
Abstract
Introduction:
Although cardiopulmonary resuscitation is an emergency life-saving procedure, the intervention itself can cause major and often fatal injuries, with diaphragmatic rupture being very rare. This report describes a patient who experienced bilateral pneumothoraces, left diaphragmatic rupture, and pneumoperitoneum after extended cardiopulmonary resuscitation.
Case presentation:
A 90-year-old woman experienced a cardiac arrest. Spontaneous circulation was restored after 49 min of cardiopulmonary resuscitation performed by a bystander, emergency medical service providers, and emergency department staff. Imaging showed bilateral pneumothoraces, left diaphragmatic rupture, and massive pneumoperitoneum. The patient’s guardian refused to permit surgery for the diaphragmatic rupture, and the patient died despite chest and abdominal decompression and post-cardiac arrest care.
Discussion and conclusion:
Procedures to restore spontaneous circulation in patients experiencing cardiac arrest may result in fatal cardiopulmonary resuscitation–related injuries. Clinicians providing post-cardiac arrest care should plan management for these iatrogenic injuries.
Introduction
The global survival rate of patients who experience out-of-hospital cardiac arrest (OHCA) and receive cardiopulmonary resuscitation (CPR) has increased over the past 40 years. 1 Although CPR is a life-saving emergency procedure, it can cause various injuries, with the most frequent CPR-related injuries including thoracic (primarily rib and sternal fractures), upper airway, intra-abdominal, and lung injuries. 2 Diaphragmatic rupture associated with CPR, however, is very rare. This report describes a diaphragmatic rupture and subsequent massive pneumoperitoneum caused by vigorous and extended CPR in a geriatric patient with chronic medical illnesses who experienced cardiac arrest.
Case presentation
A 90-year-old woman with a history of hypertension, chronic obstructive pulmonary disease (COPD), and cerebral infarction collapsed suddenly at home and was taken to the emergency department (ED) in cardiac arrest. Over the previous week, the patient had reported frequent chest discomfort, perceived that her oral intake had “gone down the wrong pipe” more frequently, and experienced increased sputum production. It was unclear whether the patient had a fever during that period. She did not visit the hospital for treatment. There had been no noticeable changes in recent physical activity (e.g. deterioration in walking or movement), and no trauma was reported. Immediately after the patient collapsed, her grandson called the emergency medical services (EMS) and then performed chest compressions for 4 min. Upon arrival, EMS providers detected pulseless electrical activity. Rescue breaths were provided with a bag valve mask, and chest compressions were performed at a compression/ventilation ratio of 30:2. The EMS providers performed CPR manually, without the use of a mechanical CPR device, for 25 min in the field and during transport. Thus, upon arrival at the ED, she had undergone CPR for a total of 29 min.
Initial evaluation of the patient in the ED showed that she was in asystole, with a slight abdominal distention. Immediately after arrival, endotracheal intubation was performed, and emergency medical technicians continued chest compressions. No foreign body or food bolus was detected in the oral cavity. Although spontaneous circulation was restored 9 min after arrival, she experienced pulseless polymorphic ventricular tachycardia shortly thereafter. Three defibrillations were performed, and intravenous amiodarone was administered. After 20 min of basic life support and advanced cardiac life support, spontaneous circulation was finally restored. The patient’s blood pressure was 136/94 mmHg, and her heart rate was 121 beats/min. Physical examination revealed no external bruises or wounds. During CPR after endotracheal intubation, respiratory sounds of both lungs were heard uniformly on auscultation. Esophageal intubation was not suspected, but the severity of abdominal distension had increased. A nasogastric tube was inserted to relieve abdominal distention. Finally, tracheal intubation was reconfirmed with a video laryngoscope. Chest radiography performed in the ED revealed a fibrocalcific change in the upper right lung field and increased consolidation of both lower lung fields, with large amounts of gas under the right diaphragm and upper abdomen (Figure 1). Complete blood count analysis revealed no abnormalities other than leukocytosis. The results of blood chemistry and electrolyte tests were normal. The cardiac markers CK-MB (1.0 ng/mL) and troponin T (0.018 ng/mL) were within their normal ranges. Electrocardiography performed immediately after recovery of spontaneous circulation (ROSC) and at follow-up revealed non-specific changes in the ST segment and T wave.
