
Abstract
Objective:
The objective of this study was to determine the impact of adding selected mechanism of injury (MOI) to the existing trauma diversion criteria adopted in Hong Kong.
Method:
This is a cross-sectional study based on the trauma registry of New Territory West Cluster (NTWC) of Hospital Authority from January 2017 to December 2019. All adult patients aged 18 years or above were recruited if their injury occurred in the catchment area of Pok Oi Hospital (POH) or Tin Shui Wai Hospital (TSWH). Performance of the protocol before and after MOI criteria being added in terms of over-diversion and under-diversion rate was determined. Model discrimination was evaluated by plotting the receiver operating characteristic curve, and the area under the curve was compared before and after MOI criteria added. Net reclassification improvement and integrated discrimination improvement indices were evaluated.
Result:
A total of 502 patients were included for analysis. Before MOI criteria were added, the over-diversion rate and under-diversion rate were 31.1% and 54.7%, respectively. After MOI criteria were added, the over-diversion rate and under-diversion rate were 33.1% and 34.3%, respectively. The receiver operating characteristic curve of current primary trauma diversion (PTD) criteria had an area under the curve of 66.9% (95% confidence interval: 63%–71%). After adding MOI criteria, the new receiver operating characteristic curve yielded an area under the curve of 73.7% (95% confidence interval: 70%–78%), which is significantly better (p < 0.001). Net reclassification improvement and integrated discrimination improvement indices indicated that including MOI criteria would improve the model prediction.
Conclusion:
Adding mechanism of injury can improve trauma diversion protocol performance.
Introduction
Primary trauma diversion (PTD) means transferring patients from the injury scene to the trauma centre directly, while in secondary trauma diversion (STD) patients are transferred from the scene to the nearest hospital but found to meet certain criteria there, and subsequently transferred to the trauma centre for definitive care. In New Territory West Cluster (NTWC) of Hospital Authority, Tuen Mun hospital (TMH) is the designated trauma centre linked with two regional hospitals Pok Oi Hospital (POH) and Tin Shui Wai Hospital (TSWH). Major trauma patients fulfilling the PTD criteria within the catchment area of POH and TSWH are primarily diverted to TMH by the ambulance service. Patients who do not fulfil the PTD criteria are transferred to POH or TSWH for initial management and then secondarily diverted to TMH for definitive management if necessary.
PTD of severely injured patients was associated with a reduction in mortality and morbidity despite longer prehospital time.1–3
A prehospital trauma diversion protocol has been implemented since 2008 in Hong Kong. 4 The trauma diversion criteria adopted in Hong Kong is different from the Guidelines for field triage of injured patients published by the U.S. Centre for Disease Control and Prevention. The anatomical and physiological criteria are similar but omitted the mechanism of injury (MOI) and other special criteria, for example, extremes of age, pregnancy and anticoagulation. 5 MOI and other special criteria might identify many major trauma patients missed by physiological and anatomical criteria alone. Figures 1 and 2 showed the trauma diversion protocol in Hong Kong and United States, respectively.
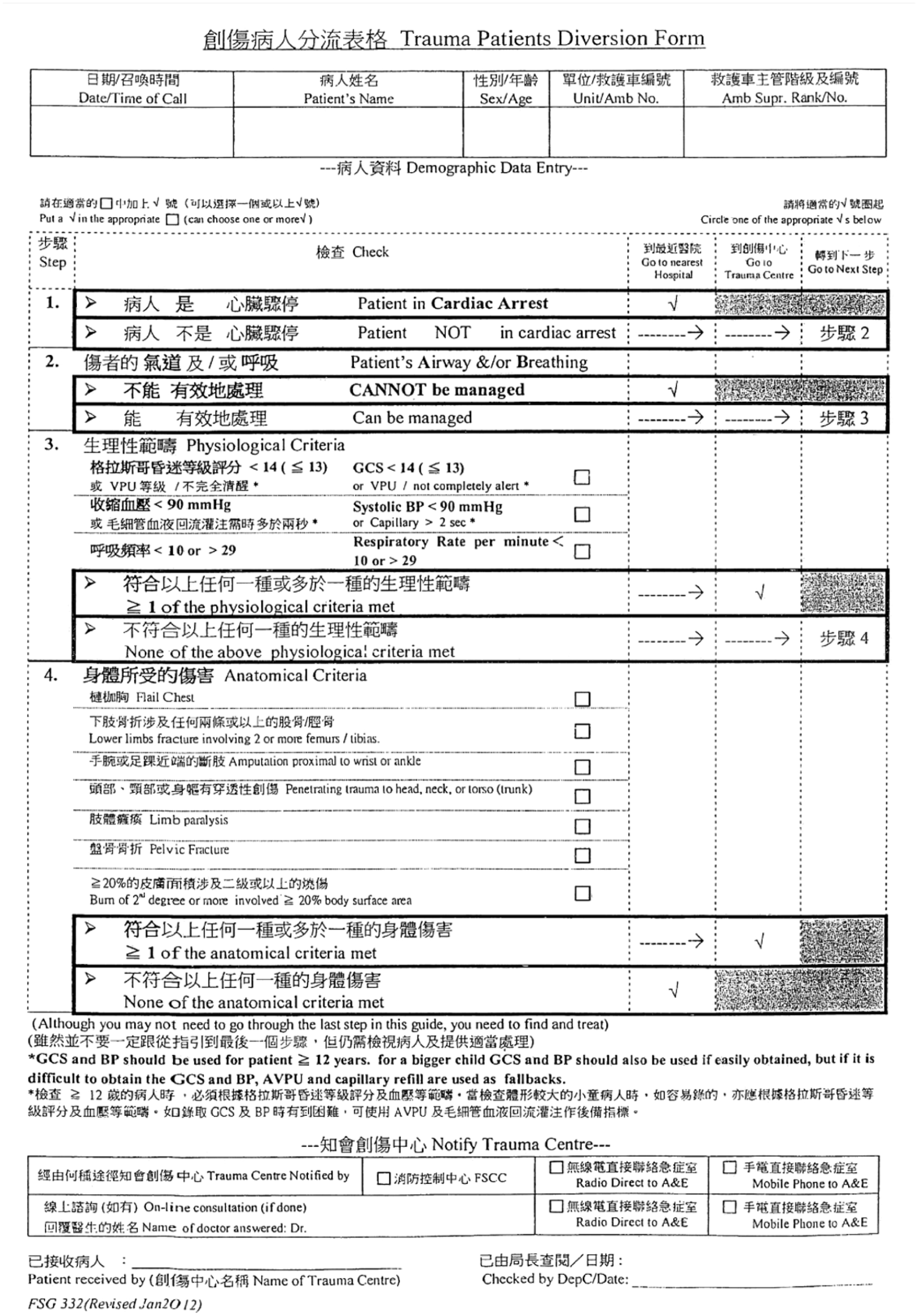
Prehospital trauma diversion protocol in Hong Kong.
