
Abstract
Current music therapy studies published in the field of dementia can often lack specificity in communicating the components of a music therapy intervention. These interventions can involve a wide range of musical activities depending on patient needs. This survey aimed to explore the use of singing, listening, playing instruments and movement with music, by music therapists working with people living with dementia, to further understand music therapists’ preferences, proclivities and clinical motivations. In total, 31 UK registered music therapists participated. The survey collected data on personal, clinical and external influences on therapists’ selection of musical activities during music therapy sessions. Analysis was completed using descriptive statistics and reflexive thematic analysis. The results showed that singing initiated by the therapist is the most common musical activity used by music therapists in this study. Reasons include therapists selecting activities that were comfortable and familiar, and those that provided musical flexibility in a clinical setting. There was also a connection found between the use of various musical activities and clinical aims. Further research can develop understanding on how various musical activities can fulfil specific needs of people living with dementia This can raise awareness for future music therapists and caregivers to choose the most appropriate musical intervention in a clinical setting.
Introduction
As of February 2023, there were 438,213 people diagnosed with dementia in the United Kingdom according to the National Health Service (NHS) Official Statistics (NDRS, 2023), with a predicted rise to approximately 1 million by 2030 (Dementia Statistics Hub, 2023). It is also estimated by the Alzheimer’s Research UK Dementia Statistics Hub that 52% of the population in the United Kingdom are impacted by dementia either through their own diagnosis or through a close family member (Public Attitudes Towards Dementia, 2021).
When considering care for people living with dementia, music therapy is becoming a common intervention with the aim of improving cognition and reducing symptoms. Recent studies included in a systematic literature review (Lin et al., 2023) show that music therapy can improve cognition, reduce neuropsychiatric symptoms and improve quality of life for people living with dementia. This review also recognises that many medical dementia treatments can have unwanted side effects, and that music therapy is a safe intervention. The most recent Cochrane review on music-based therapeutic interventions for people with dementia identified that future music research requires further clarity into the types of musical activities used for people living with dementia (Van der Steen et al., 2018). In particular, systematic literature reviews identify that music therapy studies often lack clarification as to what is involved in a music therapy intervention and recommend that future research incorporate more detailed, standardised interventions (Aleixo et al., 2017; Lam et al., 2020; Moreno-Morales et al., 2020; Vink and Hanser, 2018). To include more detail as to what is involved in a music therapy intervention, more specificity can be given on the details of the intervention such as instruments used, the proportion of various musical activities, group size and specific repertoire (Vink and Hanser, 2018). This is in addition to the proportion of various musical activities used in each session (Lam et al., 2020) which can often involve a wide variety of activities (Robb et al., 2011). Recent research is beginning to include this detail such as in the MIDDEL (Music Interventions for Depression and Dementia in ELderly care) study (Schneider et al., 2024) and should continue to do so.
In the United Kingdom, music therapists must complete a master’s degree programme in music therapy as well as be registered with the Health and Care Professions Council (HCPC), achieving and maintaining certain standards to remain registered and able to practise (HCPC, n.d.). Although there are specific standards to maintain for qualified music therapists, the use of music for people living with dementia in the United Kingdom across the whole spectrum (such as used by community musicians, professional musicians providing concerts for wellbeing) was identified in the Commission on Dementia and Music Report (Bowell and Bamford, 2018), as poorly coordinated. Based on these findings, it was recommended to ‘coordinate delivery and build intelligence’ through paths such as following a consistent format and developing resources which will combine best practice, as well as to ‘support individuals to find the right intervention at the right time’ (Bowell and Bamford, 2018). More recently, a UK-based audit of music therapy for people living with dementia has identified that there is a need to further understand how music therapy can impact this client group to improve training, collaboration and fulfilling the needs of the patients (Thompson and Odell-Miller, 2022). This research acts on the recommendations made by the commission, by uniting the approaches of music therapists throughout the United Kingdom based on the type of musical activity used for various clinical aims.
This study was a component of a PhD research project (Crabtree, 2023) embedded in an international, multisite randomised controlled trial investigating the effectiveness of a music and reading intervention for people living with dementia and their informal caregivers living at home. The trial was called home-based family caregiver-delivered music and reading interventions for people living with dementia (HOMESIDE; Baker et al., 2019, 2023). The trial recruited 864 participants in 432 dyads across five countries. The questions designed for the survey, therefore, reflect four main musical activities used in the HOMESIDE study (Odell-Miller et al., 2022). The PhD embedded within the HOMESIDE study aimed to identify the rationale for the use of singing, listening, playing instruments and movement with music to improve cognition and reduce neuropsychiatric symptoms in people living with dementia. The study further explored the various musical activities used by music therapists and informal caregivers with people living with dementia considering personal preferences, proclivity and clinical motivations (particularly improving cognition and reducing neuropsychiatric symptoms). In the HOMESIDE study, the Mini-Mental State Examination (MMSE) (Folstein et al., 1975) and Neuropsychiatric Inventory Questionnaire (NPI-Q) (Cummings et al., 1994) outcome measures were used to identify specific cognitive domains and symptoms of dementia.
Method
Participants
The participants of the following research included music therapists registered with the HCPC with any length of experience working with people living with dementia across all settings within the United Kingdom. The participants were recruited through the British Association for Music Therapy (BAMT) via their area groups and dementia network. These groups were communicated with via email and a reminder to complete the survey was also sent before it closed.
The survey took place over the summer of 2021 and closed in November 2021. In August 2021, BAMT had 905 registered therapists in the category of full practitioner and newly qualified practitioner members (BAMT, 2024, personal communication, 7 February). As of January 2022, there were 1278 music therapists registered with HCPC (HCPC, 2023, personal communication, 14 November).
The survey aimed to recruit a sample size of 30 participants to complete the survey based on a confidence level of 95% and a margin of error at 16%. This is based on there being around 130 qualified and HCPC registered music therapists working in the United Kingdom with people living with dementia around the time of the survey call, who were within the BAMT network for dementia, and who therefore could be invited to participate.
Design
The survey was created using OnlineSurveys (Jisc, 2023) which was used for the design, distribution and data collection.
The survey was designed to answer the following research questions:
Which musical activities are used most among music therapists working with people living with dementia in the United Kingdom and why?
What are the personal reasons of music therapists for these musical activities to be used?
What are the clinical aims that trigger the use of certain musical activities to be used?
What external factors influence the use of musical activities considering collaborators and online working?
For this survey, the term ‘personal’ refers to any factors that are individual to each music therapist. This may be a particular proclivity towards their use of different musical activities such as a habit developed in training, unconscious preferences or known likes and dislikes. Other terms such as ‘musical activities’ were not defined and were left to the participants’ interpretation.
The survey questions were designed based on the research questions and used a mixed methods approach. This included mostly multiple-choice questions with some free-text questions to provide the participants with the opportunity to explain any additional reasoning behind their answer. Some survey questions utilised a mixture of set themes such as the four musical activities and an ‘other’ category. All other questions used open themes. Questions were also based on the framework of the HOMESIDE study (Baker et al., 2019, 2023) and the MMSE (Folstein et al., 1975) and the NPI-Q (Cummings et al., 1994) outcome measures. This allowed the questions to relate directly to specific cognitive domains and symptoms of dementia.
Analysis
Quantitative data from the multiple-choice questions were analysed using descriptive statistics and the qualitative data were analysed using reflexive thematic analysis (Braun and Clarke, 2019; Byrne, 2022). The descriptive statistics were computed based on the number of participants who had responded with a certain answer for each multiple-choice question. Reflexive thematic analysis was used for the free-text responses. This method emphasises the researcher’s active role in identifying patterns and themes, acknowledging their own perspectives and experiences as part of the analytical process. The decision to use both forms of analysis followed from the research questions, which invited an overview of how music therapists work but also a deeper exploration of how individual music therapists think and approach their clinical work. The survey design, which utilises set multiple-choice responses as well as open-text responses, also aligns well with using a mixed method approach.
During analysis, it was identified that more practical components such as the difference in training, experience and maturity of the music therapist may also contribute to a difference in how musical activities were used. Although information about age or training was not collected, further analysis was conducted based on number of years since qualification as a music therapist.
Ethics
Ethics approval for this survey was granted through Anglia Ruskin University. All music therapists who took part were eligible to participate and consented to completing the survey.
Results – demographics
The results show the responses shared in the survey from the first to last question. This therefore addresses the demographics, reasons for using various musical activities including personal, clinical and collaborative reasons and finally influences of in-person versus online working. The last section of the results addresses additional analysis that was completed based on the responses. Within some of the survey questions, participants were able to choose multiple answers to represent multiple experiences and therefore these numbers make a total of 60 responses, rather than 31 which was the total number of participants.
