
Abstract
Background:
CPR model of a resuscitation to be ventilated with a bag valve mask constitutes a discussion when evaluated with the current guidance.
Objective:
This study aims to compare the synchronous (30–2) ventilation–compression method with asynchronous 110/min compression–10/min ventilation in cardiac arrests where an advanced airway management is not applied and where ventilation is provided by a bag valve mask on a mannequin.
Methods:
This simulation trial was performed using two clinical cardiopulmonary resuscitation scenarios: an asynchronous scenario with 10 ventilations per minute asynchronously when compression is applied as 110 compression per minute and a synchronous scenario in which 30 compressions:2 ventilations were performed synchronously. A total of 100 people in 50 groups applied these two scenarios on mannequin. Ventilation and compression data of both scenarios were recorded.
Results:
Evaluating the compression criteria in both the scenarios performed by 50 groups in total, in terms of all criteria except compression fraction, there was no statistically difference between the two scenarios (p > 0.05). Compression fraction values in the asynchronous scenario were found to be statistically significantly higher than the synchronous scenario (96.02 ± 2.35, 81.34 ± 4.42, p < 0.001). Evaluating the ventilation criteria in both the scenarios performed by 50 groups in total; there was a statistically significant difference in all criteria. Mean ventilation rate of the asynchronous scenario was statistically higher than the synchronous scenario (7.22 ± 2.42, 5.08 ± 0.75, p < 0.001). Mean ventilation volume of the synchronous scenario was statistically higher than the asynchronous scenario (353.24 ± 45.46, 527.40 ± 96.60, p < 0.001). Ventilation ratio in sufficient volume of the synchronous scenario was statistically higher than the asynchronous scenario (36.84 ± 14.47, 75.00 ± 21.24, p < 0.001). Ventilation ratio below the minimum volume limit of the asynchronous scenario was statistically higher than the synchronous scenario (62.48 ± 14.72, 17.86 ± 19.50, p < 0.001).
Conclusion:
In our study, we concluded that the cardiopulmonary resuscitation applied by the synchronous method reached better ventilation volumes. Evaluating together with any interruption in compression, comprehensive studies are needed to reveal which patients would benefit from this result.
Introduction
Cardiopulmonary resuscitation (CPR) is a treatment procedure applied to the patients without any cardiac apex beat; in other words, patients experiencing cardiac arrest that combines the manual chest compressions in an effort to provide the pump function of the heart and the positive pressure ventilation to ensure oxygenation. 1 Ventilation in CPR can be applied asynchronously without any interrupt in compression, while it can also be applied synchronously as 30 chest compressions–2 ventilations. 2
In terms of ventilation, the safest method is tracheal intubation. However, to apply advanced airway management, it is recommended that experienced persons should try it, besides a bag valve mask (BVM) should be applied for ventilation. 2 CPR model of a resuscitation to be ventilated with a BVM constitutes a discussion when evaluated with the current guidance. European Resuscitation Council (ERC) 2017 update recommends emergency medical service providers to apply the synchronous model when advanced airway methods are not applied, 3 while American Heart Association (AHA) 2017 update, however, finds it more reasonable to apply the synchronous model in the same situation (Class IIa (benefit >> risk); level of evidence B–R) and it states that the application of asynchronous may also make sense (Class IIb (benefit > risk); level of evidence B–R). 4
Prognosis of out-of-hospital cardiac arrest is poor. 5 To develop this prognosis, CPR is needed to be applied in high quality. Ventilation applied under CPR causes interrupts in chest compressions.6–8 These interruptions reduce CPR quality. 9 There are limited literature studies which compare the asynchronous model with low interruptions and the synchronous model.
This study aims to compare the synchronous (30–2) ventilation–compression method with asynchronous 110/min compression–10/min ventilation in cardiac arrests where an advanced airway management is not applied and where ventilation is provided by a BVM on a mannequin.
