
Abstract
Background:
Hong Kong Poison Information Centre publishes annual reports on all poisoning cases received by the Centre in that year since 2006. However, there is little data about acute poisoning cases requiring intensive care unit admissions in Hong Kong.
Objective:
To report and analyze the 10-year poisoning data of acute poisoning patients presenting to an Accident and Emergency Department requiring intensive care in a regional hospital of Hong Kong.
Methods:
This was a retrospective study on patients presented from January 2007 to December 2016. These cases were retrieved from Clinical Data Analysis and Reporting System of the Hospital Authority, Hong Kong. Clinical data of these cases were then retrieved from patients’ electronic records.
Results:
A total of 270 cases were analyzed during the period. There were 152 (56.3%) male patients and 118 (43.7%) female patients. The middle aged group (age 30–39 and age 40–49) constitutes nearly half (48.6%) of all these admissions. Around 50% of them had history of psychiatric illness. Nearly 40% of them were known substance abusers. Majority of the patients (66.7%) were admitted directly from Accident and Emergency Department. The commonest cause was suspected self-harm (56.3%). When ethanol (13%) was excluded, the five commonest types of poisons were benzodiazepine (26.3%), opioids (20.7%), zopiclone (18.5%), carbon monoxide poisoning (13%), and household products (10.7%). Twenty-seven patients (10%) had decontamination done in Accident and Emergency Department or Emergency Medicine Ward. 112 patients (41.5%) were given one or more antidotes in Accident and Emergency Department and Emergency Medicine Ward. Altered mental status was the most frequently found complications (72.2%) in these patients. 76 patients (28.1%) required endotracheal intubation in Accident and Emergency Department. The length of stay in Intensive Care Unit ranged from 1 to 7 days with an average of 2.1 days. There were 25 deaths (9.3%) and 31 patients with major effects (11.5%).
Conclusion:
An estimate of 9.4% of acute poisoning patients presenting to Accident and Emergency Department might need Intensive Care Unit care at certain stage of their hospital stay. Benzodiazepine, opioids, zopiclone, carbon monoxide poisoning, and ethanol were the top five poisons in our series from 2007 to 2016. The mortality rate (9.3%) was high in our series given that there were more substance abusers.
Introduction
Acute poisoning patients presented to Accident and Emergency (A&E) Departments in different ways. Majority of them were young adults. 1 Most patients required only supportive measures and had an uneventful recovery. 1 However, significant number of these patients needs intensive care. Nogue et al. 2 found that only 5% of intoxicated patients treated in emergency departments required admission to Intensive Care Unit (ICU). Acute poisoning patients constituted about 3.5% of intensive care admissions in Lam et al.’s 3 series from 2000 to 2008 in Hong Kong. Benzodiazepine (25.3%), alcohol (23%), tricyclic antidepressant (17.4%), and carbon monoxide (CO; 15.1%) were the four commonest poisons encountered in their series. The mortality rate for acute poisoning patients admitted to ICU was about 3.5%–9% in different studies.2–4
In Hong Kong, clinical toxicology was formally established as a new specialty under Hong Kong College of Emergency Medicine in 2016. Training in clinical toxicology is expected to be more structured and acute poisoning patients in A&E Departments might receive more supportive and specific treatments before hospital admissions. Patients with life-threatening conditions would be admitted to ICU while others might be admitted to Emergency Medicine Ward (EMW) under care by emergency physicians in certain hospitals.
While changes were gradual, we presented the 10-year profile of acute poisoning patients presenting to an A&E department requiring intensive care in a regional hospital of Hong Kong. This study described the pattern of acute poisoning that warranted ICU admissions and the characteristics and outcomes of these patients. It may serve as a baseline for future comparison after the establishment of clinical toxicology specialty.
Methods
This was a retrospective observational study. All acute poisoning patients attending the A&E Department of a regional hospital who required adult ICU care any time during the hospital stay were included in the study. The hospital is an acute general hospital with around 1200 beds situated in the west part of Kowloon area of Hong Kong. It provides 24-h comprehensive emergency service with 10 ICU beds to around 500,000 populations in the area. The A&E Department received an average of 360 patients per day with 25%–30% being ambulance patients. We started bimonthly Toxicology Audit Meeting since November 2010. We had on average 286 acute poisoning patients each year (0.2% of all A&E attendances). Among them, about 20–30 patients were admitted directly to ICU after consultation in A&E each year.
We used the same definition of poisoning as in Lam et al.’s 3 study. Poisoning was defined as exposure to an agent capable of producing a deleterious response in an individual 5 or to a drug at a dosage exceeding that normally used for human in the prophylaxis, diagnosis, or therapy of disease. 6 The Clinical Data Analysis and Reporting System (CDARS) of the Hospital Authority, Hong Kong was used to generate a list of all admissions to ICU from January 2007 to December 2016 with the following diagnostic coding using International Classification of Diseases, Ninth Revision (ICD9):
292.2 (pathological drug intoxication);
292.8 (other specified drug-induced mental disorders);
292.9 (unspecified drug-induced mental disorder);
294.1(32) (dementia related to drug intoxication);
294.1(33) (dementia related to nonmedicinal substance intoxication);
303.0 (acute alcoholic intoxication);
305 (nondependent abuse of drugs);
E805–E858 (accidental poisoning (drugs));
E860–E869 (accidental poisoning (other substances));
E950 (suicide and self-inflicted poisoning by solid or liquid substances);
E951 (suicide and self-inflicted poisoning by gases in domestic use);
E952 (suicide and self-inflicted poisoning by other gases and vapors);
E961 (assault by corrosive or caustic substance, except poisoning);
E962 (assault by poisoning);
E980 (poisoning by solid or liquid substances, undetermined whether accidentally or purposely inflicted);
E981 (poisoning by gases in domestic use, undetermined whether accidentally or purposely inflicted);
E982 (poisoning by other gases, undetermined whether accidentally or purposely inflicted).
This study was approved by the Research Ethics Committee of West Kowloon Cluster of Hospital Authority, Hong Kong. A total of 403 ICU admissions were identified from January 2007 to December 2016. The patient records were then retrieved from the Clinical Management System and the Electronic Patient Record system of the Hospital Authority. One hundred and thirty-three patient records were excluded from this study. The exclusion criteria included the followings:
Patients not admitted through A&E Department of the hospital (these patients were admitted clinically through other specialties to the hospital);
Patients whose age was below 18;
Patients admitted ICU for severe gastrointestinal bleeding or perforated peptic ulcer while on aspirin or non-steroidal anti-inflammatory drugs;
Patients admitted ICU for reasons not directly related to drugs or poisons but they were within this group because of drug-related liver injury (mild), the patient being a substance abuser, high INR as a result of warfarin interacting with other drugs, and mild hypoglycemia in diabetic patients;
Patients admitted ICU for serious physical injuries with concomitant insignificant poison effect like those in fire victims.
Data were retrieved from patients’ electronic records. The demographic characteristics (age, sex, marital status, residence before admission, chronic alcohol intake, history of psychiatric illness, and previous suicidal attempt) and details of intoxication (poisons involved, route of exposure, reason of exposure, history of poisoning in A&E, and whether the poisons were part of patient’s drug stock) were registered.