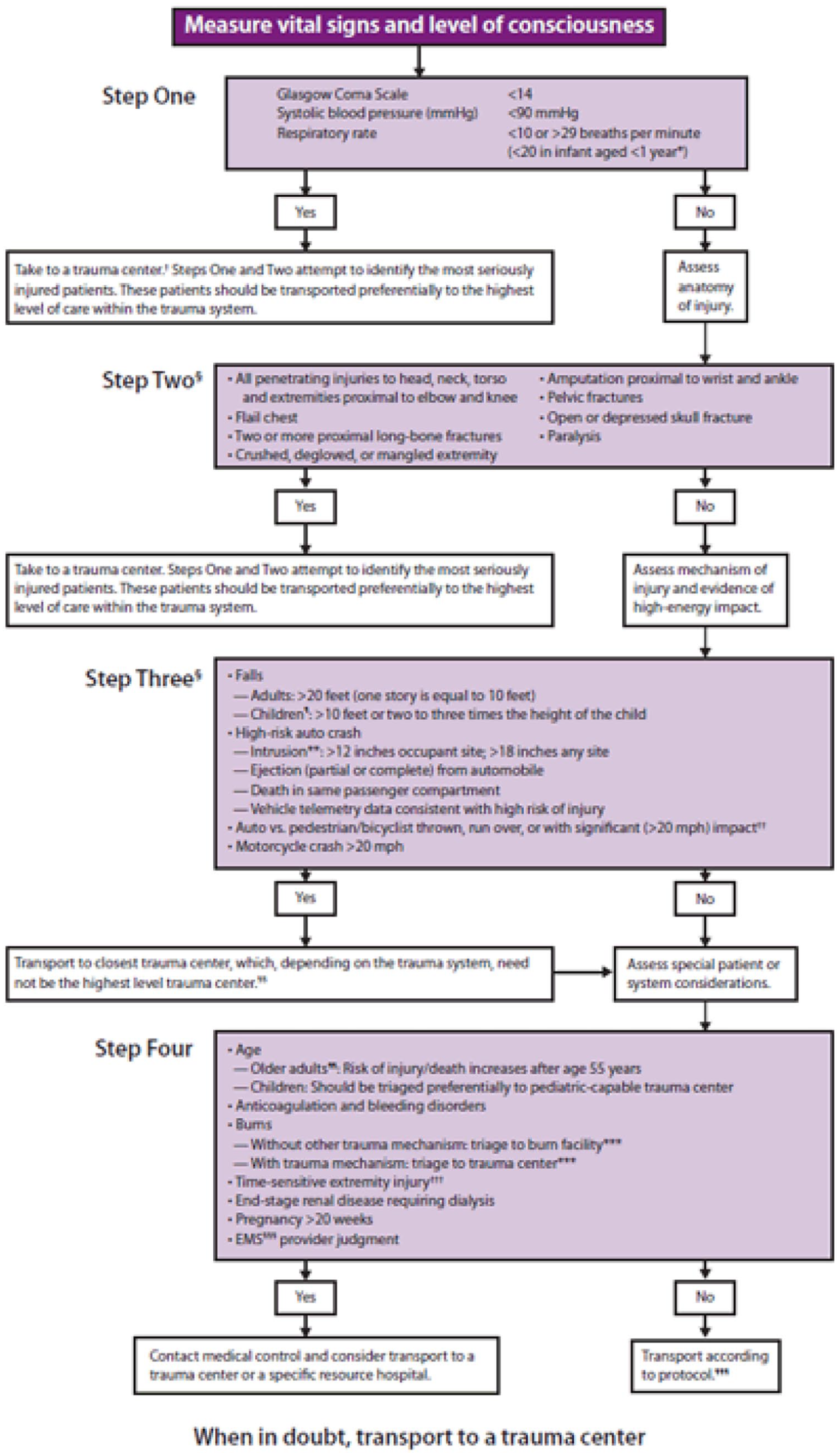
Field triage guideline in the United States.
A previous local study showed the over-diversion rate and under-diversion rate of current trauma diversion in a region of Hong Kong to be 70% and 19.7%, respectively. 6 This is higher than the acceptable range of 25%–50% for over-diversion and less than 5% of under-diversion recommended by the American College of Surgeons (ACS). 7 The current trauma diversion protocol is not accurate enough. Anatomical and physiological criteria alone are probably inadequate to ensure appropriateness of trauma diversion.
Our study aimed to report the performance of current trauma diversion protocol and determine the impact of adding MOI criteria.
Methods
The study was a cross-sectional study based on data from our local trauma registry from January 2017 to December 2019.
All major adult trauma patients aged 18 years old or above within the catchment area of Pok Oi Hospital (POH) and Tin Shui Wai Hospital (TSWH) were included in the study. Patients with prehospital traumatic cardiac arrest or required emergent airway or breathing intervention were excluded from the study as those patients should be diverted to the nearest hospital for resuscitation. Those noncompliance case to the current diversion protocol by the ambulance crew were also excluded. The definition of noncompliance is either the cases that does not meet PTD criteria but directly transferred to trauma centre or the cases that meet PTD criteria but transferred to the non-trauma centre instead.
The trauma nurse coordinator traced the following to be included in the trauma registry: (1) patients who required activation of trauma call; (2) cases transferred from other hospital and fit for trauma registry inclusion criteria/with significant injury; (3) patients with unstable vital signs with triage category 1 or 2 cases without trauma call activation; (4) all trauma-related deaths; (5) trauma cases admitted to intensive care unit or with major operations performed. Figure 3 showed the criteria for trauma team activation in our regional cluster. Figure 4 showed the triage category guideline for trauma scenarios in accident and emergency departments under hospital authority in Hong Kong.