Method
Ethics committee approval was obtained for this prospective, randomized, single-blind, and cross-over medical simulation trial being performed on a medical-training mannequin.
Hundred volunteer people with previous CPR experience from the profession groups with knowledge of advanced cardiovascular life support and basic life support (research assistant, intern doctor, emergency medical technician (EMT), and nurse) were included in the trial. The sample size was determined by considering the maximum number of people we will gather in our clinic and data that will be statistically sufficient. Written informed consent was obtained from the participants for their anonymized information to be published in this article.
These 100 persons were grouped, each composed of two individuals. 50 groups were formed in total. Persons in the groups were randomized by ignoring their information regarding their profession, age, weight, and body mass index (BMI). Laerdal Skillmeter Resusci-Anne® with SimPad mannequin and a size 5 facial BVM were used in this study.
Two scenarios were created: asynchronous and synchronous scenarios. Medical-mannequin was introduced to the participant people prior to the execution of the scenario. The participants were allowed to experience on the medical-mannequin within sufficient time. Compression and ventilation data on the medical-mannequin under this experiment were shown through SimPad. In both scenarios, the medical-mannequin was laid on the ground in supine position.
In the asynchronous scenario, one person applied ventilation 10 times per minute, while the other person made compression independent of ventilation (asynchronous) with 110 compressions per minute. At the end of the 2-min CPR, a 10-s interruption was given. The procedure was repeated after switching the tasks of the persons making the compression and ventilation for the same interventions. It took 4 min 10 s in total. In the synchronous scenario, one person applied 30 compressions at the rate of 110/min, while the other person applied 2 ventilations just after the end of the compression. There was synchronization between compression and ventilation. At the end of the 2-min CPR, a 10-s interruption was given. The procedure was repeated after switching the tasks of the persons making the compression and ventilation for the same interventions. It took 4 min10 s in total. In both scenarios, situations, such as starting the CPR, switching the task, and completing the intervention times, were monitored with a stopwatch and the participants were told about this information. Targeting 110/min heart rate in both scenarios results from taking the 100–120 heart rate as a reference specified in the 2015 AHA and ERC guidelines.10,11
Half of the 50 groups started CPR with randomized asynchronous scenario, and other half with synchronous scenario. Both groups took a rest at least 2 h after completing one scenario and they applied the other scenario which they did not performed (Figure 1).
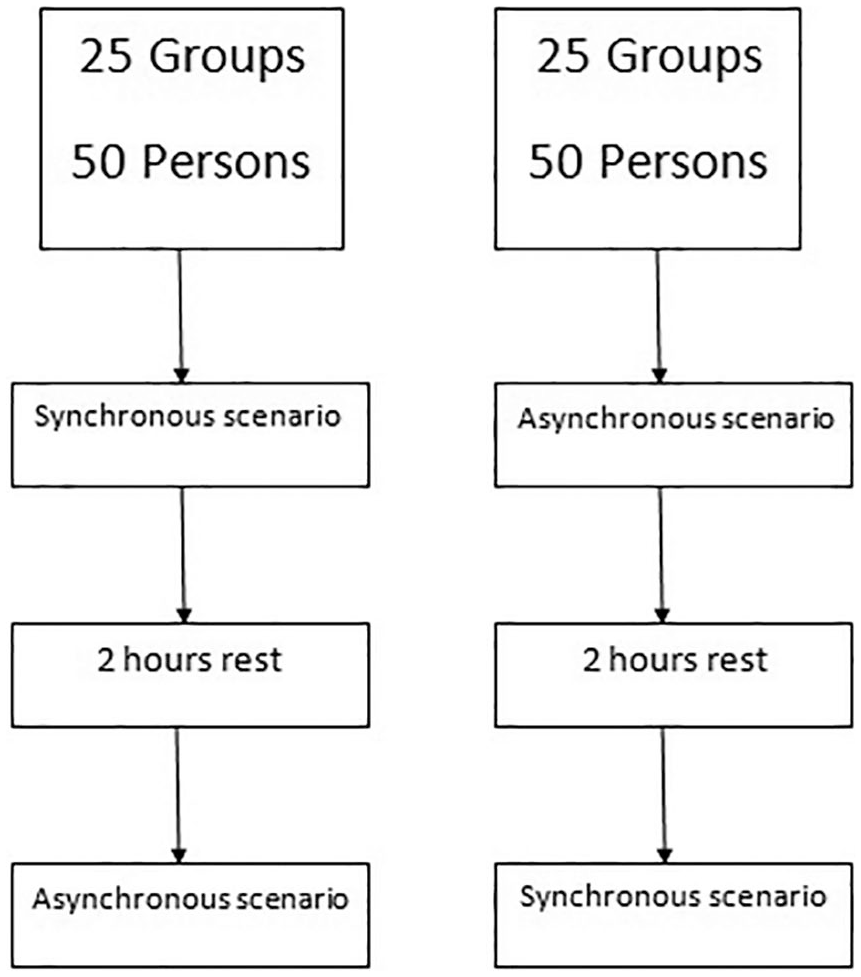
Study design.
