
Abstract
Background:
The professional quality of life of healthcare professionals in emergency departments may be compromised during the COVID-19 pandemic.
Objectives:
This study aims to examine professional quality of life and resilience as well as their relationships among emergency department healthcare professionals in Hong Kong during the COVID-19 outbreak.
Methods:
This study employed a cross-sectional design. Healthcare professionals (doctors and nurses) working in emergency departments in Hong Kong were recruited via snowball sampling. The Professional Quality of Life Scale, version 5, and the 10-item Connor-Davidson Resilience Scale were used to assess their positive (compassion satisfaction) and negative (secondary traumatic stress and burnout) aspects of professional quality of life and self-reported resilience. Socio-demographics and work-related characteristics were also analysed.
Results:
A total of 106 participants provided valid responses. The results showed an overall moderate level of compassion satisfaction, secondary traumatic stress and burnout among emergency department healthcare professionals. The mean score of the 10-item Connor-Davidson Resilience Scale was 23.8. Backward linear regression analyses revealed self-reported resilience was the only significant predictor of compassion satisfaction (regression coefficient B = 0.875; p < 0.001), secondary traumatic stress (B = −0.294, p < 0.001) and burnout (B = −0.670; p < 0.001), explaining 70.6%, 18.5% and 59.8% of total variance, respectively.
Conclusion:
Emergency department healthcare professionals in Hong Kong experienced an overall moderate level of professional quality of life during the COVID-19 outbreak. Those with a higher level of self-reported resilience had better compassion satisfaction and lower levels of secondary traumatic stress and burnout. The results support the importance of developing interventions that foster resilience among this group of emergency department healthcare professionals to combat COVID-19.
Introduction
The global COVID-19 pandemic has rocked the entire world, especially the healthcare system, in an unprecedented way. Hong Kong is one of the most densely populated cities in the world, and it is no exception to the disruptions brought about by COVID-19. Since the end of January 2020, Hong Kong has experienced several waves of infection. 1 In the first wave, Hong Kong was relatively unaffected. After a much smaller second wave in late May and June 2020, Hong Kong’s COVID-19 cases increased significantly. More than a hundred cases were reported in early August, while this third wave was mainly attributed to imported cases. In November 2020, Hong Kong entered the fourth wave. The main reason behind it was a group of wealthy people who danced together without masks. As of 27 April 2021, 11,740 COVID-19 cases have been recorded, and 209 patients have died of the disease. 1
Given that all patients infected with COVID-19 are treated in public hospitals, the huge demand for medical services during this time is expected to increase the burden on Hong Kong’s already overloaded healthcare system. 2 This situation has also imposed a huge psychological impact on healthcare workers, especially frontline medical and nursing staff in the emergency departments (EDs) because they are the first contact point to treat patients suspected or diagnosed with this potentially fatal infectious disease.3,4 The potential risk of being infected, fear of spreading the disease to family members, uncertainty in the duration of the crisis, lack of effective treatment strategies and potential shortages of personal protective equipment further intensified their psychological burden and compromise their professional quality of life.5,6
Professional quality of life
Professional quality of life refers to emotions an individual encounters in the job of helping others. 7 It is conceptualized as a combination of positive (compassion satisfaction) and negative aspects (secondary traumatic stress and burnout). 7 Compassion satisfaction refers to positive experiences resulting from work that involves helping and caring for others. 7 On the contrary, secondary traumatic stress is defined as a condition in which trauma or stressful events are witnessed but not actually experienced. 7 Burnout refers to the feeling of hopelessness and inefficacy associated with work. 7 Secondary traumatic stress and burnout not only lead to physical (headache and sleep disturbances), emotional (depression, poor concentration) and work-related (avoidance and intention to leave) symptoms but also affect the quality of patient care and pose a threat to patient safety. 8
Frontline healthcare professionals treating patients with COVID-19 were reported to have greater vulnerability to poor professional quality of life than those working with non-COVID-19 patients. 5 By contrast, another study reported lower levels of burnout among frontline workers than those working in usual wards, likely because they have a greater sense of control and more information related to the pandemic. 9 Meanwhile, moderate to high levels of secondary traumatic stress and burnout were found in ED healthcare professionals in Spain 6 and Singapore. 10
Most of the studies examining professional quality of life focused on the role of demographics and work-related factors but yielded mixed findings. Females, young age, low education levels and few years of experiences in ED were previously identified as factors exacerbating secondary traumatic stress and burnout.11,12 Physicians in Spain reported lower compassion satisfaction than nurses; 6 by contrast, nurses in Japan 13 and Singapore 10 reported to experience more burnout than physicians. However, a recent meta-analysis did not identify a significant relationship between professional quality of life and demographic and work-related variables. 14
The complex psychological responses encountered by healthcare professionals directly involved in managing patients with COVID-19 prompt the need for a closer examination of the role of psychological factors, such as resilience, on professional quality of life.