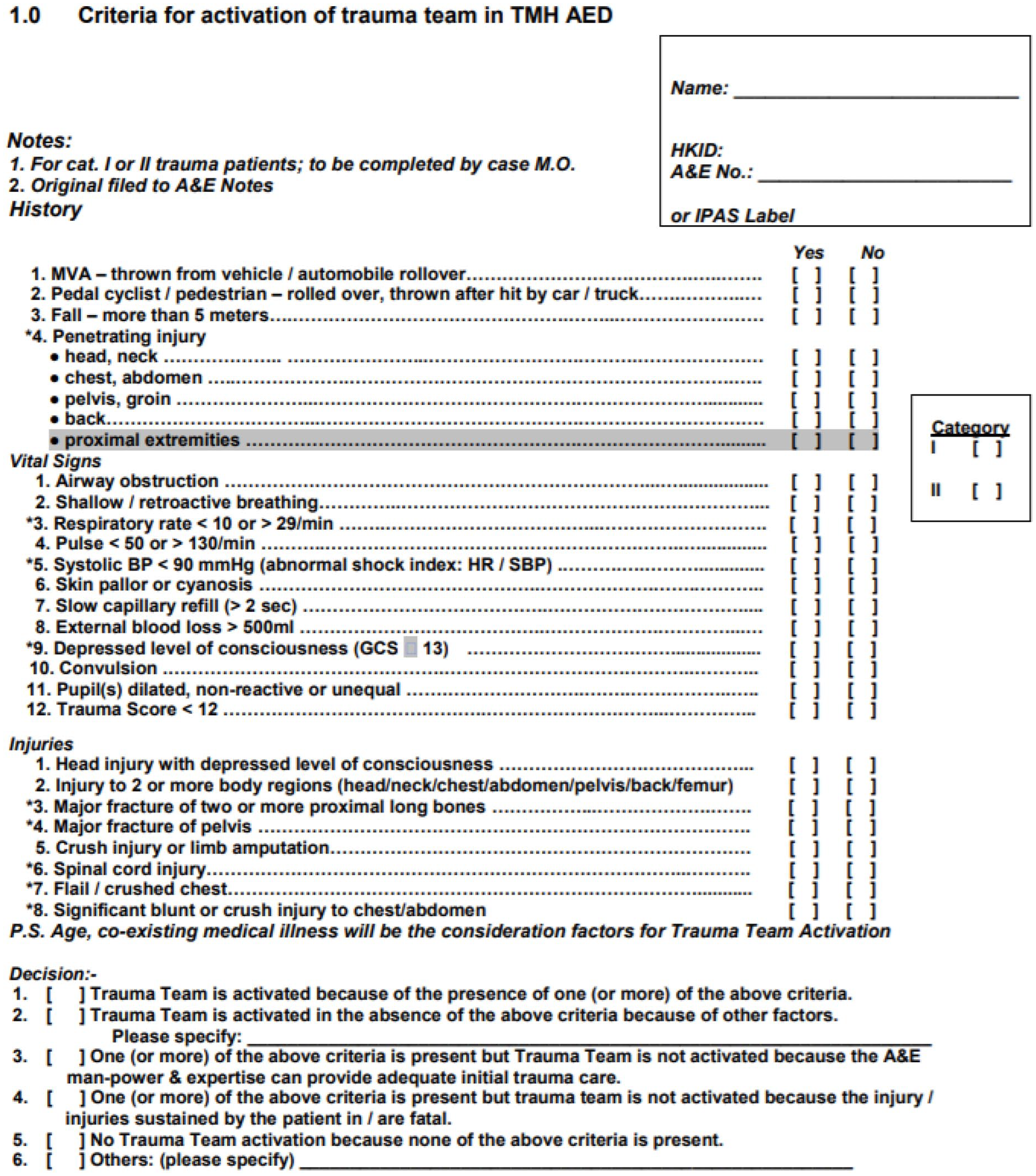
Trauma team activation criteria in Tuen Mun Hospital.
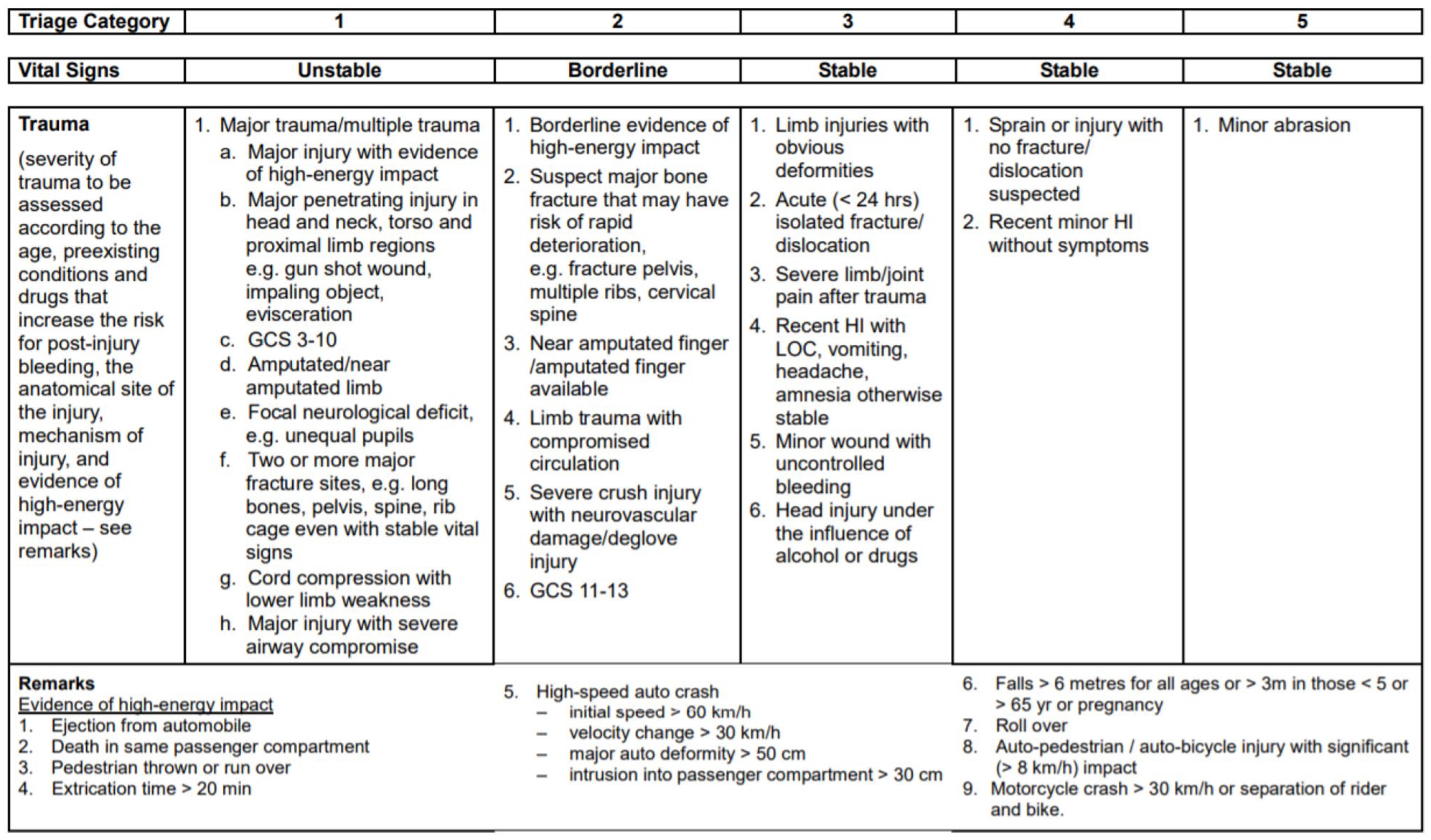
Accident and emergency triage guideline for trauma.
Relevant data were obtained from the trauma registry, including patients’ demographics, MOI, trauma score (Injury Severity Score (ISS), Abbreviated Injury Score (AIS), Revised Trauma Score (RTS)), prehospital clinical parameters, need for trauma team activation, intensive care admission, and patients’ outcome. Descriptive statistics were used to describe the characteristics of different parameters among the patients. Categorical variables were expressed as proportions and percentages while continuous variable was expressed as mean and standard deviation. No major missing data from the trauma registry were identified. Intrinsic bias of retrospective studies included misclassification bias and recall bias.
Sample size/power analysis was not calculated in this retrospective study. Duration of recruitment chosen was based on clinical experience.
The need of trauma centre level of care was defined as trauma team activation in trauma centre. Over-diversion was defined as meeting diversion protocol criteria and therefore primarily diverted but not required trauma team activation. Under-diversion was defined as not meeting diversion protocol criteria and therefore transferred to nearest hospital first but finally required trauma team activation.