In both scenarios, to reach the targeted compression rate per minute, a metronome that produces 110 metrical ticks (beats) per minute was used. In the asynchronous scenario, a second metronome was used to reach 10 ventilation rates per minute.
After applying both scenarios, the participants were asked about how satisfied they were with both scenarios. They were asked to express their level of satisfaction from 1 to 10. Albeit it is not the primary purpose of the trial, satisfaction scale measures were used to determine which CPR model was preferred more.
The participants’ information, such as age, gender, profession, weight, height, and BMI, and their satisfaction scale measures for synchronous and asynchronous CPR models were recorded. In addition, to evaluate the performances of 50 CPR applications performed in accordance with the asynchronous and synchronous scenarios, the following information was also recorded from the summary section of the SimPad QCPR:
Compression performance criteria are as follows:
Compression fraction (%)
Mean depth (mm)
Mean compression rate (compression/min)
Compression ratio with complete chest recoil (%)
Compression ratio in sufficient depth (%)
Compression ratio at sufficient rate (%)
Ventilation performance criteria are as follows:
Mean ventilation rate (breath/min)
Mean ventilation volume (mL)
Ventilation ratio in sufficient volume (%)
Ventilation ratio exceeding the maximum volume limit (%)
Ventilation ratio below the minimum volume limit (%)
The manufacturer has determined the minimum ventilation volume on the SimPad medical-mannequin as 400 mL, and the maximum ventilation volume as 700 mL, referring to the AHA and ERC guidelines.
Satisfaction scale measures and ventilation and compression data on the medical-mannequin were are compared by asynchronous and synchronous methods. Statistical analyses of the data were made using SPSS 20.0 (SPSS Inc., Chicago, IL) packaged software. Analyses of normality of the data were made using histograms and Kolmogorov–Smirnov test. Non-normally distributed quantitative data were stated as median (25%–75% quarters), while normally distributed quantitative variables were stated as mean ± standard deviation, and categorical variables were stated as frequency (percentage). The differences between the groups were investigated using the Mann–Whitney U test in non-normally distributed quantitative variables, while Student t-test was used for normally distributed quantitative variables. Categorical variables were compared between groups using chi-square test. p < 0.05 value was accepted as statistically significant.
Results
In total, 100 participants were included in this study. 55 of them (55%) were males and 45 of them (45%) were females. 37 of the participants (37%) were assistant doctors, 40 of them (40%) were intern doctors, 21 of them (21%) were nurses, and 2 of them (2%) were EMTs. The mean age of the participants was 27.11 ± 3.99, mean BMI was 24.97 ± 3.99, mean scale result for satisfaction of synchronous scenario was 7.49 ± 1.6, and mean scale result for satisfaction of asynchronous scenario was 7.23 ± 1.75. There was no significant difference between the synchronous and the asynchronous scenario in terms of satisfaction (p = 0.275). Table 1 shows the characteristics of the participants.