Resilience
Recent studies described resilience as a critical quality that enables healthcare professionals to face challenges during the COVID-19 pandemic. 15 Resilience is a dynamic process of positive adaption despite experiencing stress or adversity. 16 It can be developed through experience, learning and training. 17 Resilient individuals possess personal attributes that enable them to be able to ‘recover’ or ‘rebound’ despite unfavourable conditions. 18 Prior to COVID-19, resilience was found to be a protective factor of burnout in a group of Spanish health personnel, 3 as well as a significant predictor of compassion satisfaction, secondary traumatic stress and burnout in a group of critical care nurses in Saudi Arabia. 19
Although existing studies have examined professional quality of life and their associated factors among healthcare professionals, the professional quality of life among healthcare professionals in EDs in Hong Kong during the COVID-19 pandemic remains poorly known. 20 There is also a dearth of literature pertaining to the role of resilience on professional quality of life. There is an urgent need to identify professional quality of life and resilience, as well as their relationships, among ED healthcare professionals in this critical period.
Objectives
The study objectives were to (1) examine the level of positive (compassion satisfaction) and negative (secondary traumatic stress and burnout) aspects of professional quality of life as well as resilience among healthcare professionals in ED during COVID-19 and (2) examine the relationship between professional quality of life and resilience among healthcare professionals in ED.
Methods
Study design, participants and setting
This was a cross-sectional descriptive correlational study. All full-time medical and nursing staff working in public EDs in Hong Kong were eligible to participate in this study. We limited the study to public ED staff as all COVID-19 patients in Hong Kong were managed in the public sector. There is a total of 17 public EDs in Hong Kong. It was estimated that there are about 900 medical and nursing staff working in public EDs. Due to resource and time constraint, subject recruitment was conducted only in four public hospitals, in which there were around 200 ED medical and nursing staff.
Measures
Professional Quality of Life
The Professional Quality of Life Scale, version 5, 7 which consists of three subscales, was used to assess compassion satisfaction, secondary traumatic stress and burnout. It consists of 30 items in the 5-point Likert-type scale, ranging from (1) never to (5) very often. Each subscale score ranges from 10 to 50. An overall score of 22 or less indicates low levels; a score of 23–41 indicates moderate levels; and a score of 42 or more indicates high levels. 7 The professional quality of life is psychometrically sound and reported to have good internal consistency.7,12 In this study, the Cronbach’s alpha for the overall scale was 0.73, and subscales ranged from 0.80 to 0.96.
Resilience
The 10-item Connor-Davidson resilience scale (CD-RISC-10) was used to assess self-reported resilience of the participants. 21 It captures main features of resilience in the past month. Each item is scored on a 5-point Likert-type scale ranging from 0 ‘never’ to 4 ‘almost always’, with higher scores indicating a higher self-reported resilience. CD-RISC-10 displayed excellent psychometric properties in previous studies.21,22 For this study, the Cronbach’s alpha was 0.96.
Demographics and work-related characteristics
The demographics and work-related characteristics of the participants, such as age, gender, marital status, discipline, years of experience in the profession and in the ED, highest level of educational attainment, any emergency medicine speciality training received, working pattern and intention to leave current position within the next year, were obtained at the beginning of the survey.
Data collection
The data were collected via self-administered online surveys available in both Chinese and English. An online survey portal was created using SurveyMonkey, a secure cloud-based online survey platform. The brief study description, consent forms and questionnaires were included in the online survey portal.
The study was conducted between October 2020 and December 2020, which straddled from the end of third wave to the beginning of the fourth wave of the COVID-19 outbreak in Hong Kong. Participants were invited to participate in the study by means of WhatsApp, a social messaging application, in which a link was distributed to healthcare professionals working in four public EDs in Hong Kong through various ED medical and/or nursing WhatsApp groups. Participants were recruited via snowball; they were also invited to forward the link of the survey to their colleagues. Participants responded to the invitation by clicking a link that directed them to the online survey portal. They were asked to click the ‘yes’ button to indicate their consent to the study and complete an anonymous online survey.
