
Abstract
Background:
Ventilator-associated pneumonia is one of the commonest complications encountered in intubated patients: its incidence ranges from 20% to 60%, with higher incidences seen in patients with polytrauma. Ventilator-associated pneumonia can result in poor neurological outcomes upon discharge, longer duration of mechanical ventilation and prolonged intensive care unit stays. The use of systemic antibiotics has been proposed as one method to reduce this complication. However, its effectiveness remains to be determined, and concerns about bacterial resistance hinder its use. This study aims to evaluate the effects of systemic antibiotics on early ventilator-associated pneumonia prevention.
Methods:
This is a single-centred retrospective cohort study, using data in the local trauma registry from 2015 to 2020. Patients aged ⩾18 years who suffered from injury to the head or trunk and were intubated within 12 h of hospitalization were evaluated for early ventilator-associated pneumonia to determine the effectiveness of systemic antibiotics on the incidence of ventilator-associated pneumonia and to identify other risk factors for ventilator-associated pneumonia in patients suffering from trauma.
Result:
A total of 250 patients were recruited; 59 of them met the criteria for early onset ventilator-associated pneumonia. Early use of broad-spectrum antibiotics with potent anaerobic coverage was found to be protective for early onset ventilator-associated pneumonia (adjusted odds ratio = 0.228, p = 0.044). Increasing age and severe thoracic or abdominal injury were also found to be strong non-modifiable predictors for the development of early onset ventilator-associated pneumonia.
Conclusion:
Use of systemic antibiotics with potent anaerobic coverage within 3 h of injury was found to prevent early onset ventilator-associated pneumonia in those intubated within 12 h of injury. However, a large-scale randomized control trial may be needed to further evaluate its benefit and its potential side effects, most notably the risk of antibiotic resistance.
Introduction
Ventilator-associated pneumonia (VAP) is one of the commonest complications encountered in intubated patients. The incidence of VAP ranges from 20% to 60%, with higher incidences seen in patients with polytrauma.1,2 Several mechanisms have been proposed, for example, micro- and macro-aspiration, and brain injury–induced immunosuppression that leaves trauma patients more vulnerable to VAP.1,3 Pneumonia can cause secondary brain injury by affecting intracranial pressure and cerebral perfusion pressure, causing brain hypoxia, resulting in worse Glasgow Coma Scale (GCS) on discharge from intensive care unit (ICU) and longer durations of mechanical ventilation and ICU stay.1,2,4,5 Various preventive measures such as head elevation and minimal sedation have been suggested, but they may not be feasible in many cases and may cause patient discomfort. The use of prophylactic systemic antibiotics as an easier alternative has been proposed.
The 2005 Infectious Diseases Society of America (IDSA)/American Thoracic Society (ATS) guidelines on the management of hospital-associated pneumonia (HAP) stated that Prophylactic administration of systemic antibiotics for 24 hours at the time of emergent intubation has been demonstrated to prevent ICU-acquired HAP in patients with closed head injury in one study, but its routine use is not recommended until more data become available (Level I).
More research has been performed since then and antibiotic prophylaxis has been demonstrated to have a positive effect on preventing early onset VAP in patients with cardiac arrest, stroke, and trauma in many studies. It has also been found to decrease the length of ICU stay.3,6 Although these results seem encouraging, concerns about the development of antibiotics resistant strains still limit the use.
The aim of the study is to investigate the impact of early systemic antibiotics (within 3 h of injury) on early onset VAP in injured patients requiring intubation, and evaluate class effect of antibiotics in the prophylactic use, the impact of choice of antibiotic on the preventive capability of early VAP.
Method
Study setting
This single-centre, retrospective cohort study was performed in a level 1 trauma centre with trauma services that receives all patients with major trauma in New Territories West Cluster (NTWC), a region that encompasses the west part of New Territories and had a catchment population of around 1.15 million in 2019. 7 Major trauma patients will be primarily diverted to Tuen Mun Hospital (the level I trauma centre) unless there is cardiopulmonary arrest, failed airway maintenance or a mass casualty incidents, in which case they will be transferred to the nearest hospital for stabilization before secondary diversion. This study was approved by the NTWC Research Ethics committee (Ref. no.: NTWC/REC/20126).
Our centre adopted the Trauma and Injury Severity Score (TRISS) methodology for evaluating and monitoring of trauma outcome. A standardized trauma registry aligning with the TRISS methodology was kept and maintained by a specialized trauma nurse consultant. The trauma registry includes patient demographics, mechanism of injury, presenting vitals, imaging and laboratory findings, injury severity (Abbreviated Injury Scale (AIC; version 2005 for the year of 2015–2018, version 2015 for the year of 2019–2020), Injury Severity Score, Revised Trauma Score) and outcomes. Patients with trauma who presented to Emergency Department (ED) as critical or serious condition under triage acuity scale, who required trauma team activation, primary trauma diversion or secondary trauma diversion, and trauma cases admitted to the ICU or high dependency unit were recorded in the NTWC trauma registry.
