
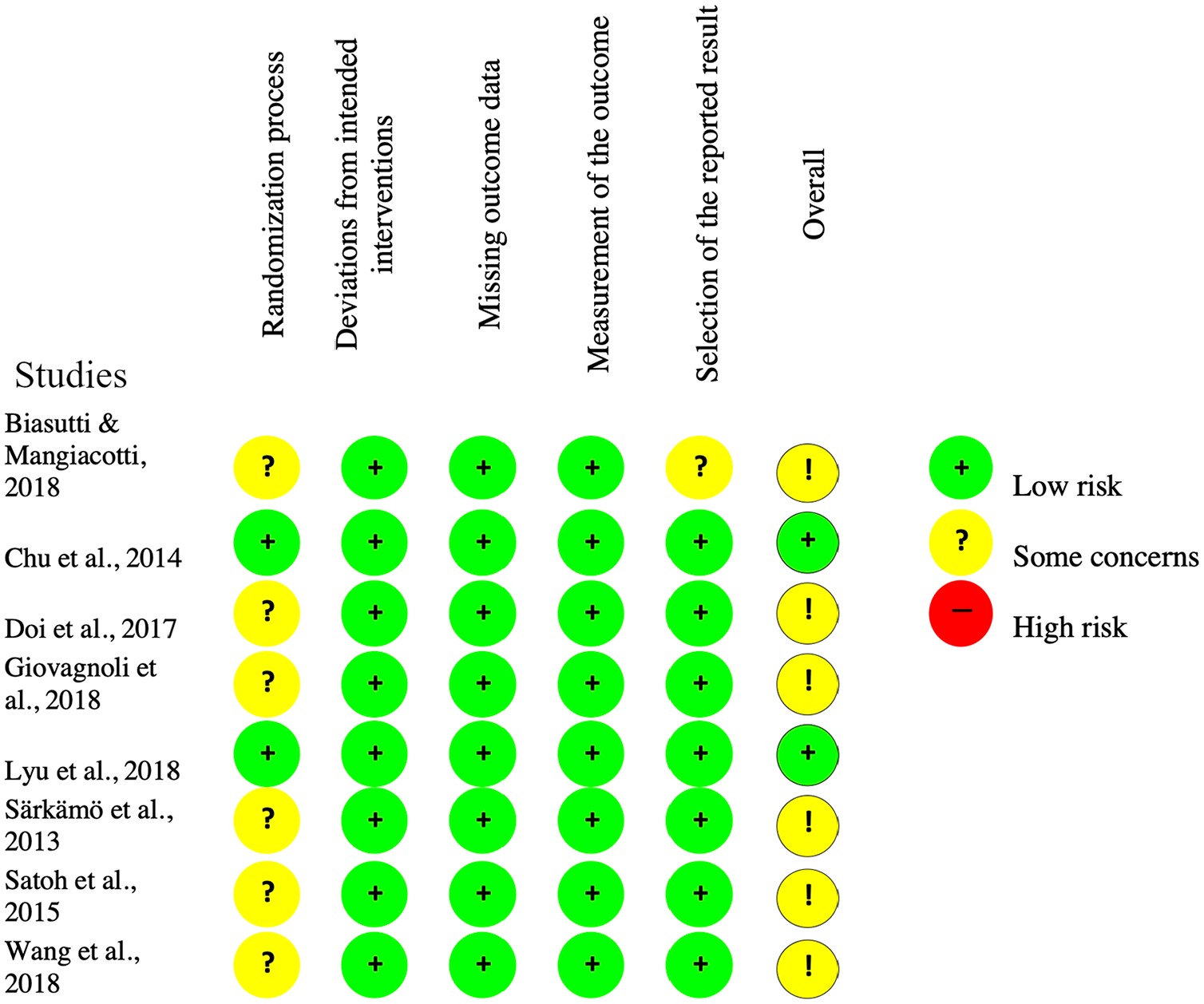
Risk of bias evaluation.