Statistical analysis
IBM SPSS Statistics for Windows version 25.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. The survey responses were downloaded, coded and input into the SPSS. Missing data were handled by listwise deletion. Descriptive statistics, such as mean and standard deviation for continuous variables and proportions for categorical variables, were used to summarize professional quality of life and resilience measure, as well as participants’ demographics and work-related characteristics. Pearson’s correlations or Spearman’s rho as appropriate were performed to examine statistical associations between study outcomes. Bivariate analyses by means of independent t-test and one-way analysis of variance (ANOVA) were used to examine the association between professional quality of life, self-reported resilience as well as participants’ characteristics. Those factors showing significance (p < 0.25) in bivariate analyses were selected as candidate variables for backward multivariable linear regression analysis to delineate factors significantly associated with professional quality of life. The statistical significance level was set at p < 0.05 (two-sided).
Ethical considerations
Ethical approval was obtained from the Joint CUHK-NTEC Clinical Research Ethics Committee prior to commencement of the study (CREC ref. no.: 2020.393). All study procedures involving human participants were handled in accordance with the Helsinki Declaration. Online consent was obtained from each participant prior to completing the study survey.
Results
Participants’ characteristics
Of the 200 eligible participants approached, a total of 126 attempted the survey. The response rate was around 63%. After excluding 20 participants who missed multiple items in the psychometric scales and/or demographic and work-related characteristics, the final sample included 106 participants who have completed all items in the survey. The participants were aged between 23 and 61 years old (median = 33.5, interquartile range (IQR) = 28–43), and 60.4% of them were female. About half of them were nurses (56.6%), married (49.1%) and received postgraduate training in emergency medicine (49.1%). The median years of professional and ED experience were 9 (IQR = 4–20) and 6 (IQR = 2–13), respectively. The majority had attained a bachelor or higher education level (85.9%), a shift working pattern (76.4%) and no intention to leave current position next year (81.1%). A summary of the participants’ demographics and work-related characteristics is shown in Table 1.
Participants’ demographics and work-related characteristics (N = 106).
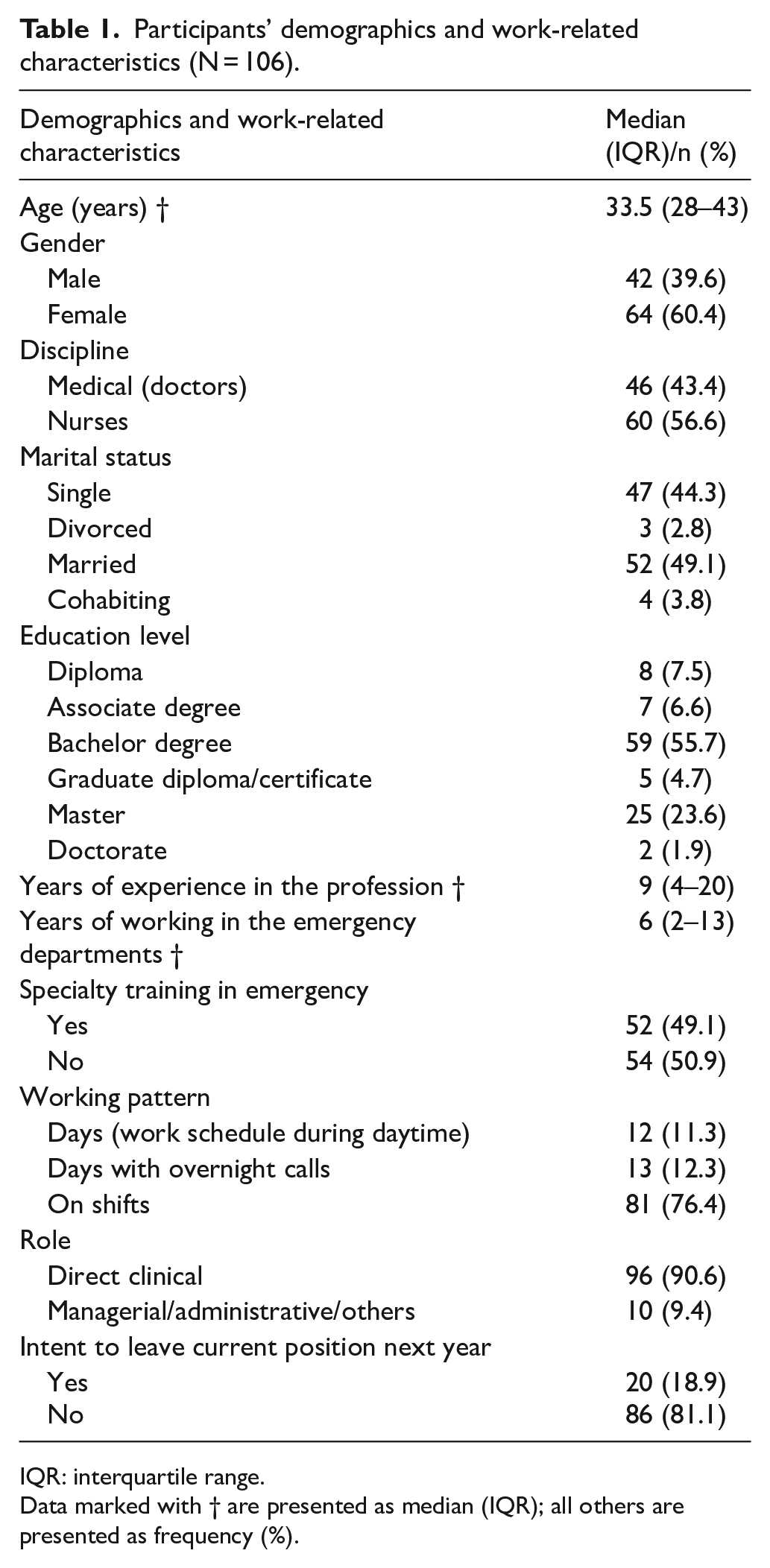
IQR: interquartile range.