In total, 31 music therapists in the United Kingdom took part in the survey. Figure 1 shows the number of years qualified as music therapist for the participants. This was comprised of music therapists qualified for <1, 1–3, 4–6, 7–9, 10–19 and 20+ years. Most music therapists had been qualified for 1–3 years.
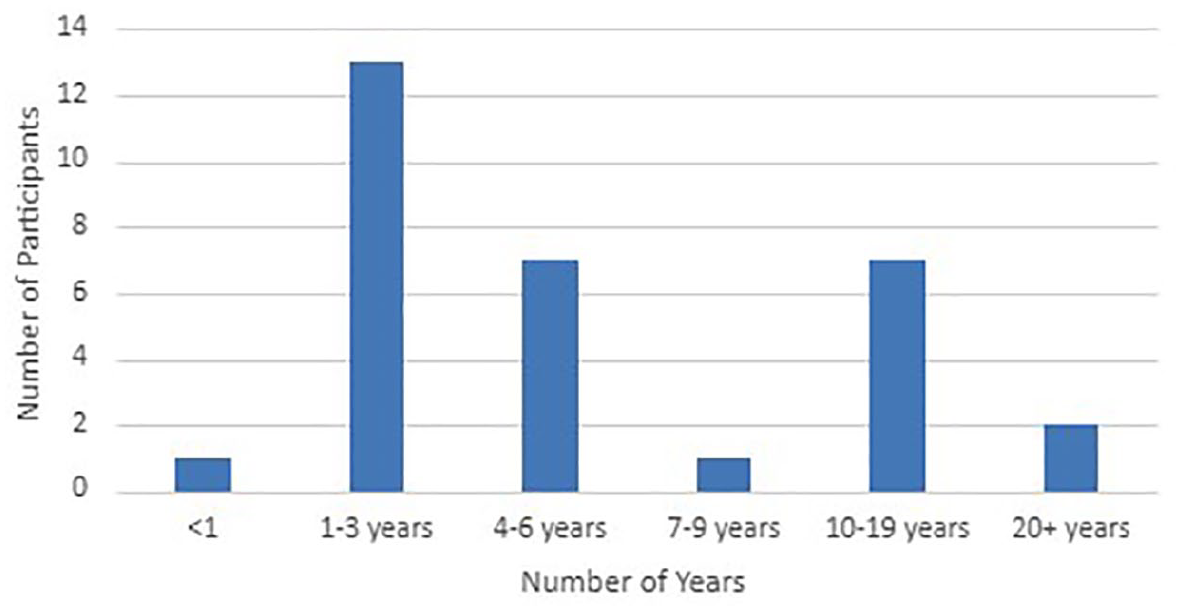
Number of years qualified as a music therapist.
Out of these participants, most music therapists had worked with people living with dementia for between 1 and 6 years. This is seen in Figure 2.
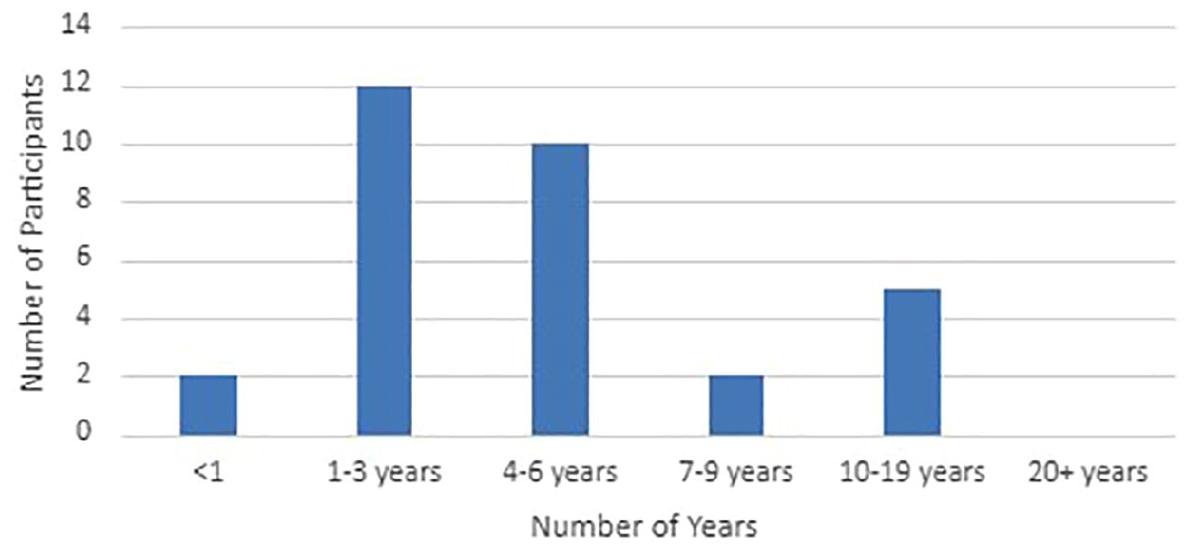
Number of years working as a music therapist with people with dementia.
Figure 3 shows that out of the 31 music therapists who participated in the study, the most common workplace was residential care homes followed by nursing homes. Others also worked in hospitals and in the community.
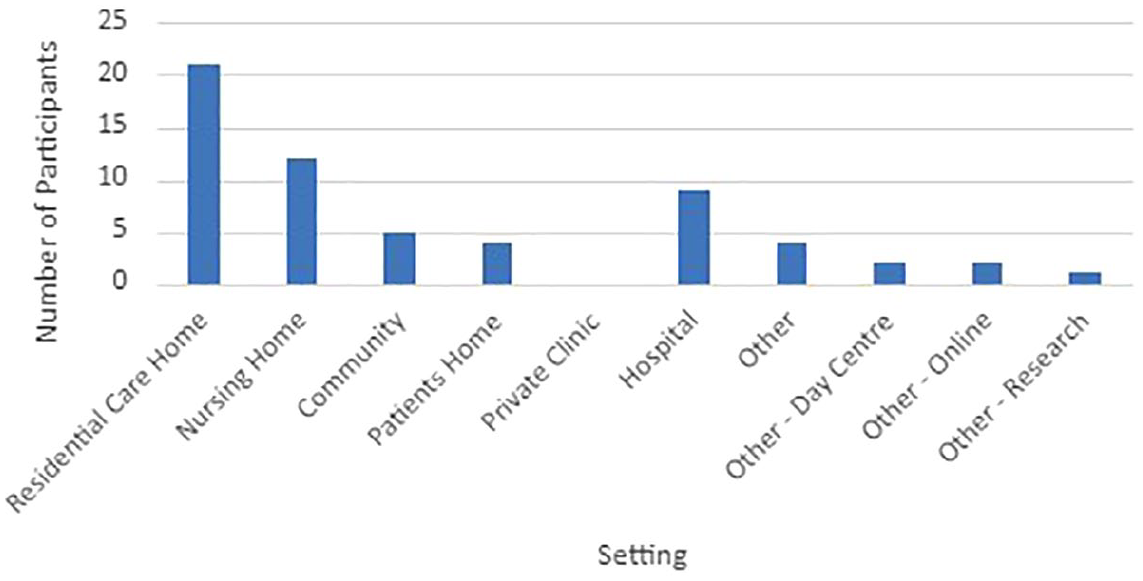
Types of settings music therapists work in.