Patient inclusion
Patients were retrieved from the trauma registry to identify all adult patients aged ⩾18 years, who suffered from injury to the head or trunk or both, and were intubated within 12 h of hospitalization. Patients who were pregnant, who died within 48 h of attendance, who were immunocompromised, or who had documented use of antibiotics within 7 days before ED attendance were excluded. Individual patient case notes and electronic patient records were manually reviewed by a single reviewer, who was a medical officer with 5 years of working experience in Accident and Emergency Department, to first determine the presence or absence of VAP and subsequently antibiotic usage (including antibiotic type and timing).
Definitions
VAP was defined as pneumonia that occurred after 2 days of endotracheal intubation. The diagnosis of VAP was established in patients who were intubated within 12 h of admission, with pneumonia defined by either (1) new or progressive infiltrates on chest imaging or (2) growth of microorganisms in sputum, tracheal aspirate or bronchoalveolar lavage with at least one of the following: signs of systemic infection such as hyper- or hypothermia, altered white cell counts or change in sputum characteristics. Early VAP was defined as VAP that occurred between 2 and 7 days after endotracheal intubation. All the chest X-rays and the chart review were performed by a single assessor. Comorbidities including coronary artery disease, congestive heart failure, diabetes, chronic obstructive pulmonary disease and mental illness were retrieved from electronic patient records.
Antibiotics with potent anaerobic coverage included the carbapenems, the combinations of a β-lactam and a β-lactamase inhibitor (amoxicillin/clavulanic acid, and piperacillin/tazobactam) and other antibiotics added on with metronidazole. Other antibiotics that were used (ceftriaxone, cefazolin, vancomycin, cefuroxime and levofloxacin) were defined as antibiotics without potent anaerobic coverage. The type of antibiotics chosen was based on physician decision according to injury pattern.
Statistical analysis
A study published in 2019 suggested that the incidence of early VAP was reduced from 32% to 10% in patients who received antibiotics prophylaxis. 8 Assuming 10% patients were given antibiotics with potent anaerobic coverage, the estimated sample size would be 257 to achieve 90% power at a 0.05 significance as calculated by PASS 2019 Power Analysis and Sample Size Software (2019).
Frequencies and percentages (for proportions) or medians and interquartile ranges (for continuous variables) were presented to describe patient characteristics, mechanism of injury, injury pattern and severity, presenting vitals, outcomes, culture results and antibiotic usage. Mann–Whitney U test and chi-square tests were used to compare the early- and no-VAP groups in univariate analysis. A multivariate logistic regression analysis was applied for confounding control to evaluate whether early (within 3 h) broad-spectrum antibiotics was an independent predictor of early VAP. The covariates included in the model were those with statistical significance at the level of p < 0.3 in univariate analysis and those that are thought to be clinically relevant for the outcome, such as administering antibiotics with anaerobic coverage within 3 h from injury. p-values < 0.05 were considered to be significant in the multivariate model. IBM SPSS Statistics (Released 2019) for Windows, Version 26.0 (IBM Corp.; Armonk, NY, USA) was employed for statistical analyses.
Results
A total of 250 patients fulfilled the inclusion criteria; 59 of these patients met our definition of VAP (Figure 1). Most patients who presented with trauma in our locality did not require intubation within 12 h of presentation.