Performance of trauma diversion protocol was represented by the over- and under-diversion rates. Over-diversion rate was represented by 1 – positive predictive value, that is, (false positive)/( (true positive) + (false positive)). Under-diversion rate was represented by 1 – sensitivity, that is, (false negative)/((true positive) + (false negative)).
Model discrimination was evaluated by plotting the receiver operating characteristic (ROC) curve and the area under the curve (AUC) before and after each MOI criteria added individually and combined was compared with non-parametric method suggested by DeLong et al. 8 Net reclassification improvement and integrated discrimination improvement indices were calculated to assess the improvement of model prediction with the addition of combined MOI criteria. A p value < 0.05 was considered statistically significant. The 95% confidence interval (CI) was reported wherever appropriate. Statistical analyses were done with MedCalc® Statistical Software version 20 and RStudio version 1.4.1717.
MOI criteria we used in this study included free fall ⩾ 2 m and pedestrian/cyclist/motorcyclist being thrown after collision. The primary outcome is trauma team activation (TTA) defining the need of Trauma Centre level of care. Secondary outcomes include mortality, intensive care unit (ICU)/high dependent unit (HDU) admission, ISS > 15. Figure 3 showed the criteria for trauma team activation in Tuen Mun Hospital. The attending emergency physician has the final decision based on the criteria. Mortality was assessed at time of discharge or at day 30 of admission.
Results
There were 566 cases in total. Nine cases of prehospital cardiac arrest or compromised airway or breathing cases were excluded. Fifty-five noncompliance cases (9.7%) of ambulance crew to the trauma diversion protocol were also excluded. A total of 502 patients were included in the analysis. Within the 55 noncompliance cases, 34 of them were over-diversion and 21 were under-diversion. Trauma team activation was required in 19 cases.
The characteristics of our cohort were shown in Table 1. The mean age was 53.8 years old. Male was a predominant proportion (71.3%). Majority of injuries were blunt trauma cases (89.8%). Fall was the most common mechanism (45.2%), followed by motor vehicle collision (36.5%). Trauma team was activated in 36.1% of all cases. The mean AIS score for head and neck injury was the highest of all body regions, scoring 1.5. The mean ISS was 11.7. The mean RTS score was 7.6. Mortality was 2.8%. About 20.1% of patients required ICU/HDU admission.
Patient characteristics.
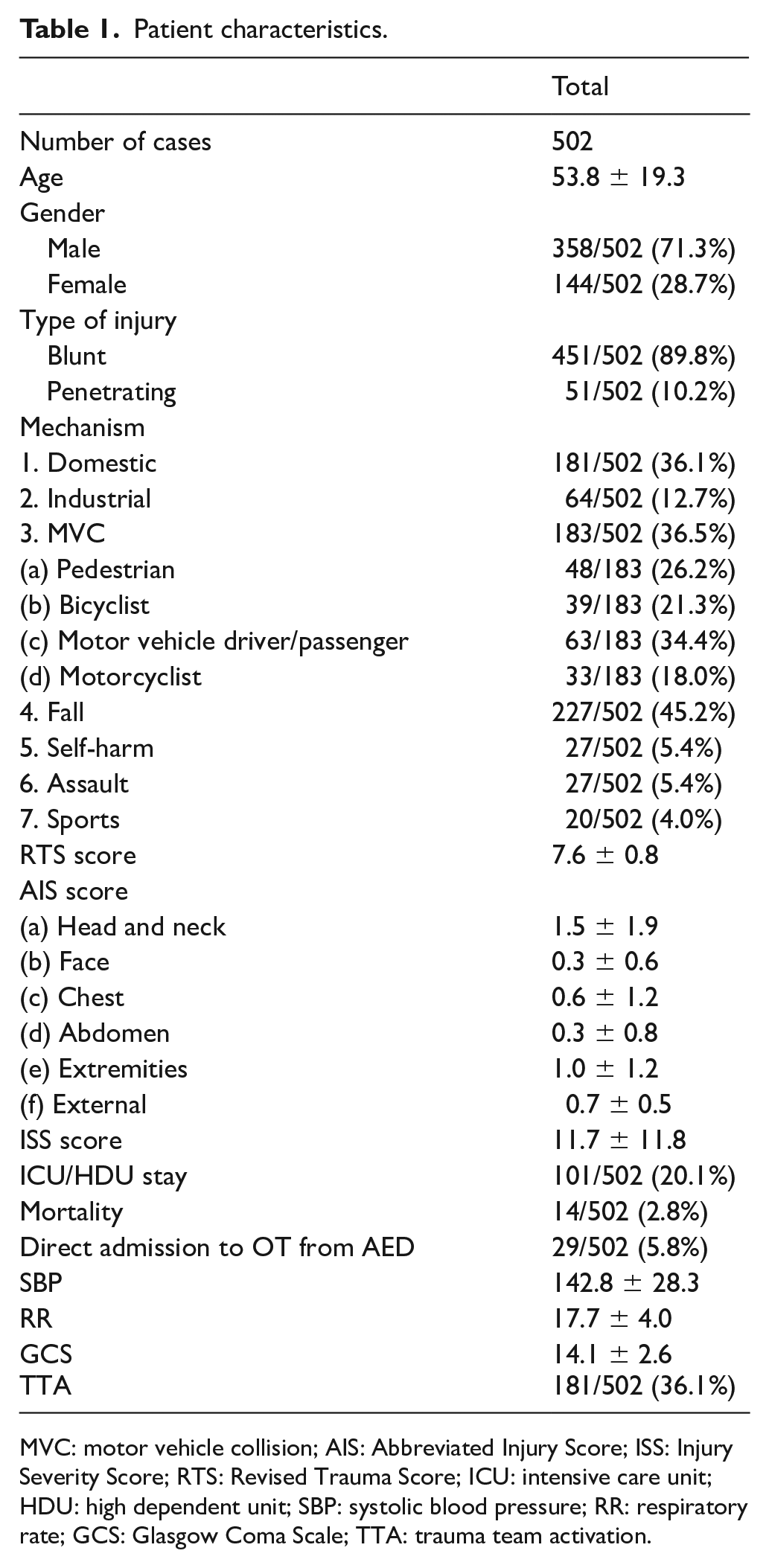
MVC: motor vehicle collision; AIS: Abbreviated Injury Score; ISS: Injury Severity Score; RTS: Revised Trauma Score; ICU: intensive care unit; HDU: high dependent unit; SBP: systolic blood pressure; RR: respiratory rate; GCS: Glasgow Coma Scale; TTA: trauma team activation.
Primary outcome
Table 2 showed the performance of current diversion protocol, new protocol after each MOI criteria added individually and combined. In the current diversion protocol, the over-diversion rate was 31.1% and the under-diversion rate was 54.7%. After both MOI criteria (fall ⩾ 2 m, motor vehicle collision (MVC) thrown) were added, the over-diversion rate was 33.1% and under-diversion rate was 34.3%. We also calculated the over- and under-diversion rates when each MOI criteria were added individually. The over- and under-diversion rates when fall > 2 m criteria added were 33.3% and 37%, respectively. The over- and under-diversion rates when MVC thrown criteria added were 31% and 51.9%, respectively.
Performance of current diversion protocol, new protocol after each MOI criteria added individually and combined.