The decontamination methods (activated charcoal, gastric lavage, multiple dose activated charcoal, whole bowel irrigation, surface decontamination, dilution, and others) done in A&E and antidotes used in A&E were searched from scanned A&E records stored in the electronic record. The following complications during the hospital stay were looked for: rhabdomyolysis was defined as serum creatine kinase more than 1000 U/L; 7 acute renal failure was defined as serum creatinine more than 1.5 times of baseline; adverse cardiac events included myocardial injury, arrhythmias, conduction abnormalities, and cardiac arrest; shock was defined as hypotension with systolic blood pressure less than 90 mmHg; altered mental status was defined as Glasgow Coma Scale Score of less than 13 or with delirium; seizure; aspiration pneumonia as judged by the attending doctor.
Outcome parameters included invasive mechanical ventilation, length of stay in ICU and in acute hospital (excluding those days in psychiatric unit). The clinical outcome was classified according to the yearly reports of Hong Kong Poison Information Centre (HKPIC) 8 into death, major effect (life-threatening or significant residual disability or disfigurement), moderate effect (more pronounced signs or symptoms requiring some form of treatment and no residual disability or disfigurement), mild effect (minimally bothersome signs or symptoms which resolved rapidly), and no effect.
Data were expressed as number (percentage). Continuous variables will be categorized or expressed using mean, median, and inter-quartile range (IQR). Categorized data were evaluated using the Fisher exact test. All tests were two-tailed and a p value of less than 0.05 was considered to be statistically significant.
Results
During the study period, there were a total of 403 ICU admissions retrieved from the list of diagnostic coding related to poisoning. After excluding 133 admissions with ICU admissions not related to acute poisoning, we had a total of 270 patient episode admissions for analysis. The demographic characteristics are shown in Table 1. There were 152 (56.3%) male patients and 118 (43.7%) female patients. There was a slight male preponderance in majority of age groups except in age groups 20–29 and 60–69. Concerning the age distribution, the middle aged group (age 30–39 and age 40–49) constitutes nearly half (48.6%) of all these admissions. The age ranged from 18 to 89 with average 41.4, median 36.5, and IQR 27.5–53.25. For the marital status, majority were single and never married (37%) and 25.6% were married but living separately (6.7%) or divorced (15.6%) or widowed (3.3%). Around one-third of them were married and living together. About 60% of these patients lived with one or more members of the family while one-fourth lived alone. Only 24.4% of the patients were chronic drinker and majority of them were either nondrinkers (48.9%) or social drinkers (20%). Around 50% of them had history of psychiatric illness which was defined as having history of psychiatric follow-up or taking psychiatric medications. Among them, 30% (39/129) was diagnosed to have schizophrenia or related psychotic disorder. Nearly 40% of patients were known substance abusers and 43.7% had previous history of drug overdose or poisoning requiring admissions to public hospitals. Table 1 also shows the source of ICU admissions. Majority of the patients (66.7%) were admitted directly from A&E after initial stabilization and ICU consultation. 24.8% were admitted first to Medical Ward from A&E before they were transferred to ICU. A significant number of the patients were transferred to ICU from our EMW which was a ward operated solely by emergency physicians.
Demographic characteristics of patients and source of ICU admissions.
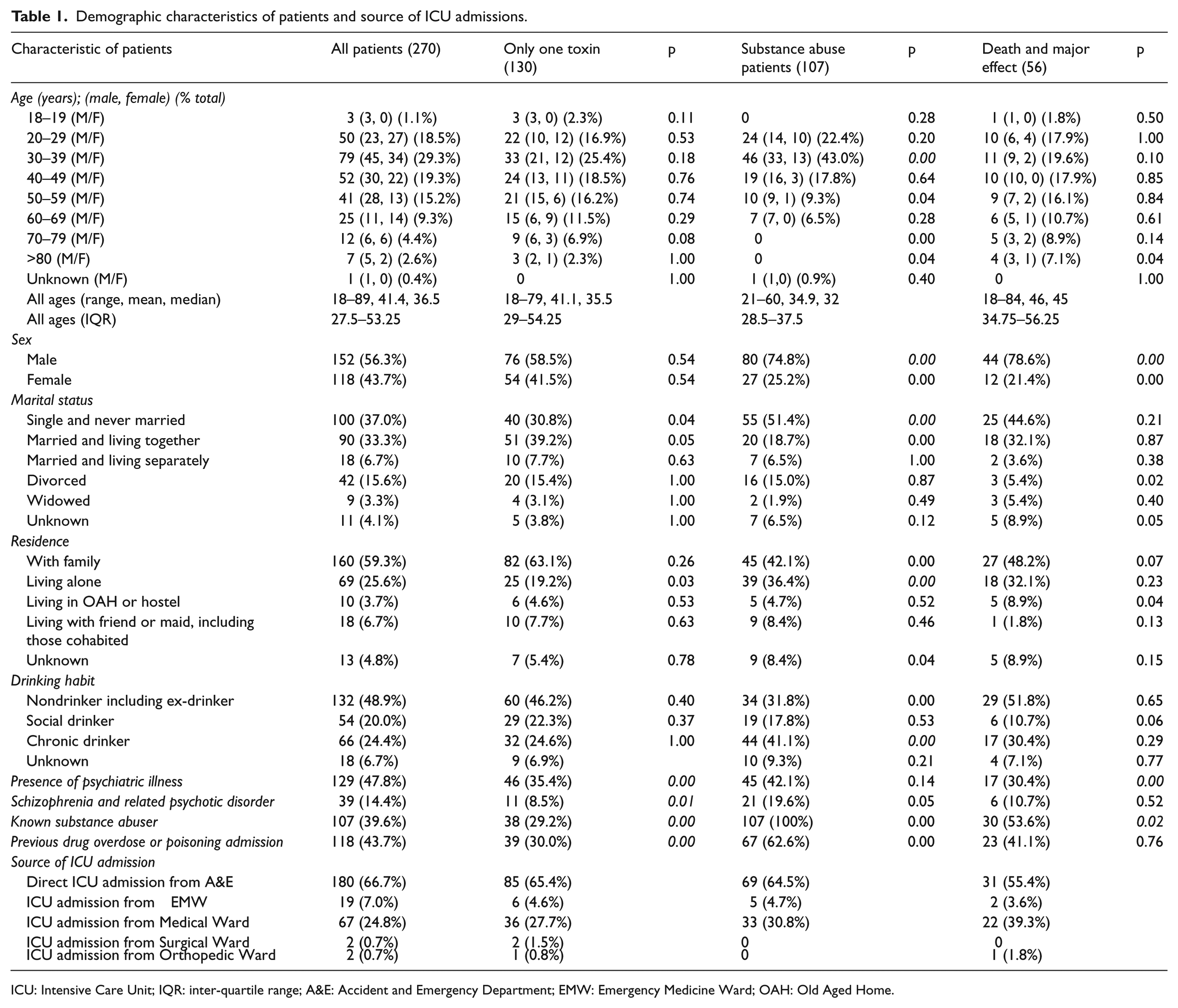
ICU: Intensive Care Unit; IQR: inter-quartile range; A&E: Accident and Emergency Department; EMW: Emergency Medicine Ward; OAH: Old Aged Home.