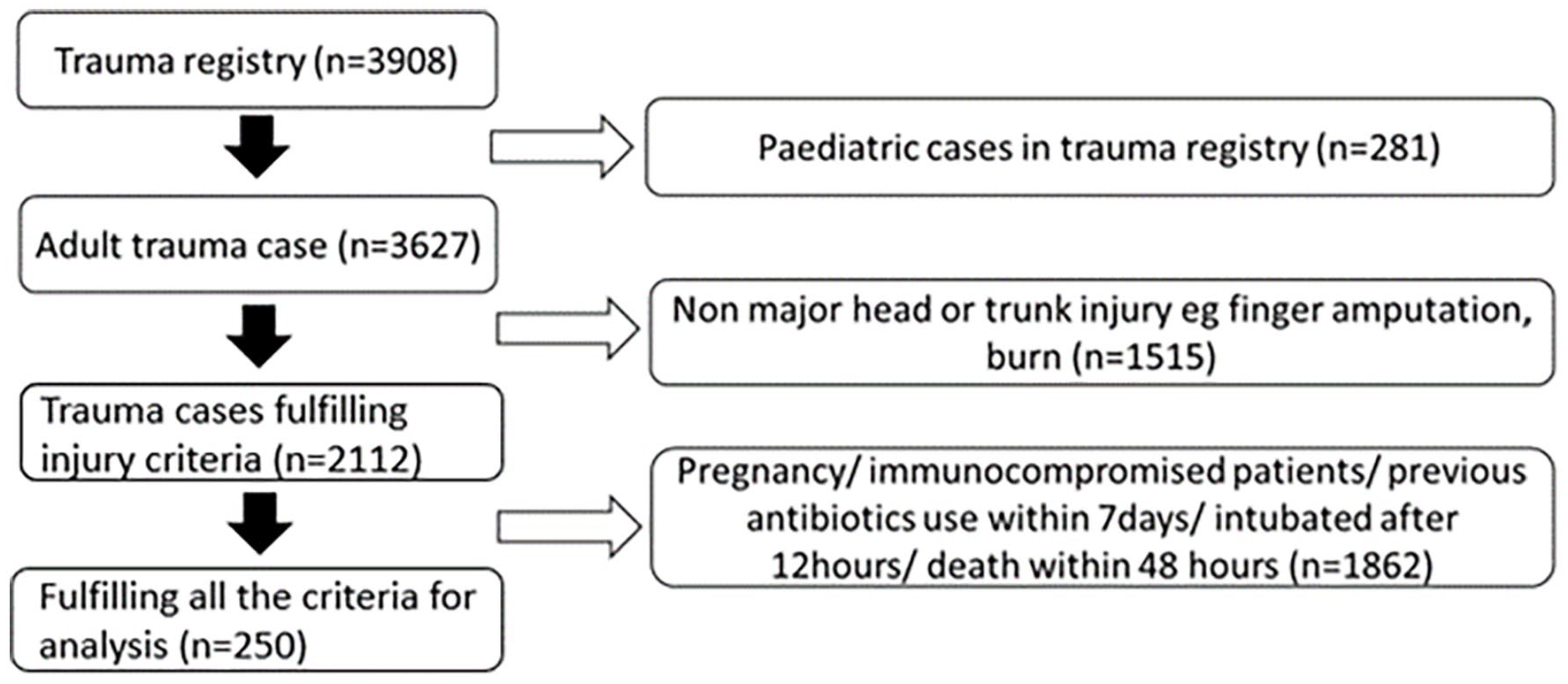
Flow diagram for case selection.
Table 1 shows the study participants demographics, injury pattern, presenting vitals and outcomes. The median age was 52 years, and 78.4% of the patients were male. Patients in both groups had similar demographic background (except for age, 59 vs 50, p = 0.014) and vitals (excepting tachypnoea (RR >20), 52.5% vs 34.6%, p = 0.013). There were significant differences in several aspects of mechanism of injury and injury location: patients with more serious (AIS ⩾3) abdominal or thoracic injury (25.4% vs 8.9%, p < 0.001 and 52.5% vs 22.5%, p < 0.001, respectively) and those with more severe injury (ISS 29 vs 22, p < 0.001) were more likely to develop early VAP. Of note, early use of any antibiotic was not associated with reduced early onset VAP incidence (18.6% vs 22.5%, p = 0.528). Further subgroup analysis of antibiotics with potent anaerobic coverage given within 3 h from injury showed a larger percentage reduction in early onset VAP. However, statistically significance cannot be demonstrated (p = 0.297).
Patient characteristics, injury severity and outcome.
