
Abstract
Background:
Traveller patients have distinctive clinical characteristics compared to non-traveller patients. Local information about the clinical features of traveller patients is lacking.
Objectives:
The objective of this study is to evaluate the clinical characteristics of traveller patients presenting to a hospital near the Hong Kong International Airport.
Methods:
This was a single-centred, retrospective cohort study. Medical records of all traveller patients presenting to the Accident and Emergency Department of North Lantau Hospital in Hong Kong from 1 January 2019 to 31 December 2019 were reviewed. The demographics, triage category, presentation, outcomes and disposal were retrospectively evaluated and compared between traveller and non-traveller patients.
Results:
There were 528 traveller patients attending the Accident and Emergency Department of North Lantau Hospital during the study period, constituting 0.6% of total annual attendance. About one-third of the traveller patients required admission. The most common discharge diagnoses were gastrointestinal diseases (14.8%), followed by trauma (12.9%) and other neurological diseases (12.9%). Traveller patients had a higher rate of being triaged as critical and emergency categories (p < 0.001), higher admission rate (p < 0.001), higher need for active resuscitation (p < 0.001) and escort (p < 0.001) when compared to non-traveller patients. Around 1.3% of traveller patients presented with out-of-hospital cardiac arrest and were eventually certified dead in Accident and Emergency Department.
Conclusion:
The traveller population constitutes a small proportion of the patient population, but they can have a significant impact on the Accident and Emergency Departments in high-impact traveller areas. Additional resources such as manpower support and training programmes would be beneficial for Accident and Emergency Departments in high-impact traveller areas.
Introduction
Hong Kong is a famous metropolitan and renowned for its tourism and hospitality. Around 60 million visitors arrived in Hong Kong in 2019, and more than 70 million passengers pass through Hong Kong International Airport (HKIA) annually.1,2 North Lantau Hospital (NLTH) is located in central Tung Chung of Lantau Island, and its ambulance service catchment includes the HKIA. NLTH is a community hospital, supporting the Princess Margaret Hospital (PMH), a tertiary hospital in the cluster. NLTH provides 24-h accident and emergency service, acute in-patient service, and various outpatient services, serving the population of Lantau Island and also the floating population in the HKIA and Hong Kong-Zhuhai-Macao Bridge. It has an annual patient attendance of 70,000, including around 600 travellers. NLTH receives travellers presenting with various types of medical complaints, from a simple minor trauma to cardiac arrest.
In NLTH, the acute in-patient service is provided by the emergency medicine wards (EMW), which offer services for patients with acute medical conditions and psychiatric diseases. Patients in EMW are under the care of emergency physicians in collaboration with other clinical specialties, such as psychiatric nurses, psychiatrists and other allied health professionals. 3 Patients who need in-patient care of other specialties, such as complex medical conditions, surgical, obstetrics and gynaecological conditions, are admitted to the appropriate specialist wards in other hospitals in the cluster, including PMH, Kwai Chung Hospital (KCH), Caritas Medical Centre (CMC) and Yan Chai Hospital (YCH). In general, patients under specialties of medicine, surgery, intensive care, orthopaedics, paediatrics, obstetrics and gynaecology are admitted to PMH. Patients with psychiatric illness, ophthalmology and ear, nose and throat diseases are admitted to KCH, CMC and YCH, respectively. Exceptions are for burns and body packer patients, where there are no appropriate specialty facilities within the same cluster; therefore, they are admitted to Kwong Wah Hospital (KWH) Burn Unit and Queen Elizabeth Hospital (QEH) custodial ward accordingly. The interhospital transfer from NLTH to PMH is 38 minutes on average, which might on occasion require escort by doctors or nurses.
Travellers with chronic medical problems may have acute exacerbations precipitated by long-haul flights and jetlag, 4 or may suffer from acquired conditions, including traveller’s diarrhoea, vector-borne diseases or rarer conditions, such as altitude sickness. Various challenges are encountered when managing international traveller patients, including language barriers, cultural differences, unclear medical records and differences in expectations for health service needs. In addition, there are some distinct entities which are exclusively featured in traveller groups, such as body packers, exotic infectious diseases and requirements for assessment for fitness for flight boarding.
The objective of this study was to evaluate the clinical characteristics of the traveller patients presenting to the Accident and Emergency Department (AED) of NLTH, including basic demographic characteristics, past medical health, triage category, presenting symptoms, diagnosis and disposal. In addition, differences in triage category, admission rate, resuscitation and escort requirement for traveller patients are compared with non-traveller patients. Local publication on the clinical features of traveller patients is lacking in Hong Kong, and this study is the first study to report the experience managing traveller patients in an AED close to the HKIA. This study may help stipulate resource allocation for traveller’s care in the hospital and facilitate clinical management for their conditions.
Methods
This retrospective cohort study was conducted at the AED of NLTH, Hong Kong. Medical notes of all traveller patients attending the AED of NLTH from 1 January 2019 to 31 December 2019 were reviewed. Data are collected and compared between the exposed group (traveller patients) and the non-exposed group (non-traveller patients). Traveller patients were defined as patients travelling from countries and territories outside Hong Kong through the HKIA and who were not Hong Kong residents. Non-traveller patients were defined as all other patients who attended AED in the study period except traveller patients.
The AED and hospital records of each traveller patient were reviewed, with the data collected including age, gender, underlying chronic illnesses, triage category, presenting complaint, discharge diagnosis, disposal, resuscitation and needs of escort. The attendance, triage, discharge and admission summary data of the study period were retrieved in the A&E master statistics module, and subsequently, the non-traveller patient data were generated by deducting the traveller patient data. Primary outcome was measured as the percentage of Triage Category 1–2 (critical and emergency). The triage system is a patient prioritisation system adopted by all AED in Hong Kong. Patients are stratified into five categories according to their medical condition as critical, emergency, urgent, semi-urgent and non-urgent for categories 1–5, respectively. 5 Secondary outcomes were admission rate, rate of resuscitation and rate of escort requirement in AED.