Characteristics of participants.
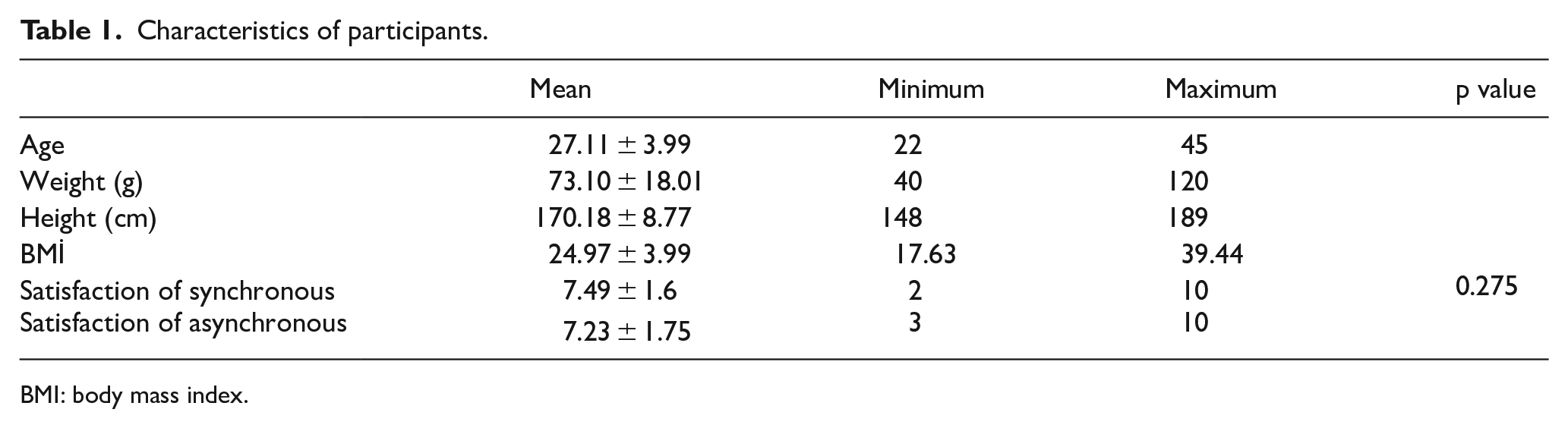
BMI: body mass index.
Evaluating the compression criteria in the synchronous and asynchronous scenarios performed by 50 groups in total, in terms of all criteria except compression fraction, there was no statistically difference between the two scenarios (for all criteria except compression fraction, p > 0.05). Compression fraction values in the asynchronous scenario were found to be statistically significantly higher than the synchronous scenario (asynchronous 96.02 ± 2.35, synchronous 81.34 ± 4.42, p < 0.001).
Evaluating the ventilation criteria in the synchronous and asynchronous scenarios performed by 50 groups in total, a statistically significant difference was found between synchronous and asynchronous scenarios in all criteria. The mean ventilation rate of the asynchronous scenario was statistically higher than the synchronous scenario (asynchronous 7.22 ± 2.42, synchronous 5.08 ± 0.75, p < 0.001). The mean ventilation volume of the synchronous scenario was statistically higher than the asynchronous scenario (asynchronous 353.24 ± 45.46 mL, synchronous 527.40 ± 96.60 mL, p < 0.001) (Figure 2). The ventilation ratio in sufficient volume of the synchronous scenario was statistically higher than the asynchronous scenario (asynchronous 36.84%± 14.47, synchronous 75.00%± 21.24, p < 0.001) (Figure 3). The ventilation ratio exceeding the maximum volume limit of the synchronous scenario was statistically higher than the asynchronous scenario (asynchronous 0.68%± 2.15, synchronous 7.14%± 16.77, p = 0.009). The ventilation ratio below the minimum volume limit of the asynchronous scenario was statistically higher than the synchronous scenario (asynchronous 62.48%± 14.72, synchronous 17.86%± 19.50, p < 0.001) (Figure 4). Table 2 shows the results of ventilation and compression parameters of the groups in detail.