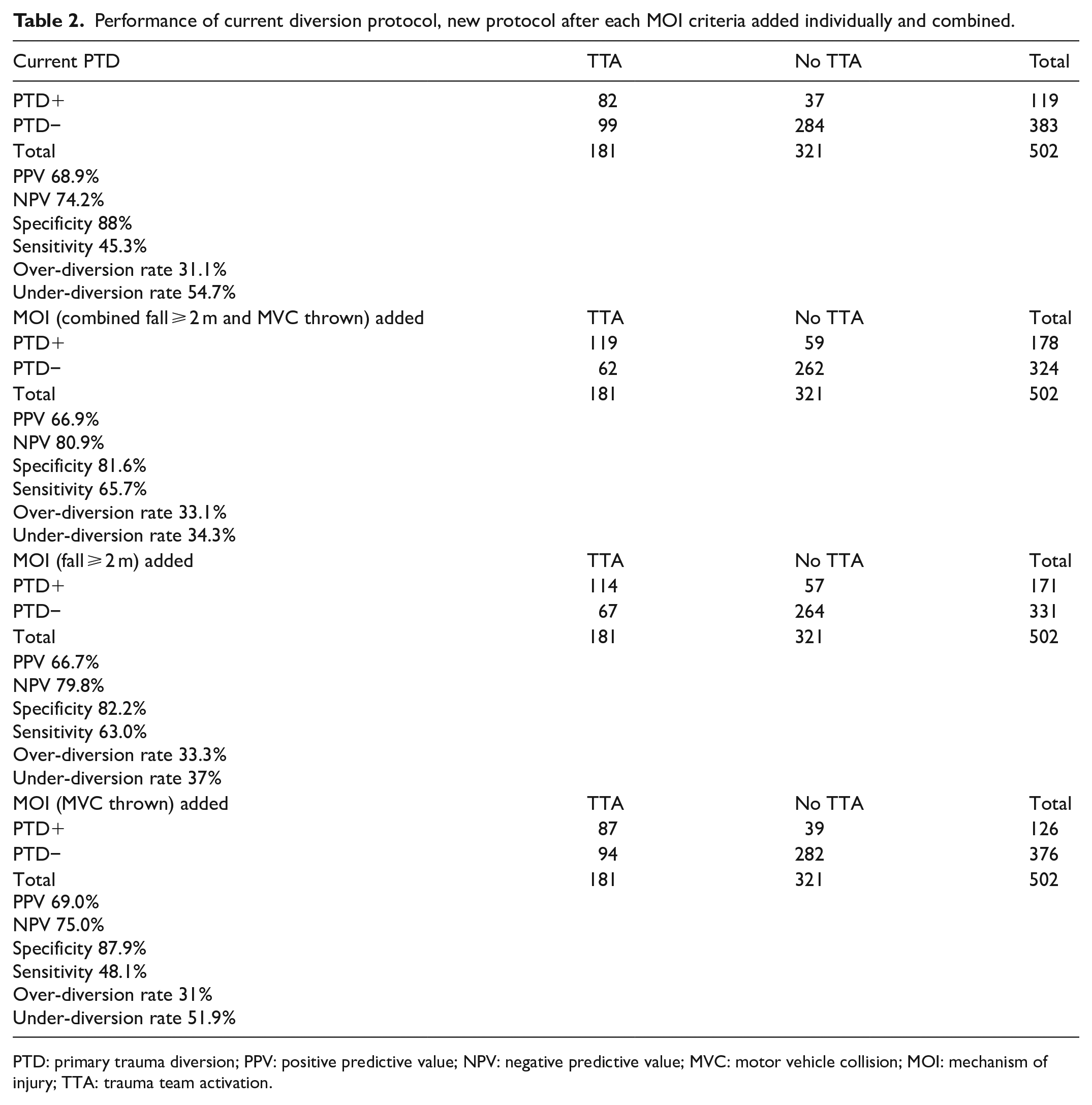
PTD: primary trauma diversion; PPV: positive predictive value; NPV: negative predictive value; MVC: motor vehicle collision; MOI: mechanism of injury; TTA: trauma team activation.
Table 3 showed the comparison of AUC of the ROC curve predicting TTA. The AUC of current trauma diversion protocol was 0.669. Adding both MOI criteria improved with predictive performance of the trauma diversion protocol (AUC = 0.737). The increment of AUC of this new model was 0.0679 compared with the current diversion protocol and showed statistically significant difference (p < 0.001). The increment of AUC after adding fall > 2 m criteria was 0.0572 which were also statistically significant (p < 0.001). The increment of AUC after adding MVC thrown was 0.0107 but was not statistically significant.
Comparison of area under receiver operating characteristic curve (ROC) predicting TTA of the diversion protocol before and after MOI criteria added.
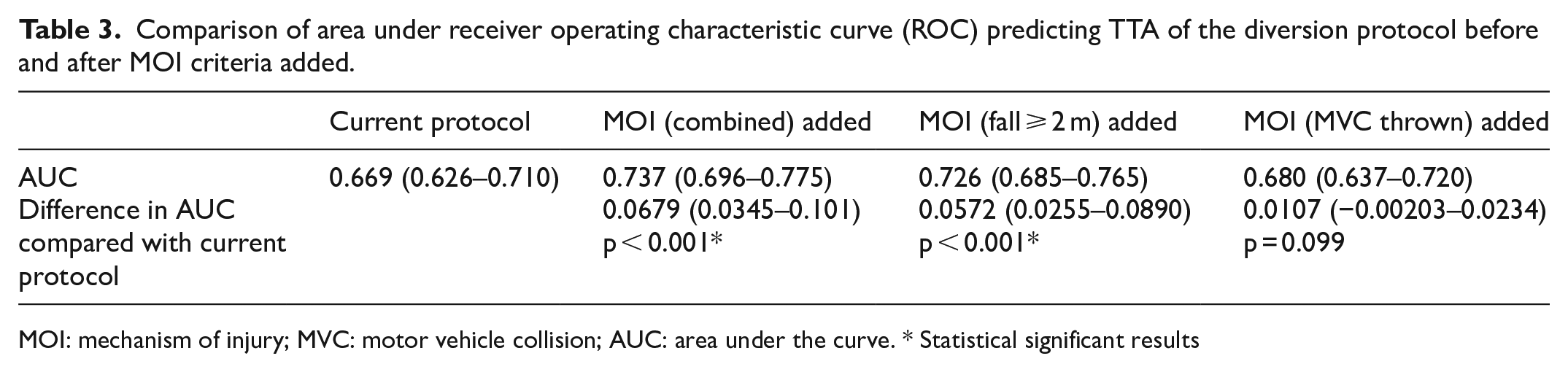
MOI: mechanism of injury; MVC: motor vehicle collision; AUC: area under the curve. * Statistical significant results
Figure 5 showed the comparison of ROC curve for predictive need for TTA.
