
Abstract
Specific tools to measure the cognitive benefits of music therapy and music-rehabilitation training available to music therapists are few and empirically weak: they are mostly psychometrically unrefined or based on unclear tasks and scoring protocols; they do not take into consideration distinct cognitive functions or are based on exclusively observational protocols. To overcome these limitations, we developed a 15-min cognitive screening tool suitable for music therapists, Music Cognitive Test (MCT), which assesses cognitive abilities stimulated by music-making activities (e.g., attentional, verbal, and executive functions, short- and long-term memory) by including music-based items. MCT was validated with 335 participants (aged 18–100 years old) presenting a range of cognitive levels, from healthy cognition to severe impairment. MCT correlated strongly and positively with well-known tests: Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), and Severe Mini-Mental State Examination (SMMSE). MCT also displayed excellent sensitivity in identifying impaired individuals according to both MMSE and MoCA diagnostic criteria (99.4% and 93.0%, respectively), and excellent specificity in identifying healthy participants based on MMSE (93.5%) and MoCA (97.8%) criteria. Overall, results highlight the reliability of this novel brief music-focused cognitive screening test, to enable music therapists to independently and consistently monitor the effectiveness of their intervention on cognitive functions.
Music therapy (MT, see World Federation of Music Therapy, 2011 for definition) and music interventions have increasingly been used both as rehabilitation treatments to support individuals with cognitive and neuropsychiatric decline (i.e., Biasutti & Mangiacotti, 2018, 2021; Hsu et al., 2015; Sung et al., 2012) and as methods to enhance protective effects on the aging brain (Rogenmoser et al., 2018). Research has shown that the cognitive domains related to music perception and processing are less affected by cognitive decline than other functions (Baird & Samson, 2009; Cuddy & Duffin, 2005), and can be usefully recruited for therapeutic interventions.
Although music is acknowledged to be effective in several therapeutic situations (Hohmann et al., 2017; Umbrello et al., 2019), the research varies in quality, and results are not always uniform due to the use of different methods of assessment. In this study, we introduce a novel music-based test—the Music Cognitive Test (MCT)—to screen cognitive functions stimulated by music that may be used as a reliable assessment method both in clinical and research contexts.
Cognitive assessments normally used in neuro-rehabilitation contexts (e.g., Montreal Cognitive Assessment (MoCA); Nasreddine et al., 2005) to screen a range of cognitive functions (e.g., orientation, attention) are not tailored to evaluate music-training and therapy cognitive benefits. Some present limitations to detect subtle impairments at very early stages of cognitive decline (e.g., Mini-Mental State Examination (MMSE), Devenney & Hodges, 2016) or have floor effects (e.g., MoCA, Skorvanek et al., 2018) making them “too difficult” for individuals with more severe stages of decline (Harrell et al., 2000), limiting their usefulness. Furthermore, these tests require specialized training for administration and interpretation (Hobson & Meara, 1999) and in some countries can only be administered by registered specialists.
Most MT academic training programs are based on a psychotherapeutic approach with limited focus on neuropsychological insights and tools (Mangiacotti et al., 2021; Thaut, 2015). Music therapists traditionally use qualitative forms of assessment during patient evaluation, which constrains identification of cognitive impairment and suitability of the therapy (Lipe et al., 2007). Rigorous assessment is essential for diagnosis and development of treatment plans (Davis et al., 2008), and in clinical practice music therapists are frequently asked to provide the reliability and validity of their tools (Sabbatella, 2004). Although diagnosis is not part of the music therapist’s role, a patient’s assessment is crucial in designing MT treatments because it establishes baseline cognitive functioning and allows the development of suitable therapeutic goals and evaluation of intervention efficacy (Wilson, 2000). Moreover, assessment can also be part of an evaluation of MT interventions hence supporting music therapists’ professional identity and their relationships with the larger professional community (Isenberg-Grzeda, 1988).
There is a growing need for MT assessment tools to assist music therapists in their everyday practice and contribute to the overall clinical assessment of patients (Norman, 2012; Spiro et al., 2017). Although MT and music intervention assessments should be specific to populations, work settings, and therapeutic approaches (Kim, 2005), music therapists must design assessments compatible with the requirements of the institution delivering care (Schlenghe & Murphy, 2000) and commensurate with their task. Assessing patients “under musical conditions not only adds to the holistic view of the patient’s functioning, but it also suggests the effectiveness of integrating MT interventions into the resident’s treatment plan” (Norman, 2012, p. 9).
In general, MT assessments were developed for children/adults with psychiatric disorders (Cassity & Cassity, 2006) or special needs (Coleman & Brunk, 1999; Douglass, 2006; Kim, 2005; Layman et al., 2002), patients with neurocognitive disorder (Glynn, 1992; Lipe et al., 2007; McDermott et al., 2015; Mitsudome, 2013; Munk-Madsen, 2001; York, 1994, 2000) terminally ill in hospice care (Groen, 2007), traumatic brain injury (Jeong, 2013; Jeong & Lesiuk, 2011; Pfeiffer et al., 2021) and unspecified or mixed populations (Bruscia, 1987; Loewy, 2000; see also Sabbatella, 2004; Spiro et al., 2017). Relatively scant research has been conducted on geriatric populations (see Adler, 2001; Norman, 2012), especially in relation to validated MT measures for individuals with neurocognitive disorders (McDermott et al., 2013). The main tools are the Residual Music Skills Test (RMST) developed by York (1994, 2000) and the Music-based Evaluation of Cognitive Functioning (MBECF) developed by Lipe (1995; Lipe et al., 2007)
The RMST (York, 1994, 2000) detects strengths in musical behavior of individuals diagnosed with possible Alzheimer’s Disease. Using a music player and simple musical instruments such as maracas and drums, the RMST comprises 11 items assessing auditory discrimination, singing, rhythmic abilities, arousal discrimination, tonal memory/pitch discrimination, musical language, and recall abilities.
The MBECF (Lipe, 1995; Lipe et al., 2007) consists of 18 items evaluating verbal, singing, melodic, and rhythmic responses, with the addition of verbal questions about the individuals’ musical background. Lipe et al. (2007) examined the content validity of RMST and MBECF, founding significant correlations with the MMSE (Folstein et al., 1983), which is among the most used neuropsychological screening test to measure cognitive impairment in geriatric populations. The study highlighted the unique relationship between elements of musical cognition and singing, melodic or rhythmic aspects. However, the tasks used in RMST and MBECF are based on expressive music behaviors, and do not assess specific cognitive functions, such as subtypes of attention and executive function (e.g., inhibitory control), engaged by those musical behaviors. Furthermore, RMST and MBECF rely heavily on culture-specific aspects: such as recognizing songs that are well-known within a specific cultural context (e.g., Western), limiting their generalizability. This is problematic given the increasing migration flow to Europe (King, 2019) and across continents, and in the United Kingdom the presence of older adults from ethnic minorities is rising (Badger et al., 2009). Therefore, the RMST and MBECF may not be suitable to assess the clinical effectiveness of MT interventions in wider cultural contexts (McDermott et al., 2015). Despite these limitations, it is encouraging that it is possible to quantify music task performance in a clinically meaningful way (Saad, 2017).
Two further tools have been developed for the geriatric population: (a) the Mitsudome’s Music Therapy Assessment Tool for People with Dementia (Mitsudome, 2013), specifically targeting individuals with neurocognitive disorder. Music Therapy Assessment Tool for People with Dementia assesses musical functioning by measuring cognitive skills, behavior, emotional reactions, and social/communication skills through music therapists’ observations. It is intended for initial assessments as well as ongoing evaluation of therapy sessions, and it has been criticized as not being psychometrically validated, including unrefined items and unclear scoring (Saad, 2017); (b) Specifically developed for geriatric patients in long-term care and rehabilitation facilities, the Geriatric Music Therapy Clinical Assessment (Hintz, 2000) measures a patient’s skills, such as musical-expressiveness, musical-receptiveness, psychosocial/behavior, motor ability, and cognitive/memory skills through musical tasks. Concerning the latter, this test primarily assesses recall memory abilities, fine and gross motor movement, and attentional functions (with no differentiation between types). The author suggests administering the test across the testing day in multiple sessions to enhance reliability. However, administration instructions are unstructured and the score is based on the therapists’ personal judgments, introducing the risk of bias. Another limitation is its lengthy administration, which might prevent some music therapists from using it effectively, particularly if they work at any given facility only intermittently. Typically, music therapists working in care-homes are employed for a few hours per week, to fit in as many patients as possible, limiting the opportunity for in-depth assessment procedures. In sum, the MT assessment tools available do not specifically and reliably tap into the evaluation of the cognitive functions engaged by musical behaviors, and do not offer the type of tool suitable for music therapists.