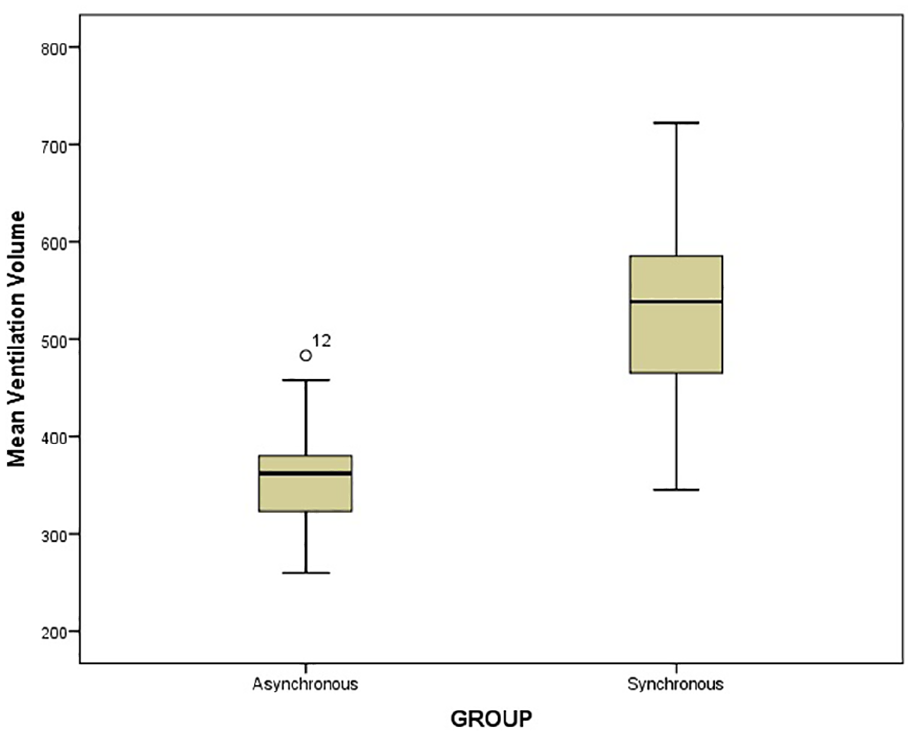
Comparison of mean ventilation volume between groups.
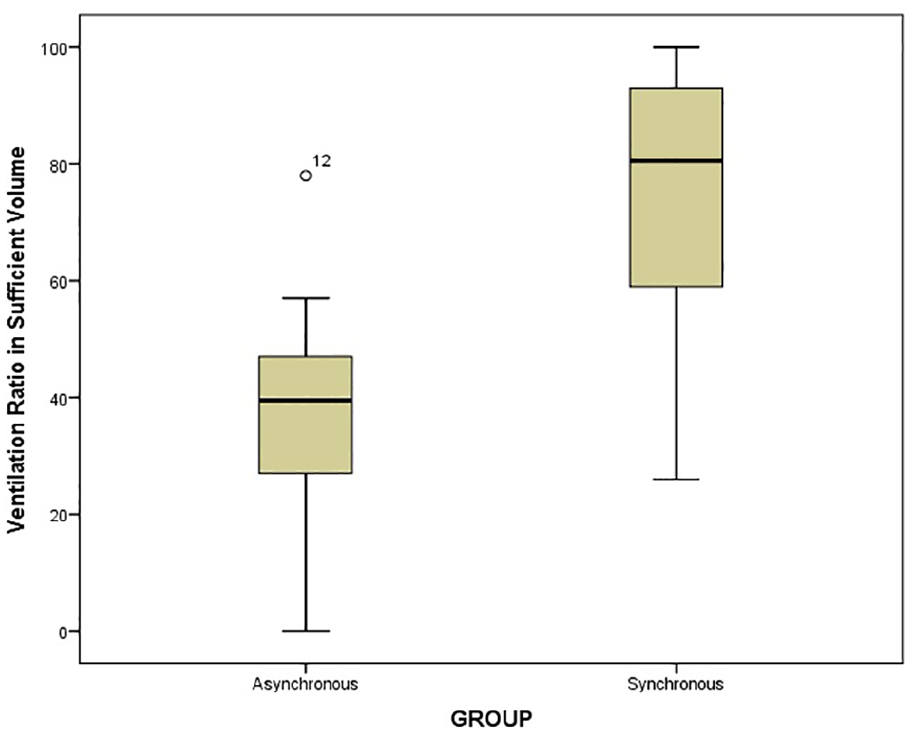
Comparison of ventilation ratio in sufficient volume between groups.