The presenting complaint was identified as the chief complaint presented in triage, and the discharge diagnosis was identified as the diagnosis documented in the AED record on disposal. Resuscitation was defined as the process of providing support to airway (intubation), breathing (high flow oxygen, non-invasive ventilation), circulation (cardiac arrest, shock, myocardial infarction, unstable arrhythmia) and disability (acute stroke, convulsion, unconsciousness). Admission was defined as direct admission from AED to a public hospital ward (including EMW, excluding observation ward). Emergency physicians had admission right to most hospital wards except Intensive Care Unit, Coronary Care Unit, Infectious disease Ward, Burn Unit, Ophthalmology ward and Ear, nose and throat ward. There was a departmental admission guideline in NLTH AED. 6
For the purpose of intra- or interhospital transfer, there were two categories of critically ill patients. Category 1 referred to patients who are intubated or ventilated, including non-invasive ventilation. Category 2 included non-intubated patients with one or more of the following conditions: at risk of losing airway patency, requiring high-flow oxygen therapy, at risk of respiratory failure, haemodynamically unstable, having recent history of sudden cardiac arrest or arrhythmia, impaired conscious level, convulsion or other conditions associated with high risk of life-threatening complications as determined by the doctor in charge. 7 Body packers were defined as individuals with concealing of illicit drugs in the abdominal or pelvic cavity of the body.
Statistical analysis
The Statistical Package for the Social Sciences (Windows, version 19.0; SPSS, Inc., Chicago, IL, US) was used for all analyses. Descriptive statistics were used to summarise patient demographics. Univariate analysis was performed with the chi-square test or Fisher’s exact test for comparison of proportions. A p-value of less than 0.05 was considered statistically significant.
Results
During the study period, the total AED attendance was 95,591. Of these, 967 were Triage Category 1–2. Meanwhile, 238 cases required resuscitation; 13,700 cases were admitted and 1918 cases required escort. However, 528 traveller patients were identified and recruited, constituting 0.6% of the total AED attendance.
Of these 528 traveller patients, 56.5% were male and 43.3% were female. The mean age was 42.4 (SD = 19.9) years, with the commonest age group being 18–39 years (35.2%). All of them travelled to Hong Kong by air travel. The most common triage category was Category 3 (59.7%), followed by Category 4 (30.7%). Triage Category 1–2 constituted 9.1% of cases. The majority of them (56.1%) had unremarkable past medical history (Table 1).
Patient demographics.
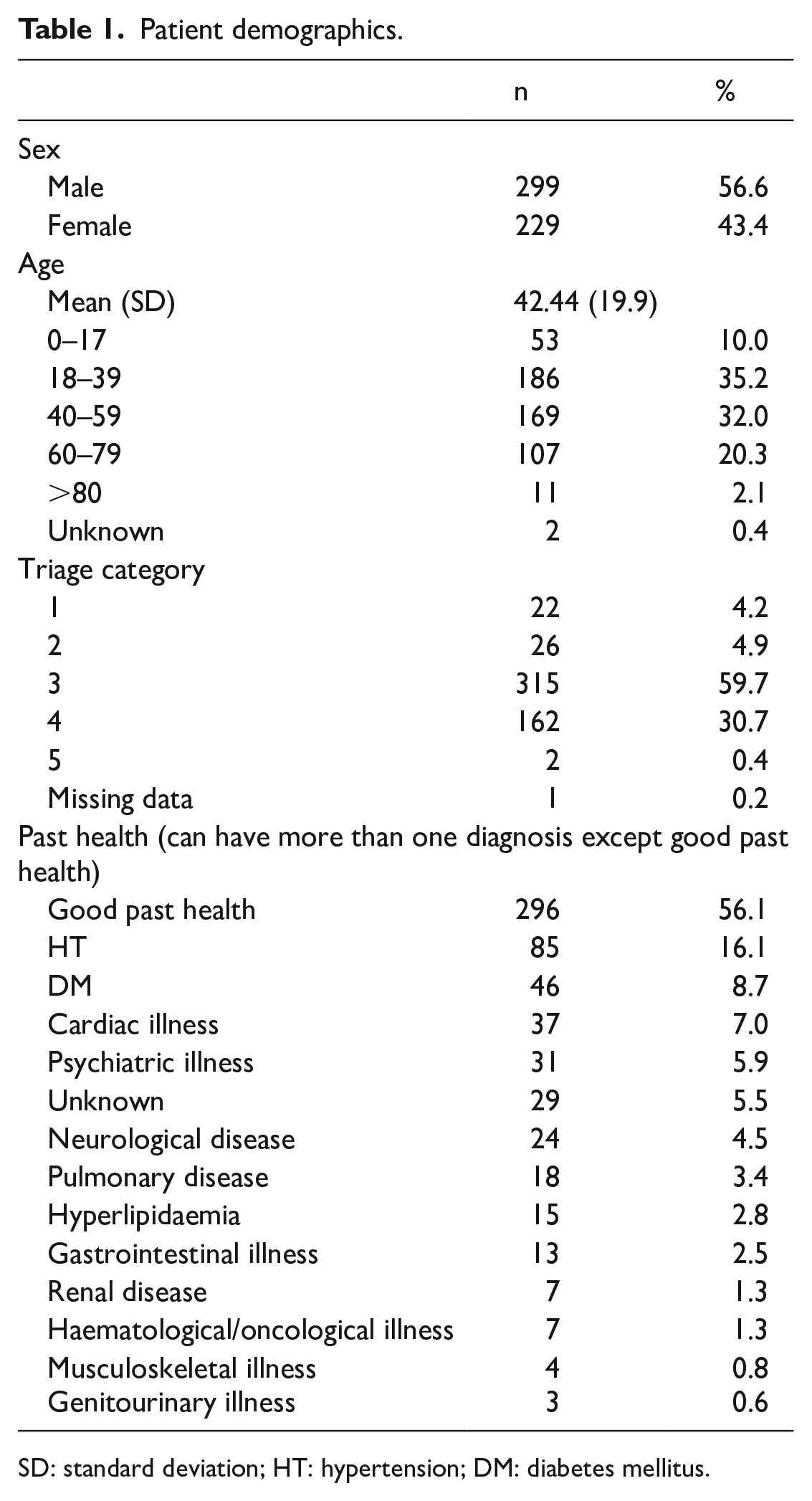
SD: standard deviation; HT: hypertension; DM: diabetes mellitus.
