
Abstract
We recently read an interesting study which demonstrated that self-inflating resuscitation bag (SIRB) lacking expiratory valve has unreliable performance in oxygen delivery during spontaneous breathing mimicked by mechanical lung simulator. It was postulated that the absence of an expiratory valve and the resulting air entrainment via the exhaust port accounts for the poor oxygen delivery performance. The current disposable SIRB in-use in our institutions (Med-Rescuer Disposable BVM Resuscitator 4000, BLS Systems Limited, ON, Canada) has a duckbill valve but no expiratory valve. Safety concerns regarding its oxygen delivery performance during spontaneous breathing were raised, as this SIRB was commonly used to preoxygenate critically ill patient with potentially transmissible respiratory infection (e.g. COVID-19) before tracheal intubation. We therefore performed an experiment on this SIRB using one of us as a healthy volunteer. Our small experiment demonstrated that air entrainment could occur via the exhaust port and affect oxygen delivery performance. Our experiment also demonstrated that attaching a positive end-expiratory pressure (PEEP) valve to the exhaust port improves the oxygen delivery performance. The findings of this experiment were sent to the relevant department of our institutions for safety consideration.
We recently read an interesting study by Grauman et al. 1 which demonstrated that self-inflating resuscitation bag (SIRB) lacking expiratory valve has unreliable performance in oxygen delivery during spontaneous breathing mimicked by mechanical lung simulator. It was postulated that the absence of an expiratory valve and the resulting air entrainment via the exhaust port accounts for the poor oxygen delivery performance. The current disposable SIRB in-use in our institutions (Med-Rescuer Disposable BVM Resuscitator 4000, BLS Systems Limited, ON, Canada) (Figure 1) has