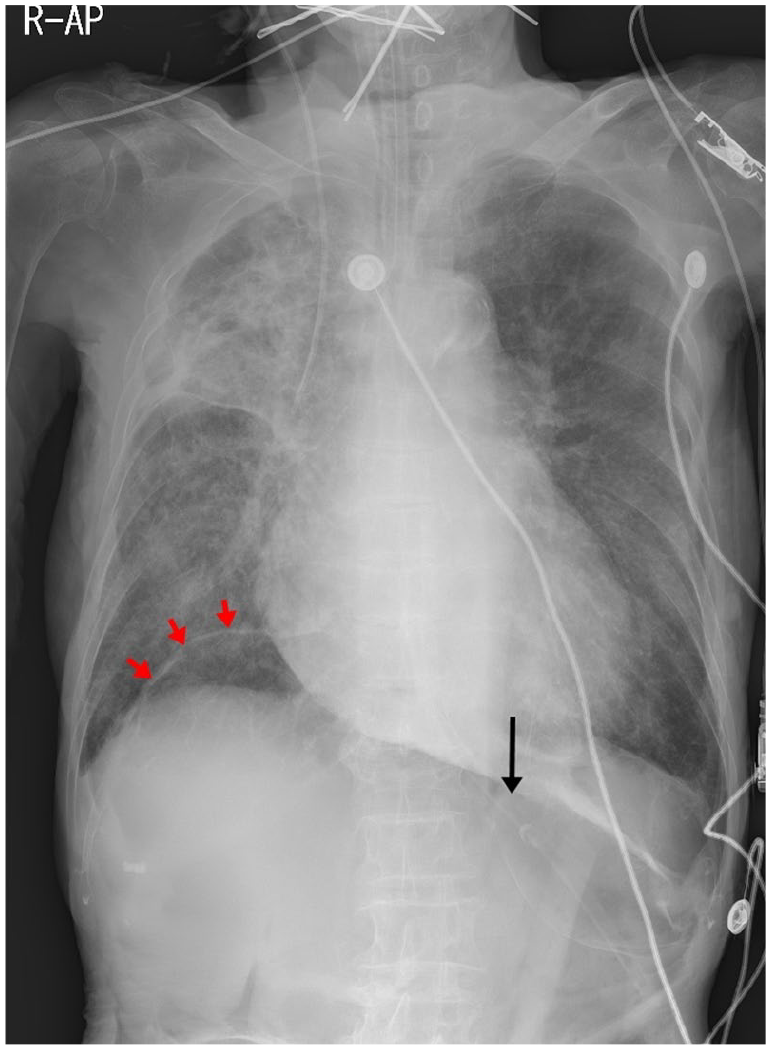
Chest radiography of this patient, showing air shadows under the right diaphragm (red arrows) and upper abdomen (black arrow).
Based on the patient’s history and simple chest imaging, aspiration pneumonia was suspected. Computed tomography (CT) scans of the patient’s brain, chest, and abdomen were performed to determine the cause(s) of the cardiac arrest, and the abdominal distention, which had been observed on physical examination, was found to have worsened. CT scans revealed multiple rib fractures, bilateral pneumothoraces, a defect in the left diaphragm (Figure 2), and massive pneumoperitoneum (Figure 3). Chest CT showed fibrotic consolidation and calcified granuloma, thought to be sequelae of previous inflammation, in the right upper lobe, and diffuse, patchy consolidations in both lower lobes, suggesting pneumonia. The amount of right pneumothorax was minimal, and its progression was monitored (Figure 2(c)). Because the left pneumothorax was accompanied by diaphragmatic injury, a chest tube was inserted.