Results – musical activities used and personal rationale
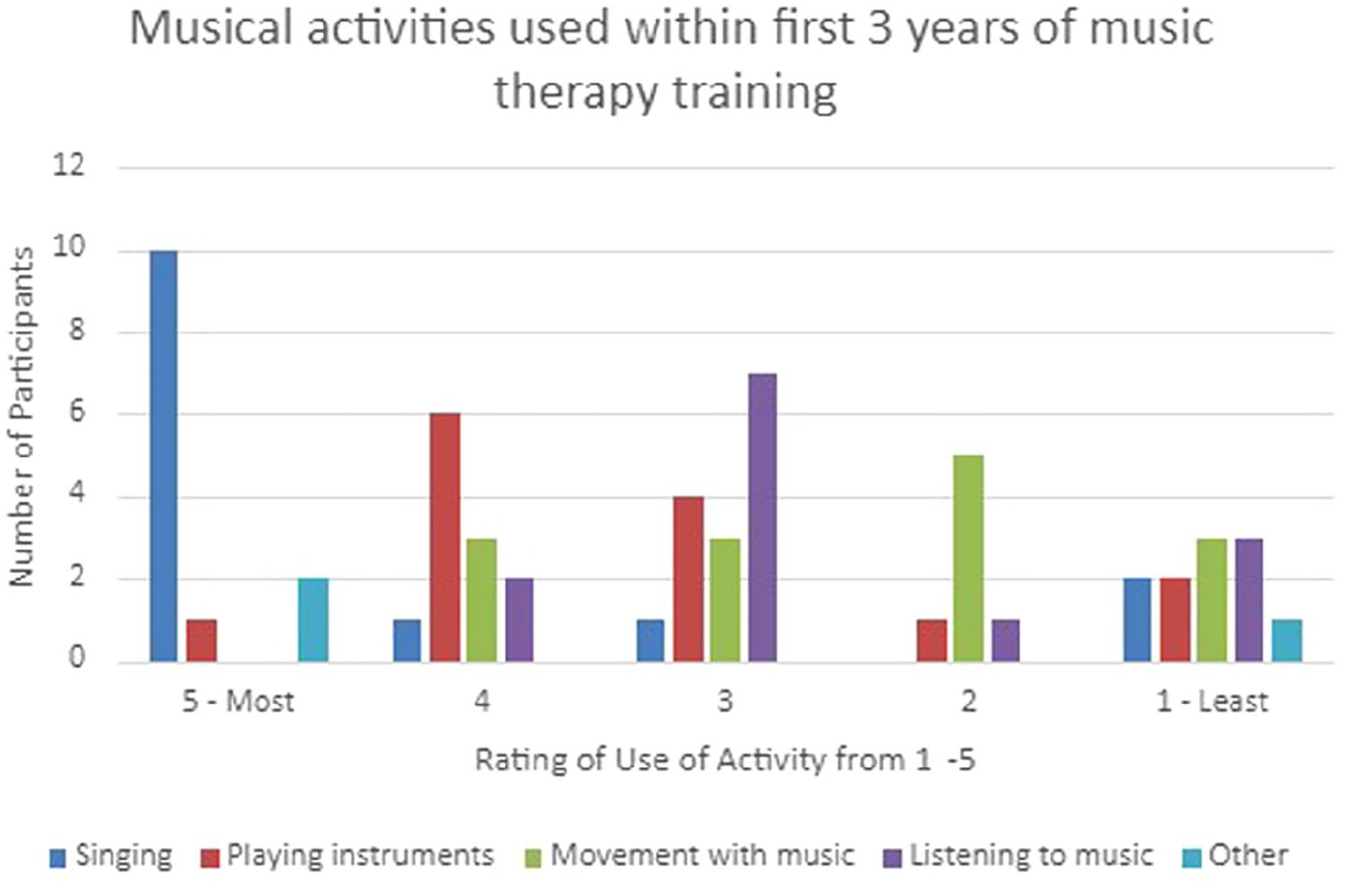
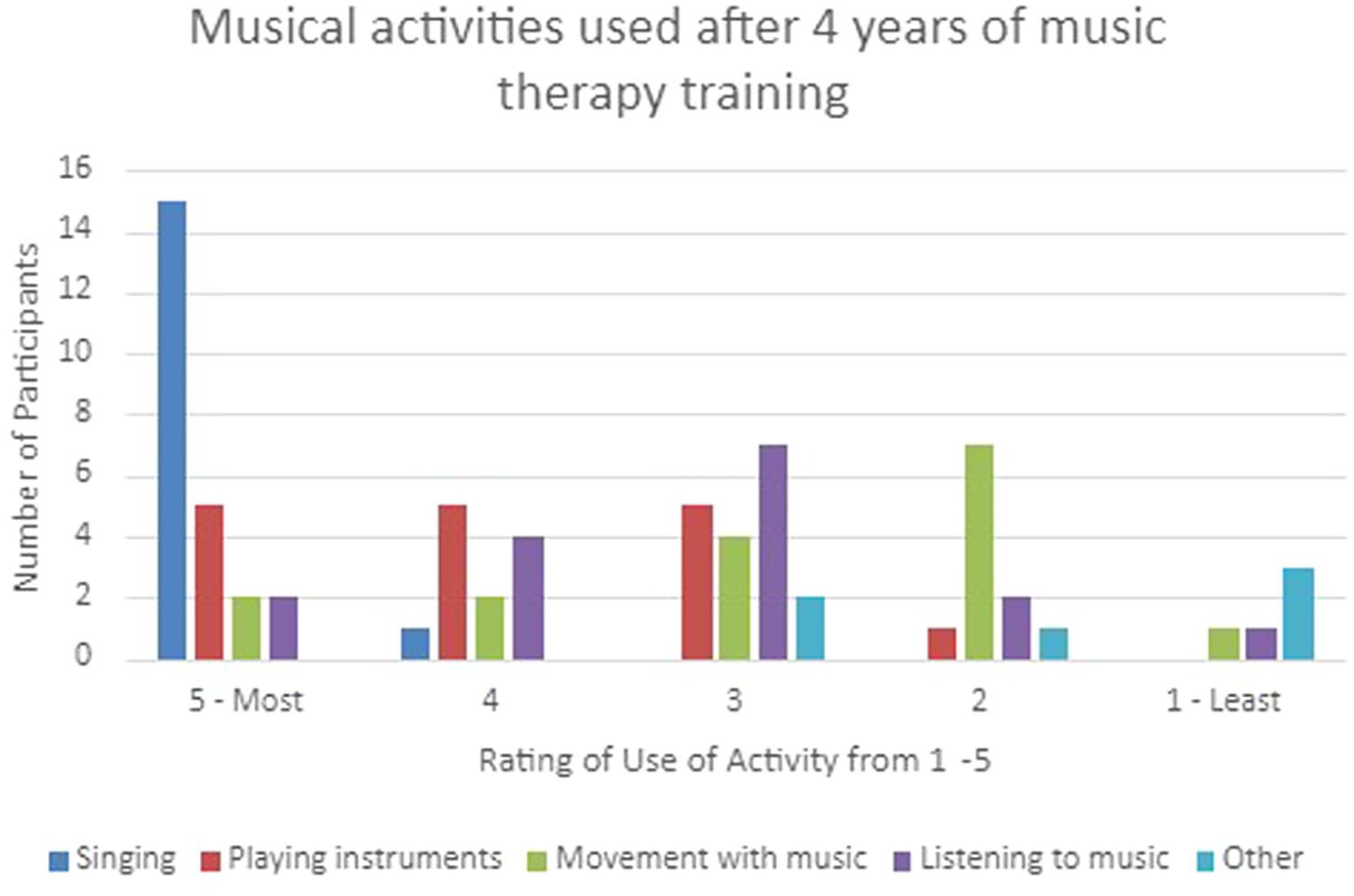
Music therapists who participated in the survey were then asked to rate their use of singing, listening, playing instruments, movement with music and/or other on a scale of 1–5 with 5 being the most frequently used activity and 1 being the least frequently used. For this survey, the musical activities were not defined and therefore there could be ambiguity between activities which involve multiple actions such as walking around while playing an instrument. For this rating question, participants were able to choose not to rate a musical activity. Although all 31 participants rated singing, playing instruments and movement, only 30 participants rated listening. Only nine rated the ‘other’ option to say that they used a music activity in addition to the four activities mentioned. Overall, Figure 4 shows that the most frequently used activity was singing followed by playing instruments, listening and movement with music.
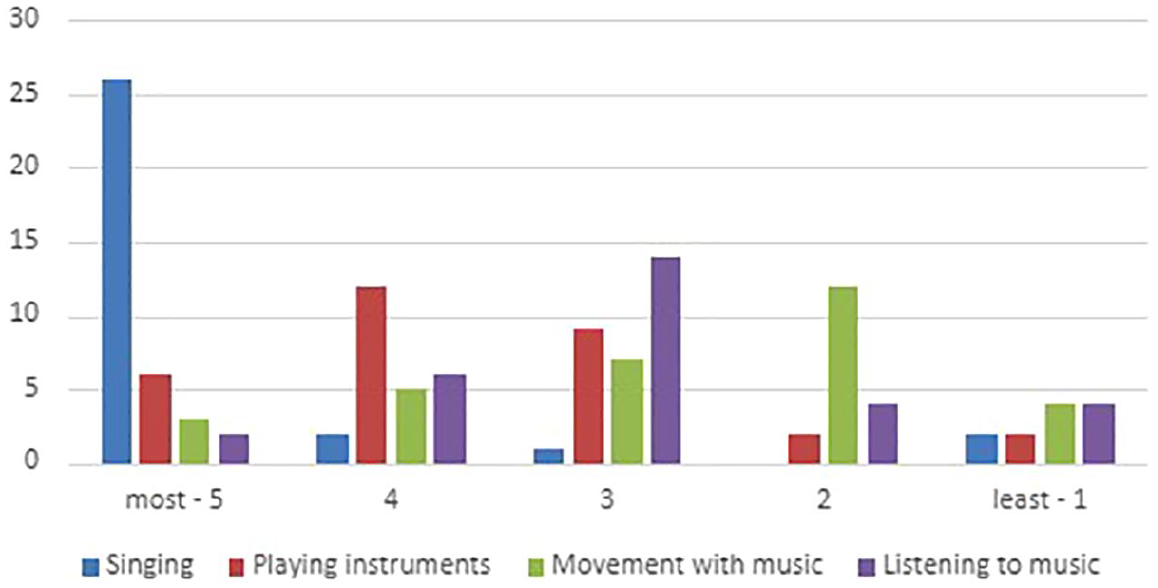
Use of musical activities by music therapists.