Several studies have supported the effectiveness of music-based interventions specifically in cognitive rehabilitation, but to measure global cognitive improvement they used general psychological tests (e.g., MMSE, MoCA). Such measures do not consider the exact cognitive functions stimulated by different musical interventions, which could be of interest for music therapists to enhance their practice. For instance, aspects of memory stimulated in MT sessions, such as in rhythmic and melodic recognition, musical memory, autobiographical music memory, may also transfer to everyday life activities, hence increasing well-being (Cunningham et al., 2019; Haslam et al., 2014), social skills, and self-esteem (Lippin & Micozzi, 2006; Wall & Duffy, 2010) (see Supplementary Materials online for further details). Overall, there are several limitations surrounding existing MT assessments for individuals with neurocognitive disorders: they are based on small samples (Hintz, 2000; McDermott et al., 2015; Mitsudome, 2013; York, 2000), lack appropriate validation, employ observational ratings, and/or have not been used widely in practice or research (Lipe, 2015; Spiro et al., 2017). On the contrary, MT assessment tools that map cognitive functions are focused on very specific parameters: music preferences (McPherson & Thompson, 1998; Rentfrow & Gosling, 2013), functional singing range in older adults (Greenwald & Salzberg, 1979), and awareness in disorders of consciousness (Magee et al., 2014). This type of test usually considers the ability level in music performance (Aldridge, 1993; Hintz, 2000; Lipe & York, 2007; York, 1994), and from this it infers a global measure of cognitive function, without an appropriate evaluation of specific cognitive components, such as memory or executive functions, or a patient’s state of mind. In many cases, the tests simply focus on observational outcomes, which may be affected by therapists’ personal evaluations (McDermott et al., 2013).
There is a clear lack of quantitative tools for evaluating and screening cognitive functions stimulated by music-based rehabilitation programs for older adults (Vink et al., 2013), and the importance of standardized assessments contributing to active music-based rehabilitation is acknowledged (Jeong, 2013; Spiro et al., 2017). More specifically, assessments designed for music therapists “may offer opportunities for increased self-disclosure, for nonverbal and symbolic communication, and may allow patients to be observed in process” (Lipe, 2015, pp. 76–77). Such assessment tools would also help music therapists acquire specific cognitive information about patients because they do not always have the opportunity to access patient’s medical data (Mangiacotti et al., 2021).
With a view to addressing the aforementioned issues and building upon previous research on MT, cognitive neuropsychology, neuro-rehabilitation, music psychology, and neuroscience, this article presents the development and validation of a novel music-based screening cognitive test (MCT), a standardized tool aiming to provide the following crucial benefits: (a) help music therapists to easily and quickly screen/monitor general cognitive functioning during music-based rehabilitation activities, supporting them in adjusting their therapy, especially for patients at early stages of cognitive decline, and independently monitor and evaluate the effectiveness of their activities along the intervention (Davis et al., 2008); (b) by targeting specific cognitive functions, establish a common ground that music therapists working with the aging population can use to communicate efficiently among themselves and, critically, with other healthcare professionals (Saad, 2017); (c) facilitate therapists in consistently highlighting music-based therapy benefits to patient’s families and other staff members for those living in sheltered accommodation or care-homes, particularly useful when a patient moves to another environment or therapist.
Method
For this study ethical approval was granted by Padua University Psychology Research Ethics Committee and by Middlesex University Psychology Research Ethics Committee.
MCT development
MCT items were designed to investigate specific cognitive functions known to be stimulated by musical activities and that are aligned with the main areas evaluated by existing tests used in the assessment of cognitive decline associated with aging, such as the MMSE (Folstein et al., 1983), the Severe Mini-Mental State Examination (SMMSE; Harrell et al., 2000), the Montreal Cognitive Assessment (MoCA), the Severe Impairment Battery (Panisset et al., 1994), and the Frontal Assessment Battery (Dubois et al., 2000). However, in contrast to existing cognitive tests, most items in the MCT are based on musical tasks, which specifically target cognitive functions of interest so that connections between test items and targeted cognitive functions are clear for music therapists intending to use it in their practice.
MCT is a non-invasive paper and pencil test consisting of two parts: Part 1—test items (16 questions), comprising tasks relating to cognitive functions stimulated during music activities (see below), some performed using a xylophone (an affordable and widely used instrument within the MT community); Part 2—observation items (three questions), assessing attentional, verbal, and comprehension skills. The overall MCT score ranges from 0 to 52 (a total of 43 points for Part 1 and 9 points for Part 2) and the overall administration time is approximately 15 min.
For developing the MCT items, a list of common cognitive functions stimulated by MT interventions and music-training activities was derived from the literature (illustrated with the relevant MCT items reported in the Supplementary Materials online) such as: space–time and name orientation, praxis and visual-perceptual reasoning, attention, rhythmic and melodic recognition, musical memory, planning and verbal comprehension/production skills, sound localization, visual research, naming and analytical reasoning abilities.
Subsequently, two researchers identified and developed a series of tasks which were then discussed with the rest of the team to create a beta-MCT version (based on 14 items). The MCT was designed to measure cognitive function stimulated by MT, but for some items where it was difficult to include a music-related technique a direct measure of function is used (e.g., space–time orientation).
Content validity
To measure content validity an expert evaluation of the beta-MCT version was first performed. Seven experts, including music-psychology (n = 2), aging-psychology (n = 2), neurocognitive evaluation and rehabilitation (n = 1), and MT (n = 2) with at least 8 years of experience in their fields were asked to review the test and provide feedback. Reviewers completed a form composed of 75 Likert questions and six open questions. The questionnaire was developed to assess different domains of each MCT exercise on a 1 to 5 Likert agreement scale, which was evaluated as to whether: (a) it was measuring specific cognitive functions, (b) it presented understandable instructions for the examiner, (c) it presented understandable instructions for the participant, (d) the scoring was appropriate, and (e) it allowed discrimination of different cognitive levels. Furthermore, three overall-judgment Likert questions were asked evaluating: (a) the overall MCT efficacy in assessing cognitive efficiency, (b) overall MCT time administration suitability, and (c) the usefulness of MCT for MT and music-based intervention. The open questions investigated possible further improvement of the test.
For the interpretation of the results, a threshold of 3.5/5 (70% of the rating scale score) was chosen as a measure of task appreciation (Mangiacotti et al., 2021). Experts’ ratings on each question were grouped by exercise (Table 1) and the results of the three beta-MCT overall-judgment Likert questions are reported in Table 2. The reviewers agreed that MCT tasks met all above-mentioned objectives (a)–(c). Replies to the open questions suggested changes in the following aspects: (a) items order sequence and classification, (b) division of the attentional subtasks into independent tasks, (c) developing an item for semantic memory, (d) details of instructions, and (e) adjustment on item scores. Subsequently, from the feedback received, a final version of the test (19 items) was developed (MCT full version can be found at https://www.mctest.eu/).
Mean (M) and Standard Deviation (SD) of Expert Replies (n = 7) for Each Beta-MCT Exercise.
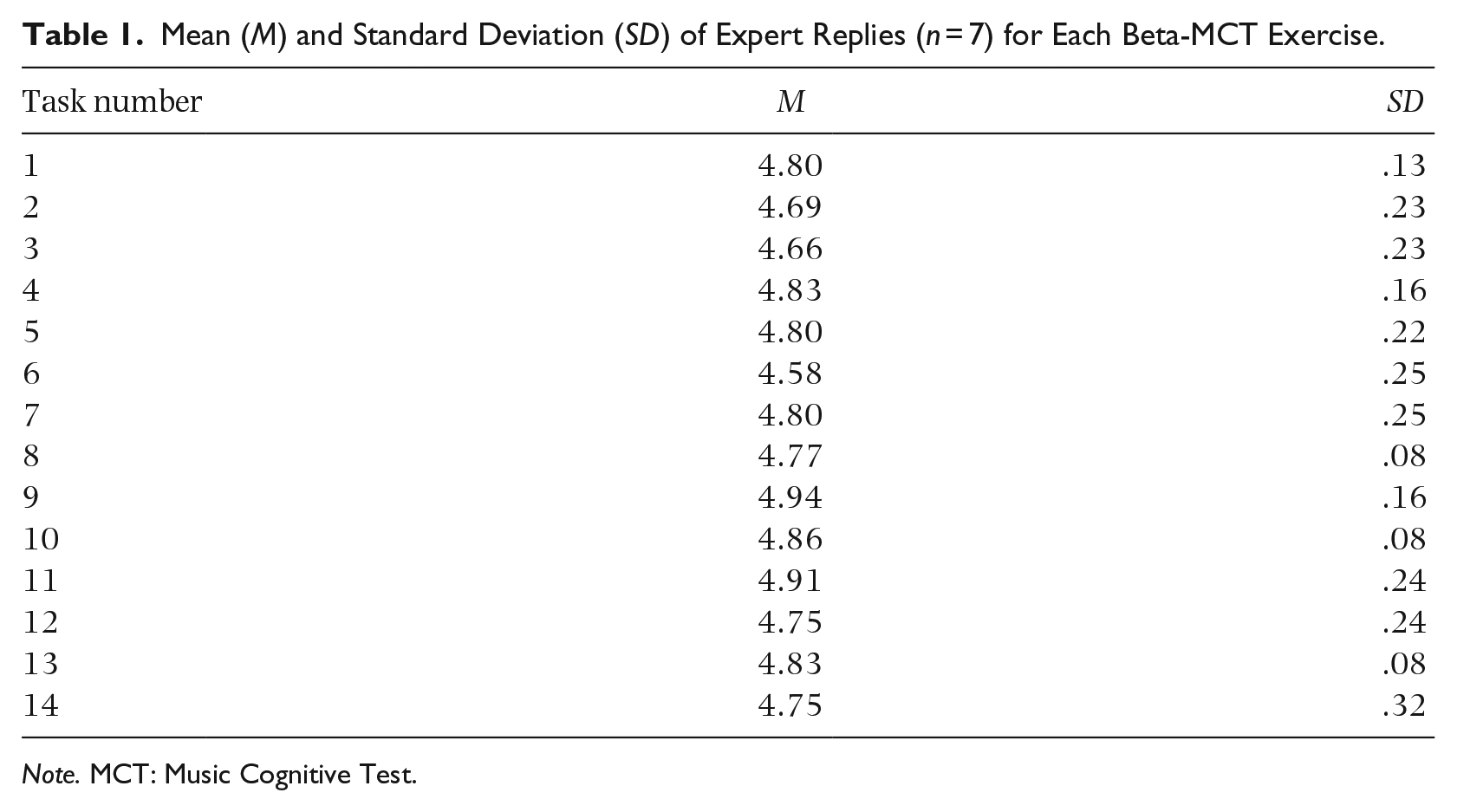
Note. MCT: Music Cognitive Test.