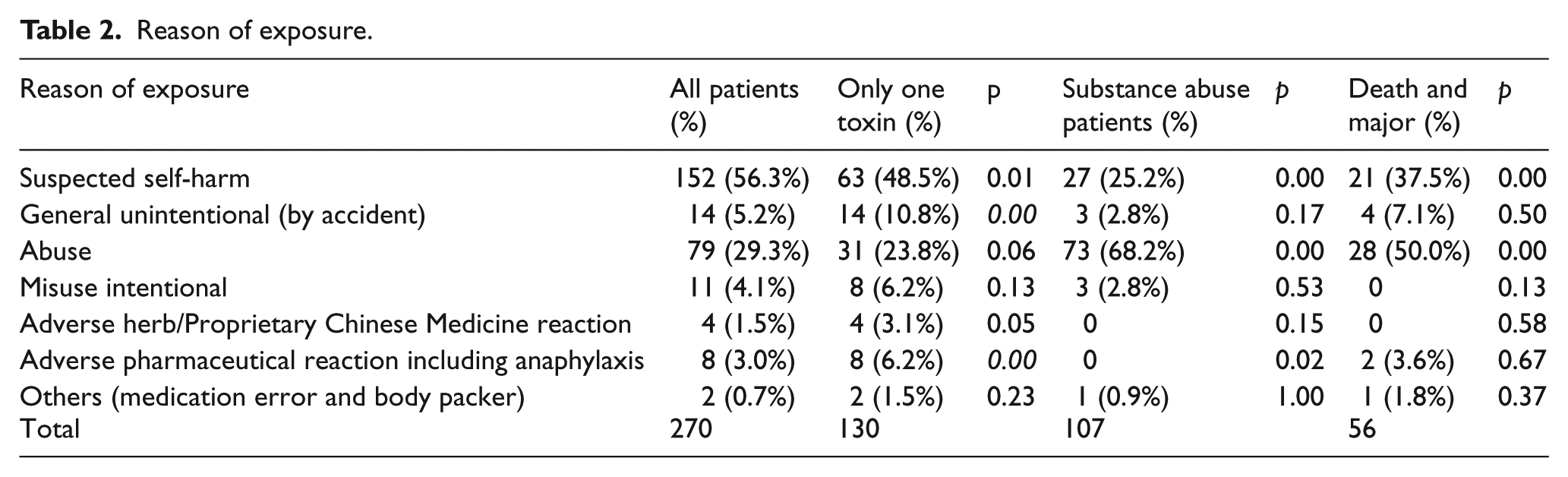
The reasons for poisoning are listed in Table 2. The commonest cause was suspected self-harm (56.3%). Poisoning due to abuse ranked the second (29.3%). General unintentional (5.2%) and misuse intentional (4.1%) ranked the third and the fourth. These four commonest reasons for exposure contributed to the vast majority of our cases (94.8%). Table 3 shows the place of exposure. The commonest place of exposure was in a residential place (69.6%) which was usually the patient’s home and in few cases in friend’s home. The next commonest place of exposure in these patients was in public places (21.5%) including streets, public toilets, and other public facilities. In Table 4, for route of exposure, majority were oral exposure (64.8%) and the rest were inhalation (19.3%), parenteral (14.1%), and insufflation (1.9%).
Reason of exposure.
Place of exposure.
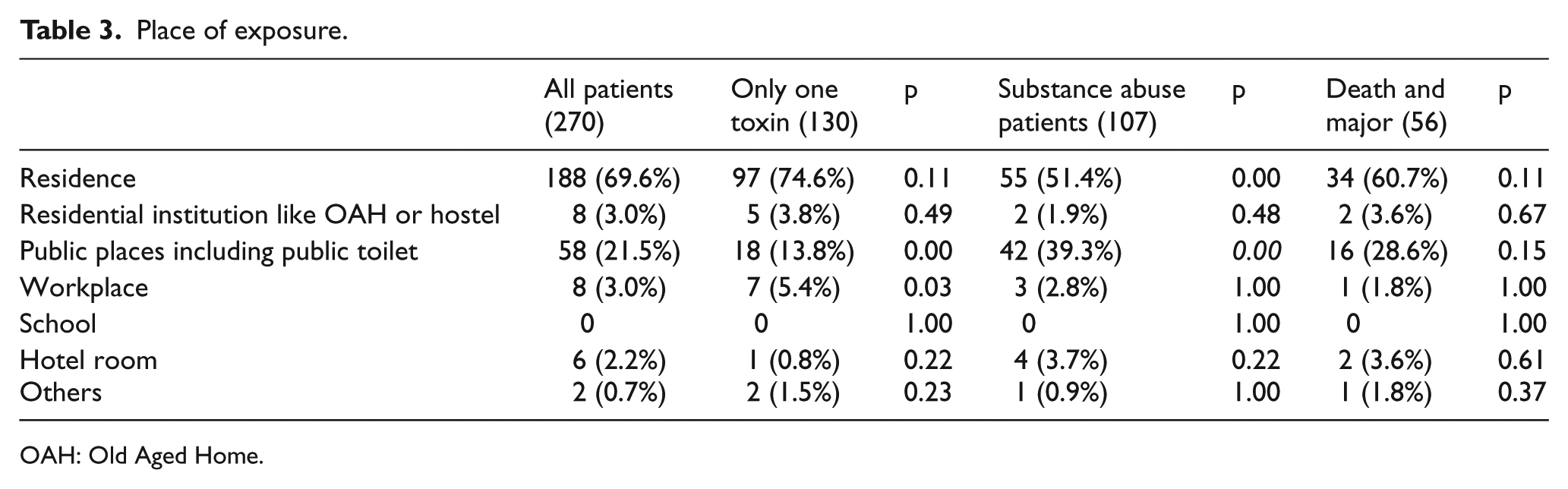
OAH: Old Aged Home.
Route of exposure.
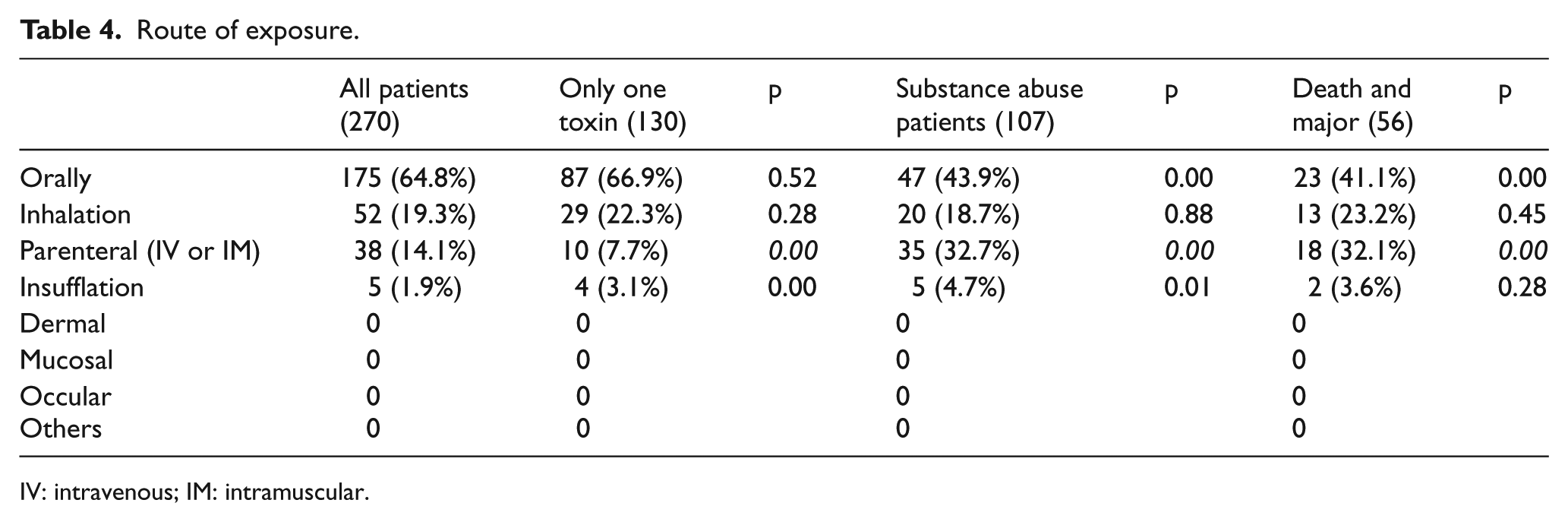
IV: intravenous; IM: intramuscular.