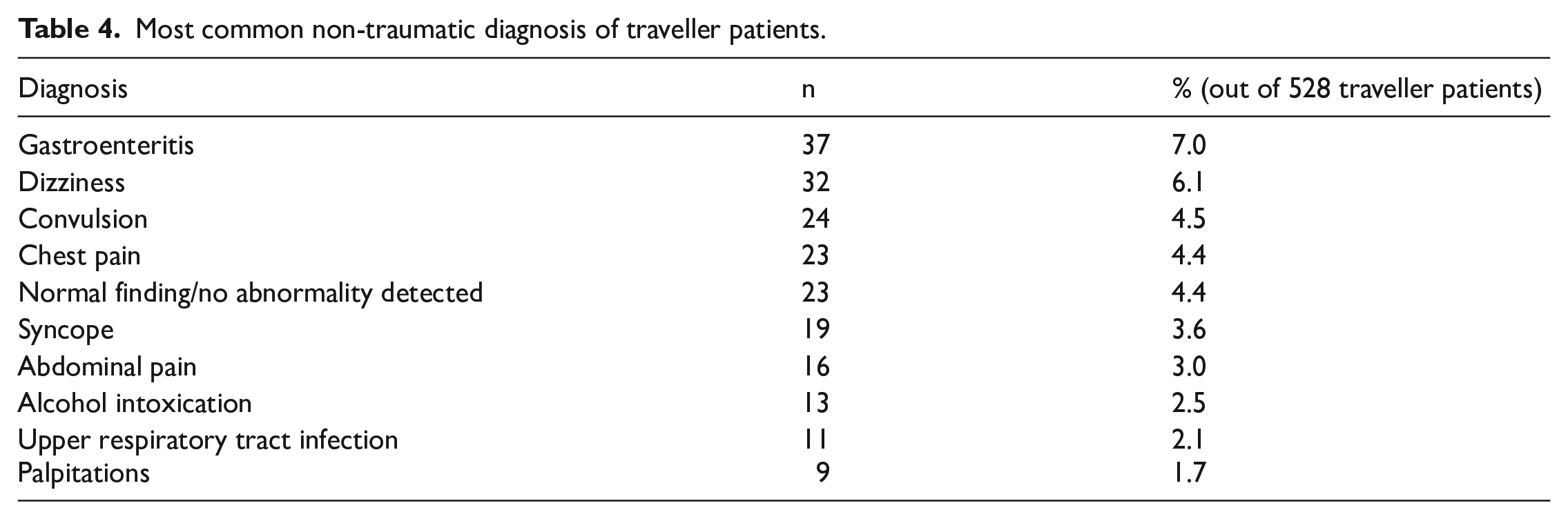
Among the presenting complaints, 86.4% were non-traumatic. The most common presenting complaints among traveller patients were gastrointestinal symptoms (15.3%), followed by trauma (12.1%) (Table 2). The most common discharge diagnoses among traveller patients were gastrointestinal diseases (14.8%), followed by trauma (12.9%) and other neurological diseases (12.9%) (Table 3). The most common traumatic discharge diagnosis was head injury (4.4%, 23/528), while the most common non-traumatic discharge diagnosis was gastroenteritis (7.0%, 37/528) (Table 4).
Presenting symptoms of traveller patients.