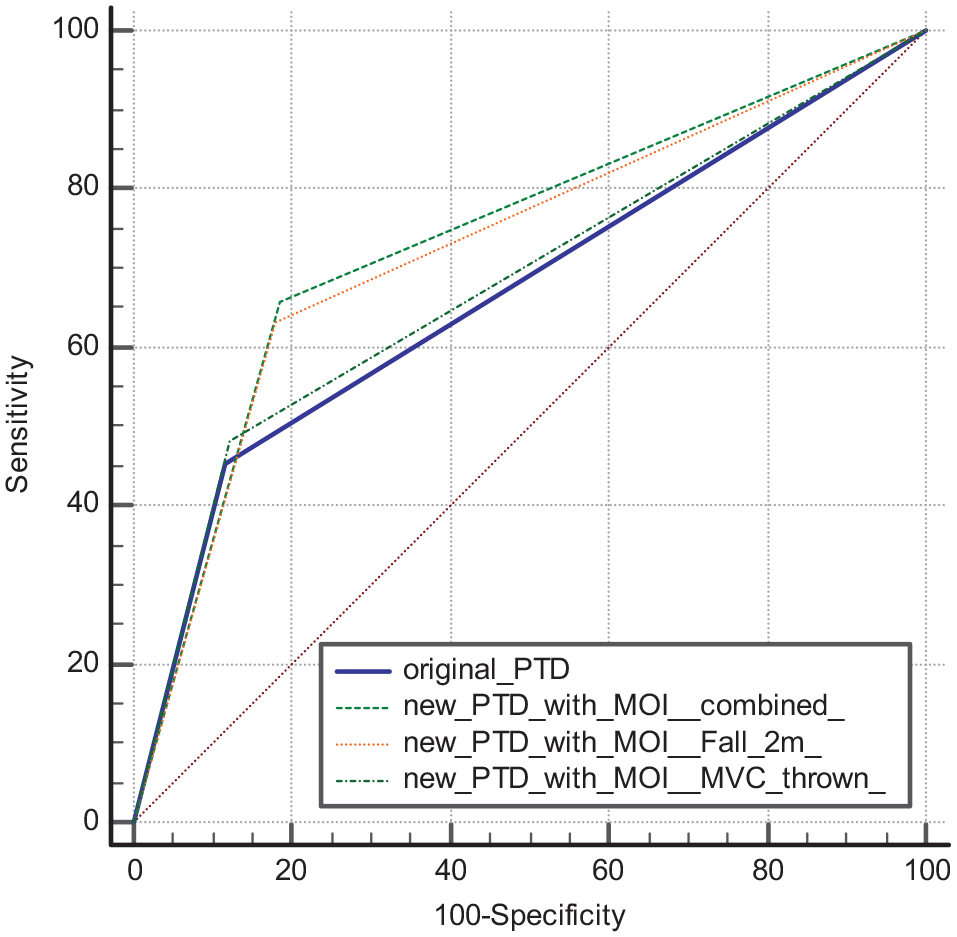
Comparison of receiver operating characteristic (ROC) curve for predictive need for TTA.
The net reclassification improvement index was 0.2828 (95% CI = 0.1519–0.4137; p = 0.013), and the integrated discrimination improvement index was 0.0806 (95% CI = 0.05–0.1112; p < 0.001). Both indices indicate that the addition of MOI criteria would improve the model’s discriminatory and predictive capacity.
Secondary outcome
Comparison of AUC of ROC curve after adding MOI criteria with current protocol predicting mortality, ICU/HDU admission, ISS > 15 as indicators of severity was shown in Table 4. Hypothesis testing for the difference in AUC revealed no statistically significant difference between current protocol before and after combined MOI criteria or fall ⩾ 2 m only criteria were added in predicting mortality, ICU/HDU admission or ISS > 15. There was a reduction in AUC of ROC curve predicting mortality after MVC thrown criteria alone were added compared with current protocol that were statistically significant (diff AUC, 0.00717, p = 0.008).