A total of 570 poisons which are listed in Table 5 were identified in our 270 patients. In total, 130 out of 270 patients (48.1%) had exposed to alcohol alone or a single poison other than alcohol. The types of poisons were classified according to the annual reports of HKPIC. 8 Ethanol was found in 35 (13%) patients. Twenty patients out of these 35 patients were purely drunk requiring ICU admissions with no other poisons found. When ethanol was excluded, the five commonest types of poisons (Table 6) were benzodiazepine (26.3%), opioids (20.7%), zopiclone (18.5%), CO poisoning (13%), and household products (10.7%). For poisoning involving only one poison excluding ethanol, the six commonest poisons (Table 6) were household products (13.8%), CO poisoning (13.1%), opioids (7.7%), zopiclone/ketamine/tricyclic antidepressants (5.4% each).
Drugs and toxins encountered.
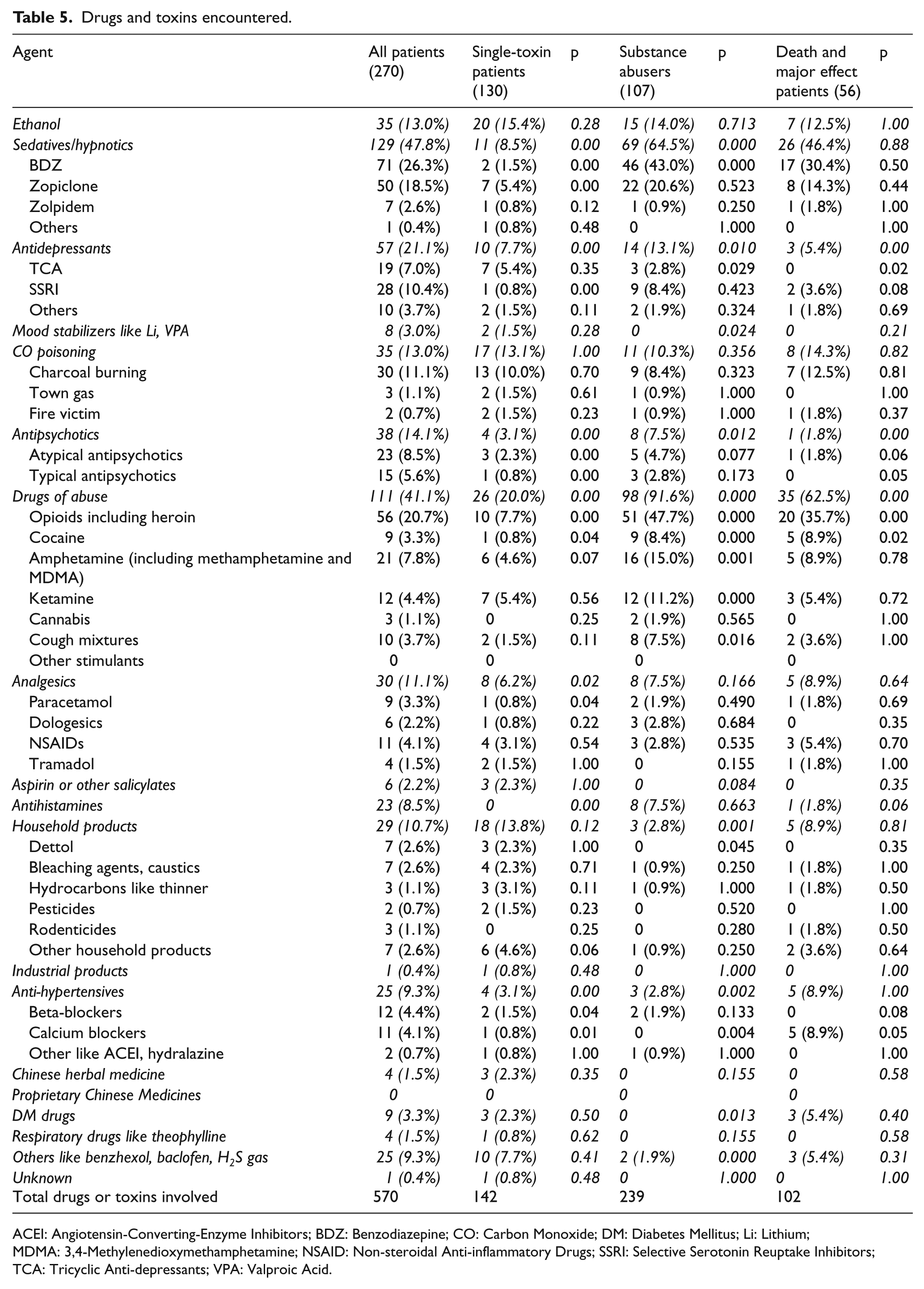
ACEI: Angiotensin-Converting-Enzyme Inhibitors; BDZ: Benzodiazepine; CO: Carbon Monoxide; DM: Diabetes Mellitus; Li: Lithium; MDMA: 3,4-Methylenedioxymethamphetamine; NSAID: Non-steroidal Anti-inflammatory Drugs; SSRI: Selective Serotonin Reuptake Inhibitors; TCA: Tricyclic Anti-depressants; VPA: Valproic Acid.
Ranking of poisons.