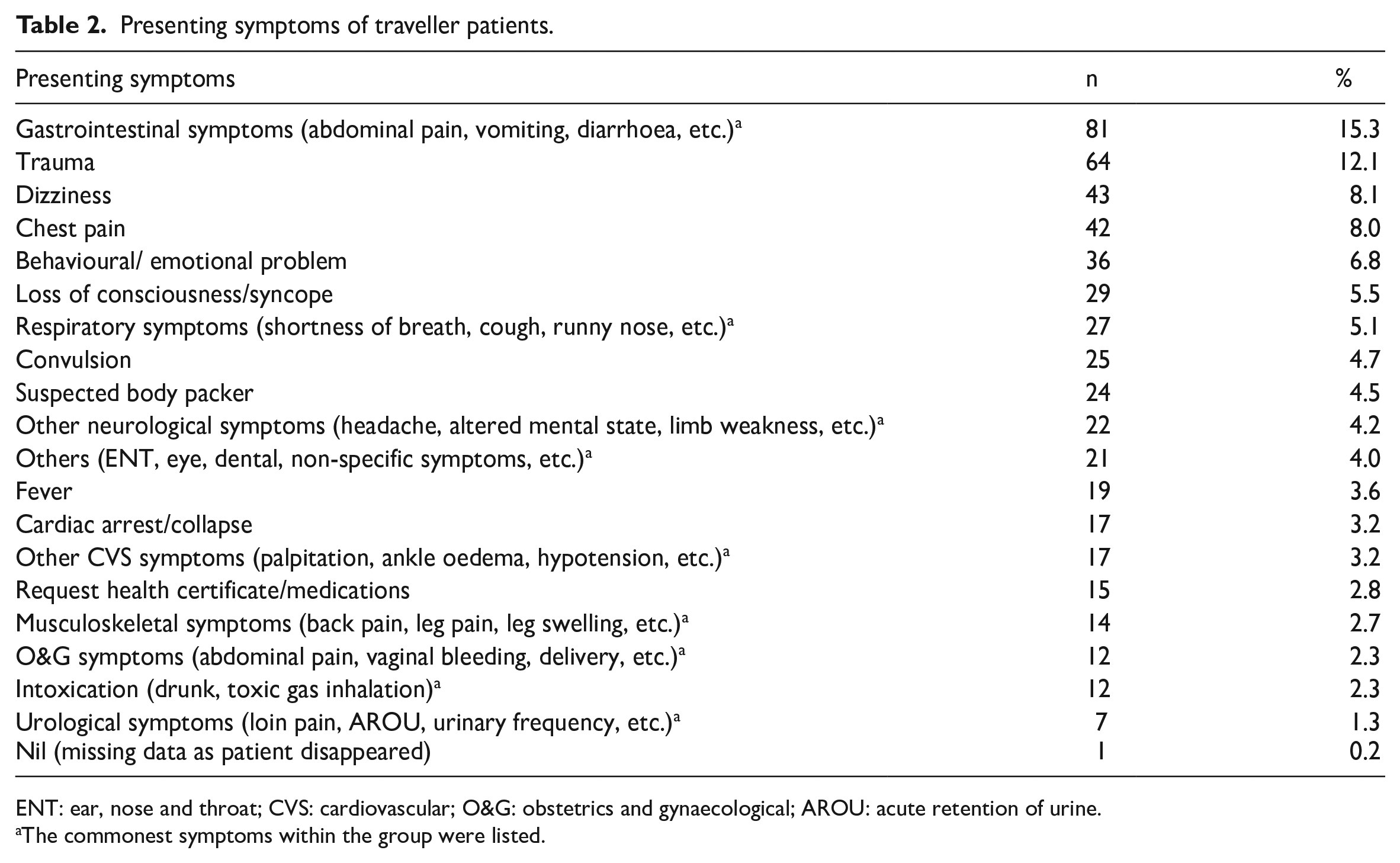
ENT: ear, nose and throat; CVS: cardiovascular; O&G: obstetrics and gynaecological; AROU: acute retention of urine.
The commonest symptoms within the group were listed.
Discharge diagnosis of traveller patients.
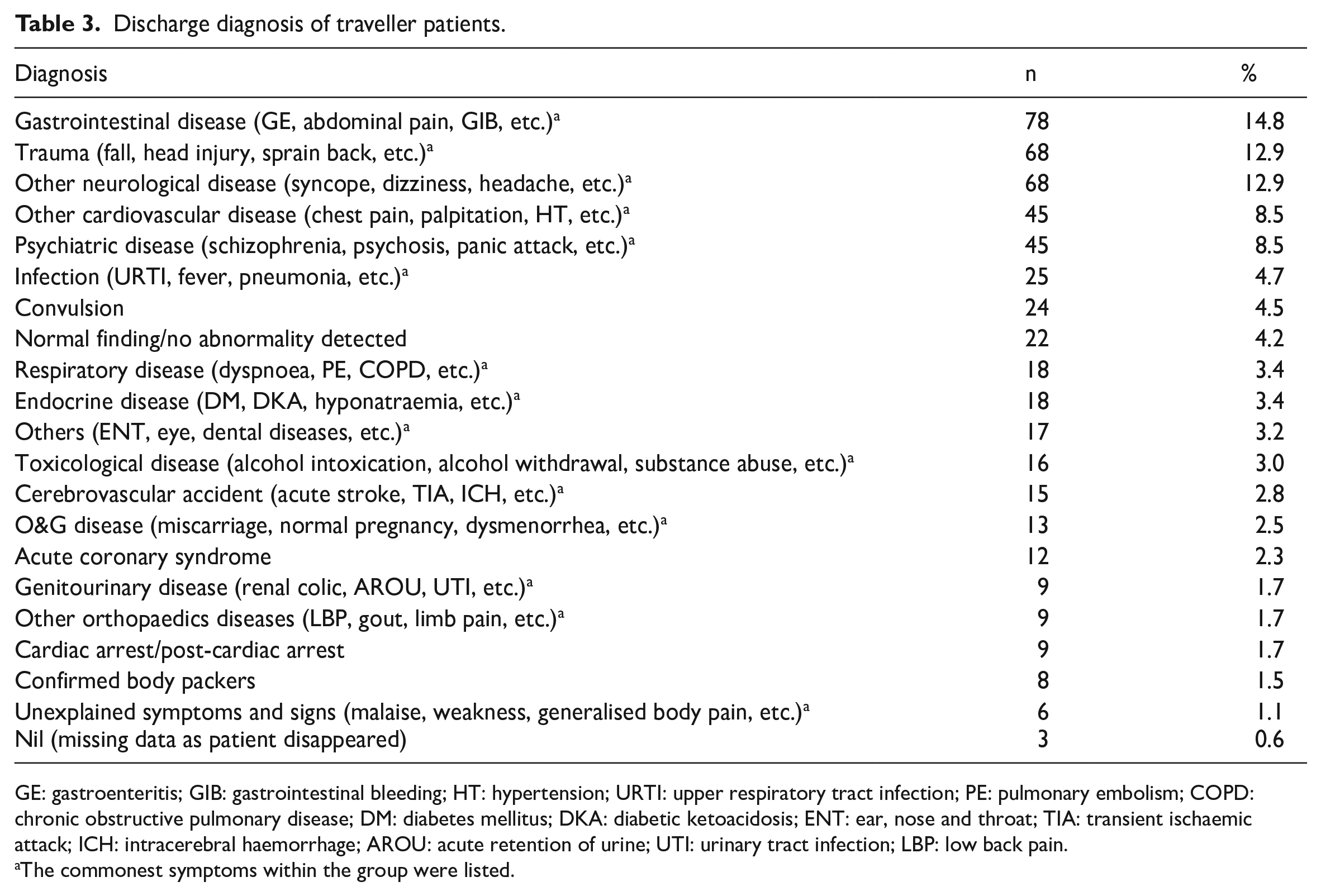
GE: gastroenteritis; GIB: gastrointestinal bleeding; HT: hypertension; URTI: upper respiratory tract infection; PE: pulmonary embolism; COPD: chronic obstructive pulmonary disease; DM: diabetes mellitus; DKA: diabetic ketoacidosis; ENT: ear, nose and throat; TIA: transient ischaemic attack; ICH: intracerebral haemorrhage; AROU: acute retention of urine; UTI: urinary tract infection; LBP: low back pain.