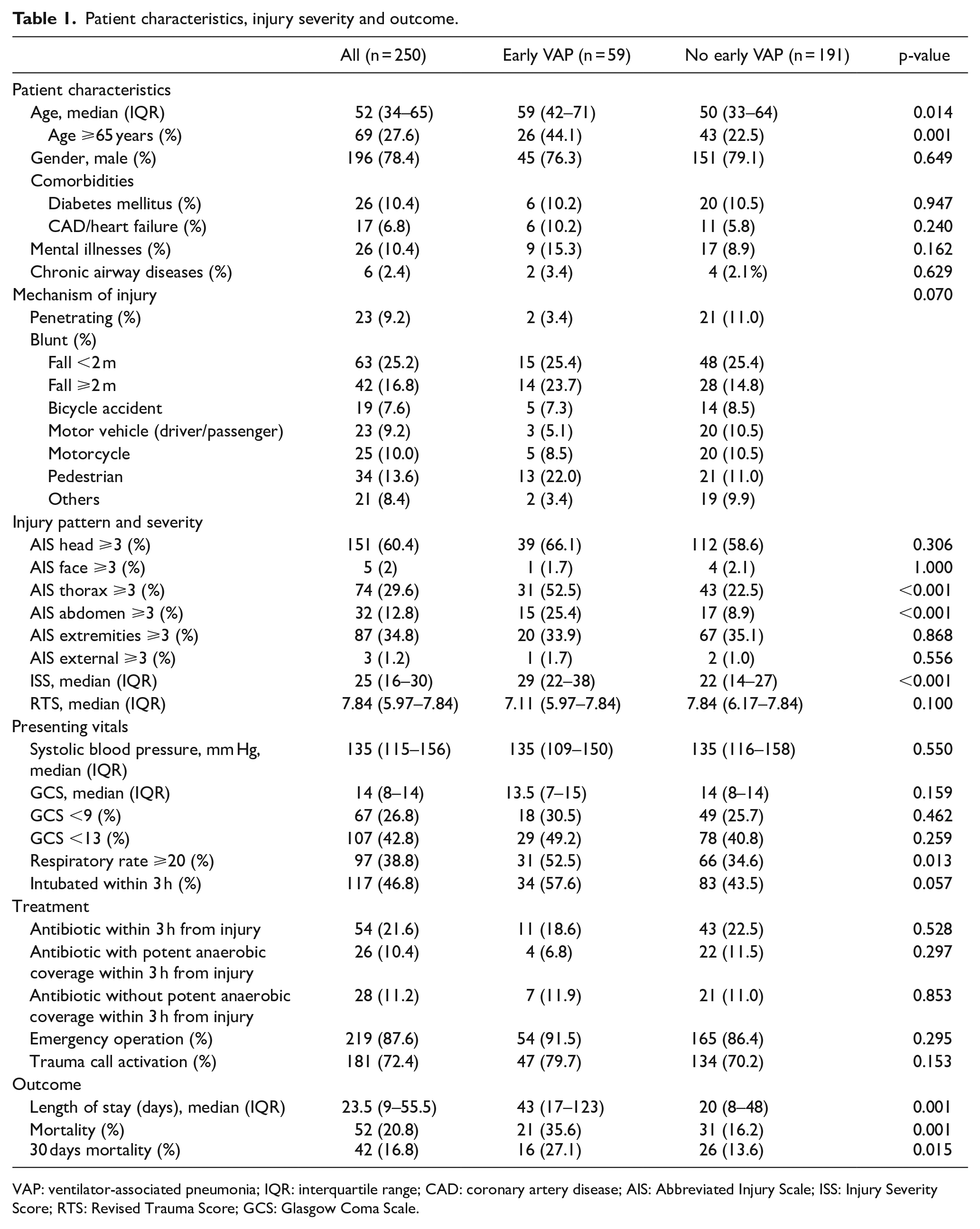
VAP: ventilator-associated pneumonia; IQR: interquartile range; CAD: coronary artery disease; AIS: Abbreviated Injury Scale; ISS: Injury Severity Score; RTS: Revised Trauma Score; GCS: Glasgow Coma Scale.
Table 2 shows the culture results of patients with early onset VAP. Thirty-nine out of 59 (66.1%) of patients had positive culture from respiratory specimens. Enterobacter, Pseudomonas and Klebsiella species were relatively common (28.2%, 25.6% and 25.6%, respectively) among culture positive VAP patients.
Microbiological workup for early VAP cases (cultured in tracheal aspirate/ bronchoalveolar lavage/ sputum within 7 days).