Mean (M) and Standard Deviation (SD) of Expert Replies (n = 7) on the Three Overall MCT Evaluation Questions.
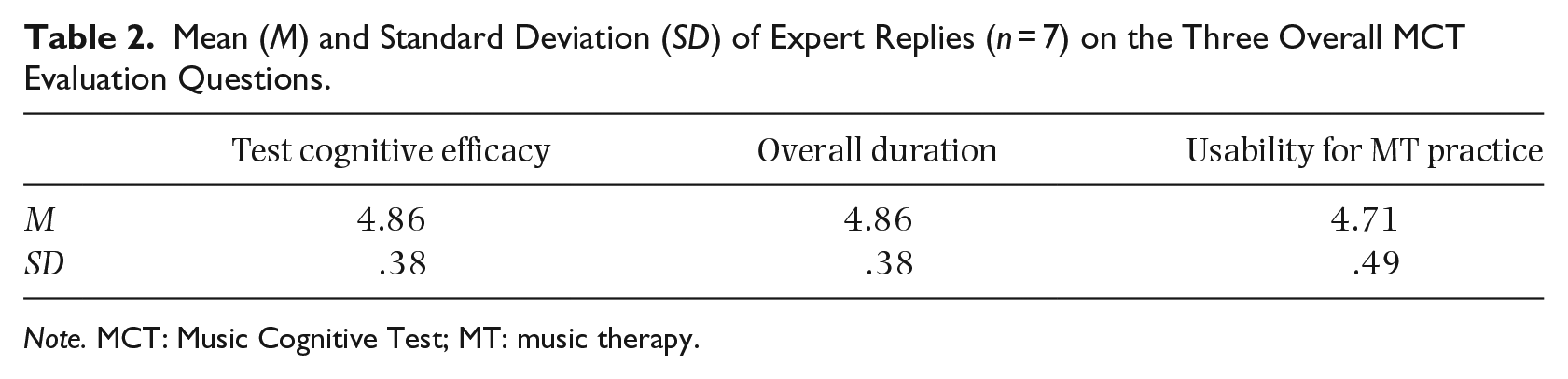
Note. MCT: Music Cognitive Test; MT: music therapy.
Participants
For the large-scale validation of MCT, 335 participants were recruited from Italy and the United Kingdom. The recruitment of the British sample was carried out in collaboration with Middlesex University London, Methodist Homes Association, the University of the Third Age and via snowballing. The recruitment of the Italian sample was carried out in collaboration with Padua University and Centro Anziani D. Sartor. Informed consent was obtained from all participants, and in the case of cognitive impairment, consent was also obtained through their guardian. Inclusion criteria were: (a) age ⩾ 18 years and (b) fluent linguistic proficiency in the English or Italian language; exclusion criteria: (a) presence of severe motor and sensorial (e.g., hearing) deficits that would not allow participants to attend administration and (b) having taken part in a cognitive assessment within the last 3 months. Participant demographic and cognitive screening data for the entire sample are presented in Table 3.
Participants’ Demographic Data of the Total Sample and Divided by Country (Italian and UK).
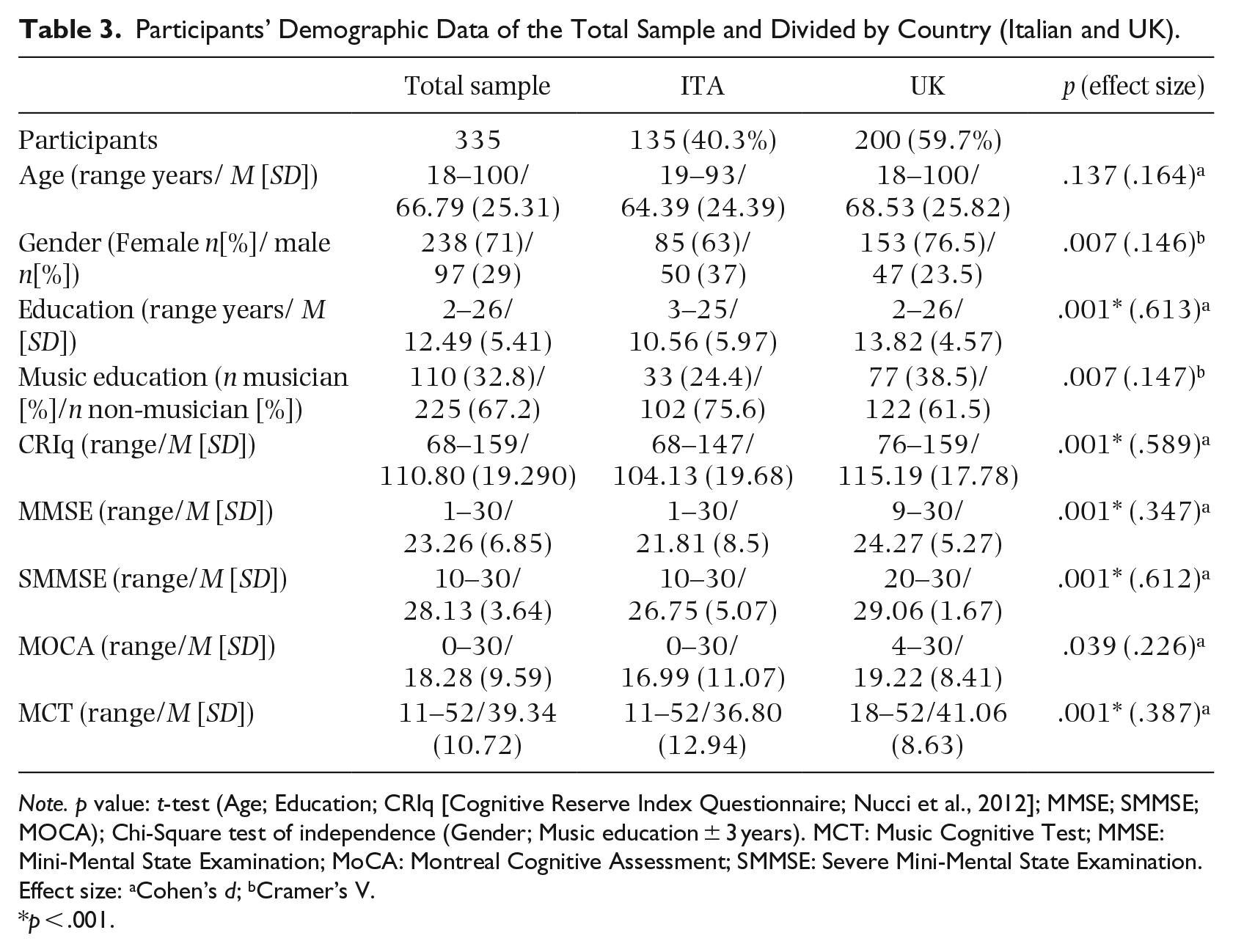
Note. p value: t-test (Age; Education; CRIq [Cognitive Reserve Index Questionnaire; Nucci et al., 2012]; MMSE; SMMSE; MOCA); Chi-Square test of independence (Gender; Music education ± 3 years). MCT: Music Cognitive Test; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; SMMSE: Severe Mini-Mental State Examination.
Effect size: aCohen’s d; bCramer’s V.
p < .001.