The commonest symptoms within the group were listed.
Most common non-traumatic diagnosis of traveller patients.
A total of 189 (35.8%) were admitted to the hospital from the AED, 327 (61.9%) were discharged from the AED, and 5 (0.9%) disappeared before or after consultation. However, 37 cases (7.0%) required resuscitation in AED, and 7 cases died in the AED. The most common destination for patients requiring admission was PMH (150/189, 79.4%), followed by the EMW of NLTH (19/189, 10.1%). Among all the admitted patients, 56 cases (29.6%) required nurse or doctor escort. In our study, 14.3% (8/56) of traveller patients were Category 1 escort, 85.7% (48/56) were Category 2 escort, whereas 75.0% (42/56) were escorted by nurse, and 25.0% (14/56) were escorted by doctor and nurse. The most common indications for escort were post-intubation (14.3%, 8/56) and convulsion (14.3%, 8/56). The most common indication for cases requiring doctor and nurse escort was again post-intubation (57.1%, 8/14), followed by ST elevation myocardial infarction (21.4%, 3/14). The most common indication for cases requiring nurse escort was convulsion (8/42, 19.0%).
A significant difference was found between the traveller and non-traveller patient groups regarding triage categories, admission rate, rate of resuscitation, rate of escort and rate of death. The percentage of Triage Category 1–2 was higher for traveller patients than non-traveller patients (9.1% vs 1.0%, p < 0.001). The admission rate was higher for traveller patients than non-traveller patients (35.8% vs 14.2%, p < 0.001). The rate of resuscitation was higher for traveller patients than non-traveller patients (7.0% vs 0.2%, p < 0.001). The rate of escort was higher for traveller patients than non-traveller patients (10.6% vs 2.0%, p < 0.001). The rate of death in AED was higher for traveller patients than non-traveller patients (1.3% vs 0.1%, p < 0.001). The proportion of traumatic cases was lower for traveller patients than non-traveller patients but statistically insignificant (13.4% vs 15.4%, p = 0.221; Table 5).