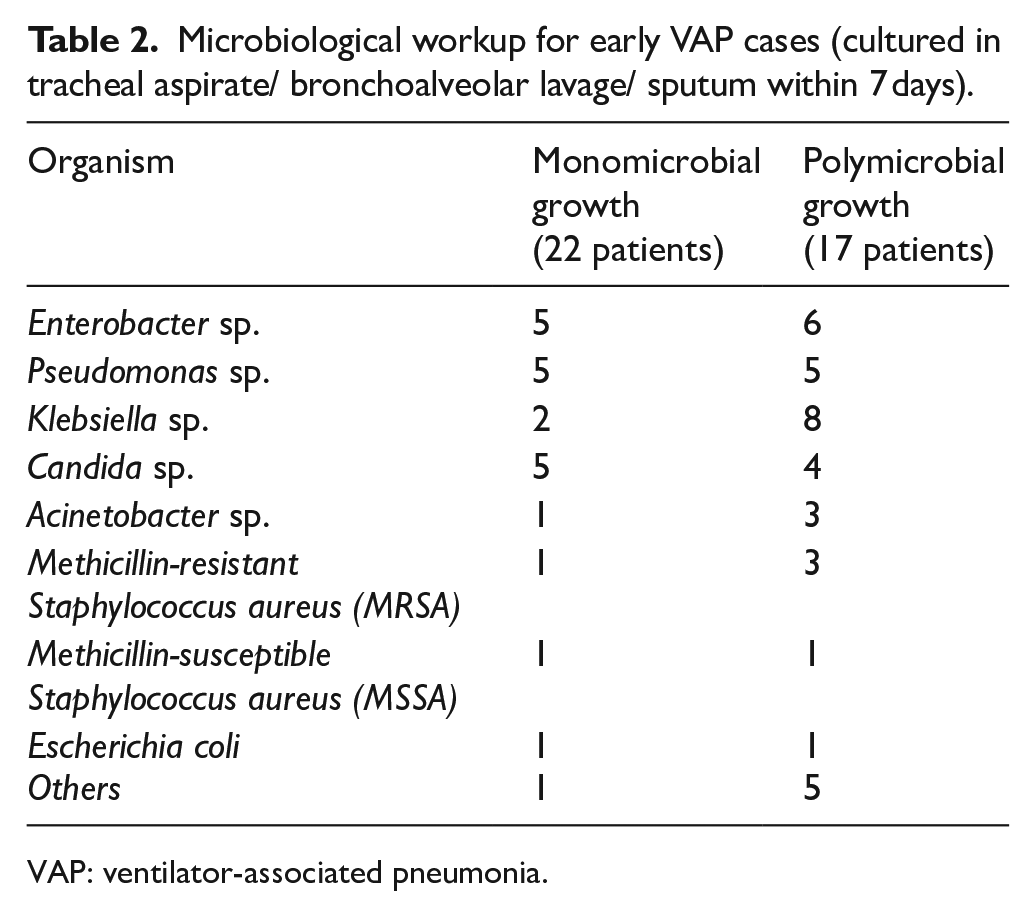
VAP: ventilator-associated pneumonia.
Table 3 shows the specific antibiotics used given within 3 h from injury. Antibiotics with potent anaerobic coverage include amoxicillin/clavulanic acid and piperacillin/tazobactam. Antibiotics without potent anaerobic coverage used included ceftriaxone, cefazolin, cefuroxime, vancomycin and levofloxacin. More commonly used antibiotics was amoxicillin/clavulanic acid and ceftriaxone, which are both targeted towards gram and negative bacteria, while amoxicillin/clavulanic acid with additional anaerobic coverage. However, these two antibiotics lack antipseudomonal coverage.
Specific antibiotics used within 3 h of injury.
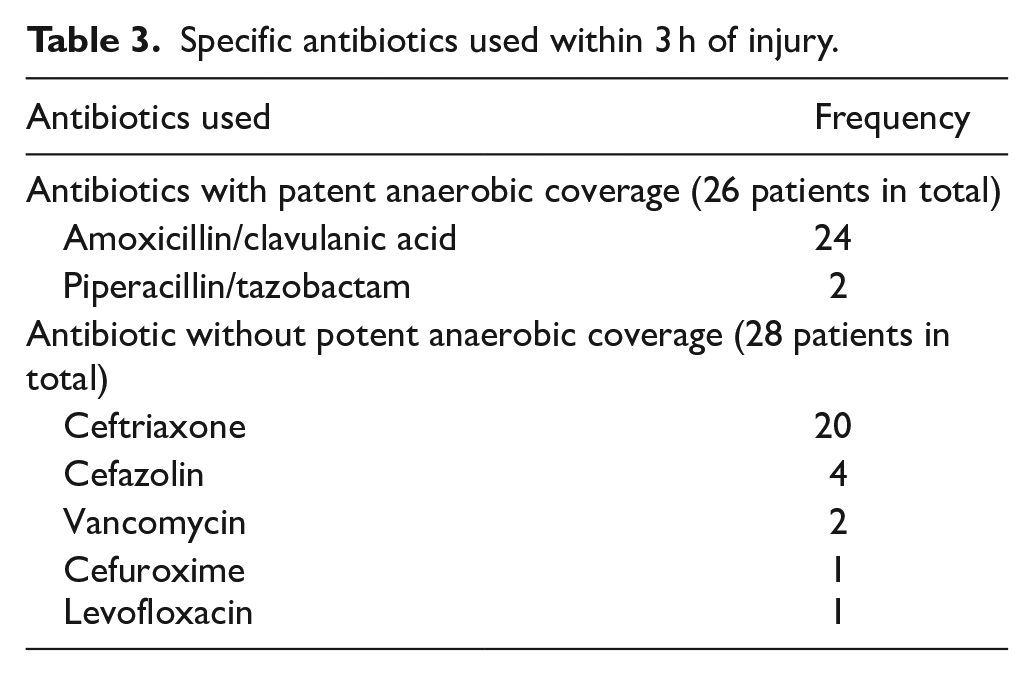
Table 4 shows the demographics, injury pattern, presenting vitals and outcomes of the patients who had early treatment with antibiotics with potent anaerobic coverage and those who did not. The two groups had similar demographics and vitals on presentation, but there were some differences in mechanism of injury, injury pattern and treatment. Patients who received broad-spectrum antibiotics had less severe injury (ISS 16 vs 25, p = 0.009), and more were suffering from severe abdominal injury (26.9% vs 11.2%, p = 0.023). There was no statistical difference between rates of severe thoracic injury (30.8% vs 29.5%, p = 0.89), and more had been intubated within 3 h (73.1% vs 43.8%, p = 0.005).