Data marked with † are presented as median (IQR); all others are presented as frequency (%).
Professional quality of life
The mean scores for compassion satisfaction, secondary traumatic stress and burnout were 34.7 (SD = 8.2), 24.7 (SD = 6.8) and 25.7 (SD = 7.1), respectively (Table 2). Furthermore, 72.6% (n = 77), 56.6% (n = 60) and 66.0% (n = 70) of the participants fell into the moderate levels (23–41) of compassion satisfaction, secondary traumatic stress and burnout, respectively. Nearly 5% of participants reported a high level of secondary traumatic stress and burnout.
Professional quality of life and self-reported resilience (N = 106).
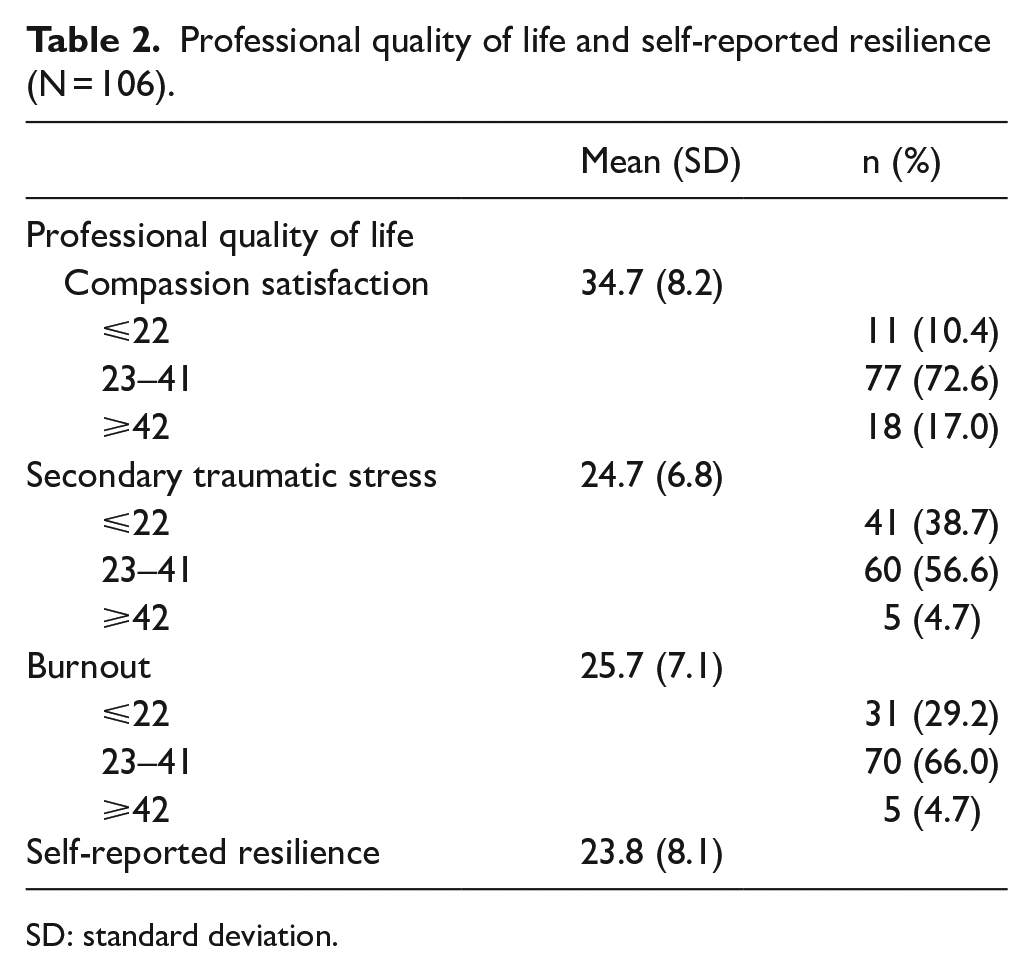
SD: standard deviation.