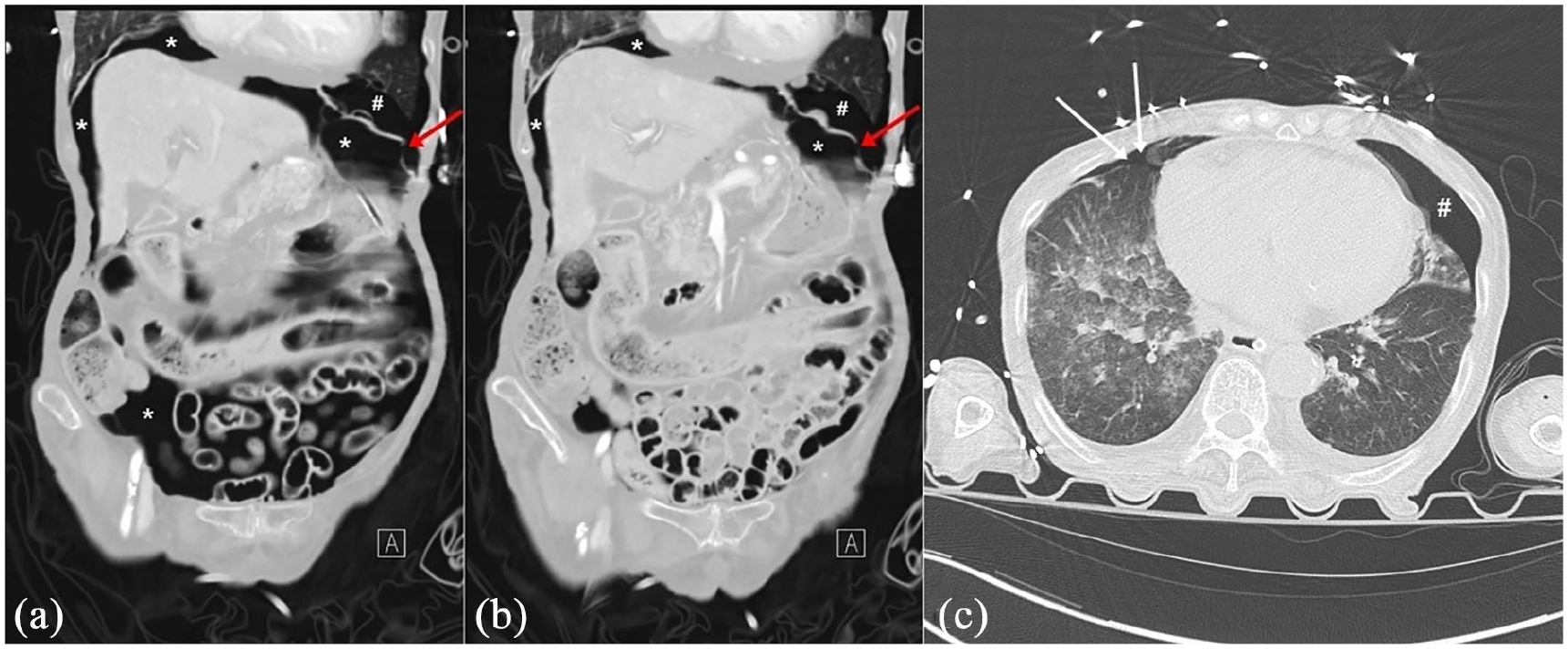
(a) and (b) Abdominal computed tomography (CT) coronal images showing a discontinuation of the left diaphragm (red arrows), pneumoperitoneum (*), and pneumothorax (#). (c) Chest CT showing a minimal right pneumothorax (white arrows) and left pneumothorax (#).