Comparison of traveller and non-traveller patients.
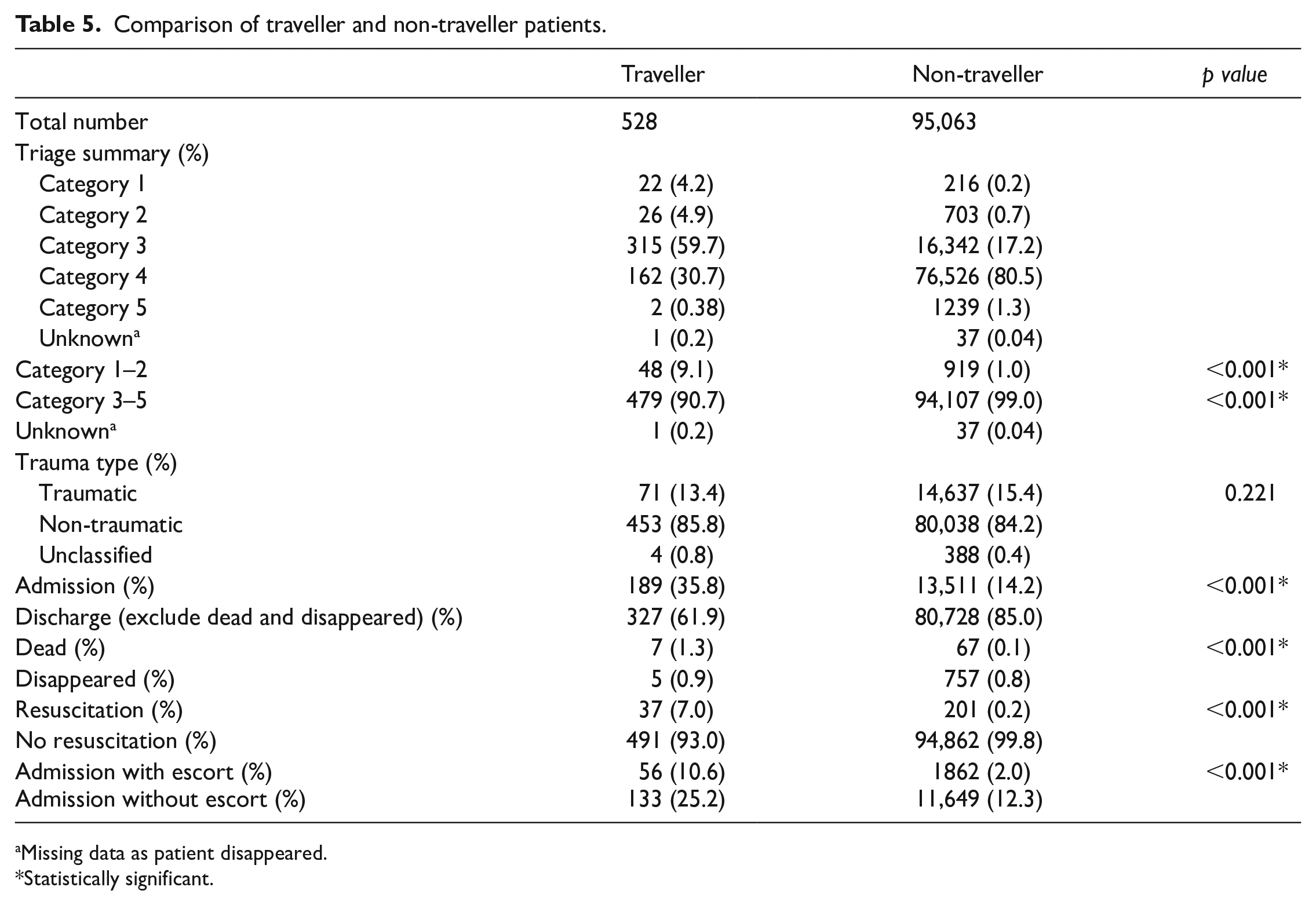
Missing data as patient disappeared.
Statistically significant.
There were seven cases of death in our study. Four were male, and three were female. The age ranged from 0 days to 61 years. All of them presented with out-of-hospital cardiac arrest and had ongoing cardiopulmonary resuscitation (CPR) on arrival to AED. Two were found arrest on flight, and five were found arrest at the airport. Four were witnessed arrest and had bystander CPR performed. Six had resuscitation commenced in AED. Resuscitation was not performed in one case due to the presence of post-mortem changes on arrival. Four had unknown past medical history, and three had chronic medical illnesses. One had a history of venous thrombosis and was found collapse on the plane during long-haul flight, there was shockable rhythm, and defibrillation was given on the plane. The suspected cause of death was pulmonary thrombosis. Another case had a history of late-stage carcinoma of colon (CA colon) and was found collapse in the airport during transit for flight. The suspected cause of death was end-stage CA colon. Another case had a history of heart disease and stroke, presented with chest pain for few days, then found collapse in the airport during transit for flight. There was an episode of pulseless ventricular tachycardia with defibrillation and amiodarone given in AED. The suspected cause of death was acute myocardial infarction. The suspected causes of death for the four remaining cases were unknown. All of them were certified dead in AED and referred to the coroner (Table 6).
Cases of death of traveller patients in AED.
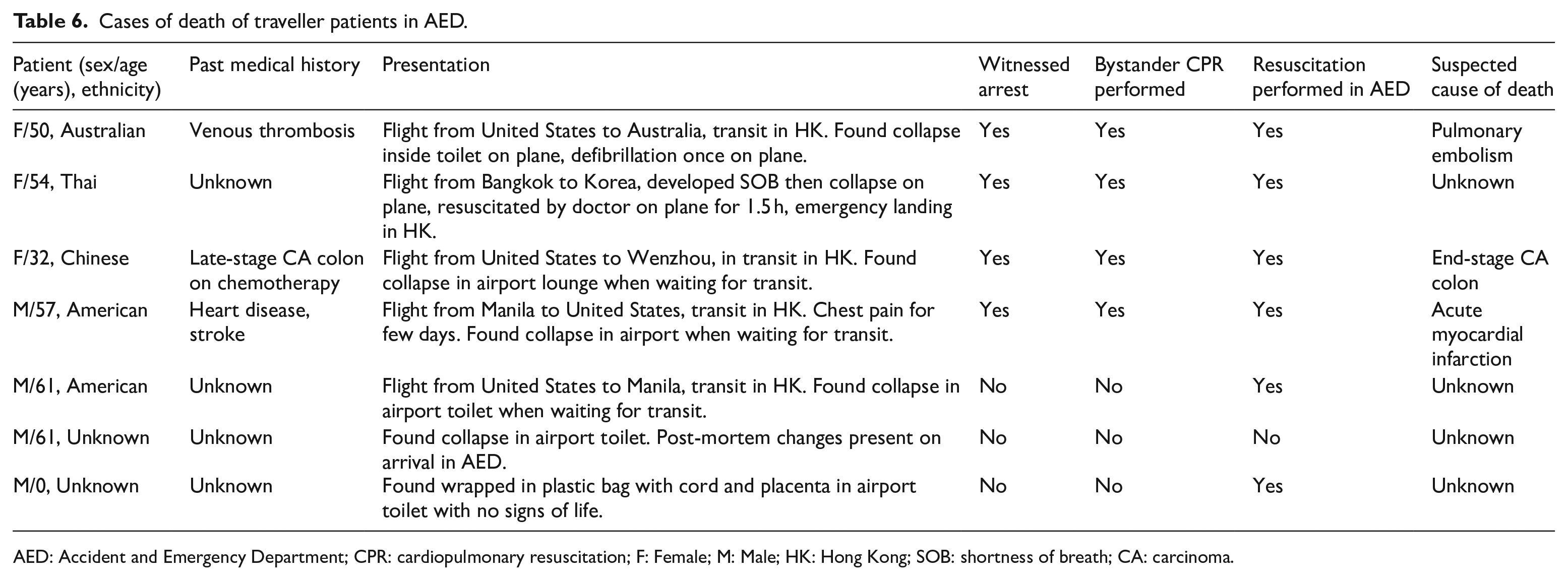
AED: Accident and Emergency Department; CPR: cardiopulmonary resuscitation; F: Female; M: Male; HK: Hong Kong; SOB: shortness of breath; CA: carcinoma.