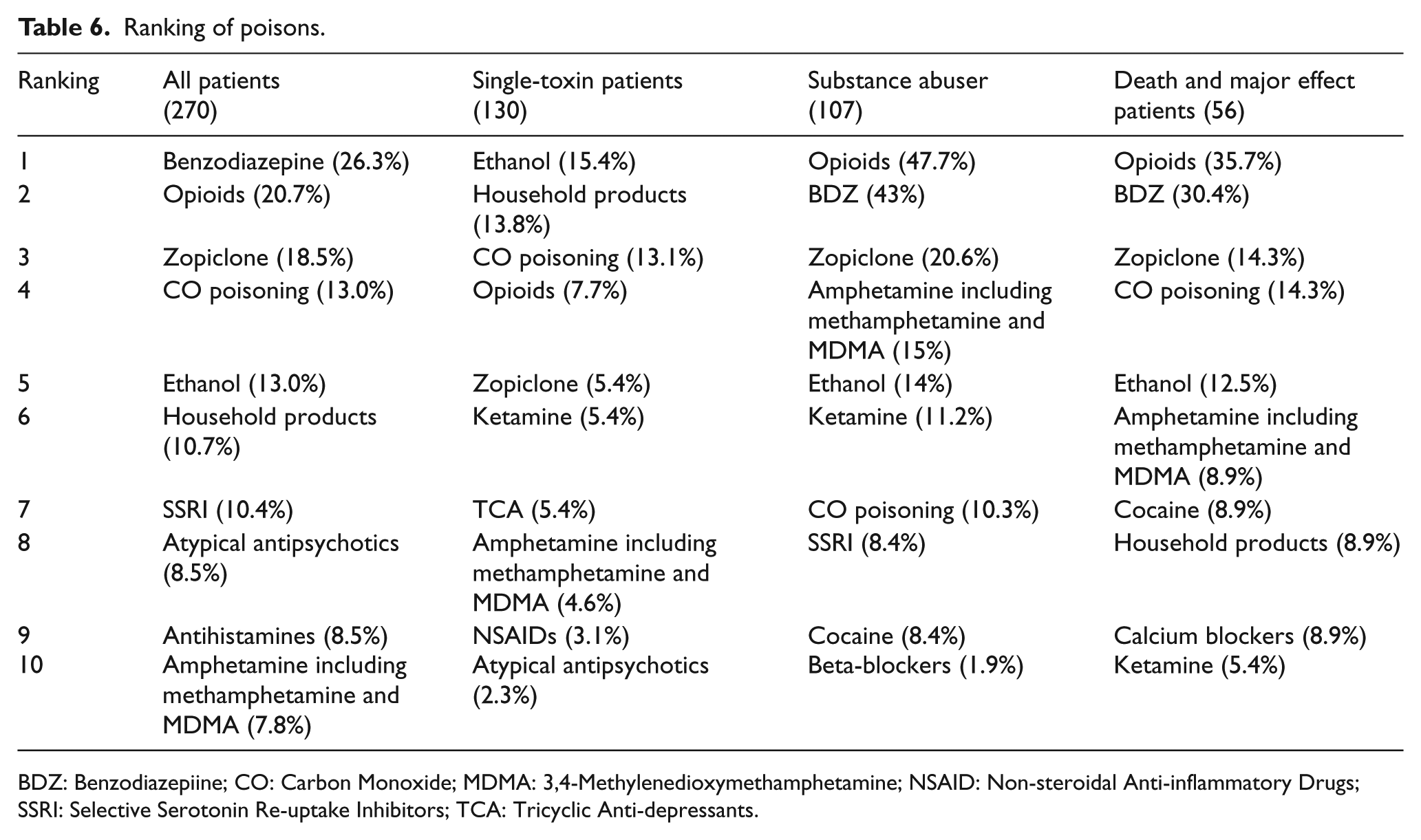
BDZ: Benzodiazepiine; CO: Carbon Monoxide; MDMA: 3,4-Methylenedioxymethamphetamine; NSAID: Non-steroidal Anti-inflammatory Drugs; SSRI: Selective Serotonin Re-uptake Inhibitors; TCA: Tricyclic Anti-depressants.
For decontamination methods and antidotes used in A&E or EMW (Table 7), 27 patients (10%) had decontamination done. Eight of them received more than one decontamination methods. The commonest method was single-dose activated charcoal (85.2% of patients with decontamination done), followed by gastric lavage (37.0%) and dilution, irrigation, washing (7.4%). One patient with slow K and other psychiatric medicine overdose underwent three decontamination methods including whole bowel irrigation in A&E. Starting from November 2010, poisoned patients may be given activated charcoal by ambulance crew after consulting HKPIC in the prehospital phase. In this study, there were a total of three patients received a dose of 50 g of activated charcoal before A&E arrival. For these three patients, no further decontamination methods were given in A&E. Regarding the antidotes used in A&E and EMW (Table 8), 112 patients (41.5%) were given a total of 149 antidotes and 29 patients (10.7%) received more than one antidote in A&E and EMW. The six commonly used antidotes were benzodiazepines (47, 31.5% of total 149 antidotes used), naloxone (43, 28.9%), sodium bicarbonate (16, 10.7%), dextrose for hypoglycemia (10, 6.7%), atropine (7, 4.7%), and flumazenil (7, 4.7%).
Decontamination methods used in A&E or EMW.
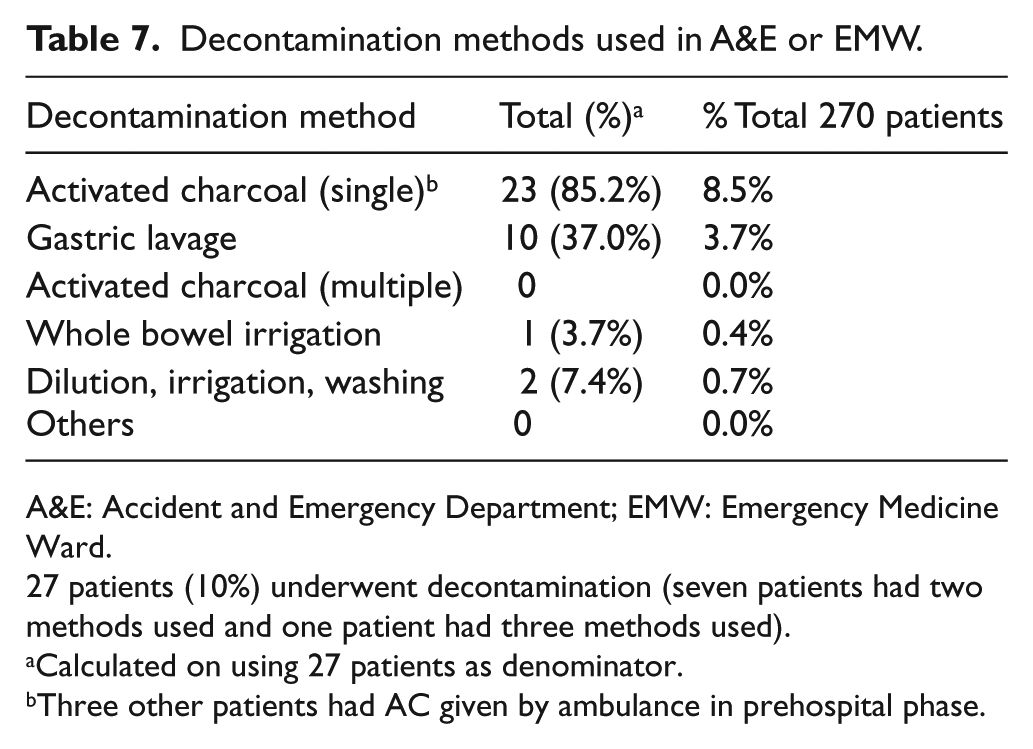
A&E: Accident and Emergency Department; EMW: Emergency Medicine Ward.
27 patients (10%) underwent decontamination (seven patients had two methods used and one patient had three methods used).
Calculated on using 27 patients as denominator.
Three other patients had AC given by ambulance in prehospital phase.
Antidotes used in A&E or EMW.