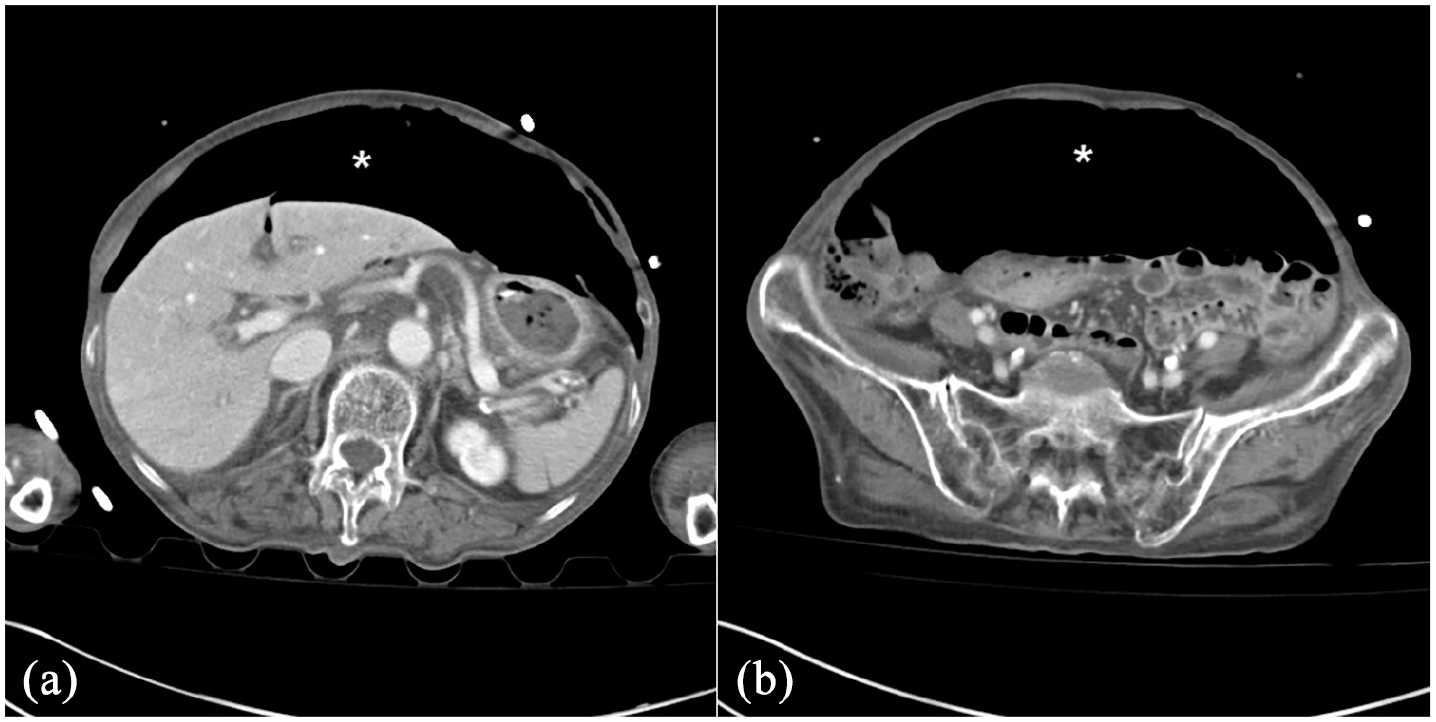
Abdominal computed tomography axial images showing a massive pneumoperitoneum (*).
Emergency surgery was considered, but the patient’s legal guardian did not consent. A diaphragmatic hernia was not observed at this time; therefore, a thoracic surgeon recommended follow-up observation. The general surgeon concluded that there was massive pneumoperitoneum, but no clear bowel perforation or bowel ischemia was found on abdominal CT, indicating that emergency laparotomy was unnecessary. Abdominal CT showed no evidence of compression of venous structures, and neither ventilatory nor hemodynamic compromise appeared soon after ROSC, indicating an absence of tension pneumoperitoneum. As the ventilatory and hemodynamic states of this patient were likely to worsen, percutaneous drainage (PCD) was performed for intraperitoneal decompression. After devising a treatment plan for the left diaphragm rupture, we determined that hospitalization in the intensive care unit (ICU) was required for the treatment of aspiration pneumonia and post-cardiac arrest care. Because of a lack of available beds in the ICU, however, treatment and monitoring continued in the ED. The patient died after 12 h in the ED.