Data synthesis
Meta-analysis was performed to integrate the outcomes of the RCTs. The primary outcomes included MMSE and NPI. Data were pooled and analyzed using Review Manager 5.3 Software (RevMan (2018), Cochrane Collaboration, Oxford, UK). Outcomes were presented as continuous variables. As standardized mean difference (SMD) is more generalizable than mean difference (MD), we used Cohen’s SMD with 95% CIs for statistical efficacy analysis. Cochran’s Q test and I2 statistic were used to examine overall heterogeneity between studies (I2 > 50% indicated substantial heterogeneity). The fixed-effect model was applied to estimate the SMDs with 95% CIs because of the absence of marked heterogeneity in this meta-analysis. Sensitivity analysis was conducted to test the robustness of the results if any single study were to be omitted. An alpha of .05 (two-tailed) was considered statistically significant for all tests. The systematic review and meta-analysis were conducted according to the Cochrane guidelines. We followed the PRISMA guidelines for reporting systematic reviews.
Results
Screening studies and study selection
Our search produced a total of 1,207 results. After they had been screened for duplicates, 747 remained. These studies were filtered by type of article, topic, and relevancy to music and cognition. One hundred thirty-nine article abstracts were screened manually, and 24 full texts were obtained for review and quality assessment using the Cochrane RoB tool. Of these studies, six were excluded