Procedure
Participants were tested in a comfortable and well-lit room, partly acoustically isolated and free of potentially interfering or disturbing stimuli. Testing for MCT validity occurred in one setting lasting 20–40 min per participant. Data were collected by three researchers who received training on MCT administration. All researchers were qualified psychologists with a music and neuropsychological background, one of whom was a certified music therapist.
Besides the MCT, the validation protocol included the following test battery:
CRIq (Cognitive Reserve Index Questionnaire; Nucci et al., 2012) is used to quantify, in a standardized model, cognitive reserve (CogR) through an interview. The questionnaire collects demographic information regarding school curriculum, work, and free-time activities combined into a single “Index of Cognitive Reserve.”
MMSE (Folstein et al., 1983) is a world standardized test for screening general cognitive function. The test consists of 11 items measuring different cognitive domains (e.g., attention, memory). Score ranges 0–30, with score ⩽23 indicating presence of cognitive deficit.
SMMSE (Harrell et al., 2000) is a brief test for the neuropsychological evaluation of cognitive domains likely preserved in individuals with moderate to severe neurocognitive disorder (i.e., MMSE < 16). The test is based on 11 items with a score range of 0–30.
MoCA (Nasreddine et al., 2005) is a brief screening tool to measure cognitive impairment. It displays good overall psychometric properties and improved sensitivity to cognitive decline compared with the MMSE (Freitas et al., 2012). It consists of 13 items measuring different cognitive domains with a score range of 0–30 and screening cutoff for normal cognition of ⩾26.
Data analysis
Data analyses were performed using IBM-SPSS Statistic V25. Effect-sizes were calculated using Cohen’s d (Cohen, 1988) for t-tests and analysis of variances (ANOVAs) or Cramer’s V (Kim, 2017) for Chi-squared test. Interpretations for Cohen’s d magnitude are given following Cohen (1988) and Sawilowsky’s (2009) suggestions.
Results
This section will firstly overview the procedures and tests conducted to evaluate MCT psychometric properties.
Test equivalence
After the development of the original version of the test in Italian, the English translation was performed following Abubakar et al.’s (2013) guidelines. The Italian version was translated by two bilinguals fluent in both languages, and subsequently back translation was made by two independent bilinguals. A panel consisting of psychologists and music therapists discussed item wording until consensus in the translation was reached.
Following Abubakar et al. (2013), to determine whether the Italian and English versions of MCT were equivalent, internal consistency based on Cronbach’s Alpha was calculated for both versions, displaying excellent and well above the recommended value α ⩾ .700 (Cicchetti, 1994; Italian-MCT α = .918, English-MCT α = .846). Furthermore, further versions equivalence was modeled on Nasreddine et al. (2005): a sub-sample of Italophone and Anglophone participants matched on age, and who had scores CRIq ⩾ 100 (medium CogR level) were selected based on two MMSE levels (healthy: MMSE ⩾ 24; moderate cognitive impairment: MMSE = 18–23). MCT scores did not differ significantly between Italophone and Anglophone participants overall, t(97.662) = .502, p = .617, d = 0.087, with Italophone M (SD) = 44.60 (8.287), Anglophone M (SD) = 43.90 (7.761), or when MMSE levels were considered separately: healthy individuals, t(69.956) = .133, p = .894, d = .0253, with Italian M(SD) = 48.58 (3.463) and United Kingdom M(SD) = 48.66 (2.808), and individuals with moderate impairment, t(16.476) = −1.485, p = .156, d = .46, with Italian M (SD) = 31.33 (5.140) and United Kingdom M (SD) = 33.78 (5.237). Therefore, results from the two countries were collapsed for further analyses.
Concurrent validity
To investigate concurrent validity making sure to avoid possible artificial inflation of correlations due to cognitive variation in the sample, Pearson’s correlations were calculated between MCT, MMSE, MoCA, and SMMSE for the total sample but subdivided by MMSE cutoff points as proposed by Tombaugh and McIntyre (1992), i.e., no impairment, 24–30; mild cognitive impairment, 18–23; and severe cognitive impairment 0–17.
Concurrent validity was robust. As can be seen in Figure 1, MCT scores were highly and positively correlated with other measures of cognitive functioning in each sub-sample. Details of MCT-Pearson correlation with the other measures are provided in Table 4, which shows that the results were significant in each MMSE sub-sample.
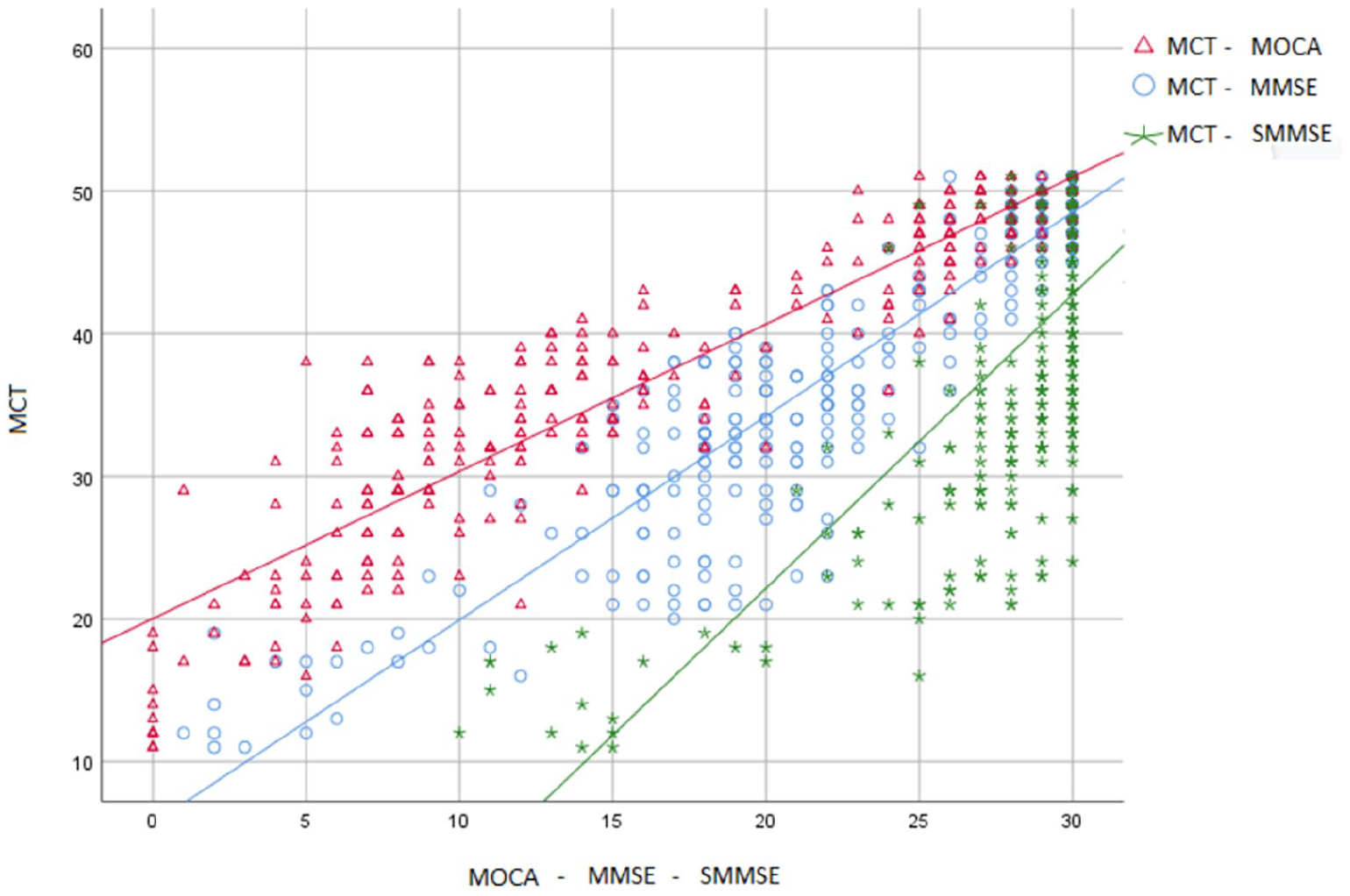
Grouped Scatterplot for the Total Sample Illustrating Pearson’s Correlations Between MCT and Three Established Tests Used in Aging Research: MMSE, MoCA. and SMMSE.
Concurrent Validity, Pearson Correlations Between MCT and MMSE, MoCA, and SMMSE.