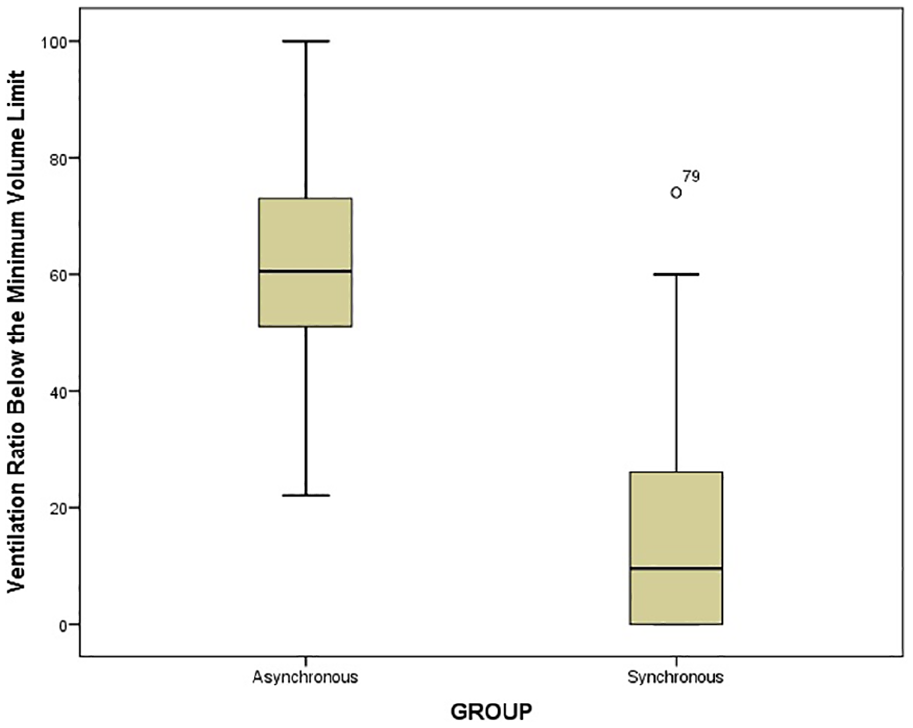
Comparison of ventilation ratio below the minimum volume limit between groups.
The results of ventilation and compression parameters of the groups.