that did not include patients with dementia, three were excluded because they were pilot studies without a control group, two because they were not designed to test the effectiveness of the music intervention, two because they used multimodal or movement-based programs, and four because cognitive function was not measured using the MMSE or NPI. Seven RCTs met the inclusion criteria, and a Google Scholar search identified two additional articles for inclusion.
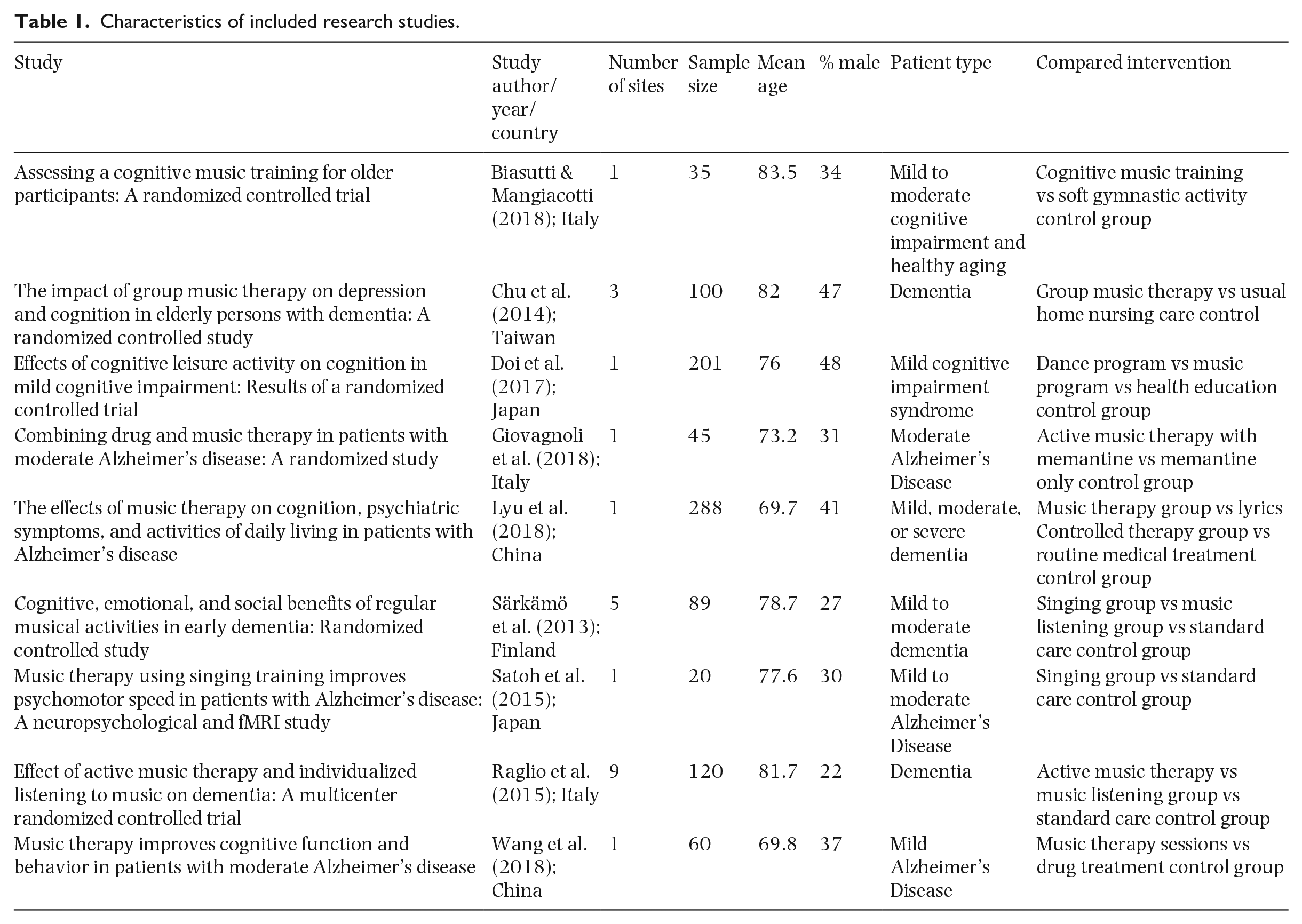
Summaries of the characteristics and outcomes of the nine studies included in this review are provided in Tables 1 and 2, respectively. Four of the studies used a singing program (Lyu et al., 2018; Särkämö et al., 2013; Satoh et al., 2015; Wang et al., 2018), three used an instrumental-music program (Doi et al., 2017; Giovagnoli et al., 2018; Raglio et al., 2015), and two used a combined singing and instrumental-music program (Biasutti & Mangiacotti, 2018; Chu et al., 2014). In five studies, participants were described as having mild to moderate dementia or cognitive decline; in two studies, participants were diagnosed with Alzheimer’s disease; and in two studies, the type of dementia was not specified.
Characteristics of included research studies.
Outcome measures for included studies.
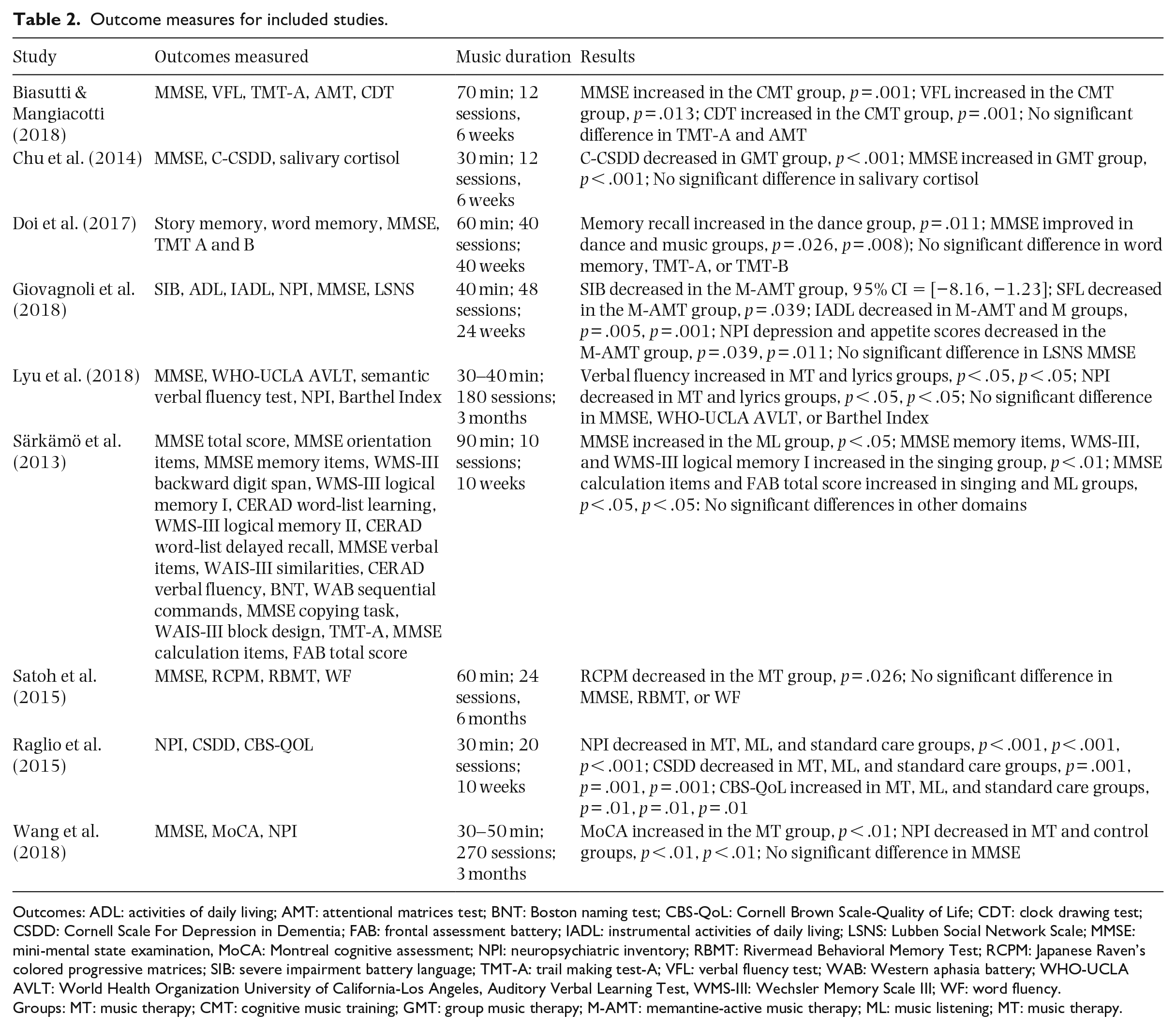