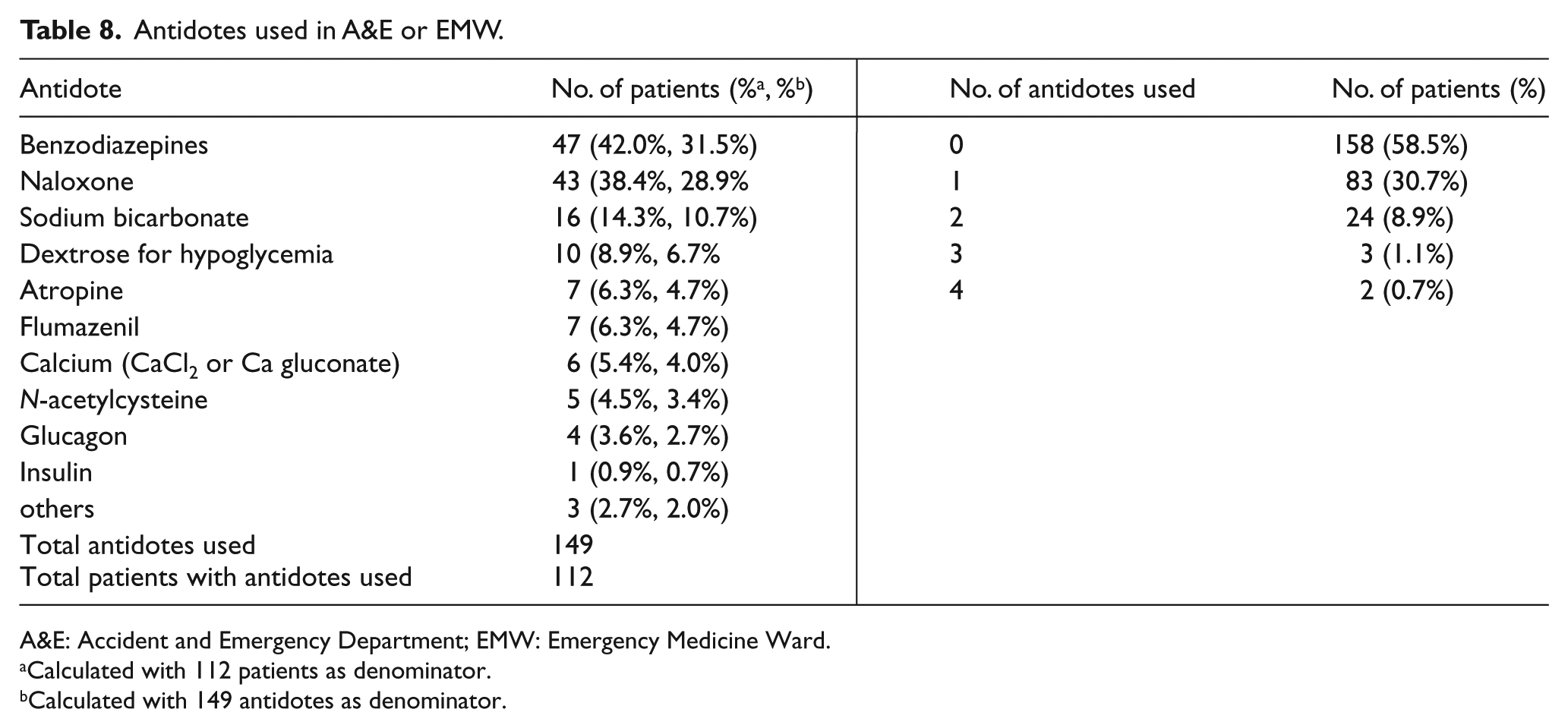
A&E: Accident and Emergency Department; EMW: Emergency Medicine Ward.
Calculated with 112 patients as denominator.
Calculated with 149 antidotes as denominator.
The complications that developed among these patients are shown in Table 9. Altered mental status was the most frequently found complications (72.2%). The other complications encountered by our patients included acute renal failure (29.3%), aspiration pneumonia (26.7%), shock (25.9%), and rhabdomyolysis (23.3%). Significant amount of patients had seizure (13%) and adverse cardiac events (10.7%). A total of 23 patients who ingested caustics or other household or industrial cleaners ended up with nine gastrointestinal tract damages. These complications were more significantly found in those patients ended up with death or major effects. Seventy-six patients (28.1%) required endotracheal intubation in A&E while 77 patients (28.5%) had endotracheal intubation done after admission to ICU or other specialties. One hundred and seventeen patients (43.3%) did not require mechanical ventilation during their stay in acute hospital.
Complications and patients requiring Endotracheal Intubation.
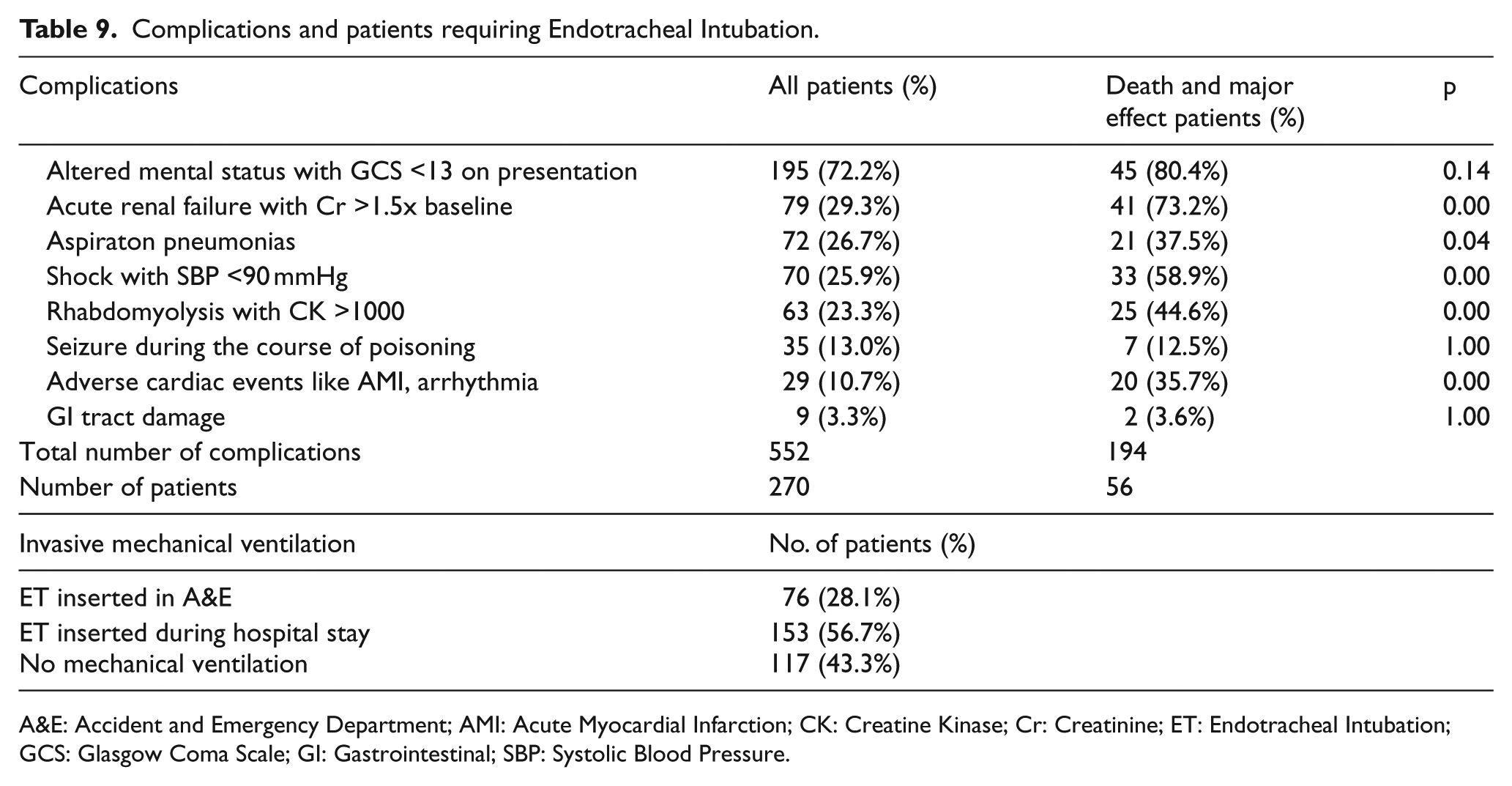
A&E: Accident and Emergency Department; AMI: Acute Myocardial Infarction; CK: Creatine Kinase; Cr: Creatinine; ET: Endotracheal Intubation; GCS: Glasgow Coma Scale; GI: Gastrointestinal; SBP: Systolic Blood Pressure.