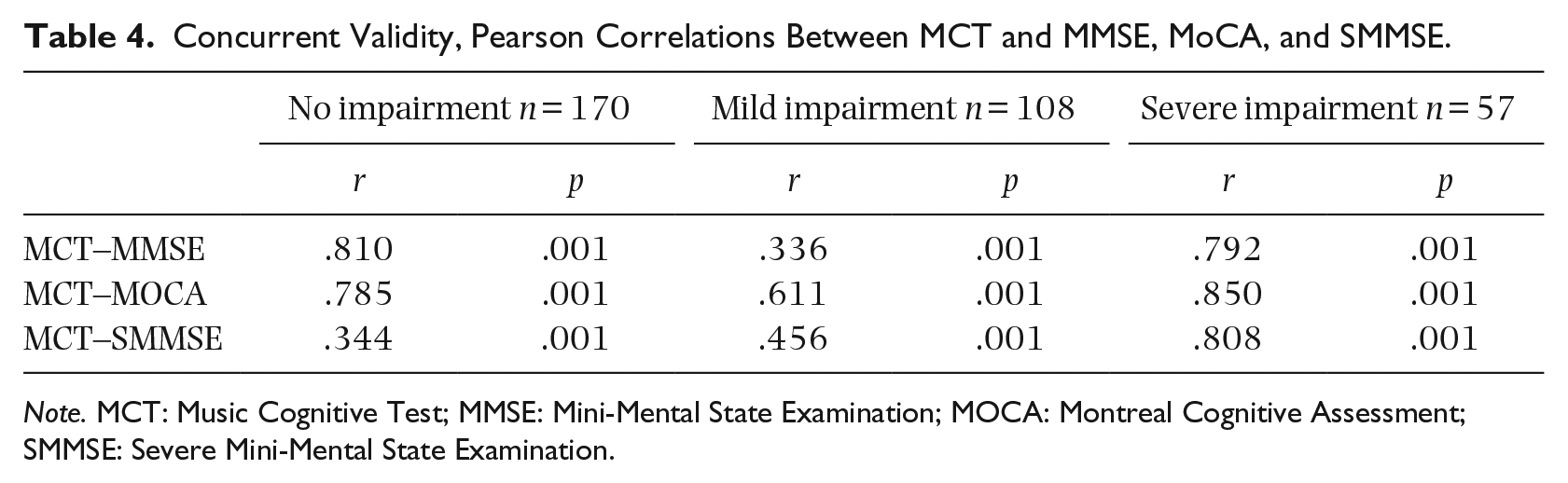
Note. MCT: Music Cognitive Test; MMSE: Mini-Mental State Examination; MOCA: Montreal Cognitive Assessment; SMMSE: Severe Mini-Mental State Examination.
Factor analyses and internal consistency
The factorability of the 19 MCT items was examined. Several recognized criteria for the factorability of a correlation were used. Firstly, it was observed that all items correlated at least with r ⩾ .2 to at least one other item, suggesting reasonable factorability. Secondly, the Kaiser–Meyer–Olkin measure of sampling adequacy was .927, above the
Mean (M), Standard Deviation (SD), and Factor Matrix (Exploratory Factor Analysis) for the MCT.
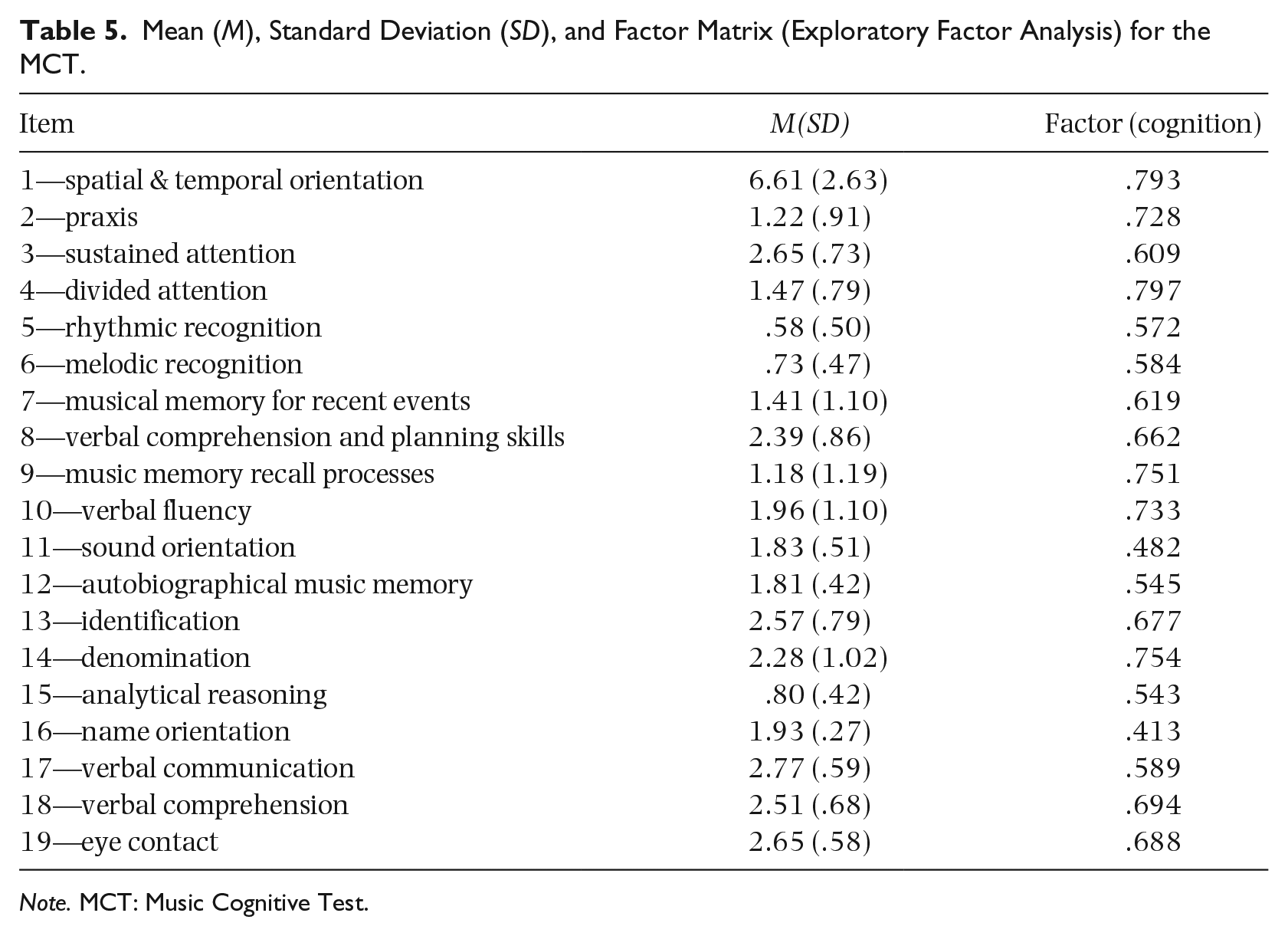
Note. MCT: Music Cognitive Test.
To avoid over-extraction of factors, web-based parallel analysis engine of eigenvalues from randomly generated correlation matrices was used (Patil et al., 2017) and values were compared with the data extracted from MCT. From the comparison of the extraction analyses, one main factor emerged: “cognition,” which explained 42.52% of the variance (Table 6).
Descriptive Statistics Mean (M) and Standard Deviation (SD), Eigenvalue, Percentage of Variance, Cronbach’s Alpha (Reliability) for the MCT Factor.
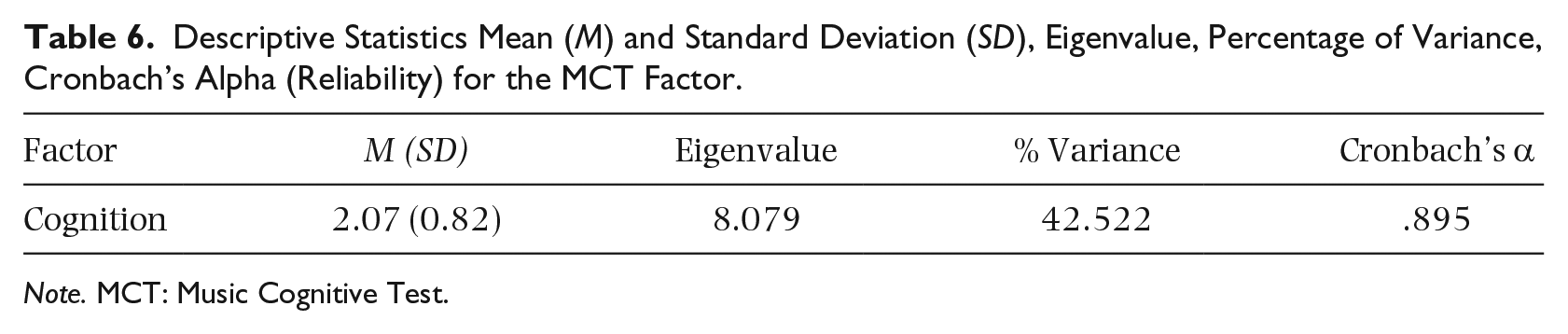
Note. MCT: Music Cognitive Test.
Internal consistency was calculated through Cronbach’s alpha to understand whether all items of the test measured the same latent variable “cognition” (Green et al., 1977). MCT internal consistency for the total sample was very good (Cronbach’s α = .895, Table 6). SPSS Cronbach’s alpha function showed that no substantial increases in alpha value would have been achieved by eliminating any of the MCT items.