Out of the nine participants who suggested they use another activity in addition to the four activities provided, eight specified what those activities were (Figure 5). Song writing, reminiscence and making personal play lists were most common followed by musical tasks such as ‘Pif Paf Poltrie’, a Nordoff and Robbins musical story-game or guessing songs from an excerpt and finally improvisation. It is also helpful to note that some participants had mentioned more than one additional activity, and some music therapists may have considered these activities within the four musical activities provided.
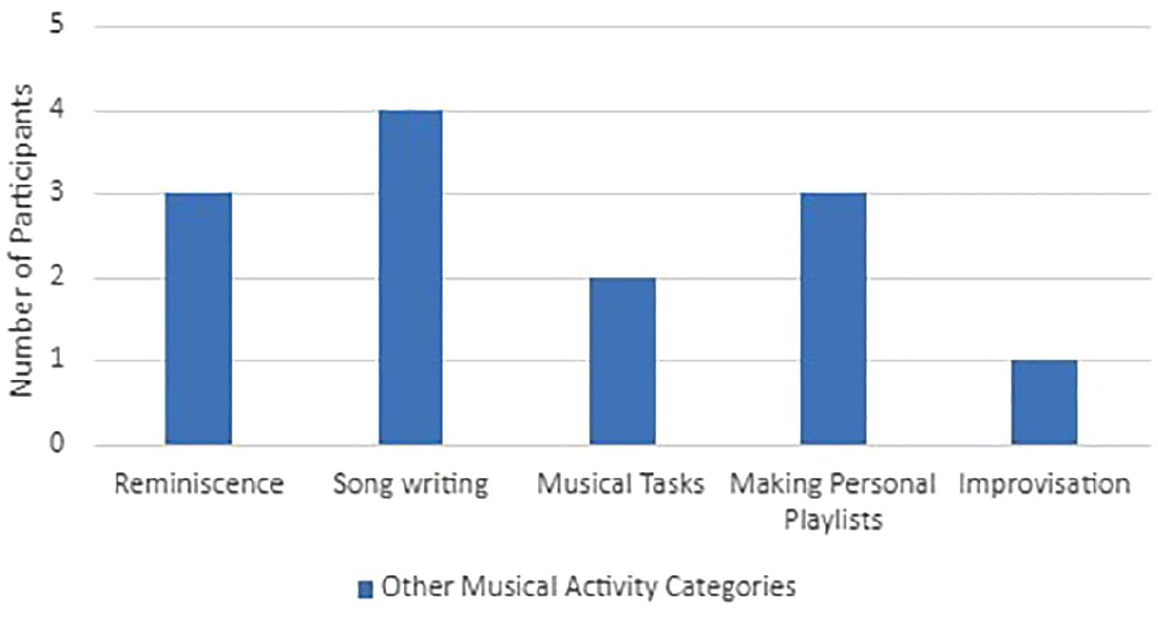
‘Other’ musical activities used.
In addition to the multiple-choice style question asking how frequently the participant used specific musical activities, open-answer questions were also asked to identify any reasons that this may be the case. Figure 6 identifies the themes of the responses and the number of participants who discussed them. All participants provided a free-text response.
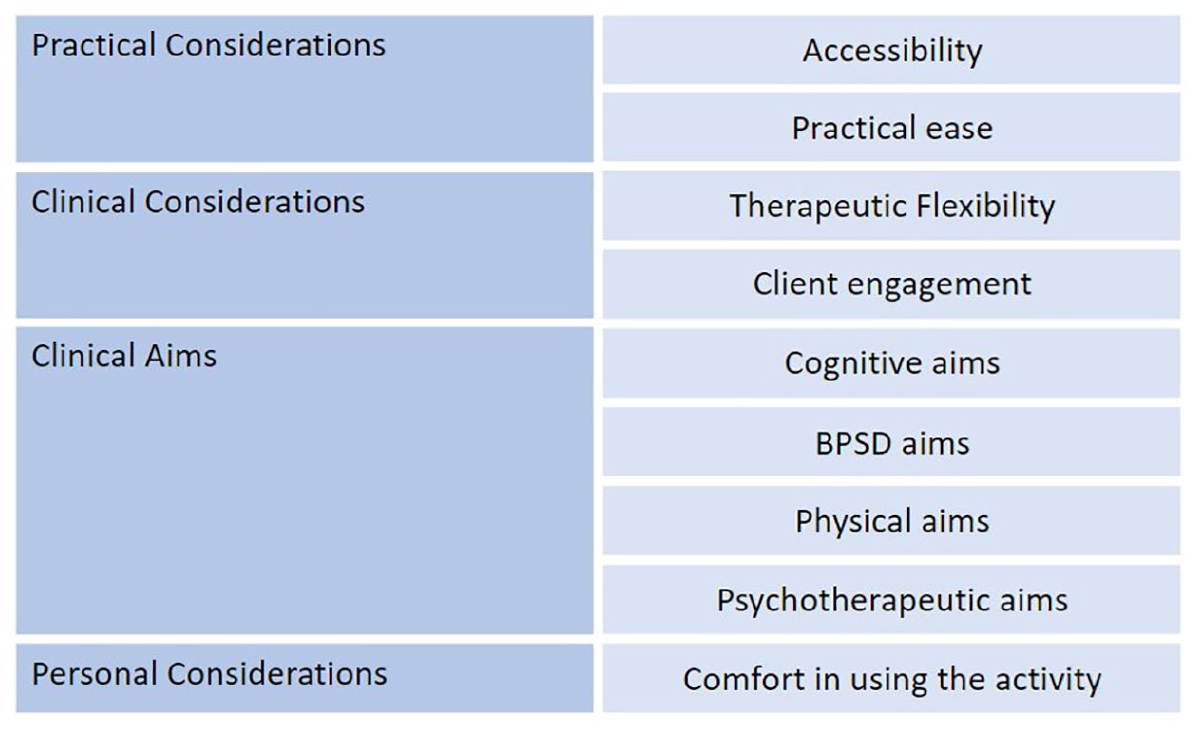
Reasons for using a musical activity.
After identifying general information about which musical activities were used and why, further questions were asked to determine if certain activities were used more depending on specific clinical aims related to improving cognition or reducing neuropsychiatric symptoms in a patient living with dementia. Music therapists were asked to select the musical activity they would be most likely to use when aiming to improve a certain cognitive domain or reduce a certain neuropsychiatric symptom. The choice of musical activities provided included singing, listening, playing instruments, movement with music or other. Participants were able to choose multiple activities or choose to refrain from responding for a specific domain or symptom.
With the aim of improving specific cognitive domains, Figure 7 shows that singing was a frequently used activity. This was specifically the case for orientation (25 participants), memory recall (28 participants) and language (29 participants) of which participants said they would use singing to improve these domains. For short-term memory (27 participants) and attention (29 participants), playing instruments was the preferred musical activity. To improve the visuo-spatial skills domain, movement with music was the most used activity (23 participants).