Self-reported resilience
The total scores in CD-RISC-10 ranged from 10.0 to 39.0, with a mean score of 23.8 (SD = 8.1) (Table 2).
Correlations between professional quality of life and self-reported resilience
Significant correlations were found between the positive and negative aspects of professional quality of life (Table 3). Compassion satisfaction has a negative correlation with secondary traumatic stress (r = −0.282, p < 0.01) and burnout (r = −0.808, p < 0.01), whereas secondary traumatic stress has medium and positive correlation with burnout (r = 0.631, p < 0.01).
Correlations between the professional quality of life and self-reported resilience.
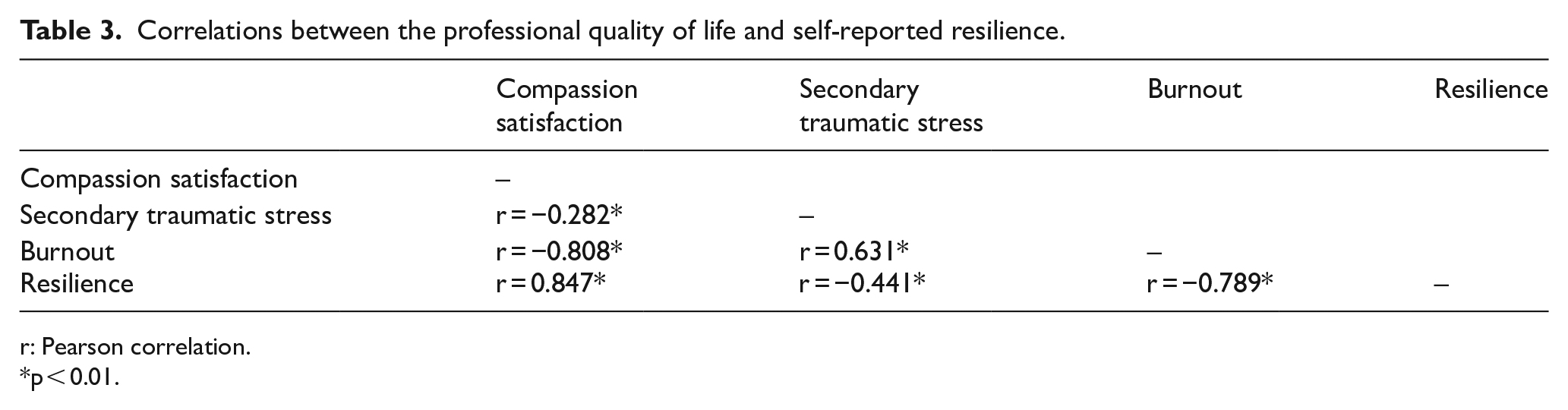
r: Pearson correlation.
p < 0.01.
Self-reported resilience was significantly correlated with all aspects of professional quality of life (p < 0.01). It has a strong, positive correlation with compassion satisfaction (r = 0.847) but negative correlation with secondary traumatic stress (r = −0.441) and burnout (r = −0.789).
Univariate analyses of the factors associated with professional quality of life
Independent sample t-tests and ANOVA revealed that female gender and nurses showed higher secondary traumatic stress and burnout (p < 0.05). The burnout scores differed significantly among participants with different years of experience in the profession (p = 0.025). Post hoc analysis using Turkey HSD showed that those with less than 5 years of experience in the profession reported significantly higher burnout than those with more than 15 years of experience (p = 0.031). Healthcare professionals who had received postgraduate training in emergency medicine and reported no intention to leave current position were found to be associated with higher scores of compassion satisfaction and lower scores in secondary traumatic stress and burnout (all p < 0.05). Those with non-shift work pattern were associated with higher compassion satisfaction and lower burnout (p < 0.05). Table 4 shows the association between compassion satisfaction, secondary traumatic stress, burnout with demographics and work-related characteristics.
Univariate associations of demographics and work-related characteristics on compassion satisfaction, secondary traumatic stress and burnout.