Concerning the outcome of these patients (Table 10), the length of stay in ICU ranged from 1 to 7 days with an average of 2.1 days, a median of 1 day, and IQR 1–2.25 days. The length of stay of these patients in acute hospitals ranged from 1 to 210 days with an average of 9.4 days, a median of 5 days, and IQR 3–9 days. We adopted the definition of clinical outcome from the annual reports of HKPIC. 8 There were 25 deaths (9.3%), 31 patients with major effects (11.5%), and 214 patients with moderate effects (79.3%). In another words, 20.7% of our patients either died or ended up with major effects while 79.3% were discharged with no residual disabilities or disfigurement.
Outcomes.
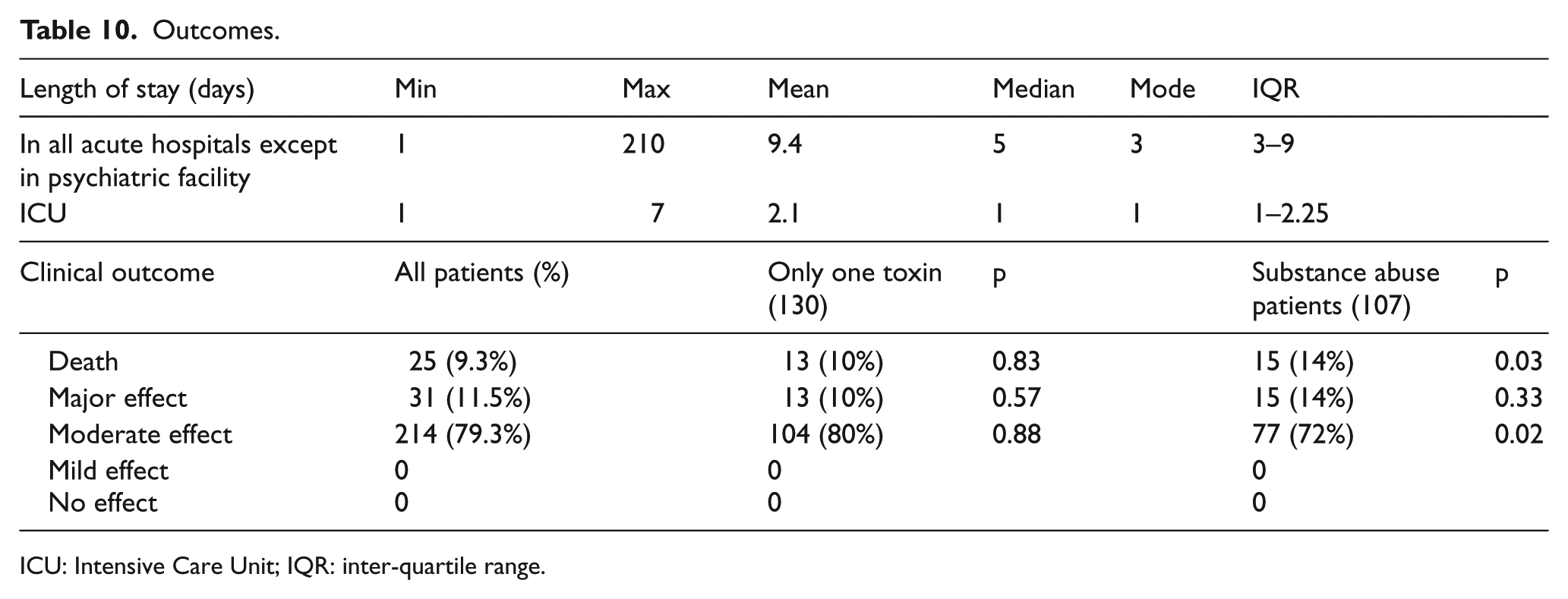
ICU: Intensive Care Unit; IQR: inter-quartile range.
We re-grouped our patients into three subgroups for analysis—group A patients were those involved with only one toxin as defined above; group B patients were those known substance abusers; group C patients were those ended up with death or major effects with disabilities or disfigurements. In group A, patients were involved with ethanol only or with one toxin other than ethanol. When compared with all patients in the study, there were more patients exposed to the toxin by accident (10.8% vs 5.2%, p < 0.001), and more patient suffering from adverse pharmaceutical reactions (6.2% vs 3.0%, p = 0.003). There were less patients with psychiatric illness (35.4% vs 47.8%, p < 0.001), less substance abusers (29.2% vs 39.6%, p = 0.001), less patients with previous drug overdose (30% vs 43.7%, p < 0.001), and less patients taking the poison parenterally (7.7% vs 14.1%, p = 0.004). From Table 6 about the ranking of toxins, the top five poisons involved were ethanol, household products, CO poisoning, opioids, and zopiclone in this subgroup.
For group B of substance abuser patients, there were significantly more patients in the age group of 30–39 (43% vs 29.3%, p < 0.001), more male patients (74.8% vs 56.3%, p < 0.001), more single and never married patients (51.4% vs 37%, p < 0.001), more patients living alone (36.4% vs 25.6%, p = 0.001), more chronic drinkers (41.1% vs 24.4%, p < 0.001), and more patients taking the poison parenterally (32.7% vs 14.1%, p < 0.001). These substance abusers were found poisoned more frequently in public places including public toilets (39.3% vs 21.5%, p < 0.001) than the whole series of patients, although more than half of them were still found in their residential places (51.4%). The top five poisons involved were opioids, benzodiazepines, zopiclone, amphetamines, and ethanol in this subgroup.
In group C with patients ended up with death or major effect, there were significantly more male patients (78.6% vs 56.3%, p < 0.001), more substance abusers (53.6% vs 39.6%, p = 0.02), more patients taking the poison by parenteral route (32.1% vs 14.1%, p < 0.001). However, there were less patients with psychiatric illness (30.4% vs 47.8%, p = 0.004). The top five poisons involved in this group were opioids, benzodiazepines, zopiclone, CO poisoning, and ethanol.