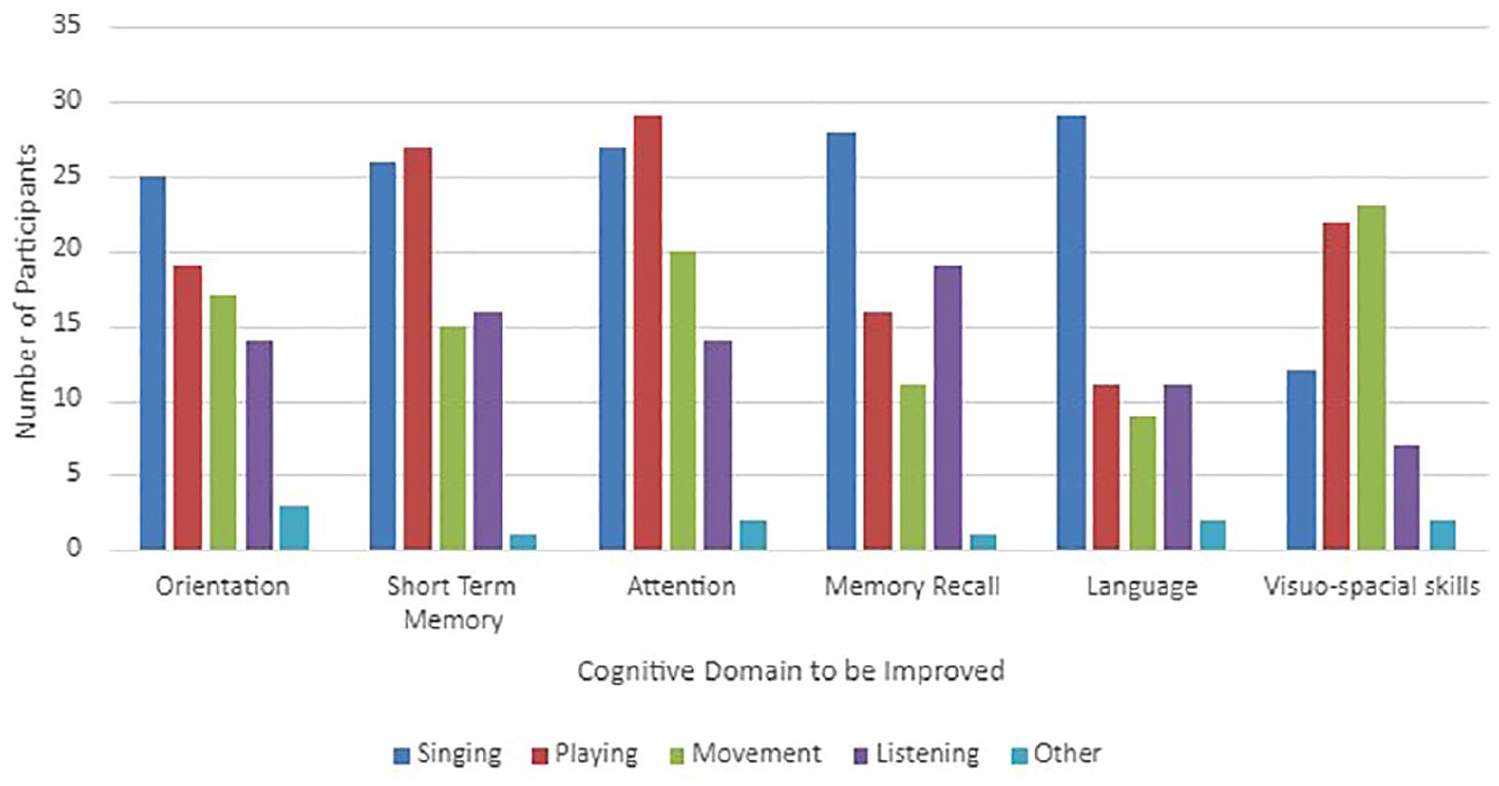
Musical activities used with the aim of improving certain cognitive domains.
Figure 8 shows that singing was also frequently used with the aim of reducing neuropsychiatric symptoms. Singing was the main activity used to reduce five symptoms and tied as the main activity with the use of playing instruments for one symptom and the use of listening for two symptoms. Listening was the most frequently used activity to reduce symptoms of nighttime behaviours (19 participants) and appetite (20 participants) and playing instruments was the preferred activity to reduce motor disturbance (25 participants).
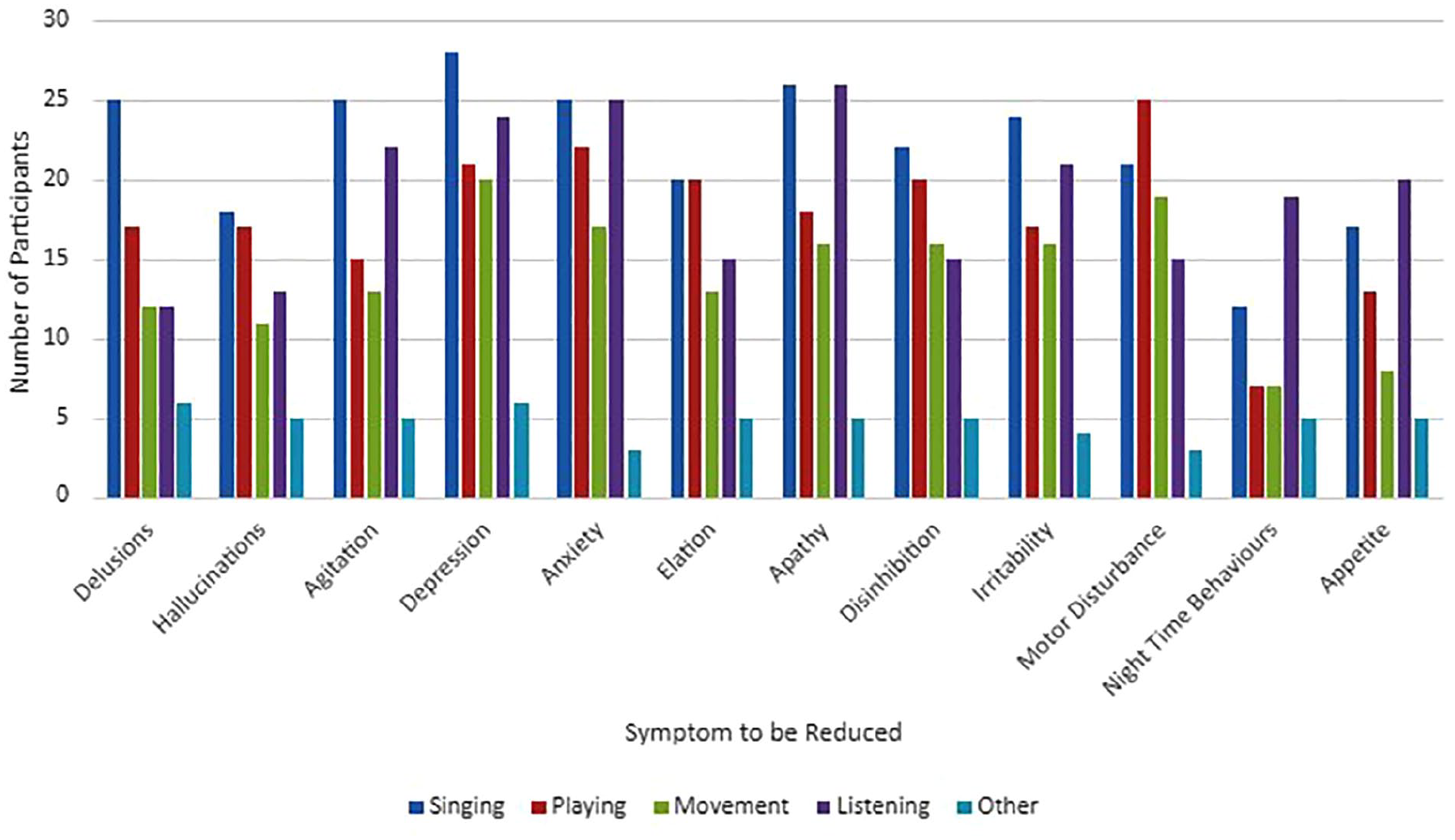
Musical activities used with the aim of reducing certain neuropsychiatric symptoms.
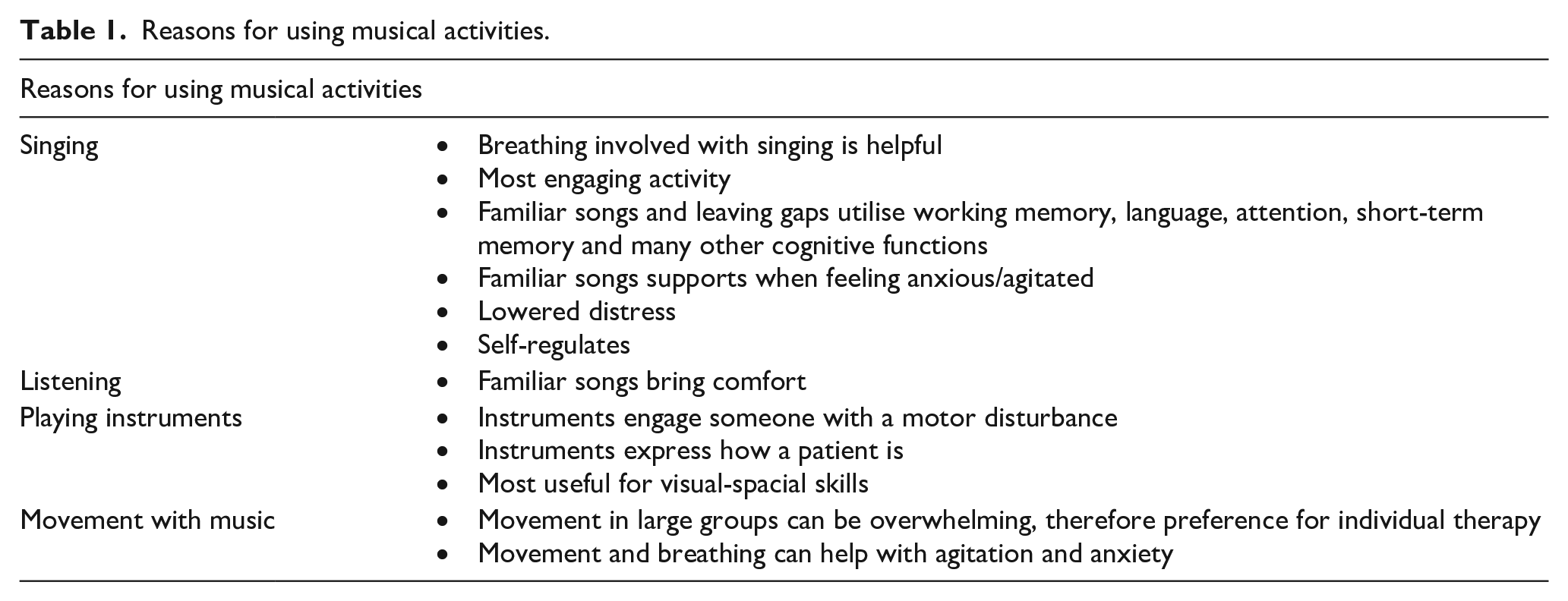
For this section of the survey, free-text responses were available in addition to the multiple-choice questions. Participants were encouraged to share any reasoning as to why a certain musical activity would be used with the aim of improving a cognitive domain or reducing a neuropsychiatric symptom for a patient living with dementia. In total, 27 of the 31 participants chose to complete the free-text responses as shown in Table 1.