Antibiotics with potent anaerobic coverage within 3 h from injury compared with no antibiotic with potent anaerobic coverage.
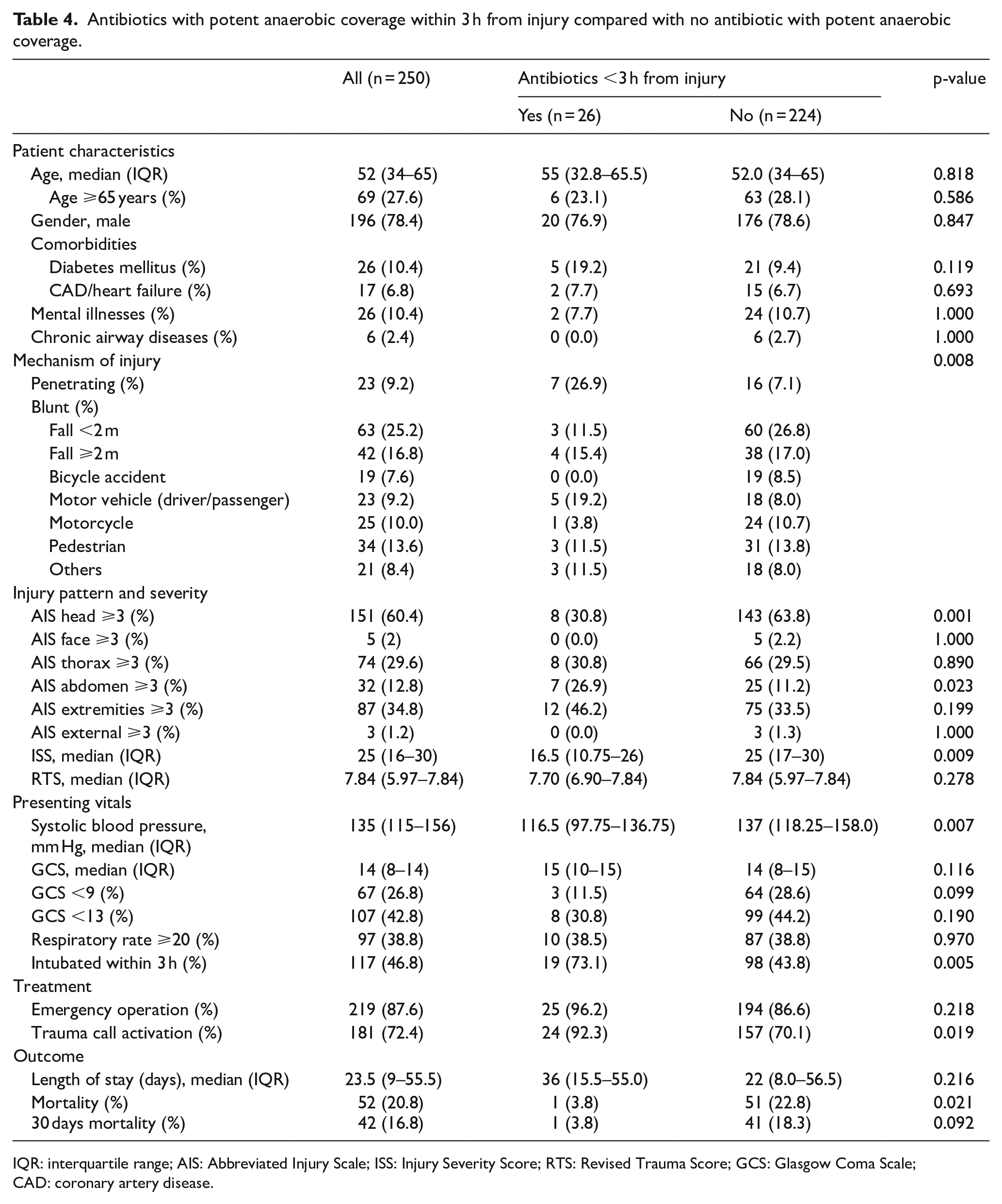
IQR: interquartile range; AIS: Abbreviated Injury Scale; ISS: Injury Severity Score; RTS: Revised Trauma Score; GCS: Glasgow Coma Scale; CAD: coronary artery disease.