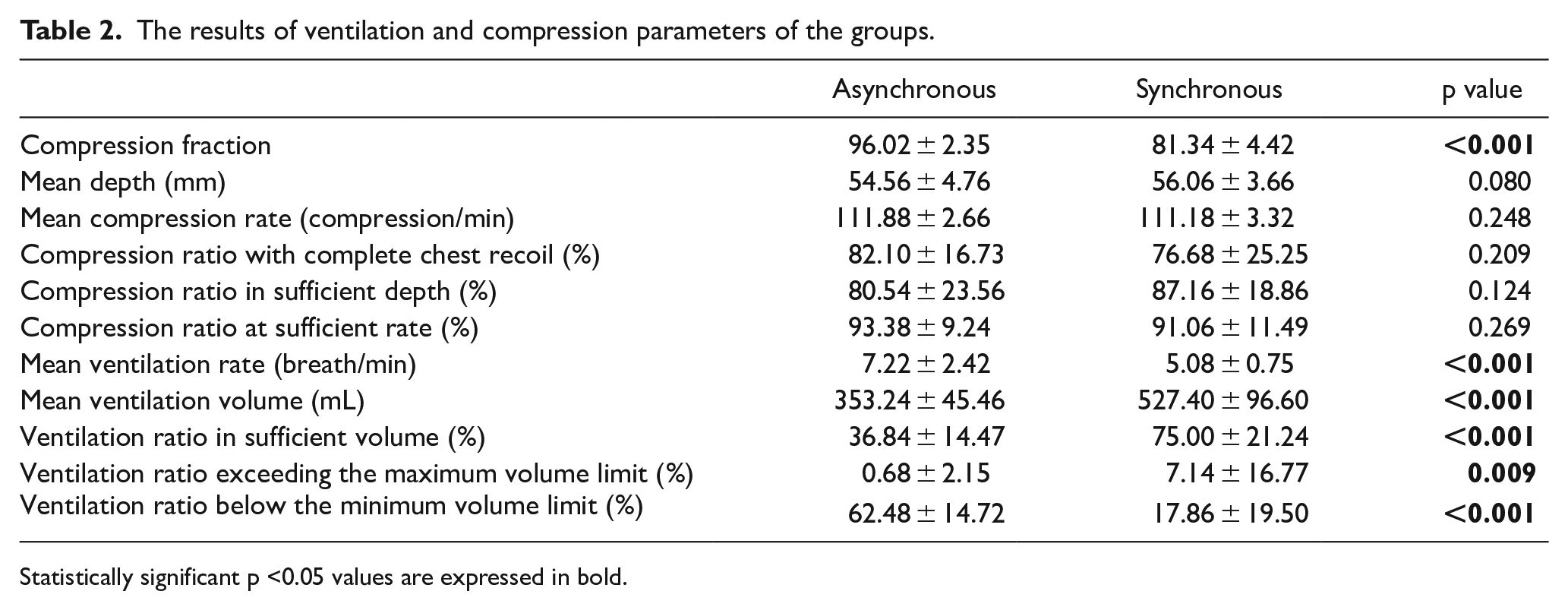
Statistically significant p <0.05 values are expressed in bold.
Discussion
Our study, in the cardiac arrest cases ventilated using a BVM, compares the CPR that is performed asynchronously without interrupting the compression and the CPR that is performed synchronously 30:2. In our study, the mean ventilation volume, the ventilation ratio in sufficient volume, and the ventilation ratio exceeding the maximum volume were significantly higher in the synchronous scenario, while the ventilation ratio below the minimum volume was significantly higher in the asynchronous scenario.
Reviewing the literature, it was found that Nichol et al. 12 compared these two methods in out-of-hospital cardiac arrest patients, while Manrique et al. 13 in pediatric animal model with cardiac arrest due to asphyxia, and Sanson et al. 14 in out-of-hospital cardiac arrest patients. In this study, the mean ventilation rate was found to be statistically significant in favor of asynchronously. In their study comparing these two scenarios, Sanson et al. 14 found the ventilation rate to be high in favor of asynchronous. In this study, the ventilation rate in the asynchronous scenario was found to be 10.2 ± 3.7 breaths/min. The reason why we remained below the average of 10 breaths/min (7.22 ± 2.42) in the asynchronous scenario although we used a metronome in our study may be due to the difference in the ventilation rate assessment of two studies. Ventilation in medical-mannequin studies is perceived by the volume that will occur in the artificial lung, while in human-driven studies, however, it is perceived by the screen waves on the defibrillator software or chest wall-induced movement. In addition, another study showed that high ventilation rate had no effect on survival. 15 We could not find any data in the literature comparing the two scenarios by evaluating the volume and volume ratios. This is because, particularly in the human experimentations, failure to collect data including volume and volume ratios other than ventilation rate is the limitation of those studies. In their study using experimental animals, Manrique et al. evaluated the respiratory parameter by controlling the arterial carbon dioxide pressure, although they found lower in the asynchronous scenario, they did not find any difference statistically. The reason for low volumes in the asynchronous scenario may be due to the fact that the volume to be delivered with positive pressure in compression cannot be provided with the BVM.