Reasons for using musical activities.
Results – external factors
To explore additional reasons for certain musical activities being used over others, questions were asked about how the music therapist collaborates with other professionals or loved ones and how the COVID-19 infection prevention measures or online working may have also influenced their choice of musical activities.
First, participants were asked who they collaborate with and whether this collaboration occurs during music therapy sessions or outside of music therapy sessions. Participants were able to select more than one option. Formal caregivers were collaborated with the most (28 participants) followed by other allied healthcare professionals (20 participants), additional music therapists (19 participants) and informal caregivers, family or friends supporting the care of a loved one living with dementia (16 participants). The least common was collaboration with family, friends or other collaborators. For the nine participants who selected ‘other’, four commented to clarify who these collaborators were including:
‘Nursing staff, Doctors, Consultant Psychiatrists’
‘All staff on ward, nurses, junior doctors, consultants’
‘All other staff on the ward’
‘Activities coordinator’
It was also noted that all 31 participants collaborate with someone during and/or outside of music therapy sessions themselves (Figure 9).
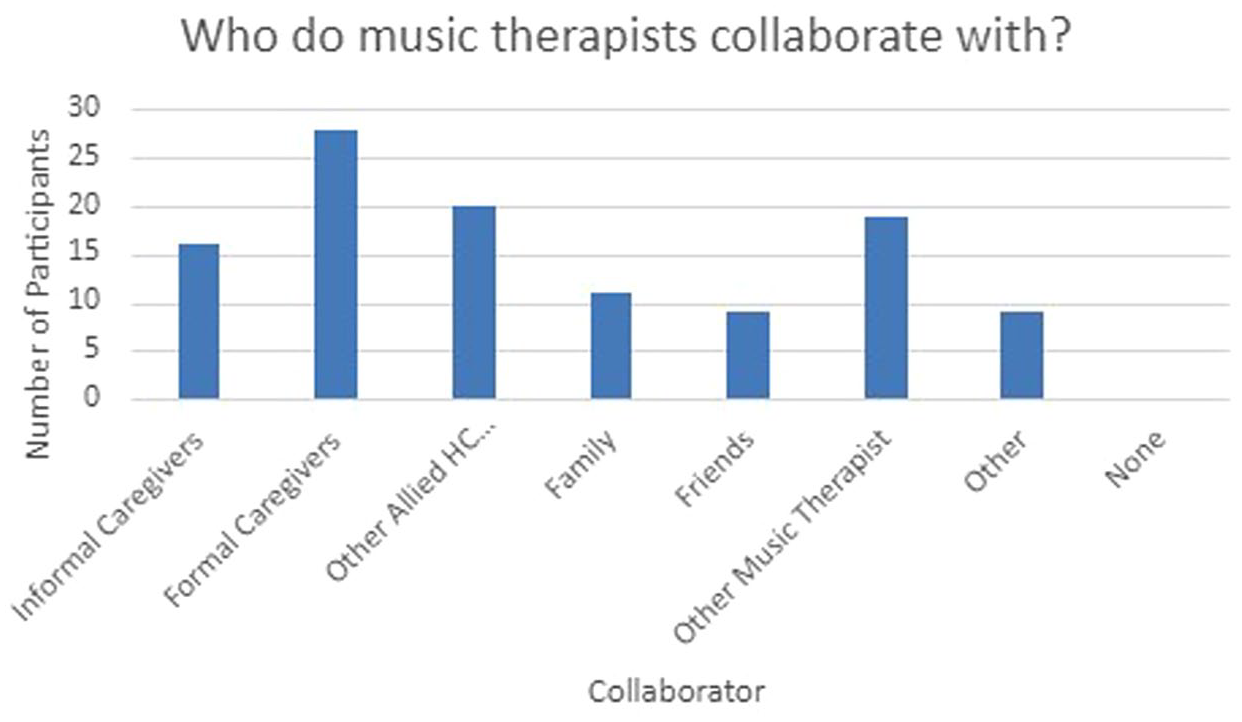
Collaborators with music therapists.
Participants next shared whether the collaboration occurs during music therapy sessions or outside of music therapy sessions which resulted in an almost equal number with 28 and 29 participants selecting during and outside of music therapy sessions, respectively. Two of the 31 participants also selected ‘other’ both of whom commented to clarify their selection.
‘Sometimes offer support/feedback to family members who have not come into the hospital but can share collateral information or feedback on ideas that may aid caregiving at home’
‘In team meetings while discussing care for residents’
Out of the 31 participants, 27 participants said that collaboration with other professionals influences their choice of musical activities used within music therapy sessions with 4 participants saying that their collaborators do not change their use of music. The free-text component of this question addressed how collaboration influences the choice of musical activities and raised four main themes. These responses in Table 2 show the importance of collaborative work to understand the client and maintain a person-centred approach.
Influences from collaborators on choice of musical activities.

The final component of the survey asked about the COVID-19 infection prevention measures and whether this had an influence on their choice of musical activity. Overall, 30 participants shared that during the lockdowns, they had collaborated in-person and 17 shared that they had also collaborated online. The following question then identified whether working in-person compared to online had influenced their choice of musical activity or not. Given the larger number of responses to this question, it is assumed that either participants responded based on assumption or that more participants worked online than collaborated online. Overall, 22 participants shared that working online influences their use of musical activities compared to three participants who said no and eight who said the question was not applicable to them.
The free-text component of this question received 27 out of 31 responses to share how working online influenced their use of musical activities. The responses were categorised into four main themes.
Fewer instruments and more listening (13 participants)
Less spontaneity and more structure (7 participants)
Technical challenges (7 participants) Delay Access to technology Muting Sound quality
Lack of understanding from the person living with dementia (2 participants)
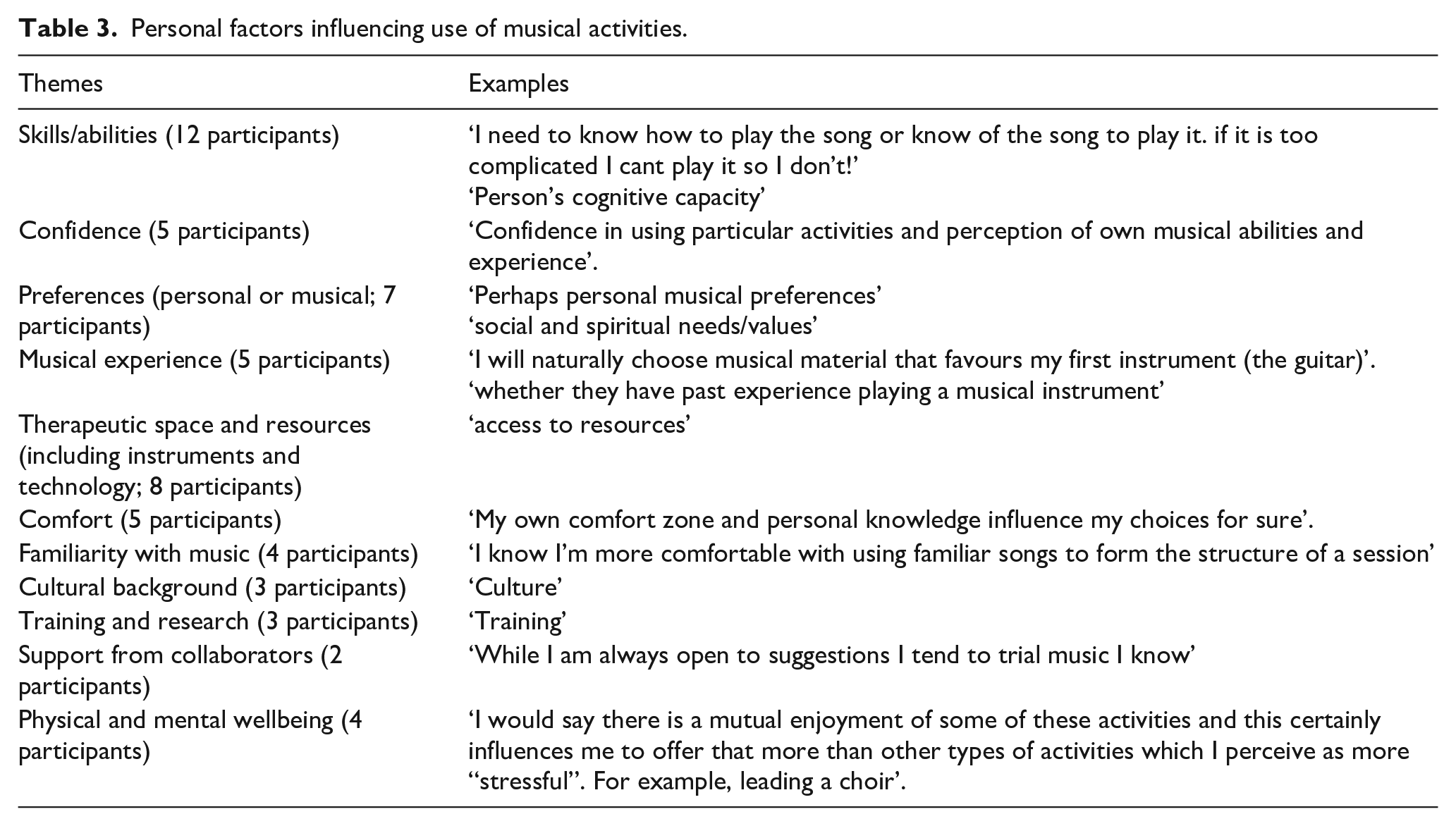
The final question in the survey was designed to capture any additional information that had not been considered or raised throughout the survey on personal factors which may influence the music therapists’ use of musical activities during a music therapy session. The question specifically asked for one-word responses which were categorised into 11 different themes presented in Table 3.