Discussion
In our study, there were a total of 270 A&E poisoning patients who required ICU care during their hospital stay. During the bimonthly toxicology audit meeting of our A&E since 2010, there was on average 286 acute poisoning patients presenting to our A&E each year. By extrapolation, it was estimated that there would be about 2860 acute poisoning A&E patients in this 10-year study period. This gave an average 9.4% (270/2860) of A&E acute poisoning patients who required ICU care at some stage during their hospital stay. Benzodiazepines, opioids, zopiclone, CO poisoning, and ethanol were the commonest poisons encountered. Majority of them were young (83.3% with age less than 60) and independent in activities of daily living. There was a preponderance of male (56.3%). Just less than half (47.8%) of our patients had history of psychiatric illness and 39.6% of them were known substance abusers. This contrasted with Lam et al.’s 3 study in 2010 which was done in another regional hospital on the eastern side of Hong Kong Island with better socioeconomic condition in their local population involving data from 2000 to 2008. In their study, they had a total of 265 patients with female preponderance (54.3%) in an 8-year period. Benzodiazepines, ethanol, tricyclic antidepressants, and CO poisoning were the commonest poisons. Their patients had a similar proportion of psychiatric illness history (47.9%) but substance abusers only constituted 18.4% (p < 0.001). This could be explained by the far lower socioeconomic condition of our local community served by our hospital. There were many intravenous drug addicts living in tiny subdivided units in our locality and the majority of them were male. This also explained why significant proportion (21.5%) of our patients was found overdosed in public places including the public toilets. Apart from the difference in the local community each hospital served, we observed a change in the poisoning pattern in Hong Kong. In Lam’s series, tricyclic antidepressant (TCA) was among the commonest four poisons while in our series, TCA was not within the top 10. Instead, we observed that zopiclone was the third commonest poison. This was most likely because tricyclic antidepressants were now replaced by other safer antidepressants while zopiclone known as white melon seeds among the public is widely available from our local community pharmacy and is increasingly used as sleeping pills and abused by the public.
From the annual report 2015 of HKPIC, 8 the five commonest types of poisons were paracetamol, benzodiazepine, household products, zopiclone, and Chinese herbal medicine. The difference with our ICU poisoning cases was explained by the fact that poisoning by paracetamol, household products, and Chinese herbal medicine usually would not present with altered mental status and majority of these cases could well be managed in our EMW with consultation from HKPIC.
Also in the annual report 2015 of HKPIC, 8 about three quarters of these cases (74.2%) had exposed to a single poison. In our series, only 130 patients (48%) had exposed to a single poison. Of interest is the poison, benzodiazepine which ranks the first poison ingested in all patients but only 2 out of 71 patients took benzodiazepine alone. Majority of these patients had mixed poisoning using benzodiazepine together with other poisons. This was particularly obvious for those substance abuse patients; 43% of substance abuse patients also took benzodiazepine (Table 5). Patients taking benzodiazepines alone were usually managed in our EMW without the need for ICU care.
Concerning the admission source of the patients, 66.7% of our patients had direct admission to ICU from A&E and this proportion was comparable with Lam et al.’s series of 63%. There were few patients who had ICU consultations in A&E but were then admitted to other wards because ICU needed time for bed re-arrangement. Other patients had deterioration in their clinical conditions after admission to the other wards from A&E and were subsequently transferred to ICU for close observation and intervention.
Decontamination was important in treating acute poisoning patients especially when they presented early. In our series, only 27 patients (10%) received decontamination in A&E and in our EMW with single-dose activated charcoal (85.2% of all decontamination methods used) being the commonest method used. Only three patients had activated charcoal given by ambulance crew in the prehospital phase. This makes up a total of 30 patients (11.1%) with decontamination done before ICU admission. The decontamination rate in the annual report 2015 of HKPIC 8 was 16.4%. Our relatively low percentage of decontamination might be partly explained by the lower oral route of exposure (82.4% in HKPIC audit vs 64.8% in our series) and partly explained by the delayed presentation in some of our cases. In this study, 45 patients (17%) presented to A&E within 1 h of drug overdose or poisoning. Definite poisoning history was only available in 170 cases (63%) while others did not have a clear cut poisoning history. However, in view that 76 patients (28.1%) had endotracheal intubation done in A&E, if decontamination was indicated in some of these cases, it would be safer to perform gastric lavage and to give activated charcoal when the airway of these patients was protected. With the relatively low decontamination rate of our patients in A&E, there may be room for improvement in the future. In fact, nine patients not given activated charcoals in A&E were given activated charcoals in ICU on admission. Majority of these patients were intubated.
Concerning the use of antidotes, 41.5% received antidotes in A&E and EMW with 10.7% having more than one antidote. This was much higher than that quoted in the annual report 2015 of HKPIC 8 (16.2% received antidote with 2.4% more than 1). The reason was obvious because our patients were more serious and required ICU admissions during their hospital stay.
There were 25 deaths (9.3%) and 31 patients (11.5%) had major effects ending up with disabilities or disfigurements. The median lengths of stay in ICU and in acute hospitals were 1 and 5 days, respectively. In Lam et al.’s study, their death rate was 3% and median lengths of stay in ICU and in hospital 1 and 3 days respectively. The higher mortality rate in our series might be explained by the higher proportion of substance abusers. In our subgroup analysis, substance abusers had a higher death rate of 14% (p = 0.029).
Lam et al. reported a rising trend of CO poisoning in Hong Kong. In our series, we had a total of 35 patients having CO poisoning. Among them, 30 patients burnt charcoal in an enclosed space, 3 burnt town gas in an enclosed space, and 2 were fire accident victims with significant CO poisoning. The number of these cases fluctuated in our study (6 in 2007, 3 in 2008, 0 in 2009, 4 in 2010, 2 in 2011, 3 in 2012, 3 in 2013, 4 in 2014, 3 in 2015, and 7 in 2016). This suggested that CO poisoning remained popular and was an important route of acute poison exposure requiring ICU care in Hong Kong.
There are limitations of this retrospective study. Data completeness could not be guaranteed. The data were not all available in the soft copies of hospital record of the patients. We need to search through all the available electronic records. The employment status of this group of patients was ever changing and it was difficult to establish their current status on A&E presentation. This was the reason why it was not recorded in our series. This was a single-center study with some of the characteristics of patients being unique to the local community and the result may not be extrapolated to other A&E Departments of Hong Kong and overseas. Agrochemicals would be commonly involved for poisoning presenting to a hospital which received patients from rural areas.9,10
Conclusion
Most if not all of acute poisoning patients would present themselves to an A&E Department in Hong Kong. An estimate of 9.4% of these patients might need ICU care at certain stage of their hospital stay. Benzodiazepine, opioids, zopiclone, CO poisoning, and ethanol were the top five poisons in our series from 2007 to 2016. The mortality rate (9.3%) was high in our series given that there were more substance abusers in our locality. The lengths of stay in ICU and in acute hospital were reasonable in view of the higher mortality and complication rates. There may be room for improvement to increase the rate of decontamination in A&E given that high proportion of these patients had endotracheal intubation performed in A&E before ICU admission. This study serves as an update for the evolving pattern of poisoning in this particular group of acute poisoning patients with more serious clinical presentations that warrant ICU care. With the development of the new specialty of clinical toxicology in Hong Kong College of Emergency Medicine, this group of patients will be better managed in A&E.
Footnotes
Acknowledgements
The author would like to thank HKPIC for use of their data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data were retrieved from the Clinical Data Analysis and Reporting System, the Clinical Management System, and the Electronic Patient Record system of the Hospital Authority, Hong Kong.
Informed consent
Written informed consent was not necessary because no specific patient data have been included in the manuscript.
Ethical approval
The study was approved by the Research Ethical Committee of Kowloon West Cluster of Hospital Authority, Hong Kong
Human rights
This is a retrospective study and all human rights were well respected.