a duckbill valve but no expiratory valve. Safety concerns regarding its oxygen delivery performance during spontaneous breathing were raised, as this SIRB was commonly used to preoxygenate critically ill patient with potentially transmissible respiratory infection (e.g. COVID-19) before tracheal intubation.

The disposable self-inflating resuscitation bag under testing.
We therefore performed an experiment on this SIRB using one of us as a healthy volunteer. The oxygen inlet of this SIRB was connected to 16 L/min oxygen throughout the experiment. A filter (Ultipor, Pall Medical, Fribourg, Switzerland) was attached between the facemask and the SIRB. Gas was sampled from the sampling port of the filter and oxygen content was analysed by the built-in analyser of an anaesthetic machine (Zeus Infinity Empowered, Dräger AG & CO., Lubeck, Germany). With this setup, the following scenarios were tested in sequence consecutively without rest in-between: The volunteer was first instructed to perform tidal breathing on 16 L/min oxygen flow via the SIRB. He was then instructed to breathe ‘deep and fast’ (to mimic respiratory distress) on the same flow. The fractional inspired oxygen concentration (FiO2) delivered in each scenario was measured. We found that FiO2 dropped significantly when respiratory distress was mimicked (Figure 2). This is likely because in spontaneous inspiration, the final inspired gas is composed of oxygen from the self-inflating bag and entrained room air (Figure 3). Air entrainment is expected to increase when peak inspiratory flow rate (PIFR) is high such as in patients with respiratory distress. 2
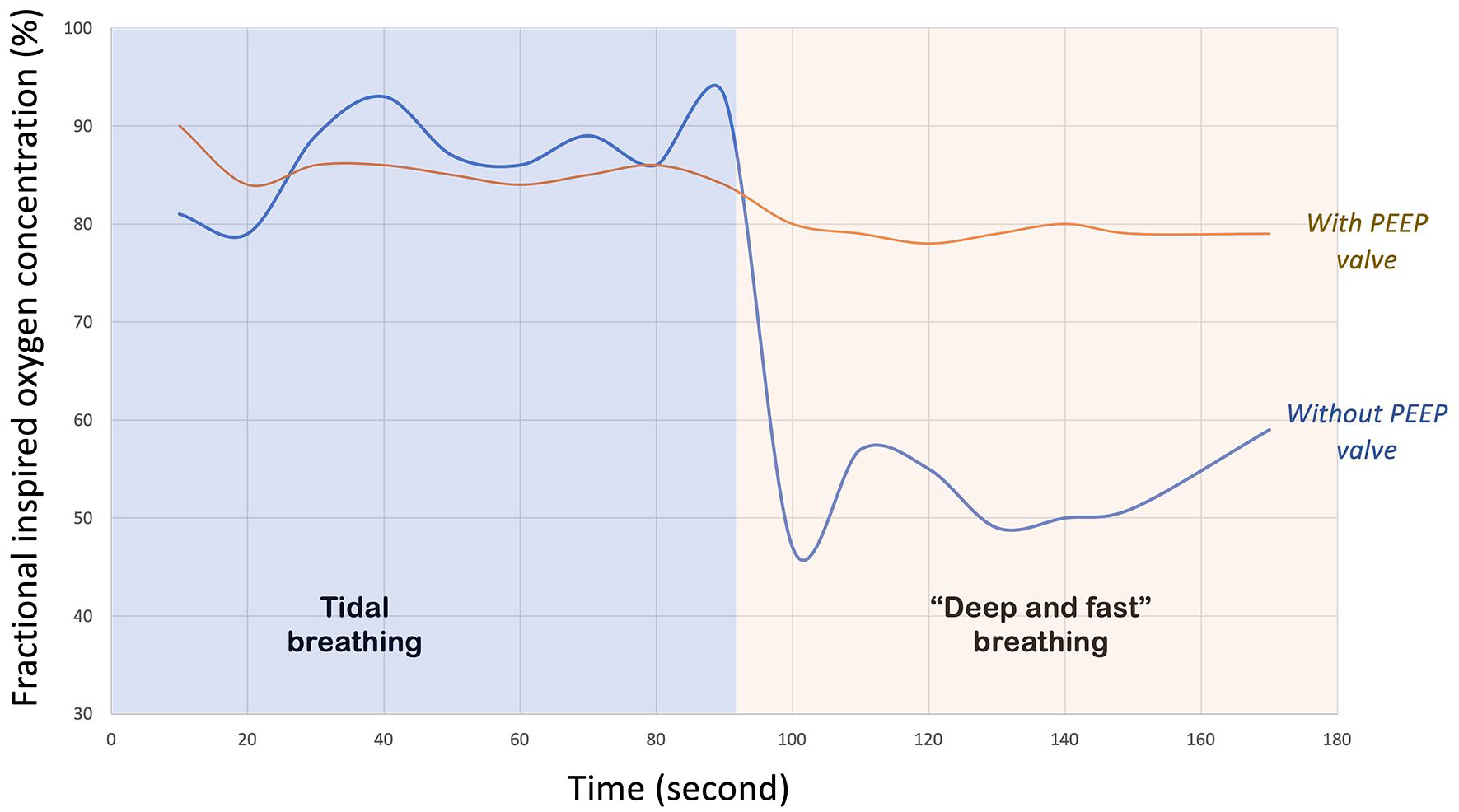
A graph showing how fractional inspired oxygen concentration (FiO2) changed with the pattern of breathing, and the effect of adding a PEEP valve. FiO2 decreased when respiratory distress was mimicked. This was reversed by addition of a PEEP valve.