Personal factors influencing use of musical activities.
Further results – impact of experience
Participants were placed into two categories based on the number of years as a music therapist. To maintain a roughly even number of participants in each category, the split was made between participants who had been qualified for up to 3 years and those who had been qualified for 4 or more years. The first category ranging from newly qualified to being qualified for 3 years included 14 participants and the second category ranging from being qualified for at least 4 years included 17 participants.
Overall, both music therapists with less than 3 years of experience and music therapists with more than 4 years of experience had similar uses of singing, listening, playing instruments and movement with music. There is a slight tendency for more experienced music therapists to use singing more frequently than other musical activities with 71% of those qualified for up to 3 years sharing singing is their most frequently used activity compared to 88% of those qualified for more than 3 years. The graphs also show that for those qualified for up to 3 years, there may be more varied use of musical activities. The small sample size, however, does not make this statistically significant.
The two graphs in Figures 10 and 11 show that music therapists still use singing more than other musical activities during music therapy sessions whether they are newly qualified or experienced music therapists. Among newly qualified music therapists, listening to music was the second most frequently used activity followed by playing instruments and movement. More experienced music therapists use movement more than newly qualified music therapists which was equalled by listening to music and followed by playing instruments.
Use of musical activities for music therapists qualified for up to 3 years.
Use of musical activities for music therapists qualified for 4 years or more.
Discussion
Reflections
Results showed that most participants, all of whom were qualified music therapists, had experience working with people living with dementia for between 1 and 6 years. It was also shown that most of these therapists worked at care homes, mostly residential but also nursing homes. According to the Alzheimer’s Society (2019), two thirds of people living with dementia live in the community. People living with earlier stages of dementia are less likely to have challenging symptoms and be able to live at home. The survey results suggest that music therapists are not working in all settings that reflect the wide range of people living with dementia in the United Kingdom. Also, the results suggest that music therapy is prioritised for those with more advanced dementia, who are therefore likely to have more challenging needs and symptoms. It is also interesting to note that the data show some participants had experience working as a music therapist with people living with dementia for longer than they had been qualified as a music therapist. This may be because placement experience was included in their response, or perhaps that some music therapists worked as carers for people with dementia prior to training.
Overall, results show that singing is the most frequently used activity followed by playing instruments, listening and movement with music. Music therapists in the United Kingdom choose these activities based on practical, personal, clinical and external reasons.
Exploring the musical activities therapists used to maintain or improve a certain cognitive domain identified the following results as summarised in Figure 12.
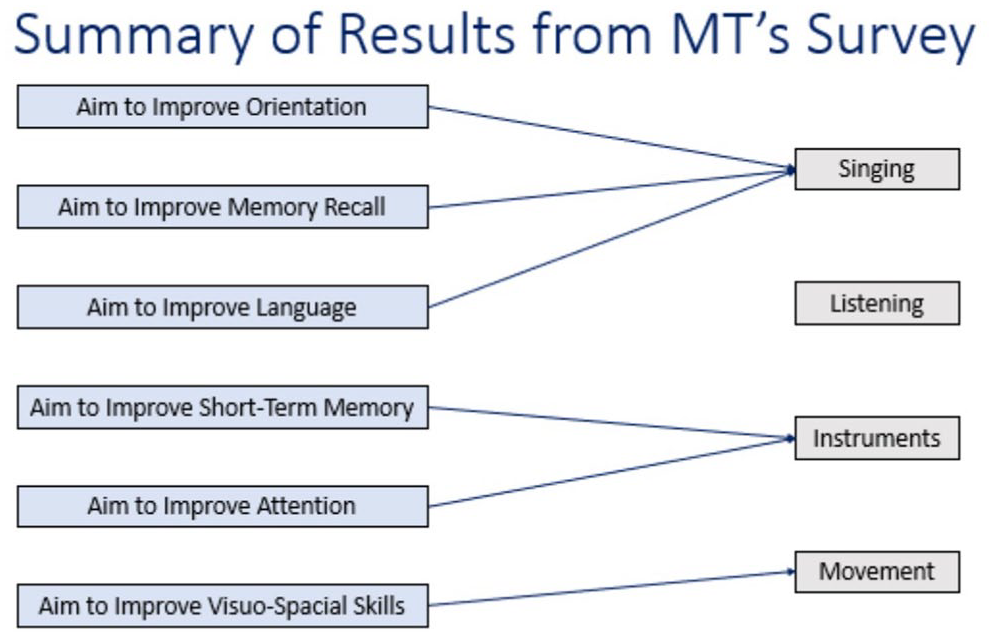
Summary of results from MT’s survey (1).
The summary in Figure 13 similarly identifies the musical activities used by music therapists with the aim of reducing a certain neuropsychiatric symptom.
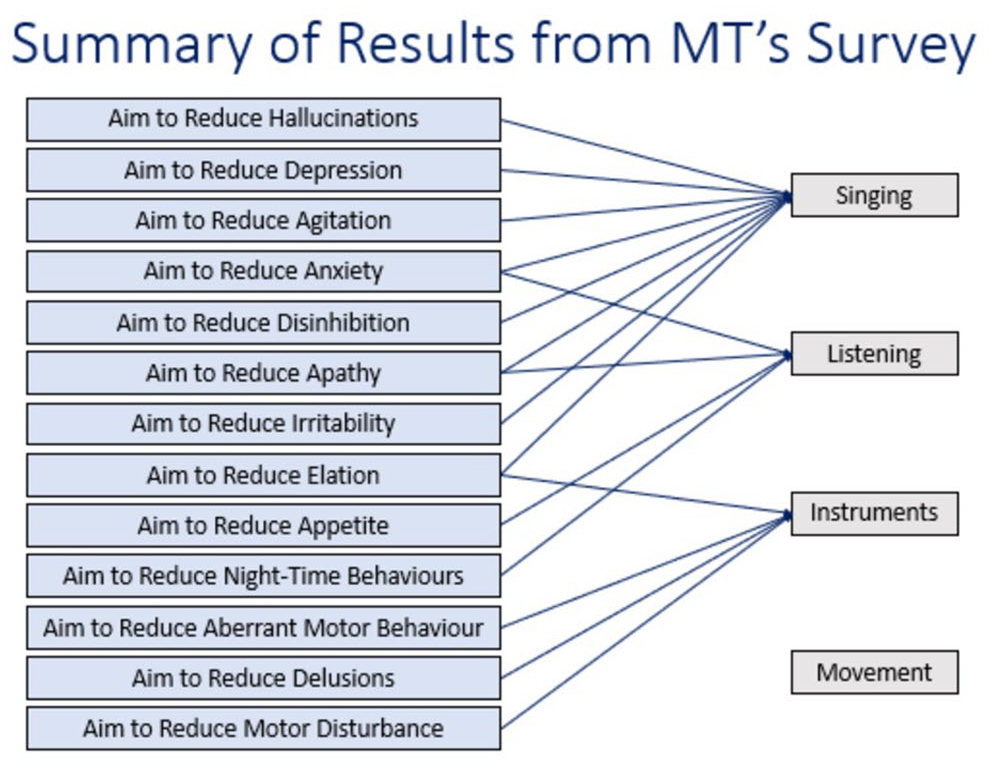
Summary of results from MT’s survey (2).