Outcomes: ADL: activities of daily living; AMT: attentional matrices test; BNT: Boston naming test; CBS-QoL: Cornell Brown Scale-Quality of Life; CDT: clock drawing test; CSDD: Cornell Scale For Depression in Dementia; FAB: frontal assessment battery; IADL: instrumental activities of daily living; LSNS: Lubben Social Network Scale; MMSE: mini-mental state examination, MoCA: Montreal cognitive assessment; NPI: neuropsychiatric inventory; RBMT: Rivermead Behavioral Memory Test; RCPM: Japanese Raven’s colored progressive matrices; SIB: severe impairment battery language; TMT-A: trail making test-A; VFL: verbal fluency test; WAB: Western aphasia battery; WHO-UCLA AVLT: World Health Organization University of California-Los Angeles, Auditory Verbal Learning Test, WMS-III: Wechsler Memory Scale III; WF: word fluency.
Groups: MT: music therapy; CMT: cognitive music training; GMT: group music therapy; M-AMT: memantine-active music therapy; ML: music listening; MT: music therapy.
The average age of participants in all the studies was 75.5 years. The number of music intervention sessions delivered ranged from 10 to 180 and the length of each session was from 30 to 90 min. The outcomes of each study were measured immediately after the defined intervention had ended, and these data were used in analyses reported below. Insufficient information was included in these studies for follow-up data to be analyzed or subgroup analysis to be carried out. Other study variables, such as length of interventions, length of sessions, and the qualifications of staff, were not assessed due to the heterogeneity of interventions across studies and the limited information provided about these variables.