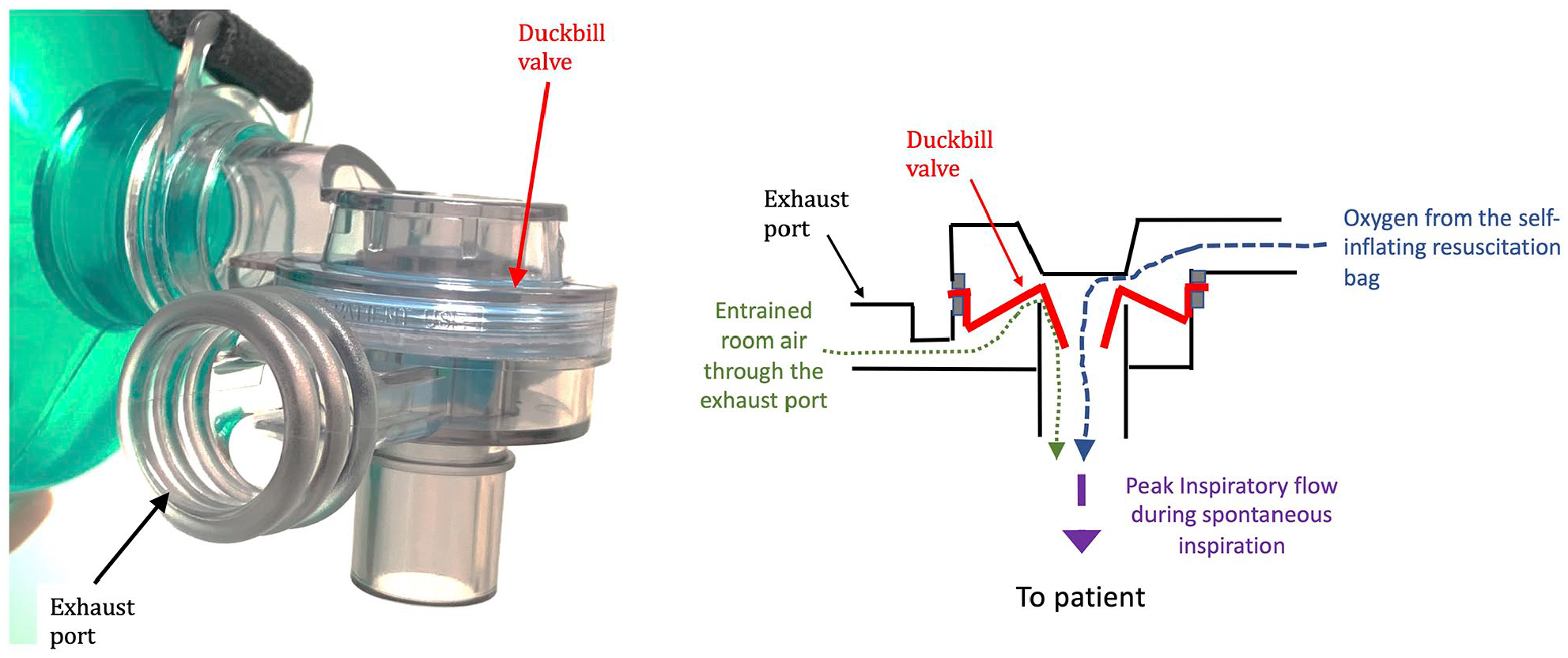
A schematic diagram showing how entrained room air and oxygen match with patient’s peak inspiratory flow during spontaneous inspiration. The relative contribution of the different components to the inspired gas is represented by the weight of the different arrows.
We then repeated the scenarios with a PEEP valve (PEEP level set at 5 cmH2O) attached to the exhaust port of the SIRB to eliminate air entrainment from the exhaust port. The FiO2 remained static even when respiratory distress was mimicked (Figure 2). This provides evidence that the exhaust port acts as a major source of air entrainment during pre-oxygenation and leads to poor oxygen delivery performance.
Our small experiment demonstrated that air entrainment could occur via the exhaust port and affect oxygen delivery performance. Our experiment also demonstrated that attaching a PEEP valve to the exhaust port improves the oxygen delivery performance. We acknowledge that our experiment only has one subject, and therefore, we are planning a formal study to prove the concept. But at the meanwhile, we hope our experiment can alert emergency care providers to consider air entrainment via the exhaust port as a cause of failed preoxygenation and pay attention to the design of the SIRBs currently in-use in their institutions. The findings of this experiment were sent to the relevant department of our institutions for safety consideration.
Footnotes
Acknowledgements
The authors thank our department information technology staff Mr Alex Lee for his help in investigating the structure of the self-inflating resuscitation bag concerned in this article.
Author contributions
Y.-Y.Y., C.P.-T.L. and J.C.H.C. all contribute equally in preparing this manuscript. C.P.-T.L. also acts as the healthy volunteer subject in the experiment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable (except C. P.-T.L., who is one of the authors of this manuscript, no other patients or volunteers were involved in this experiment).