Comparison of area under the receiver operating characteristic curve (ROC) predicting secondary outcome of the diversion protocol before and after MOI criteria added.
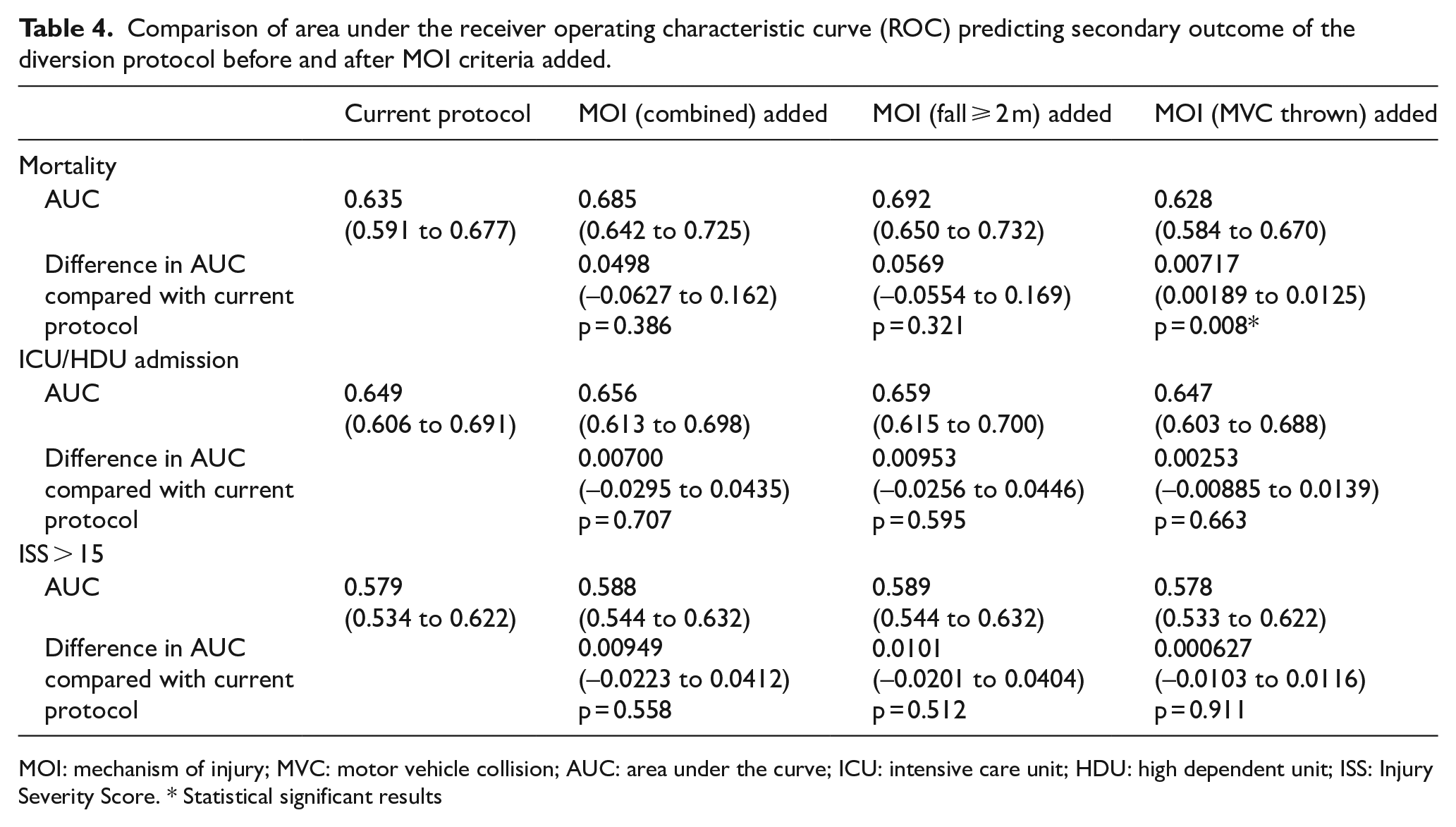
MOI: mechanism of injury; MVC: motor vehicle collision; AUC: area under the curve; ICU: intensive care unit; HDU: high dependent unit; ISS: Injury Severity Score. * Statistical significant results
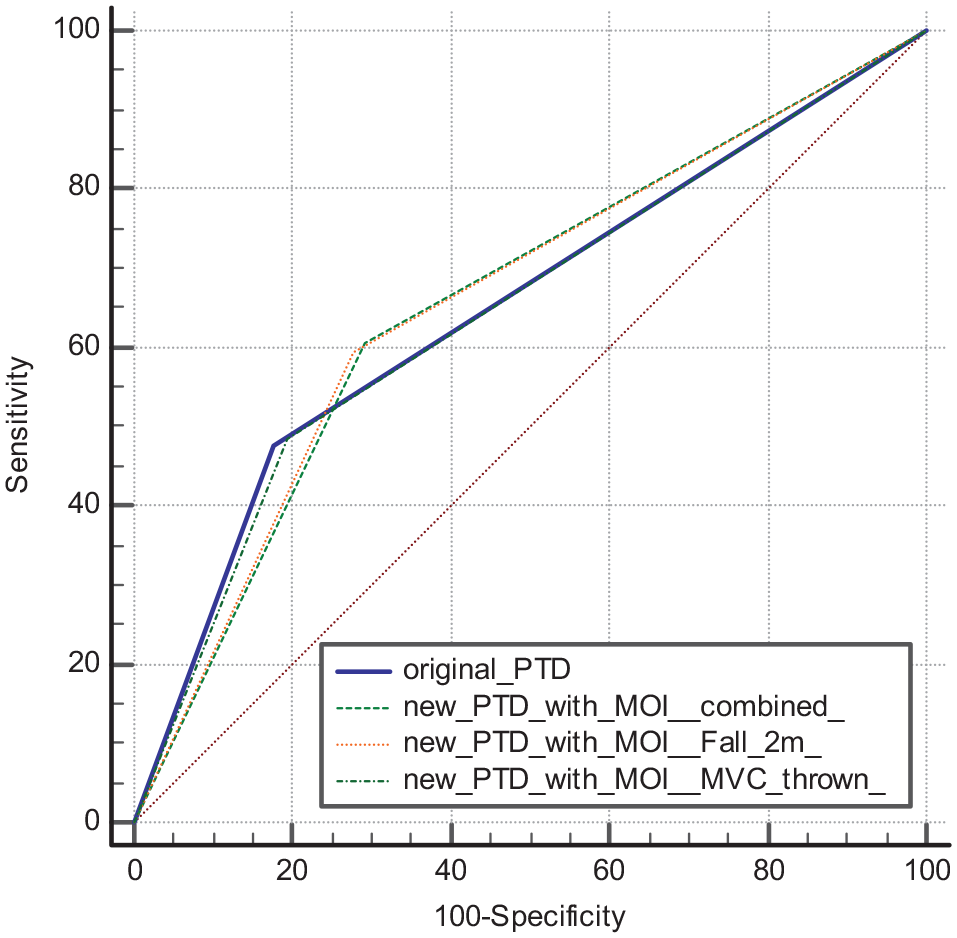
Figures 6 to 8 showed the comparison of ROC curve for secondary outcome.

Comparison of receiver operating characteristic (ROC) curve for predicting mortality.
Comparison of receiver operating characteristic (ROC) curve for predicting ICU/HDU admission.
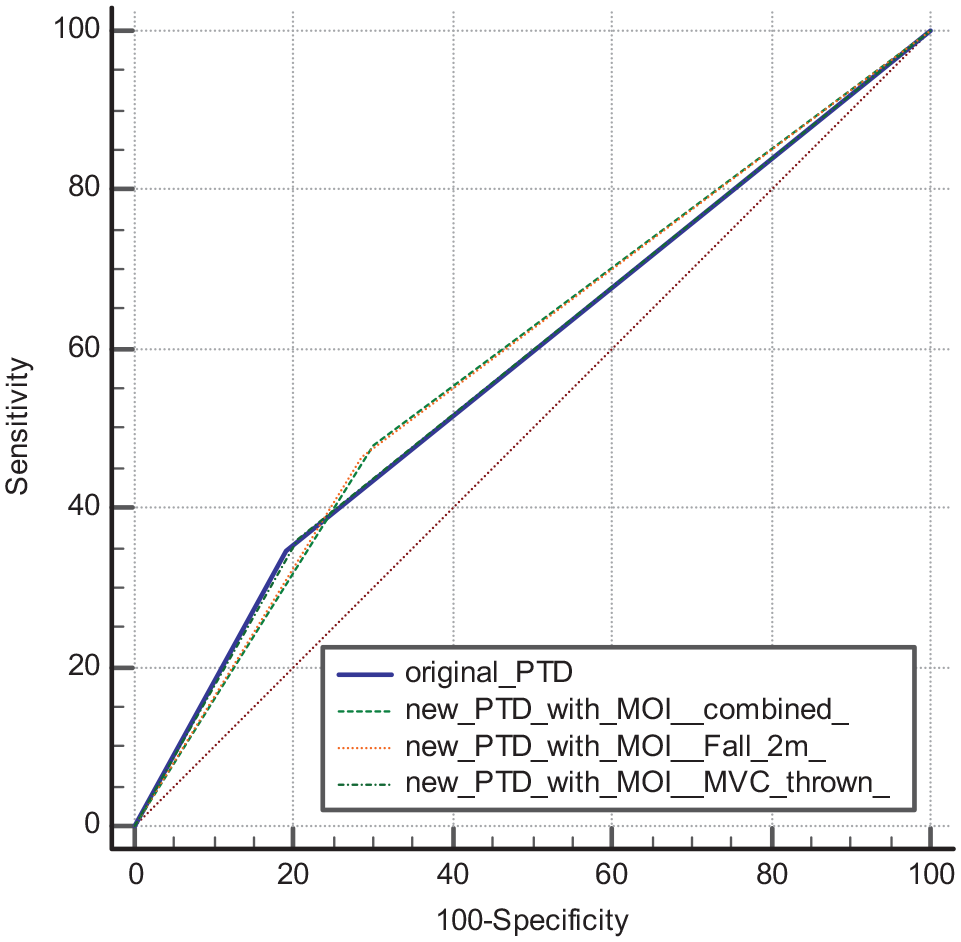
Comparison of receiver operating characteristic (ROC) curve for predicting ISS > 15.