Sensitivity and specificity
Sensitivity and specificity were determined comparing MCT results with the MMSE and MoCA cutoff. Following Nasreddine et al.’s (2005) guidelines, a cutoff ⩾ 26 was used for MoCA and MMSE to select participants with no cognitive decline (Tombaugh & McIntyre, 1992) and compare them to a MCT healthy sample. Through contingency tables, a cutoff at MCT = 45 yielded the best balance between sensitivity and specificity (i.e., scores < 45 indicate impairment). The MCT exhibited excellent sensitivity in identifying individuals with cognitive impairment both with MMSE and MoCA diagnostic criteria (99.4% and 93.0%, respectively), with a positive predictive value of 94.7% with MMSE and 98.4% with MoCA. Specificity was delineated as the percentage of participants that scored at or above the cutoff scores of MCT ⩾ 45 and MMSE and MoCA ⩾ 26. MCT showed excellent specificity as it correctly identified 93.5% and 97.8% of healthy participants based on, respectively, MMSE and MoCA diagnostic values. Negative predictive value was 99.3% in relation to MMSE and 90.3% for MoCA.
From the 335 participants, 68 had a diagnosis of neurocognitive disorders according to medical referral data, with 57.4% having a degenerative disorder (Alzheimer, Parkinson, or Lewy body disease), 16.7% mixed dementia, 16.7% vascular dementia, and 9.2% mild cognitive impairment. To test if MCT sensitivity was also confirmed in this sub-sample, a group of healthy participants with no declared neurocognitive disorder (n = 25) and MMSE scores ⩾ 24 cutoff (normal cognition), matched for age, education, and CRIq level, were selected from the total sample and a t-test was performed to compare the two sub-samples. The results (Table 7) showed a statistically significant difference between healthy individuals and individuals diagnosed with neurocognitive disorder, with a very large effect size in all tests measuring cognitive performance, including MCT.
Demographic and Cognitive Assessment Data of Participants With and Without Neurocognitive Disorder.
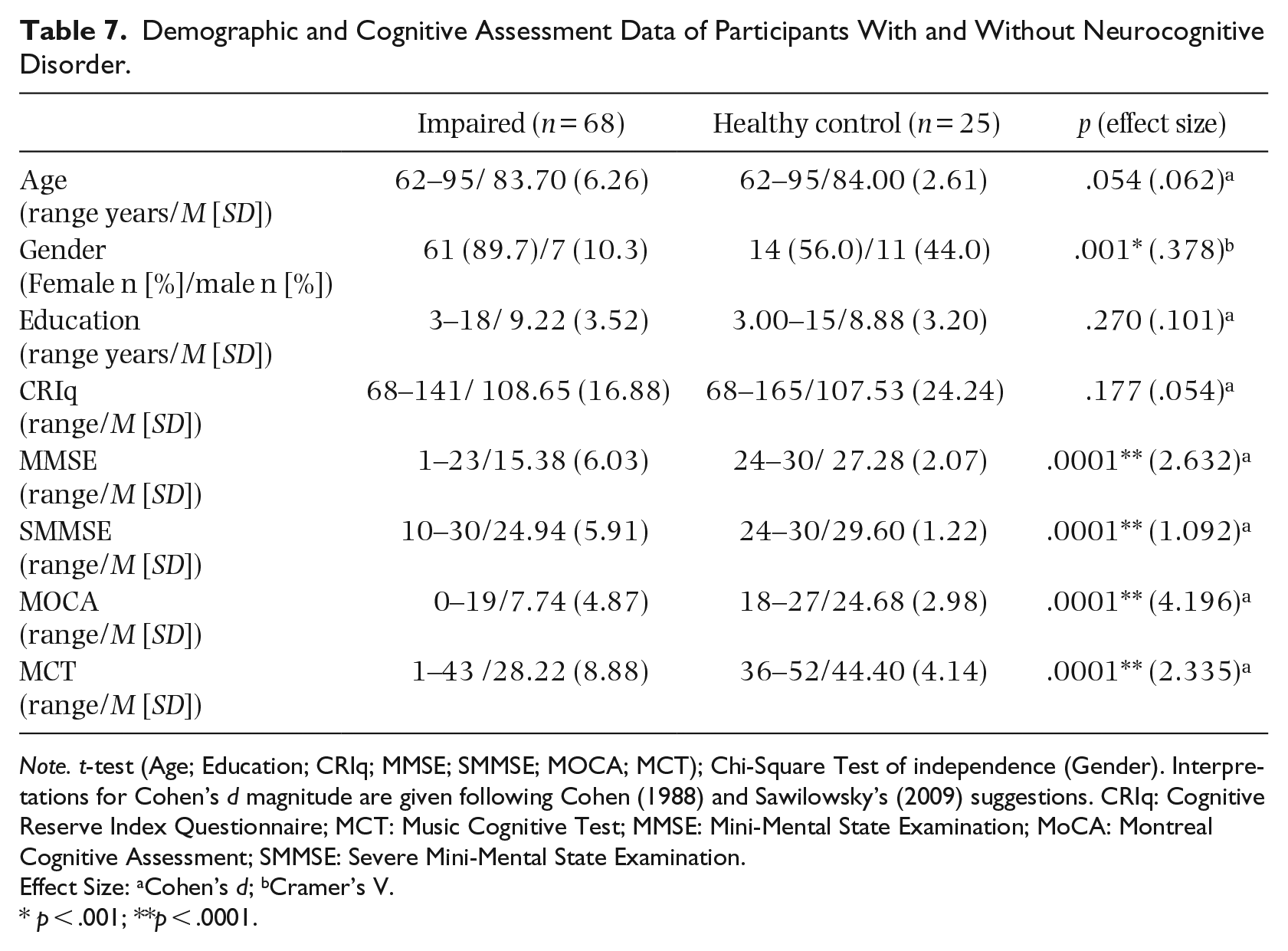
Note. t-test (Age; Education; CRIq; MMSE; SMMSE; MOCA; MCT); Chi-Square Test of independence (Gender). Interpretations for Cohen’s d magnitude are given following Cohen (1988) and Sawilowsky’s (2009) suggestions. CRIq: Cognitive Reserve Index Questionnaire; MCT: Music Cognitive Test; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; SMMSE: Severe Mini-Mental State Examination.
Effect Size: aCohen’s d; bCramer’s V.
p < .001; **p < .0001.
MCT inter-rater reliability
Two expert music psychologists were trained in the MCT scoring by the first author, practiced independently on a minimum of n = 5 to n = 10 non-study participants and had the opportunity to discuss any difficulties with the trainer. Subsequently, they observed the main researcher during the administration of MCT to n = 30 participants (age: M [SD] = 75.36 [16.69]; education: M [SD] = 8.65 [4.49]; CRIq: M [SD] = 106.53[23.10]) and scored each participant independently.
Inter-rater reliability of the MCT scores between the main researchers and the two judges was analyzed using Intraclass Correlation Coefficient (ICC) for average measure analyses. Absolute agreement, 2-way mixed-effect model was chosen to evaluate how consistent the rates by the three examiners were. The inter-rater reliability was excellent, with ICC = .986, with a 95% confidence interval from .975 to .993, F(29, 58) = 72.018, p < .001.
MCT adjustment scoring coefficient
In some contexts, it might be useful to correct scores in function of relevant demographic variables that may have an impact on the total score (e.g., as reported for MMSE and MoCA). To calculate scoring adjustment coefficients for MCT, an initial linear regression model was computed between MCT total score and age (<60 years; >60 years), educational level (higher, lower) and years of music education. Following Magni et al.’s (1996) recommendation, only individuals with MMSE scores ⩾24 were included, to limit the influence of participants affected by cognitive decline. The results revealed no significant regression for years of music education in either the two age groups (p > .05), and for age in the age range < 60 years (p > .05). However, the regression was significant for age (p < .05) in the age range > 60 years. Therefore, this group was further divided into three sub-groups (60–69; 70–79; >80 years). To have an adequate sample stratification, participants were divided into 2 educational levels: higher (>11 years) and lower (<11 years). The 11-year cutoff was chosen because in many countries this corresponds to the end of compulsory education. Based on the linear regression model, final adjustment coefficients for the raw MCT scores were calculated by subtracting the mean MCT score of the whole sample from the predicted values for each education and age class (Magni et al., 1996). Table 8 presents the derived adjustment scoring coefficients to correct MCT scores in function of age and educational level.
MCT Adjustment Scoring Coefficients.