Discussion
CPR involving artificial ventilation and chest compression is essential for preserving the life of patients in cardiac arrest. Rib fractures can occur, however, even if chest compressions are performed properly. An autopsy study of patients who died after CPR showed that rib fractures (13%–97%) and sternal fractures (1%–43%) were the most common CPR-related injuries. 3 Other complications occurring after CPR include pneumothorax, hemothorax, pulmonary contusion, liver laceration, fat embolism, hemopericardium, aortic laceration, and splenic rupture, 3 with major CPR-related injuries to internal organs often being fatal.
Risk factors for CPR-related injuries include depth of chest compression, advanced age, prolonged CPR, and OHCA.3–7 Moreover, the rate of CPR-related injuries has been found to increase with age and CPR duration.4,5 A recent autopsy study found that older age, male sex, and administration of CPR in a public place were associated with CPR-related injuries, with the higher rates of CPR-related injuries in elderly patients being attributed to age-related osteoporosis, tissue stiffness, and degenerative skeletal changes. 6 Abnormal hand positions and compression pressure during ambulance transport 4 and more intense chest compressions due to the stress of performing CPR in a public place 6 may result in high rates of complications in patients who experience OHCA. The effects of patient sex and bystander CPR on rates of CPR-related injuries, however, vary among studies.3,6,7
Elderly patients with physical weakness due to chronic illness and malnutrition are at high risk of CPR-related injuries, suggesting the need to modify chest compression depth and pressure during CPR on these patients. Additional studies are needed to determine the optimal depth of chest compression required to provide efficient perfusion while avoiding CPR-related injuries in geriatric patients.
Injuries to the diaphragm after CPR have been reported rarely.8–10 An autopsy of a patient with an intrathoracic stab wound showed a left diaphragmatic laceration resulting from manual and mechanical CPR. 8 Retrospective examination showed that the compressive hemothorax and the presence of a penetrating wound contraindicated the use of a mechanical CPR device in this patient and that the displacement of the constrictive band during ambulance transit may also have been harmful, suggesting that these interventions may have been jointly responsible for this iatrogenic diaphragmatic injury. Another patient, who had undergone heart valve surgery 10 years earlier, experienced a right intrathoracic diaphragmatic hernia after 20 min of vigorous CPR, but rib fractures were not observed. 9 Another report described a pregnant woman who experienced left diaphragmatic rupture following CPR, 10 with evaluation suggesting that slightly caudal mispositioning of chest compressions during CPR (because of the advanced stage of pregnancy) led to a sudden and sharp increase in intra-abdominal pressure, resulting in diaphragmatic injury. The diagnosis of diaphragmatic injury in the latter two patients was based on the herniation of abdominal organs into the thoracic cavity after CPR.9,10 Both of these patients were treated successfully by surgical diaphragm repair.
A CT scan of our patient showed that pneumoperitoneum was likely caused by a diaphragmatic injury. The presence of a diaphragmatic hernia on chest radiography after CPR may be diagnostic for diaphragmatic injury,9,10 whereas the absence of an apparent diaphragmatic hernia may complicate the diagnosis. CT may be useful as it can assess posterior lumbar elements other than the anterior leaflets of the diaphragm, with several indicators, such as signs of a discontinuous or dangling diaphragm, being helpful in the diagnosis of diaphragmatic injury. 11 Helical and multidetector CT are also helpful for diagnosing concomitant injuries.11,12 Pneumoperitoneum initially presents with a tympanic abdomen and gross distension, clinical features that are also indicative of intra-abdominal hemorrhage. Abdominal CT is regarded as more specific and sensitive than other methods for determining the etiology and extent of injury in patients diagnosed with pneumoperotineum. 13
Traumatic diaphragmatic rupture may be caused by increased shear force within the diaphragm, tearing at the point of muscle insertion, or increased abdominal pressure that exceeds the rupture pressure in the diaphragm.11,12 Although increased abdominal pressure caused by chest compression at an inappropriate site may be a risk factor for diaphragmatic injury, abdominal CT of our patient showed no clear evidence of intestinal or intraperitoneal organ injury. Further investigation was limited, as we were unable to confirm these findings through autopsy or laparotomy. The multiple rib fractures and bilateral pneumothoraces in our patient are in agreement with findings showing that direct blunt force resulting from chest compressions may be a risk factor for diaphragm injury in some geriatric patients with chronic medical illnesses. Barotrauma in patients with hyperinflation and COPD may increase due to a combination of chest compression pressure and forceful inspiration through positive pressure ventilation. The musculoskeletal system in our patient was likely weakened due to the effects of aging, COPD, and malnutrition. This may have resulted in tearing at the insertion point of the diaphragm or injury to the diaphragm due to increased shear force resulting from the distortion of the rib cage due to chest compression. Unlike previously described patients, our patient did not have a diaphragmatic hernia; rather, massive pneumoperitoneum was accompanied by diaphragmatic rupture.