Discussion
We compared the ROC curves for predicting trauma team activation in current diversion protocol and after MOI criteria were added. Our study showed a statistically significant increase in AUC (0.0572, p < 0.001) after fall ⩾ 2 m criteria were added. Although the increment of AUC (0.0107, p = 0.099) after adding MVC thrown criteria were not statistically significant, combining it with fall ⩾ 2 m as combined MOI criteria further increase the AUC (diff. AUC, 0.0679, p < 0.001). Under-diversion rate was much improved (from 54.7% to 34.3%) while Over-diversion rate was similar (from 31.1% to 33.1%). The American College of Surgeons suggested that the overall acceptable level of over-diversion is 25% to 50% and an under-diversion rate of 5% or less. Although our methodology was different from the one adopted by the ACS-COT, the concept of reducing under-diversion to minimise delay in definitive management in trauma centre was evident, thereby reducing morbidity and mortality. There is no perfect trauma diversion protocol but adding MOI criteria could improve its under-diversion rate without much increase in over-diversion rate. This showed that the two MOI criteria in our study were highly selected. This is important that addition of MOI criteria minimises the additional workload incurred in the trauma centre while identifying more patients who would need trauma centre level of care.
We also compared the AUC of ROC curve predicting secondary outcomes as indicators of severity. Our result demonstrated the severity of patient in terms of mortality, ICU/HDU admission, and ISS > 15 having a trend of higher AUC after adding both MOI criteria, but the difference was not statistically significant. There was paradoxical decrease in AUC predicting mortality after inclusion of vehicle ejection into the criteria. But the difference was quite small (difference in AUC = 0.00717, p = 0.008) and may not be clinically significant. The severity of the additional cases picked up by vehicle ejection criteria may not differ much clinically to other cases picked up by the current diversion protocol. It may still worth adding this criterion, and further study can elaborate more on its severity.
Literature review regarding the role of MOI in trauma diversion showed conflicting results. There is heterogeneity in definition of the need for trauma centre level of care, making comparison between previous studies difficult. In several studies, it has been defined as a composite measure of whether the patient had urgent non-orthopaedic surgery within 24 h, admission to ICU/HDU, mortality. 9 ISS greater than 15 is also a common surrogate indicator of need for a trauma centre. There is no consensus definition. In our study, trauma team activation was chosen as a practical indicator of need of trauma centre level of care. It should be better in reflecting practical needs. Also, most of the studies were done in foreign countries. The results may not directly apply to local prehospital situation. There was paucity of local study looking at the effect of adding MOI criteria to current diversion protocol. Moreover, most of the studies evaluating role of MOI criteria in diversion protocol looked at MOI criteria alone and did not evaluate its use after identifying those patients who met the first two steps of the field triage criteria (i.e. the physiologic and anatomic steps). 10
We studied only two selected MOI criteria among the many other criteria in the literature. The reason is obvious. For example, as we do not have accurate telemetry information of vehicle speed on injury scene, MOI criteria using vehicle speed may not be accurate. Death of passenger in the same compartment was found to be very rare on review and therefore not being used as criteria. Vehicle intrusion inches were not available in clinical record. MOI criteria had to be simple and objective for ambulance crew to assess to enough good compliance. Therefore, we choose fall ⩾ 2 m and pedestrian/cyclist/motorcyclist thrown after collision as MOI criteria.
Limitations
There are several limitations in this study. Only one region of Hong Kong was studied. There may be variability of results in different clusters in Hong Kong especially on the criteria of trauma team activation, service population size, geographical distance from injury scene to hospital, and so on.
Due to the retrospective nature of study, there may be missing information in the clinical record and trauma registry which could have affected the results. The determination of compliance issue of diversion protocol was based on record in trauma registry which was determined by trauma nurse on monthly review. This may also affect the accuracy. The better way we are doing now is to discuss the cases in monthly trauma meeting and communicate with fire department for feedback. Future studies may present a more accurate noncompliance rate. The noncompliance rate in our study is 9.7% which is compatible with the clinical observation from our trauma team meeting. This is better than that of 25.5% quoted in a previous study published in 2013 in our cluster. 11 This could be due to the increased familiarity of ambulance crew to the diversion protocol.
Our secondary outcome analysis showed a trend of higher AUC after adding combined MOI criteria but failed to show statistically significant. It could be due to sample size or inadequate power problem. A larger sample or multicentre study may better address this issue. There is also limitation of using ICU/HDU admission as one of the surrogates of severity as this is also affected by resources availability issue.
Our study focused on MOI only and aimed to demonstrate that adding certain MOI criteria can improve the performance of diversion protocol. However, there are other special factors adopted in the field triage guideline of The American College of Surgeons Committee on Trauma (ACS COT) our study did not investigate, like extremity of age, anticoagulants use, pregnancy > 20 weeks, end staged renal failure requiring dialysis, and so on. Future studies may further analyse the benefit of adding these factors in additional to anatomical, physiological and MOI criteria.
As mentioned in the discussion session, there were heterogeneity in definition of the need of trauma centre level of care in previous trauma diversion literatures. It was difficult in deciding on a perfect primary outcome. Trauma team activation was one of the factors assessing the usefulness of trauma diversion. It was therefore chosen as the primary outcome in our study. Other outcomes such as mortality, ICU/HDU admission, trauma score, massive blood transfusion, and so on may also have their own limits. For example, mortality may just be part of the reasons reflecting trauma centre need. There may be other reasons warranting trauma centre care, like interventional radiology facilities, speciality care such as neurosurgery, thoracic surgery, and so on. ICU/HDU admission could be limited by resources factors. Trauma score has intrinsic limitations. Even composite outcome may not be a good solution as a significant composite outcome does not mean individual outcome is significant.
There are several limitations of using trauma team activation as primary outcome. First, different clusters have different trauma team activation criteria though in general they are similar. This may limit external validity. Second, clinicians have clinical judgement. In general, clinicians follow the guidelines with rare exceptions. But subjectivity could be a limitation.
Last but not least, there are intrinsic limitations in any statistical methods. C statistics in AUC comparison is an insensitive measure of improvement in model accuracy. Large odds ratio or relative risks may be needed to achieve significant increase in C statistics. Also, it does not measure a clinically meaningful quantity on adding a proposed predictor, that is, how many cases are being risk stratified correctly. Net reclassification improvement index and integrated discrimination improvement index can give additional information. However, one concern of NRI/IDI is that it puts equal weights for sensitivity and specificity. In prehospital trauma diversion, the tolerance of under-diversion is much less than over-diversion. The improvement of overall accuracy may not necessarily reflect a better clinical model in this sense. Therefore, the over-diversion and under-diversion rates were also reported in the study.
Conclusion
The trauma diversion protocol currently in use in Hong Kong is not accurate enough. Anatomical and physiological criteria alone are probably inadequate to ensure appropriateness of trauma diversion. Addition of MOI criteria can improve performance of trauma diversion.
Footnotes
Acknowledgements
We would like to thank Mr. Jay Huang, New Territories West Cluster research office statistical officer, for his advice on statistics in this research.
Author contributions
The author alone was responsible for the content and writing of the paper. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data
The data sets generated and/or analysed during the current study are available from trauma registry of NTWC.
Informed consent
Written informed consent was not necessary because no patient identity data have been included in the manuscript.
Ethical approval
Ethical approval for this study was obtained from the New Territories West Cluster Research Ethics Committee (NTWC/REC/21043).