MMSE scores
Eight of the studies included in the meta-analysis measured the effect of music interventions on MMSE scores (Biasutti & Mangiacotti, 2018; Chu et al., 2014; Doi et al., 2017; Giovagnoli et al., 2018; Lyu et al., 2018; Särkämö et al., 2013; Satoh et al., 2015; Wang et al., 2018). Overall, a significant improvement in MMSE scores was found through meta-analysis. I2 was 0% and a Q test for between-study variance showed no heterogeneity among the studies. The standardized mean difference (SMD), representing the size of the effect of the music intervention in each study, was used as a summary statistic in the meta-analysis of MMSE scores. The total value of SMD was .20, significantly greater than 0, revealing a significant improvement in MMSE scores among groups that had received music interventions (95% CI = [.04, .36], p = .01; see Figure 3) although the effect size (Cohen’s d) was small (Cohen, 1988).
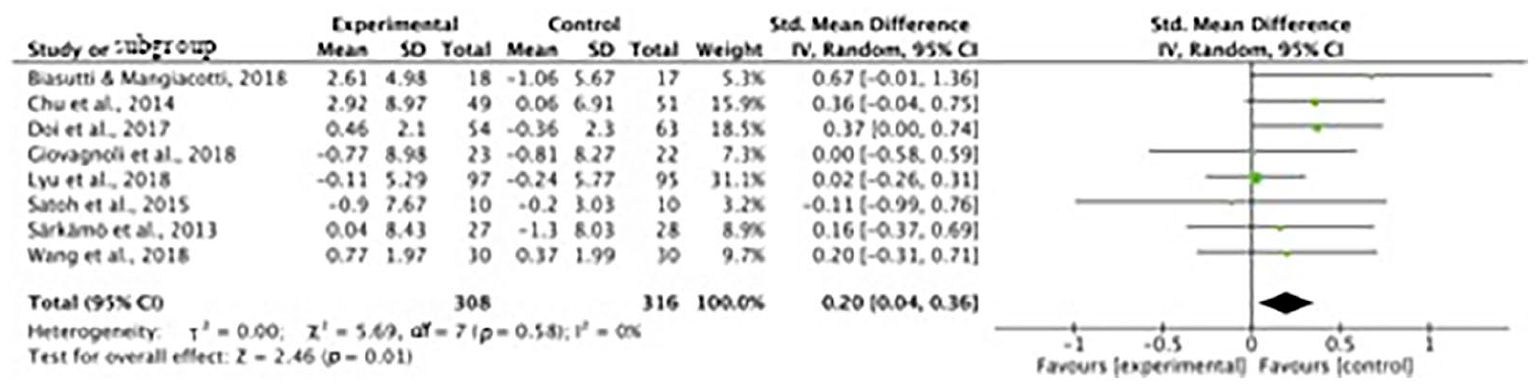
Standardized mean difference (SMD) for MMSE scores.
NPI scores
Four of the studies measured the effect of music interventions on NPI scores (Giovagnoli et al., 2018; Lyu et al., 2018; Raglio et al., 2015; Wang et al., 2018). A significant decrease in NPI scores was found. I2 was 0% and a Q test for between-study variance also showed no heterogeneity among included studies. SMD for each included study was calculated and summarized in the meta-analysis for NPI scores, and the total SMD value was −0.23, suggesting a significant decrease in neuropsychiatric symptoms among groups that had received music interventions (95% CI = [−.43, −.02], p = .03; see Figure 4).

Standardized mean difference (SMD) for NPI scores.