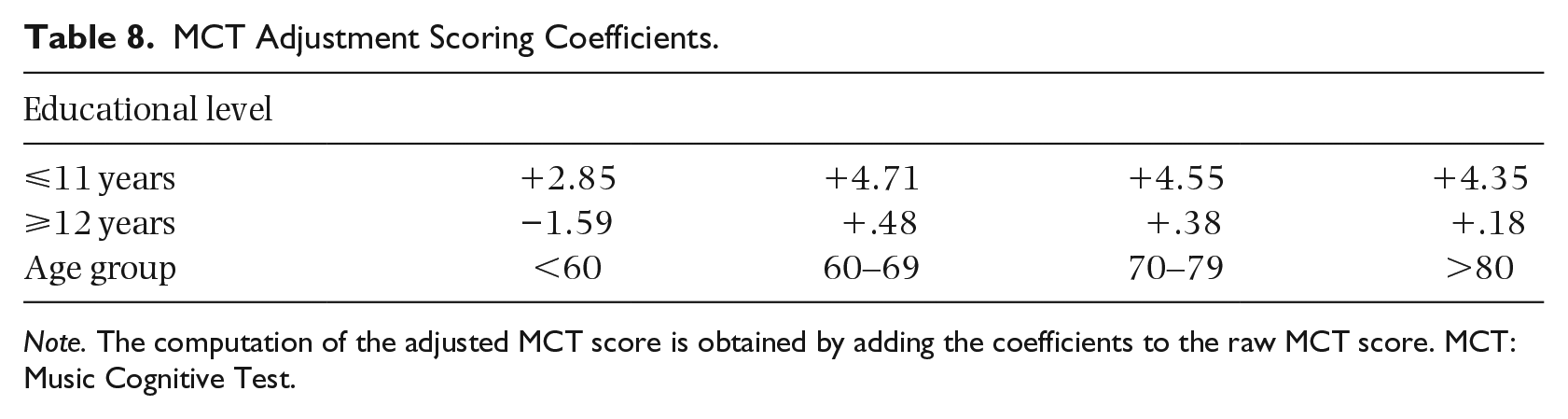
Note. The computation of the adjusted MCT score is obtained by adding the coefficients to the raw MCT score. MCT: Music Cognitive Test.
Test-retest reliability
Test-retest reliability was assessed on a sample of 70 participants (age: M [SD] = 75.01 [19.62]; education: M [SD] = 10.18 [4.84]; CRIq: M [SD] = 105.78 [18.05]) who had a second evaluation 1 month after their first. Pearson’s correlation of scores collected on the first and second evaluation revealed a strong linear relationship, r = .942, p < .001; with a 95% confidence interval from .86 to 1.0 and a mean change in MCT test of 0.88 ± 1.28, thus indicating excellent test-retest reliability.
Evaluation of MCT pleasantness
As musical experiences are usually enjoyable (Biasutti & Mangiacotti, 2021), the use of a music-based assessment might mitigate anxiety associated with testing situations and could provide a non-threatening condition for self-expression (Layman et al., 2002; Lipe, 2015). At the end of the MCT, participants commented on the test by answering a verbal open-ended question (“How did you find the present [MCT] test compared to the other cognitive assessments that you have experienced?”). This form of assessment was chosen to minimize participant burden with further quantitative evaluations and to give them freedom to express themselves. Answers were manually transcribed by the examiner and analyzed using content analysis (Biasutti, 2013) through ATLAS.ti (Scientific Software Development-GmbH for qualitative text analysis) to achieve a quantitative insight on the responses. Three content categories were obtained: “MCT pleasantness,” “MCT interest,” “No Statements.” Across the 335 participants, 69.55% found the test “entertaining”/“enjoyable”/“fun,” and from those, 52.86% stated that MCT was “more enjoyable compared to the other [MMSE, MOCA, SMMSE] tests [of the assessment battery]”; 16.42% found the test “interesting,” and 14.03% did not provide any statement.
MCT in older participants (60+)
To understand whether MCT is a useful tool to investigate cognitive functions specifically in older adults 60+ (n = 222 from the total sample n = 335), an independent samples t-test was performed within each of the three age subgroups (60–70; 71–80; 81+) to compare scores across MMSE cutoff (MMSE = 24). MCT scores reliably differentiated participants across the MMSE cutoff in all three older age groups with statistically significant differences and a very large effect size for MCT (p < .001), similarly to MMSE (p < .001), MoCA (p < .001), and also SMMSE (p < .05; Table 9).
MCT Results of the 60+ Sample Divided by Age Subgroup and MMSE Cutoff = 24.
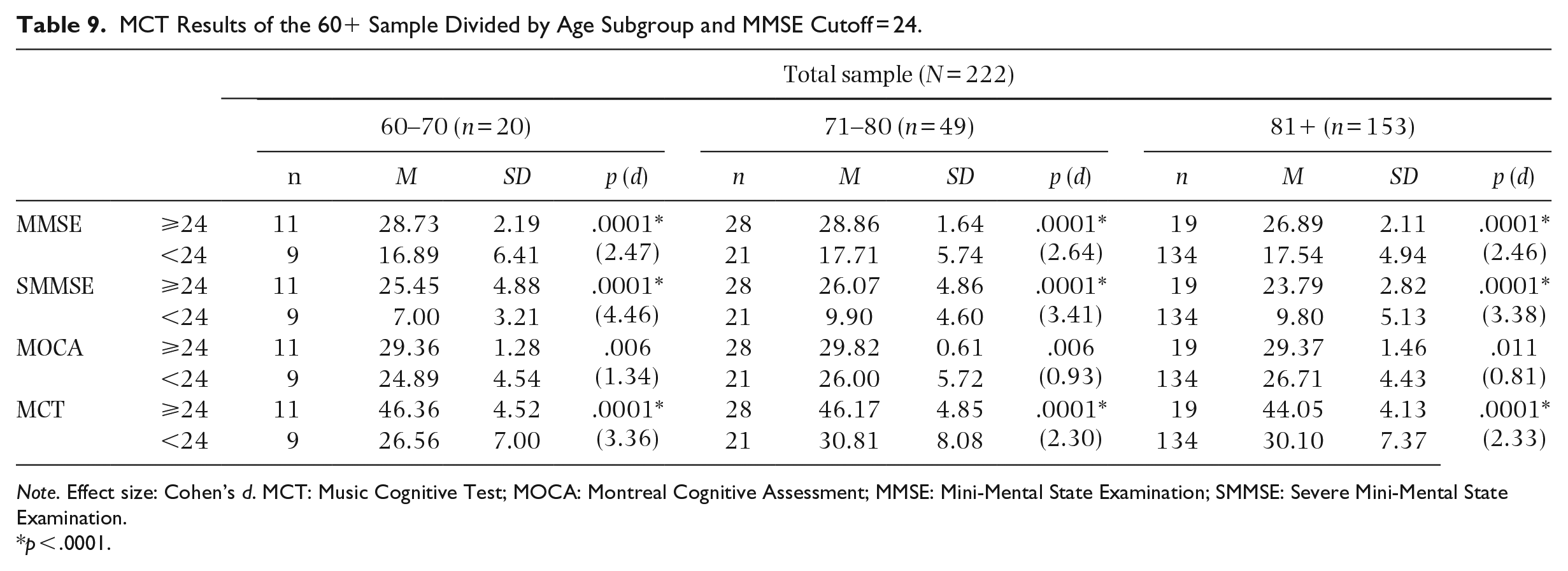
Note. Effect size: Cohen’s d. MCT: Music Cognitive Test; MOCA: Montreal Cognitive Assessment; MMSE: Mini-Mental State Examination; SMMSE: Severe Mini-Mental State Examination.
p < .0001.
Discussion
In this article, we presented MCT, a novel screening test created to assess cognitive abilities stimulated by music-making treatments, with a view to facilitate music therapists in monitoring cognitive functions that may be targeted within their interventions, particularly with older individuals. We aimed for a test based on objective assessments, quick to administer and easy to use, and therefore suitable for music therapists’ everyday practice. Similarly to MoCA and MMSE, MCT covers domains of spatial and time orientation, language (comprehension and production), memory, attention, executive functions, and motor performance. MCT can help therapists understand patient cognitive status and fine-tune treatment (Davis et al., 2008), establishing a participant’s baseline, defining therapeutic goals (Norman, 2012), and evaluating the overall intervention efficacy (Wilson, 2000). That is, the test can be used by music therapists to understand the general cognitive level of their patients at baseline (prior to starting intervention) and compare it with performance assessed a few months after the beginning of the intervention period. Furthermore, therapists may use MCT as a starting point before implementing music-based activities targeting a particular cognitive ability. Importantly, it could be used to consistently highlight music-making benefits to patient’s families and staff members (Saad, 2017), for example, in care-homes. Moreover, because the test assesses specific cognitive functions stimulated by guided musical engagements, it could be used more broadly in research to measure possible cognitive effects of pre-post music-interventions (Mangiacotti et al., 2019).
To explore MCT psychometric characteristics, we developed a large-scale multinational validation. MCT revealed high test-retest reliability and validity, and good internal consistency. Moreover, MCT showed excellent concurrent validity with existing tests, thus confirming that it can provide reliable evaluations of participants’ cognitive functioning. Furthermore, the strong correlation with the SMMSE indicated that MCT is useful in detecting cognitive decline at lower ranges of functioning, thus expanding the range captured by MMSE and MOCA (avoiding “flooring” effects)—a feature that was not considered by other musical tests (Hintz, 2000; Lipe et al., 2007; Mitsudome, 2013; York, 1994, 2000). Importantly, the correlation between MCT and SMMSE suggests that MCT, similarly to SMMSE, measures “overlearned” knowledge, which is possibly better maintained in severely impaired individuals (Harrell et al., 2000). Furthermore, it appears that MCT provides useful information about both general cognitive functioning and musical abilities while effectively measuring the overall progression of neurocognitive disorder in people with mild to severe cognitive impairment.