In this study, the compression fraction was found to be statistically significantly higher in favor of asynchronously. Similarly, Sanson et al. 14 found the compression fraction statistically significant and high in favor of asynchronous. This can be caused by the interruption of compression for ventilation in the synchronous scenario. In our study, no statistically significant difference was found between both scenarios in terms of mean compression rate, compression depth, compression ratio at a sufficient rate, compression ratio with a complete return of rib cage, and compression ratio in sufficient depth. In the studies conducted by Nichol et al. 12 and Manrique et al., 13 no statistically significant difference was found between the two scenarios in terms of compression depth and compression rate, while Sanson et al. 14 found no difference in terms of compression rate. Study data are compatible with the literature.
Under the guidance of current guides,3,4 in the study conducted by Sanson et al., 14 the survival rates of synchronous CPR, which were recommended at times when no advanced airway method was applied, were found to be lower compared to asynchronous or Nichol et al. 12 did not found any significant difference. Since we performed this study using a medical-mannequin, we were not able to determine the survival rates. However, considering this survival rates with the ventilation data in this study, it may come to mind that there is a contradiction. The reason for this case may be due to the fact that the minute ventilation volume of the asynchronous scenario in our study exceeds at least 300 mL tidal volume threshold, and that this situation is considered to be sufficient for gas exchange in the literature.16–18 Besides, the fact that the asynchronous scenario achieves better compression fraction values may be another reason. This result may be also due to the fact that non-volume reasons such as compression interruptions become more effective in human and animal experiments with better survival rates.
Compression interruptions and lower compression fraction in the synchronous model indicate that the asynchronous model produces better compression quality. However, in the literature, while an uninterrupted compression in cardiac arrests with shockable electrical rhythm increases the survival rates;19–21 uninterrupted compressions in non-cardiac arrest patients 22 with non-shockable electrical rhythm 19 were not associated with a significant healing. Although there were compression interruptions in the CPR applied by the synchronous method, the fact that better ventilation volumes were observed suggested that better results can be obtained if non-cardiac (such as asphyxiation) arrest patients with special ventilation conditions are used before the advanced airway method is applied.
As a result, in this study, we concluded that the CPR applied by the synchronous method reached better ventilation volumes and the CPR performed with the asynchronous method reached a better compression quality in terms of compression fraction. Comprehensive studies are needed to reveal which patients would benefit from this result.
The factors, such as being a mannequin study, failure to evaluate the survival rates, and scarcity of the research population can be considered as the limitations of our study.
Footnotes
Author contributions
Z.D.D. and K.K. contributed to concept and control. K.K. contributed to design, analyze, literature review, and writing the article. Z.D.D., K.K., and M.K.A. contributed to critical review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data will be made available on request to bona fide researchers only. Data transfer agreement states that data cannot be used to identify participants
Ethical approval
This study obtained ethical approval by Necmettin Erbakan University Meram Medical Faculty, Pharmaceutical and Non-Medical Device Studies Ethical Committee by the decision number of 2019/2152.
Informed consent
Informed consent form was obtained from the participants of this study.
Human rights
During the research, the World Medical Association (WMA) Declaration of HELSINKI and/ or the World Psychiatric Association HAWAII Declaration of Good Clinical Practice rules were complied.