Discussion
Our results suggest that patients with dementia experienced a significant improvement in cognitive function and fewer neuropsychiatric symptoms following active music interventions in comparison with control groups. The clinical measures used in this systematic review (MMSE and NPI) are two of the most reliable and commonly used (Schmitt & Wichems, 2006). Although effect sizes were small, there are few published RCTs using active music interventions, and many were conducted using small samples. For example, in the study by Satoh et al., only 20 participants (10 experimental, 10 controls) were enrolled in the study. Other studies included in the meta-analysis also had small sample sizes, including Biasutti and Mangiacotti (2018) with 35 participants (18 experimental, 17 controls) and Giovagnoli et al. (2018) with 45 participants (22 experimental, 23 controls). Other systematic reviews of the music therapy literature have also indicated the need for further RCT studies to be carried out (Kamioka et al., 2014). In our meta-analysis, sample sizes ranged from 20 to 288 participants. It is also worth mentioning that the RCTs discussed in this meta-analysis included patients with mild-to-moderate dementia. Further research is necessary to examine the effects of active music therapy programs and interventions for patients with severe dementia. Nevertheless, our results are consistent with those of a recent review of literature that showed improved cognitive function in healthy older adults who participated in active musical performance (Schneider et al., 2019).
This systematic review and meta-analysis included a focus on the benefits of active music therapy and interventions in older adults with dementia, tested via RCTs. Research included in our analysis offered some form of cognitive stimulation (e.g., lyric reading) as the control task. However, the time spent in carrying out control tasks varied across studies. In addition, many meta-analyses focus on art-based interventions collectively, failing to differentiate between outcomes relevant to specific art forms. For example, a systematic review by Schneider (2018) evaluated the effects of visual arts, music, and dance on social and behavioral outcomes in dementia patients. However, the music interventions included only passive music listening.
Music interventions involve engagement with complex temporal sequential stimuli that have long been associated with neuroplasticity and enhanced cognitive outcomes (Maes et al., 2017). While our results suggest an improvement in MMSE scores after active music interventions, there are several limitations to this study. In the currently available literature, there are few RCTs that measure executive functions and cognition after a music intervention. Instead, many studies have examined changes in mood, behavior, anxiety, and agitation. Additional reasons for excluding studies included a lack of control groups and inconsistent measures of cognition among RCTs (e.g., the use of the Montreal Cognitive Assessment (MoCA) rather than the MMSE). Several studies utilized multimodal interventions or incorporated a dance or movement-to-music component. These studies were also excluded due to their focus on movement, making it different to distinguish confounding variables (Schneider, 2018).
Questions arise from our findings that necessitate future research. Although the original aim of our review was to test the claim that interventions involving active music-making are more effective for older people with dementia than passive music interventions, we cannot conclude from our results that music interventions with active components are more effective than passive music listening interventions, because we did not find enough relevant studies. We therefore modified our approach to compare the outcomes for participants who took part in music interventions with nonmusic controls. Only two of the studies compared a singing intervention to a music-listening intervention. Särkämö et al. (2013) reported that the music-listening group scored higher on the MMSE than those in the singing intervention, as compared to controls. However, they also found that the singing intervention improved attention and working memory in comparison with the music-listening intervention and standard treatment control groups. In a separate study that examined psychosocial outcomes following a 20-session instrumental-music intervention, a music-listening intervention, or standard treatment, researchers found that all groups demonstrated enhancements in psychosocial outcomes of depression symptoms, neuropsychiatric symptoms, and quality of life (Raglio et al., 2015).
Taken together, these results suggest that there is a need to differentiate the effects of active and passive music interventions on cognition by using a variety of research paradigms that account for external factors such as motivation, personality, and prior experiences. An important question for future research is whether active music interventions are truly more beneficial than music listening alone and whether integration of the two types of interventions could generate additional benefits.
Many RCTs use different dosages of music interventions. In this meta-analysis, total intervention time ranged from 360 to over 10,000 min. There is a need for studies using standardized music interventions in which dosage, time, and intensity are quantified and reported rigorously. Reporting standards for RCTs should require reports of dosage as well as administration of music protocols by qualified music therapists and educators (Schneider et al., 2019). The qualifications of staff involved with the administration of standardized measures need to be considered and consistency among interventions and measures must be ensured.