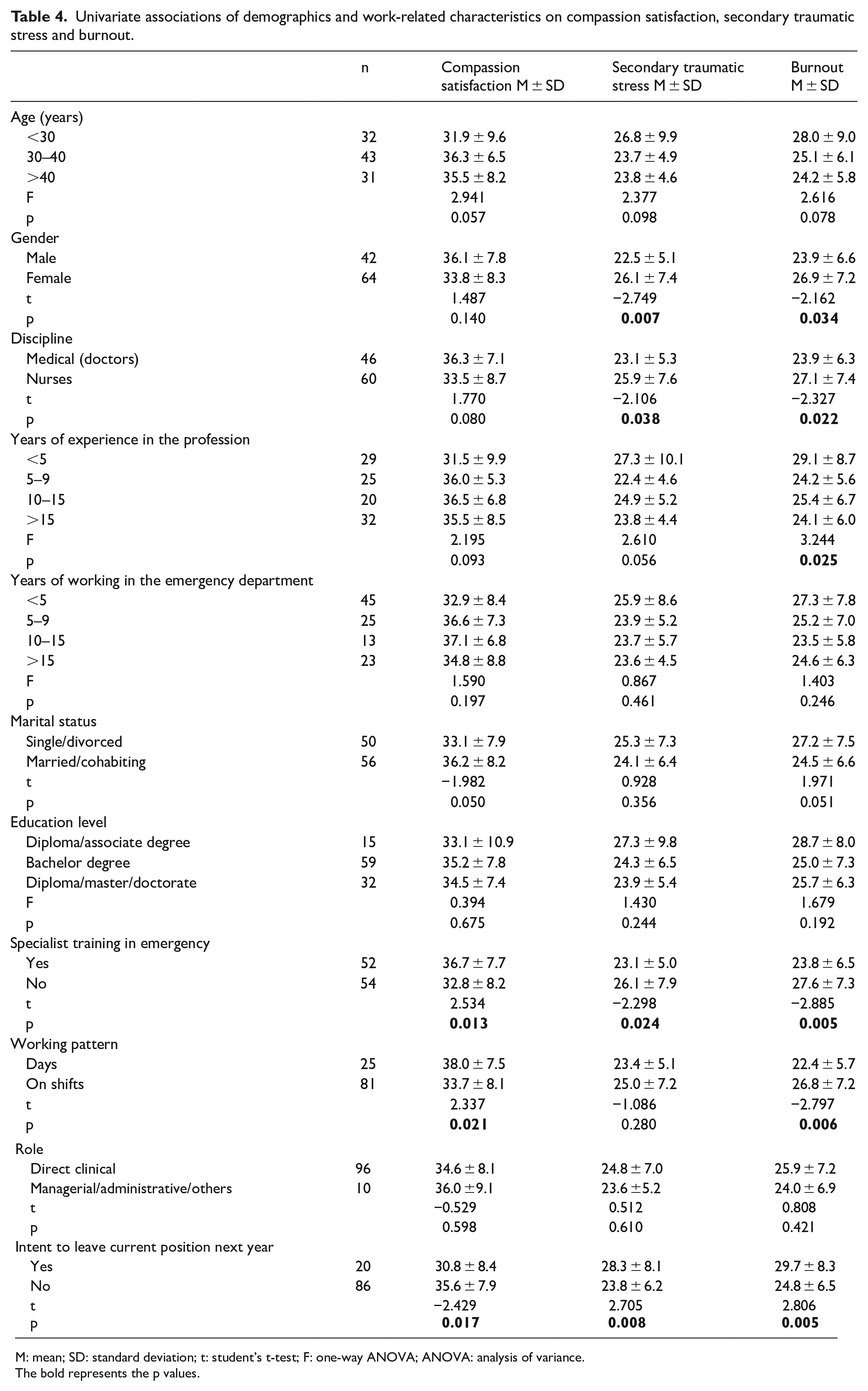
M: mean; SD: standard deviation; t: student’s t-test; F: one-way ANOVA; ANOVA: analysis of variance.
The bold represents the p values.
Predictors of professional quality of life
The factors listed in Table 4 were assessed for associations with professional quality-of-life outcomes. Backward multivariable linear regression analysis using those factors with p < 0.25 in univariate analyses as candidate variables revealed that self-reported resilience (regression coefficient B = 0.875; p < 0.001) was the only factor significantly and independently associated with compassion satisfaction and explained 70.6% of the variance. In addition, self-reported resilience (regression coefficient B = −0.294; p < 0.001; regression coefficient B = −0.670; p < 0.001) was a negative factor of secondary traumatic stress and burnout, explaining 18.5% and 59.8% of the variance, respectively. Table 5 shows the results of the backward regression analyses.
Regression analyses of demographics and work-related characteristics and self-reported resilience associated with compassion satisfaction, secondary traumatic stress and burnout.