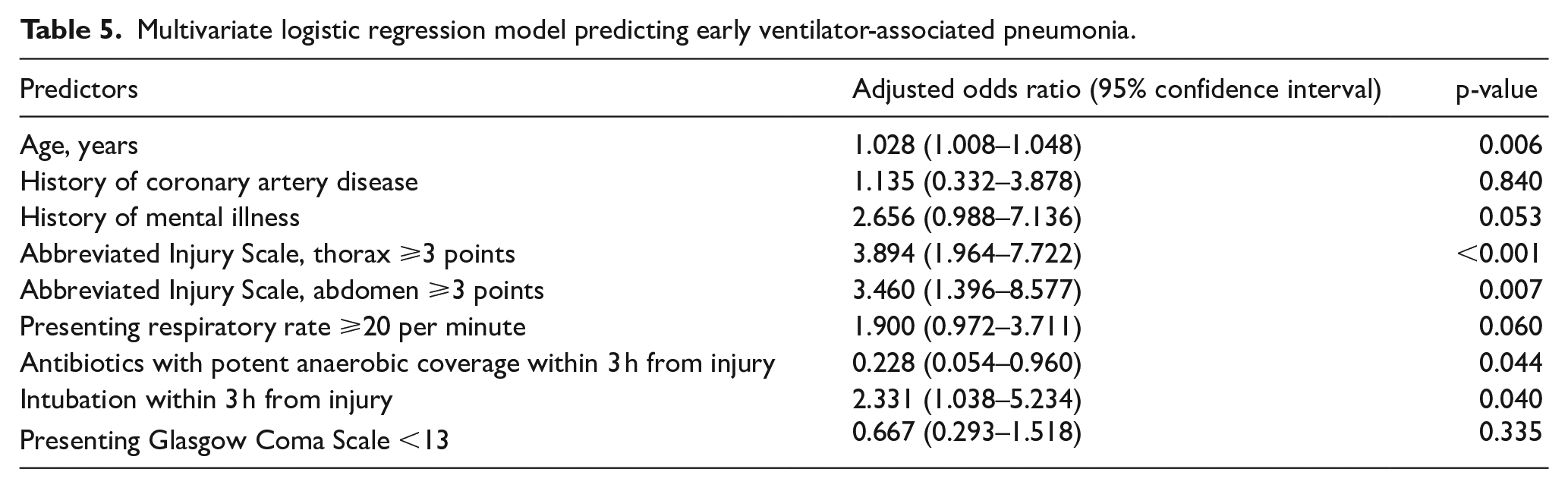
Table 5 shows the results of logistic regression. Age and anatomic injury were found to be strong non-modifiable predictors for the development of early onset VAP. Early intubation was found to be independent predictor of risk of developing VAP, while early use of broad-spectrum antibiotics with potent anaerobic coverage was found to be protective (adjusted odds ratio (OR) = 0.228, p = 0.044). Tachypnoea was not statistically associated with the early VAP after logistic regression (p = 0.060).
Multivariate logistic regression model predicting early ventilator-associated pneumonia.
Discussion
The incidence of early VAP was 23.6% in this study. The rate is relatively low compared to other studies ranging from 22% to as high as 57%. 3 More severe injury including higher ISS and more severe thoracic injury were associated with VAP, a finding also reported by other authors.5,9 Patients with rib fractures, pulmonary contusions and haemothorax are at higher risk of VAP. 10 It is believed that severe brain injury increases the risk of VAP due to aspiration, brain-induced immunosuppression, and neurogenic pulmonary edema.9,11 However, this study did not find an association between VAP and head injury or GCS. This may be due to differences in patient inclusion. Previous studies mainly included intubated patients in the ICU setting. These patients commonly had conditions with much lower GCS such as non-traumatic cardiac arrest, non-traumatic cerebral vascular events and severe traumatic brain injury,6,12 while in this study, which focused on trauma patients, the median presenting GCS was 14, and the indications of intubation in this study included airway protection due to impaired consciousness, respiratory distress or in patients who will proceed to emergency operation. Patients with higher presenting GCS may have lower aspiration risk. The difference in the initial GCS may also cause a relatively low in VAP rate in this study.