There were 24 cases of suspected body packers, and 8 (33.3%) were confirmed positive in AED. On presentation, most of them (91.7%, 22/24) were asymptomatic patients brought in by customs officers for examination. Two were symptomatic; one presented with abdominal pain and passed packets on arrival to AED. One presented with collapse and opioid overdose due to leakage of drug packets. The patient was intubated and admitted to Intensive Care Unit, subsequently requiring laparotomy and gastrostomy for the removal of packets. Among the confirmed positive cases, three were confirmed by spontaneous passage of packets before or on arrival to AED, three were confirmed by radiography, and two were confirmed by direct visualisation of packets on proctoscopy. Seven confirmed positive cases were transferred to the custodial ward of QEH, and all of them had packets expelled on discharge. For negative suspects, one had equivocal findings on plain abdominal radiography and required computed tomography scan of abdomen and pelvis, which showed negative for body packing. Others were confirmed negative by physical examination and radiography.
In total, 36 cases presented with emotional or behavioural problems. However, 17 had a history of mental or psychiatric illness. The most common presentations were abnormal, aggressive or disturbing behaviour in the airport or on flight (50.0%, 18/36), unstable emotion (19.4%, 7/36), and anxiety or panic attack (13.9%, 5/36). The most common discharge diagnoses were acute symptoms of schizophrenia (27.8%, 10/36) and acute psychosis (19.4%, 7/36). For disposal, 11 were admitted to the psychiatric ward of KCH by compulsory admission, 9 were admitted to EMW of NLTH, 3 were admitted to PMH and 11 were discharged home. However, 29 required psychiatric consultation in AED or after admission to the EMW. Among cases admitted to NLTH and PMH, 5 were eventually transferred to KCH by compulsory admission after psychiatric consultation. The most common diagnoses for compulsory psychiatric admission were acute symptoms of schizophrenia (50.0%, 8/16) and acute psychosis (37.5%, 6/16).
There were six cases who attended AED for a request of medical certificate for flight. Four had good past health, and two had a history of chronic medical illness. All of them were relatively asymptomatic. Three complained of subjective hotness and worry of fever. One had uncomplicated pregnancy at 34 weeks of gestation. One was under detention by Immigration Department and was required to have verification of usual medication and fitness for flight. One was recently discharged from the hospital for acute stroke and on rehabilitation. All of them had stable vital signs and normal examination findings in AED. Five were discharged with a certificate for fitness for flight, one was admitted for stroke rehabilitation, and no certificate was issued.
Discussion
The results of the analysis of our traveller patient data provide insights into the characteristic of this particular patient population. Only a few studies in the literature reported the epidemiology of traveller patients presenting to the AED. Oktay et al. 8 reported that a significant number of travellers required medical evaluation for traumatic injuries and for new acute medical conditions, such as traveller’s diarrhoea and other infectious diseases, which is similar to our findings. Despite the fact that the number of traveller patients constituted a small proportion of AED attendance, our data support that a significant number of them were actually critically ill and required emergency care support. It was evidenced by the statistically significant higher percentage of Triage Category 1–2 (p < 0.001), higher admission rate (p < 0.001), higher rate of resuscitation (p < 0.001), higher rate of escort in AED (p < 0.001) and higher mortality rate (p < 0.001). Besides the difference in disease severity, there were some other factors which might explain the results. Regarding the admission rate, travellers might require more deliberate care considering the difficulty of re-consultation with the referral or primary hospital by themselves. Due to the language barrier, the responsible staff on triage might tag patients in a higher category, and more escorts were required for translation purposes.
Along with the trend in the worldwide expanding aged population, the number of travellers with advanced age, including those with significant medical or physical impairment, will increase significantly. Moreover, managing traveller patients is often more difficult and time-consuming with obstacles, such as language barriers, unclear medical records, payment issues and problems in arranging follow-ups. Planning on the manpower and resources in AED may be required in high-impact traveller areas as AED is often the first point of contact for traveller patients requiring medical care. Implementing health policies such as introducing additional staff during hot seasons of tourism and designated clinics for travellers in airports will help the AED management. Emergency physicians are expected to face the increasing burden of managing traveller patients with both minor and major medical and traumatic conditions.