Furthermore, little is known regarding the sustainability of benefits from active music interventions. Although some studies reported follow-up results, our analysis of long-term effects was limited by variations in the modality and dosage of the interventions, and when (and how often) the effects were tested. The results of studies that followed participants longitudinally appeared to be highly variable. Särkämö et al. (2013) reported that benefits to general cognition found immediately after the intervention were no longer demonstrated after six months. In contrast, Wang et al. (2018) reported that MMSE scores continued to improve in control and intervention groups after a 3-month follow-up. More studies are required to establish a clearer understanding of how long cognitive benefits are maintained after the music intervention.
The social aspects of music interventions may influence cognitive function, so it is important for study designs to include active control conditions providing a similar social environment. Social behaviors can influence mood and reduce agitation. In one study, researchers found decreases in agitated behaviors after a 4-week music program that integrated movement (Sung et al., 2006). Similar findings of reduced agitation were reported after music therapy sessions with group interaction, such as the playing of instruments, and dance, in participants with Alzheimer’s disease (Gallego & Garcia, 2017). The results suggest that participants’ moods were positively influenced not only by the musical activities but also by their social interactions.
The selection of appropriate standardized measures for clinical populations that examine constructs to isolate specific aspects of cognition or quality of life is methodologically demanding (Ibanez et al., 2014). Task impurity is an issue when assessing patients with dementia, as tests to measure executive functions may not correlate with the progression of the disease. Task impurity issues also arise when the task also evaluates several other domains of cognition (Snyder et al., 2015). The overlap among areas of cognitive processes presents further challenges when assessing executive functions.
The quality of studies included in the meta-analysis also requires consideration. The Cochrane RoB tool provides a framework for assessing the validity of RCTs. While the Cochrane RoB guidelines were followed, many of the studies included in the meta-analysis provided substandard quality assessments. In many cases, it would have been impossible for full experimental control to have been achieved. For example, research cannot be truly double-anonymized, as participants are inevitably aware that they have been assigned to receive either a music or a non-music intervention. Lack of anonymizing makes such studies subject to the Hawthorne effect. Additionally, prior musical experiences, music aptitude, and music achievement were not considered in study designs. These variables may have had an impact on the effectiveness of the intervention.
In further research, factors including subtypes of dementia and gender should be differentiated to determine which nonpharmacological interventions may be most effective, as is standard practice for medical research (Health Quality Ontario, 2014). Research with participants diagnosed with mild to moderate dementia often fails to specify its type (e.g., Alzheimer’s disease, vascular dementia, frontotemporal dementia). Many studies using music-based interventions recruit more women than men. Subgroup analysis based on gender in future studies may reveal whether it has an impact on study results.
Despite these limitations, our findings suggest a small positive effect of active music interventions on cognitive function in patients with Alzheimer’s disease. The strengths of our review include bringing research using active music interventions to the attention of researchers, psychologists, and gerontologists. In future, the consideration of experimental design based on the studies included in this systematic review and meta-analysis will contribute to the careful conduct of RCTs using consistent standardized measures with larger, more diverse samples. In addition, we found reduced neuropsychiatric symptoms in our meta-analyses with research referencing reductions in depression and anxiety as well as global NPI scores (Giovagnoli et al., 2018; Lyu et al., 2018; Raglio et al., 2015).
Conclusion
The findings of this systematic review and meta-analysis suggest that, while active music interventions have significant effects on cognitive function and neuropsychiatric symptoms, there is still a need for a rigorous approach to the identification of the effects of active music interventions on older adults with dementia. Many other gaps in research were identified, including the need for standardized outcomes, larger sample sizes, and similar music interventions. In future studies, these issues should be addressed and explored to examine sustainability and add more specificity and nuance to music interventions.