The exact cause of post-CPR pneumoperitoneum has not yet been identified. However, in most cases, this condition results from perforation of the gastrointestinal tract following CPR. 14 It can also occur when pneumothorax and pneumomediastinum accompany air moving through the diaphragmatic apertures. 15 In our patient, positive pressure ventilation, which actively pumps air into the combined thoracoabdominal cavity, 13 occurring after endotracheal intubation may have caused air in the thoracic cavity to move directly into the abdominal cavity through the diaphragmatic rupture site.
In general, traumatic left diaphragm rupture requires surgical repair immediately after diagnosis. If traumatic intraperitoneal injury is suspected, then a simultaneous abdominal approach is required.11,12 Evidence of peritonitis in patients who experience pneumoperitoneum following CPR indicates a need for an exploratory laparotomy. 16 Although abdominal CT showed no evidence of abdominal injury in our patient, emergency surgical intervention was considered necessary for the repair of diaphragmatic rupture and exploration of injury to abdominal organs. However, because of our patient’s advanced age (90 years) and the high likelihood that extended CPR resulted in a hypoxic brain injury, the patient’s caregiver declined to actively treat her diaphragmatic rupture. As an alternative, we attempted to decompress the pneumothorax and massive pneumoperitoneum. Considering the patient’s underlying COPD, we thought that respiratory failure resulting from aspiration pneumonia may have been the cause of the cardiac arrest experienced by this patient. Despite the lack of clear evidence of tension pneumoperitoneum in the early stages, she showed progression of ventilatory and hemodynamic compromise after 6 h of PCD and chest tube insertion. Her condition worsened, and she died due to long cardiac arrest times, aspiration pneumonia, and pre-existing lung problems.
In summary, CPR has saved, and will continue to save, many lives. CPR is used by emergency physicians to revive spontaneous circulation in patients who present in the ED with cardiac arrest. These physicians must also quickly determine the cause of cardiac arrest to initiate proper post-cardiac arrest care treatment and minimize further brain injury. Emergency physicians and other emergency personnel should be aware that CPR itself can cause serious internal organ injuries, and that this unintended iatrogenic injury can itself be life-threatening to the patient.
Conclusion
This case report describes a geriatric patient with chronic medical illnesses who experienced cardiac arrest, for which she was treated with extended CPR and subsequently sustained a diaphragmatic rupture as a complication after extended CPR. Emergency physicians treating a patient with cardiac arrest should be aware of both the life-saving potential of CPR and of its complications, and be prepared to effectively treat these complications, in addition to providing post-cardiac arrest care. Strong clinical suspicion of CPR-related complications is required if abnormal clinical findings, such as severe abdominal distention after CPR, are observed, especially in patients, such as ours, with a high risk of CPR-related injuries. Early and active use of imaging modalities is required to effectively diagnose and treat these possibly fatal complications.
Footnotes
Author contributions
Study concept and design was by W.Y.S. Writing – original draft preparation was by H.S.L. and W.Y.S. Writing – review and editing were performed by H.S.L. and W.Y.S. Approval of final manuscript was given by W.Y.S.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All data and materials are available from the corresponding author upon reasonable request.
Informed consent
Written informed consent to anonymize information to be published in this article was obtained from the patient’s son (legal representative).
Ethical approval and human rights
The authors removed the identifying features of the patient in this article. Anonymized patient information was published in this article, and we also cautiously read the regulations of human rights in the submission guidelines of the Hong Kong Journal of Emergency Medicine.