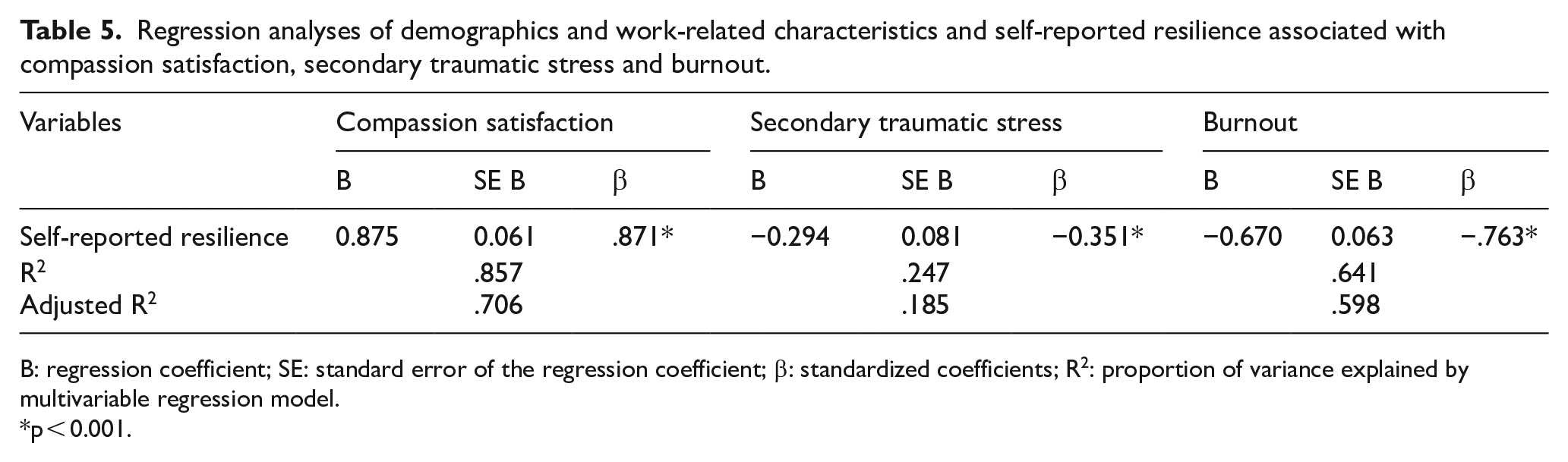
B: regression coefficient; SE: standard error of the regression coefficient; β: standardized coefficients; R2: proportion of variance explained by multivariable regression model.
p < 0.001.
Discussion
To the best of our knowledge, this is the first study which examined professional quality of life and resilience in ED healthcare professionals in Hong Kong during the COVID-19 outbreak. Although this study was conducted in Hong Kong, healthcare professionals in EDs around the world are one of the major groups affected by the pandemic.6,10 Therefore, the findings of this study may be a useful reference for international audiences.
Overall, the study participants reported moderate levels of compassion satisfaction, secondary traumatic stress and burnout. Of note, around 5% experienced a high level of compassion fatigue. Similar results were reported in healthcare professionals working in EDs in Spain 6 and Italy. 11 Prior to the COVID-19 pandemic, the fast-paced environment of an ED, the pressure caused by overnight shifts and the stress triggered by emergency cases already contributed to their reduced capacity to be compassionate in the workplace. 12 Compounded with being in the frontline with direct contact to patients who are suspected or confirmed to have COVID-19, the fear of contracting and spreading the virus to their families and witnessing the poor and deteriorating conditions of the patients, were factors that further contributed to the low compassion satisfaction and high levels of secondary traumatic stress and burnout among ED healthcare professionals in Hong Kong. 4 However, the overall professional quality of life of our sample were higher than that of Italian healthcare professionals directly involved in caring the COVID-19 patients. 5 The difference may be explained by two reasons. First is that the prevalence of COVID-19 and mortality rate in Hong Kong was very low compared to that of Italy. The second is that healthcare professionals in Hong Kong already had experiences in combating the severe acute respiratory syndrome epidemic in 2003. Nevertheless, our findings still highlight a pressing need for efforts to improve the professional quality of life among healthcare workers in ED during this critical period.
Our results showed there were significant correlations between compassion satisfaction, burnout and secondary traumatic stress among ED healthcare professionals in Hong Kong. Specifically, higher compassion satisfaction was associated with less burnout and secondary traumatic stress, implying that compassion satisfaction might be a protective factor for poor psychological health among ED healthcare professionals. Similar findings were observed in studies on healthcare professionals working in various settings using the same scale.6,14 By contrast, an earlier study on Australian emergency nurses did not find any significant associations among the three aspects of professional quality of life. 23 Further studies are needed to better understand the relationship between the positive and negative aspects of professional quality of life among ED healthcare professionals.