When analyzing the correlation coefficient by MMSE cutoff, the results suggested similarities between MCT and the other cognitive assessments. The strong MCT–MoCA correlation in the range of people with mild cognitive impairment suggests that, similarly to MoCA, MCT is more sensitive than MMSE to subtle cognitive deficits, perhaps due to the presence of brief executive function assessments (Dong et al., 2010; Pinto et al., 2019). From the correlational analysis, it also emerged that MCT defines a unique musical cognitive aspect, similarly to RMST (York, 1994). As reported in the literature, music can trigger different brain regions simultaneously, hence stimulating impaired brain areas by activating alternative pathways in those with cognitive impairment (King et al., 2019; Putkinen et al., 2021). Consequently, MCT could provide an enhanced picture of a person’s residual cognitive skills and, in turn, be suitable to seize possible cognitive improvement resulting from music-rehabilitation therapy.
Our validation covered a wide age range (18–100 years old), and two important findings indicate that MCT is a suitable tool for aging populations: (a) in the large-scale cross-national validation, 65.1% of participants were aged 60+, 79.43% of whom lived in care-home setting; (b) MCT was found to reliably discriminate 60 + year old individuals with established neurocognitive decline. Therefore, it can be confidently concluded that MCT is a sensitive screening tool for the assessment of older adults, and suitable to be used in care-home setting (Kim, 2005; Schlenghe & Murphy, 2000).
Participant feedback in relation to the pleasantness of the assessment was generally positive, highlighting that MCT is enjoyable, making it particularly suitable in challenging evaluation settings, such as care-homes, or with participants with mild cognitive impairment who often find some MMSE items “insultingly simple” (Nasreddine et al., 2005, p.698). These findings are in line with Layman et al. (2002) and Lipe (2015), suggesting that a music-based assessment would more likely produce a pleasurable experience, reduce test anxiety, and facilitate participants’ self-expression. Thanks to these features, MCT is well tolerated also by participants with moderate to severe cognitive impairment—playful and interactive aspects being important when working with older adults with neurocognitive disorders, considering that fatigue could seriously affect their performance. Moreover, participants with cognitive decline sometimes get frustrated when facing difficulties in responding to the examiner during cognitive tests, and this may negatively affect their performance, and potentially increase the risk of withdrawal from studies or clinical programs. Through its playful nature, MCT overcomes these problems, increasing its effectiveness, particularly with the frailer group suffering from cognitive impairment.
Consistently with other cognitive test validation studies, performance on either MMSE, MoCA, SMMSE, and MCT correlated with participants’ educational backgrounds (Folstein et al., 1975; Harrell et al., 2000; Nasreddine et al., 2005). However, this study is the first of its kind in the music assessment field because it takes into consideration also the participants’ CogR level (Katzman et al., 1988; Stern et al., 1994), which allows us to have a more nuanced picture of their cognitive profile. Future studies should include this variable instead of or alongside participants’ educational level. CogR is a measure of the amount of learning, skills, and knowledge acquired during lifespan (not only in childhood), which may explain the ability of some individuals with high CogR to show only minor symptoms during neurodegenerative brain damage. This concept is therefore closely related to neurobiological processes of learning, and it has been found able to predict not only the evolution of neurocognitive degenerative symptomatology but also the effect of cognitive stimulation of individuals with neurocognitive disorders, or the rehabilitation of people with traumatic brain/vascular injuries (Mondini et al., 2016; Puccioni & Vallesi, 2012). In other words, the brain of an individual with high CogR has built many synaptic connections to the point of creating alternative brain networks, which can be easily accessed in special conditions (i.e., remaining more plastic).
Statistical analyses comparing MCT scores based on (a) participant’s educational level (higher/lower), (b) musical background level (with/without experience) and (c) age group (<60 years; >60 years) did not detect any differences in MCT scores in the levels of musical background or according to age group <60 years. Although an MCT score difference in the age range >60 years was found, therefore, this group was further divided into three sub-groups (60-69; 70–79; >80 years) and adjustment coefficient scores were calculated accordingly. However, unequal sample size between those with and without musical experience should be noted, and future research should aim to control the level and type of music education/practice.
There is some ambiguity in the literature around MMSE and MoCA cutoff scores to identify individuals with normal versus impaired cognition (e.g., Carson et al., 2018; Elkana et al., 2020; Mitchell, 2017). In this study, we calculated MCT cutoff through sensitivity and specificity analyses based on MMSE and MoCA cutoff of ⩾26 (Tombaugh & McIntyre, 1992). To obtain a more specific cutoff, future studies should consider defining an MCT cutoff based on percentile scores with an extended sample of the relevant population (Nguyen et al., 2002; Solias et al., 2014). Further studies should also examine whether some MCT tasks are more sensitive to different types of cognitive changes (e.g., performance in music memory tasks in relation with Alzheimer’s stages), which could help understanding the course of the impairment and, conversely, a therapeutic intervention could take. Moreover, it would be useful to investigate the convergence between MCT and other measures (MT, well-being), to understand the relationship between cognitive functions measured by MCT and quality of life improvement brought by music-related interventions. Finally, it is hoped that future research will also explore MCT usability in different contexts (e.g., children with special needs, psychiatric settings), perhaps with some specific adjustments such as adding more items to measure each sub-dimension.
To achieve a good overall understanding of MCT outcomes, we suggest that practitioners intending to use it (including music professionals working in rehabilitation settings) carefully familiarize themselves with the administration and scoring procedures and are suitably trained and experienced in the use of cognitive screening measures to interpret the outcomes.
Our findings suggest that MCT is a novel, highly reliable cognitive-neuropsychological measurement tool that has filled the gap between main cognitive tests not generally suitable for use by music therapists and music evaluations not rigorous enough. When addressing important questions concerning the effectiveness of an increasingly used form on non-pharmacological intervention, such as MT, MCT will allow researchers and therapists to assess participants, including those with impaired cognitive functions, in a playful way. This is consistent with previous findings on how music could be used to reduce participant burden in rehabilitation settings (Biasutti & Mangiacotti, 2018). The enjoyability of the musical tasks and short duration make MCT a suitable tool to also be used independently by therapists implementing music therapies and activities, enabling them to understand which cognitive abilities are impaired and flexibly adapt therapy (Lipe & York, 2007). In this respect, MCT could be a game-changing tool in the field of intervention studies involving music-based activities, particularly with the older population.
Supplemental Material
sj-docx-1-pom-10.1177_03057356221100851 – Supplemental material for Development and validation of the Music Cognitive Test: A music-based cognitive screening test
Supplemental material, sj-docx-1-pom-10.1177_03057356221100851 for Development and validation of the Music Cognitive Test: A music-based cognitive screening test by Anthony Mangiacotti, Giovanna Cipriani, Emma Ward, Fabia Franco and Michele Biasutti in Psychology of Music
Footnotes
Acknowledgements
The research was conducted as part of the first author’s doctoral studies co-supervised by MB (Padua, Italy) and FF (Middlesex, United Kingdom). AM was funded by MURST PhD scholarship University of Padua and supported by Middlesex University for the duration of the project. We are grateful to SEMPRE for providing seed funding for the cross-national project and for funding AM’s participation to the Alzheimer’s Association International Conference 2019. The positive outcome of this research would not have been possible without the support of Dr. Ming Hung Hsu and MT Clare Barone at MHA; Thanks to Dr Jana Martiskova, CEO Danny Bluestone, Dr Maura Bellio, and MHA for supporting data collection in United Kingdom and the Centro Anziani D. Sartor for supporting data collection in Italy. Psy MT Ros Flowerdew (MHA) and Psy Elena Bruzzi (UniPd) for helping in the data collection and Dr Sam Barnett (Imperial College London) for technical, logistical, and moral support. Finally, many thanks to professional artist Angelica Fazzari (Ig: @angymoo_) who designed the MCT logo and produced the drawings used in the test.
Author contributions
AM and MB conceptualization of MCT; AM and GC created the first draft of MCT items; FF, MB, and EW contributed to the final version of MCT; AM collected and analyzed the data; FF and EW supervised the research in the United Kingdom; MB and GC supervised the research in Italy; AM prepared the first draft of the paper; all authors contributed to writing of the paper.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SEMPRE 3,821£; AM was funded by MURST PhD scholarship University of Padua and supported by Middlesex University for the duration of the project.
Ethical approval
Ethical approval has been granted by Padua University Psychology Research Ethics Committee (November 2017—Application no. 2449) and by Middlesex University Psychology Research Ethics Committee (February 2018—Application no. ST020-2018).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.