Currently, there is a lack of formal training for travel medicine among emergency physicians; further education and training programmes could enhance the knowledge and experience in managing traveller patients by emergency physicians. Resources should be budgeted for emergency training and drills, with priorities given to hospitals in high-impact traveller areas or near borders. Overseas travel medicine courses are not new and are available in many countries, for example, a two-day online course is organised by an international travel medicine organisation yearly. It covers principles of immune response, risk assessment, travel vaccine overview, the care of special groups, emerging infectious diseases, and so on. 9 Another 6-month online certificate course is organised by the Royal College of Physicians and Surgeons of Glasgow in the United Kingdom. It is a more advanced course covering four core modules: Pre-Travel Risk Assessment and Management, Travel-Related Infections, Malaria and Mosquito-Borne Diseases, and Immunology and Immunisations. 10
In addition, emergency physicians are frequently asked to assess the fitness for flight for travellers when they are discharged from the AED. Guidelines for assessment for fitness for flight were published by different aviation organisations and airlines.11-13 The principal factors for consideration of fitness lay in the assessment of physical conditions in the reduction of atmospheric pressure and oxygen tension and challenges in inaccessibility to advanced medical care. Cabin air pressure changes occur after take-off and before landing, leading to gas expansion and contraction, which may cause pain and pressure effects. The aircraft cabin is pressurised to an equivalent of 6000–8000 feet, and oxygen partial pressure is approximately 20% less than on the ground. 14 Healthy passengers tolerate well at these altitudes, but passengers with anaemia, or heart and lung conditions may be at risk and require supplemental oxygen during air travel. Medical kits and cardiac defibrillators are available onboard, but advanced medical care onboard is not possible. While fitness for flight should be decided on a case-by-case basis, as a general rule, patients with unstable medical or mental conditions, including those with an evolving, unpredictable or rapidly changing medical condition should not fly on a commercial aircraft for the sake of patient’s and other passengers’ safety. Of particular concern are cardiovascular disease, thromboembolic disease, anaemia, asthma, chronic obstructive pulmonary disease (COPD), epilepsy, stroke, recent surgery or procedure, recent trauma, diabetes, infectious disease and mental illness. 15 Most aviation guidelines suggest that travel by flight is contraindicated in the following conditions: Infants less than 48 h old, women after the 36th week of pregnancy (32nd week for multiple pregnancies), unstable angina, decompression sickness, increased intracranial pressure, infections of the sinuses, ear or nose, recent myocardial infarction and stroke, recent surgery or injury where trapped air or gas may be present, severe respiratory disease where the patient is breathless at rest, unresolved pneumothorax, sickle cell disease, psychotic illness not fully under control and untreated communicable disease.11-13
Among the traveller patients, suspected body packer constitutes 4.5% and confirmed body packers around 1.5%. Body packing refers to the concealing of illicit drugs in the abdominal or pelvic cavity of the human body. It is a frequently used method for drug trafficking to avert detection at border crossings or airport customs. The commonest illicit drugs encountered are cocaine and heroin. They are usually brought in by customs officers for medical examination but can occasionally present with complications, such as acute intoxication from the rupture of packages, or surgical problems, such as intestinal obstruction. 16 Radiological evaluation by plain abdominal radiography is a commonly adopted approach for screening and diagnosing body packing of illicit drugs. A computed tomography scan is required only if plain abdominal radiography is inconclusive. Failure to detect drug body packing may result in medicolegal consequences. Tsang et al. 17 retrospectively reviewed 269 suspected body packers presenting to the AED of NLTH from 1 January 2015 to 28 February 2017, and found that 69 cases were confirmed body packers radiographically. The majority of them (81%) were cocaine packers. Powder form cocaine (67%) was the most popular drug packed, followed by liquid cocaine (15%). There was a trend of increasing incidence of liquid cocaine packers.
There were several limitations in this study. First, this was a retrospective study, and the data analysis depended on the completeness of the clinical data. The data on primary language, original country, the purpose of travel, occupation, and transit and entry details of traveller patients were not available. The data on sex, age distribution and proportion of patients with underlying diseases in the non-traveller patients were also not available. Future studies with further data analysis on the travel details are warranted to evaluate any confounding factors. Second, only traveller patients coming from the HKIA were included as traveller patients. Due to the limitation in the method of data capture, traveller patients from other borders such as Hong Kong-Zhuhai-Macao Bridge may be counted as non-traveller patients, which may cause bias. Third, some cases had more than one presenting complaint and discharge diagnosis; however, for simplicity of analysis, only the one which is considered the most relevant was counted, which may underestimate concurrent illnesses. Fourth, the study data were captured before the COVID pandemic and the result might not be generalised to the post-COVID era. Finally, this was a single-centre study, as NLTH is a small-scaled hospital with unique admission flow and diversion to different cluster hospitals; the result might not be generalised to other hospitals.
The authors believed that this publication can help emergency physicians better understand the unique healthcare needs of traveller patients, thus better preparedness and more efficient resource allocation in AEDs.
Conclusion
Traveller patients represent a unique patient population in the AED, and managing traveller patients is often challenging for emergency physicians. This study shows that traveller patients have a higher proportion of being critical and emergent and higher demand for emergency care services compared to the non-traveller group. Although the traveller population constitutes a small proportion of the patient population, they can be critical. They can have a significant impact on AED operations, especially for those in high-impact traveller areas. Additional resources, such as on-site translation services, designated clinics for travellers in airports and training programmes in travel medicine, would be beneficial for AEDs, particularly in high-impact traveller areas.
Footnotes
Acknowledgements
The authors thank Mr Lee Wing Chung, Secretary of AED NLTH, for the clerical support of this publication.
Author contributions
L.M.L. and O.F.W. developed the study concept and designed the study. L.M.L. and L.W.N. conducted the study. L.M.L., O.F.W. and S.K. analysed the data. L.M.L. drafted the article. O.F.W., S.K., and Y.N.S. revised the article critically for important intellectual content. All authors read and approved the final article.
Availability of data and materials
All participants’ identifications were removed before storage. The master data set was kept by the investigators in computer and password was required to open the file. Access to the data would be limited to the investigators and clinical research ethics committees of Kowloon West Cluster, Hong Kong Hospital Authority. Please contact principal investigator if further information of the data is required.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was waived by the clinical research ethics committees of Kowloon West Cluster, Hong Kong Hospital Authority.
Ethical approval
This study was approved by the clinical research ethics committees of Kowloon West Cluster, Hong Kong Hospital Authority (KW/EX-22-069(175-08)).