In this study, we identified a number of demographic and work-related factors that were associated with negative aspects of professional quality of life. Participants who were female, nurses, with less than 5 years of experiences, with no specialty training in emergency medicine, who work on shifts and who intended to leave their current position next year were reported to experience higher levels of secondary traumatic stress and/or burnout than their counterparts. Nurses in Hong Kong may similarly perceive a lesser sense of personal success on treating COVID-19 patients and a lower sense of control than doctors;11,13 junior healthcare professionals with limited experience may have poor coping strategies. Likewise, a recent meta-analysis including 21 studies suggested that education and training may have a moderating effect on secondary traumatic stress and burnout. 24
Nevertheless, the aforementioned factors were either excluded or became insignificant in the multivariable models after considering the effect of resilience, indicating that resilience was a salient predictor of both positive and negative aspects of professional quality of life among this group of ED healthcare professionals. Prior to the COVID-19 pandemic, resilience had been reported to partially mediate the relationship between trait-negative affect and compassion satisfaction among a large sample Australian nurses from public, private and aged care sectors, 25 and to be a univariate predictor of compassion satisfaction, secondary traumatic stress and burnout among a sample of Saudi Arabian critical care nurses. 19 Resilience has also been identified as an independent predictor of secondary traumatic stress among medical staff and emergency workers during the first phase of the COVID-19 pandemic. 26 Our study is in line with existing literature and provides evidence that supports resilience as a strong positive predictor of compassion satisfaction and a strong negative predictor of burnout among healthcare professionals in ED during the COVID-19 pandemic. Fostering resilience in ED healthcare professionals was recently set as a high priority to prepare them to deal with the challenging and evolving conditions of COVID-19. 27 These findings call for concerted efforts to foster resilience among ED healthcare professionals in Hong Kong.
Implications
The results of this study offer insights into the regular assessment of professional quality of life and support the importance of developing tailored interventions to optimize resilience among ED health care professionals during the climax of COVID-19. For instance, resilience is considered an essential quality in healthcare professionals that can be learnt and improved, 19 and previous studies provided evidence on the effects of educational programmes on improving professional quality of life 28 and the mindful self-compassion training programme 29 or resilience-training programme 30 on the improvements of resilience. Therefore, the development of an educational programme that incorporates strategies to foster resilience among ED healthcare professionals is warranted. Such a programme is also imperative for them to manage future pandemics.
Limitations
There are several limitations in this study. First, due to the cross-sectional study design, the causality between professional quality of life and self-reported resilience could not be determined. Future interventional studies examining the effects of resilience on professional quality of life should be considered. Second, similar to other studies, this study did not allow for comparison to pre-pandemic data or the following of developments during the pandemic, as it only measured the study outcomes at a single time point. Longitudinal studies are needed to understand the trajectories of professional quality of life and resilience of ED healthcare professionals in the pandemic and beyond. Third, the small sample size with a moderate dropout rate and lack of random sampling might lead to selection bias and limit the generalizability. Fourth, the relatively small sample size may have limited power due to the problem of multiple comparisons; therefore, the regression analysis used to examine factors associated with professional quality of life should be viewed as exploratory. Finally, the self-reporting nature of surveys likely lead to bias as those with high levels of burnout or low compassion satisfaction are less likely to respond to the survey.
Conclusion
ED healthcare professionals in Hong Kong experienced overall moderate levels of both positive and negative aspects of professional quality of life during the COVID-19 outbreak. Those with a higher level of self-reported resilience had a higher level of compassion satisfaction and lower levels of secondary traumatic stress and burnout than their counterparts. The results highlight the importance of supporting ED healthcare professionals during the COVID-19 pandemic and support the importance of developing interventions to foster resilience among this group of ED healthcare professionals to combat COVID-19.
Footnotes
Acknowledgements
The authors would like to thank all the participants in the study.
Author contributions
C.L.W. and J.L.T. researched literature and conceived the study. C.L.W. was involved in gaining ethical approval. C.L.W., J.L.T., B.Y. and B.S.C.L. were involved in data collection. C.L.W. and A.W.Y.L. analysed the data and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
The anonymous data which form the basis for this study are available from the authors on reasonable request.
Informed consent
Online consent was obtained from each participant prior to completing the study survey.
Ethical approval and human rights
Ethical approval was obtained from the Joint CUHK-NTEC Clinical Research Ethics Committee prior to commencement of the study (CREC ref. no.: 2020.393). All study procedures involving human participants were handled in accordance with the Helsinki Declaration.