In this study, it is demonstrated that the antibiotic choice to use for prophylaxis of early VAP in intubated patients does matter. The prior viewpoint of generalizable class effect of antibiotics for prophylaxis is not substantiated. Broad-spectrum antibiotics with potent anaerobic coverage were demonstrated to be able to prevent early VAP while antibiotics with less potent anaerobic coverage failed to demonstrate a protective effect. This contrasts with the findings presented by Vallés et al., 6 who reported that a single dose of ceftriaxone in comatose patients who were ventilated was useful in preventing early VAP. This may be due to differences in microbiology in the two studies. The more common bacteria found in early VAP in previous studies, including Vallés et al., were Staphylococcus aureus, Streptococcus pneumoniae and Haemophilus influenzae1,13 while multidrug resistance bacteria including, methicillin-resistant Staphylococcus aureus (MRSA), Acinetobacter and Pseudomonas aeruginosa are more commonly found in late onset VAP. 14 However, in this study, Enterobacter, Pseudomonas and Klebsiella species were more commonly seen. Enterobacter and Klebsiella species are known for their abilities to produce extended-spectrum β-lactamases and are shown to have emerging resistance to multiple antimicrobials and may require more potent antibiotics coverage. Whether this difference led to different antibiotic regimens for early VAP prevention is another topic that should undergo further research. This difference in the microbiology is not without reason. One of the reasons is differences in local microbiological patterns. A study that investigated microbiological characteristics of VAP in 2011 15 suggested that Pseudomonas and Klebsiella species were more common in Hong Kong or even in Asia. One study also found out that trauma patients were more likely to have VAP with non-fermentative gram-negative bacilli, such as Acinetobacter and Pseudomonas spp. 13 Another study pointed out that more resistant strains are appearing in early onset VAP in the ICU setting16,17 and the use of microbiology to classify early onset and late onset pneumonia and subsequent treatment based on onset time of pneumonia are now not very useful and may lead to undertreatment. 16 Some advocated this change as prior antibiotic use which reduces those antibiotic susceptible gram-positive cocci and Haemophilus influenzae, but at the same time increases the risk of multidrug-resistant pathogens.1,14,17,18 As some of our patients had been given less potent antibiotics such as cephalosporins, the effects of these antibiotics in reducing some strain of bacteria may lead to an increase in more resistant strain as previous studies demonstrated. This change in microbiology is an important concern as different antibiotics may be needed. Empirical antibiotic treatment of early VAP is suggested based on the risk of multidrug-resistant bacteria, for example, patients who have received antibiotics or have been hospitalized within the past 90 days.16,17,19 –21 Covering of multidrug-resistant bacteria is needed if patients have risk factors.
There is still no widespread consensus about the use of systemic antibiotics in VAP prevention as current studies are of small scale with conflicting results,3,4,8 and there are worries about the emergence of resistance strains. 19 Guidelines about management of hospital-acquired pneumonia and VAP in 2017 suggested selective oral decontamination (with topical non-absorbable antibiotics) and avoiding supplementary intravenous antibiotics (as in selective digestive decontamination strategy) as one of the strategies for VAP preventions. 22 Although the use of systemic antibiotics is not currently recommended, research is still undergoing to determine its role in VAP prevention.
This study has several limitations. The sample size was small, and there was heterogeneity among the patients, including trauma severity and presenting GCS. Subgroup analysis was also limited by the sample size. The limitation of sample size also impacts further evaluation of antibiotic class effects. Further validation and subgroup analysis are required in future research. Another limitation came from the changes in AIS version used in trauma registry. AIS aimed to provide an objective evaluation of injury, and it underwent revision from time to time. However, the change in the AIS version may lead to a different interpretation of injury severity. Although this difference did not affect choice of antibiotics or intubation, it could affect our analysis of injury severity across the groups. Our cohort of patients was generally young and without many comorbidities, which limited our ability to demonstrate the effects of comorbidities on early VAP. And since this study was retrospective in nature, it had problems such as missing data (e.g. private medical records), and no standardized pneumonia prevention bundle or standardized antibiotic regimens. Furthermore, due to incomplete medical records, the neurological and functional outcomes of individual patients were difficult to be assessed, and long-term effects of VAP cannot be demonstrated. A larger, multicentre prospective study may be needed to determine the incidence, risk factors and effect of antibiotics on early VAP.
Conclusion
This study demonstrated that antibiotics with potent anaerobic coverage were useful in preventing early onset VAP when administered within 3 h of injury. However, due to heterogeneity and limited sample size, a further large-scale analysis may be needed to identify risk factors for VAP, and the impact of prophylactic antibiotics on VAP and the emergence of multiresistant bacteria.
Footnotes
Author contributions
C.Y.W. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Availability of data and materials
The data sets generated and analysed during the current study are available from C.Y.W.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was not necessary because no patient data have been included in the manuscript.
Ethical approval
This study was approved by the NTWC Research Ethics Committee (Ref. no.: NTWC/REC/20126) on 21 December 2020.
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.