Consistent with the music therapists’ use of different music activities, singing is the most used for both improving cognitive domains and reducing neuropsychiatric symptoms. The use of musical activities, however, differs where listening was never the most used activity to improve cognitive domains and movement was never the most used activity to reduce neuropsychiatric symptoms.
Although few music therapy studies separate the impact of various musical activities, these results are in line with other more recent music therapy research which suggests that music therapy can reduce agitation for people living with dementia on in-patient psychiatric wards (Thompson et al., 2023). In Europe and more globally, systematic reviews show studies resulting in reduced agitation (Sousa et al., 2020), and contrary to this, also show no clear reduction of agitation but show a reduction in anxiety, depression and apathy (Lam et al., 2020).
The use of singing has been common for much of human history and is seen in natural intuitive interactions between the mother and infant. Daniel Stern identifies that a form of vocal communication is seen within 3- to 4-month old infants and their mothers in his study and suggests that the vocalisations are a component to ‘establishing group membership or bonding’ (Stern et al., 1975). In more recent research, the term ‘communicative musicality’ is used to describe the vocalisations between mother and child where these exchanges are found to have measurable characteristics (Malloch, 1999; Trevarthen, 2011). This parent and baby intersubjective attunement can be transferred to the therapeutic setting, particularly through improvised vocal exchanges or singing familiar songs together. It can therefore be understood that through music therapy in later life, singing may be the ideal method for building a connection between the two people singing whether between therapist and person living with dementia or between two family members.
In current research, we can see that singing involves instinctive human behaviours which can also provide stimulation for the brain (Lyu et al., 2018). Non-verbal musical communication through forms other than singing can also be particularly important once the ability to communicate through language is reduced in later stages of dementia (Ho et al., 2019). Listening, in particular, has been seen to reduce neuropsychiatric symptoms such as anxiety because it brings back familiar childhood memories (Weise et al., 2019). In more active musical interventions, research shows that a music and movement intervention can improve memory and reduce depression for people living with mid-stage dementia (Cheung et al., 2018).
Results from the survey show the influence of external factors of music therapy such as other collaborators and, during the COVID-19 infection prevention measures, the difference between online and in-person working. Within the field of dementia, working with family members and staff is seen frequently and almost all participants had collaborated with others whether directly within therapy sessions or through external communication. Future research and clinical work should intentionally consider how to involve these collaborators in music therapy. Working more collaboratively has shown to provide additional benefits for the person living with dementia as well as the network that supports them (Hsu et al., 2015; Melhuish et al., 2019). Changing the approach to delivering music therapy sessions could show huge improvements in quality of care.
In the additional analysis of the survey results, exploring the difference between the use of musical activities between more and less experienced music therapists, it was observed that more experienced music therapists use singing more than newly qualified music therapists. This may be something for music therapists to consider through training and throughout a career when reflecting on clinical work. Continuing to gain experience and practise in a variety of musical activities could also be important as part of continuous professional development.
Limitations of the study
There are several limitations to this study involving the study design and the participants. The survey contained a large amount of freedom in how to respond, such as the ability to select more than one answer or choose not to respond. Although it was designed this way to collect accurate data on how music therapists use music, as it was known that multiple musical activities may be used, this may have also created the opportunity for participants to select responses without a critical thought process to determine the most frequently used activity. This reflects a common challenge in music therapy research in which a diverse range of musical activities are used throughout a therapy process and even during one music therapy session making it difficult to unpick the benefits of each activity. Another limitation of the survey design is the open nature of the free-text responses. Participants may have been able to provide a more concise response if there was more direction or clarity on the type of information requested. Likewise, encouraging longer free-text responses to capture a deeper understanding could have been beneficial, particularly in the final question in which one-word responses were asked for. However, this was designed to reflect the flexible nature of the work of music therapists, which is not a ‘one size fits all’ form of therapy. In particular, the question on in-person compared to online working could be further clarified to determine the difference between job role and collaborations.
In order to understand more about the people who took part in the survey, questions could have been asked about the background of the music therapist participating, to collect data on information such as their main instruments, where they trained and other work experience. Such information would be helpful to identify the influence of experience with a certain instrument, upon decisions within a therapy session. It would also potentially identify various approaches to music therapy taught in different universities, leading to improved training and knowledge about these programmes across the United Kingdom.
Another limitation of this study is the number of participants. Within the framework of the PhD, aiming to recruit 30 participants in the United Kingdom only was most reasonable. A much larger sample size would provide a smaller margin of error and more accuracy on the overall use of musical activities for people living with dementia in the United Kingdom. It could also be beneficial to recruit participants on a global scale, to identify a broader use of musical activities for people with dementia considering diverse cultures and training. This survey would then need to include additional questions such as what country the participant is from and what is involved in the training to become a music therapist as it is not a regulated profession globally.
Future implications
These data alone cannot show whether a particular musical activity is best suited to achieving certain aims for participants. However, it does provide some insight into why different activities might be used, which fills a recognised gap in music therapy research. These data can be the basis for further exploration into what happens within music therapy sessions for people living with dementia.
This survey identifies various areas for further research. Most importantly, this includes the need to connect the reasoning for music therapists using certain musical activities with scientific theory. Study designs can include mechanisms for choosing a certain domain or symptom to compare the impact of several different music activities. An example of a future study aim could be to improve the language domain in a person living with dementia, where singing is the main musical intervention. A specific song list would be created along with a description of other activities such as discussion around the song and lyrics or leaving out a word of a song for the person with dementia to fill in. The use of singing could be compared to listening to music, using instruments and movement with music. This method would include a clear and detailed intervention as recommended in the literature (Van der Steen et al., 2018). In addition, other areas could be considered such as whether the use of music differs for patients with earlier stages of dementia compared to later.
This survey also identifies areas for future training for music therapists working with people living with dementia. This could include improving guidance for music therapy trainees about how to choose appropriate musical activities in their sessions. Given that the data show clinical decisions are not the only factors at play when determining musical activities in a therapy session, it is also important for trainees to think outside of purely clinical factors. Music therapists should consider their personal preferences and experiences, as well as those of the people living with dementia and their families and carers. Also, their external environment and other people they collaborate with should be a focus for music therapy trainees in whatever context they are working within.
In addition to music therapists, there are other arts and/or care professionals who use music with people living with dementia, especially in care homes. These professionals are often able to engage people living with dementia at earlier stages of dementia but are less likely to work with those in later stages. Further guidance for these staff members could help increase engagement for residents in later stages of dementia towards end of life. An example of this is a study currently in progress called MELODIC (National Institute for Health and Care Research, n.d.). This study is developing a manualised music therapy treatment for staff to deliver in hospital in-patient dementia wards. Another form of collaboration could include supporting music therapists to share information about the therapy sessions. This can encourage care professionals to be more independent in using music throughout the week between music therapy sessions, for example in care homes. Another current study, Music4theMind (Anchor, 2022), is delivering music therapy session two times per week for someone living with dementia. During this intervention, video communication with staff is used to support staff to use music to manage symptoms through their regular care. Music4theMind has been based on a previous study (Hsu et al., 2015) showing positive effects of video communication with staff. Providing support through continuing good communication with other care professionals can encourage the use of daily music, as well as help manage symptoms for people living with dementia.
Conclusion
This work is important in deepening understanding of the specific musical activities music therapists use within sessions for people living with dementia. The previous lack of clarity on what exactly happens in music therapy sessions in the literature has been highlighted as an area requiring further research. This study also raises awareness of the connections between the musical activities used and the aims of the therapy, along with the importance of connections to personal knowledge, backgrounds, skills and experiences of the therapists themselves.
Footnotes
Acknowledgements
This study was completed in partial fulfilment of the PhD at Anglia Ruskin University, UK. The authors would like to thank anonymous participants who contributed to the survey data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SC and the research conducted were funded by a PhD Vice Chancellor Studentship through Anglia Ruskin University. MHH, JP and HOM were supported by Alzheimer’s Society, UK (grant no. 462) as part of the Joint Programme for Neurodegenerative Diseases consortia scheme for the HOMESIDE Study.
Ethics approval
Ethics approval for this survey was provided through the Arts, Humanities and Social Sciences Faculty Research Ethics Panel at Anglia Ruskin University, UK. All music therapists who took part were eligible to participate and consented to completing the survey.