
Abstract
Acute abdomen may often prompt surgeons to send patients to the operating theatre directly, especially in unstable conditions. Nevertheless, if clinically allows, it would be ideal if surgeons can have a better grasp of the root cause before operating. This case illustrates the integration of meticulous history taking and analysis of simple imaging could have led to a different clinical approach.
A man in his 50s with diabetes mellitus, hypertension and hyperlipidaemia complained of sudden onset of around 1 h of generalized abdominal pain. He had no past surgical history. There was no fever, vomiting, diarrhoea, tarry stool, per rectal bleeding, history of analgesic intake, dysuria or tea-coloured urine. He was in distress on a stretcher. He was afebrile, fully alert and conscious, but pale looking. No pallor or jaundice was noted. His H’stix was 18.3 mmol/L, blood pressure was 111/73 mmHg, and pulse was 98 per minute. Chest was clear with symmetrical air entry; however, there was generalized tenderness and guarding over his abdomen. Electrocardiography (ECG) showed sinus rhythm. A chest radiograph was ordered (Figure 1).
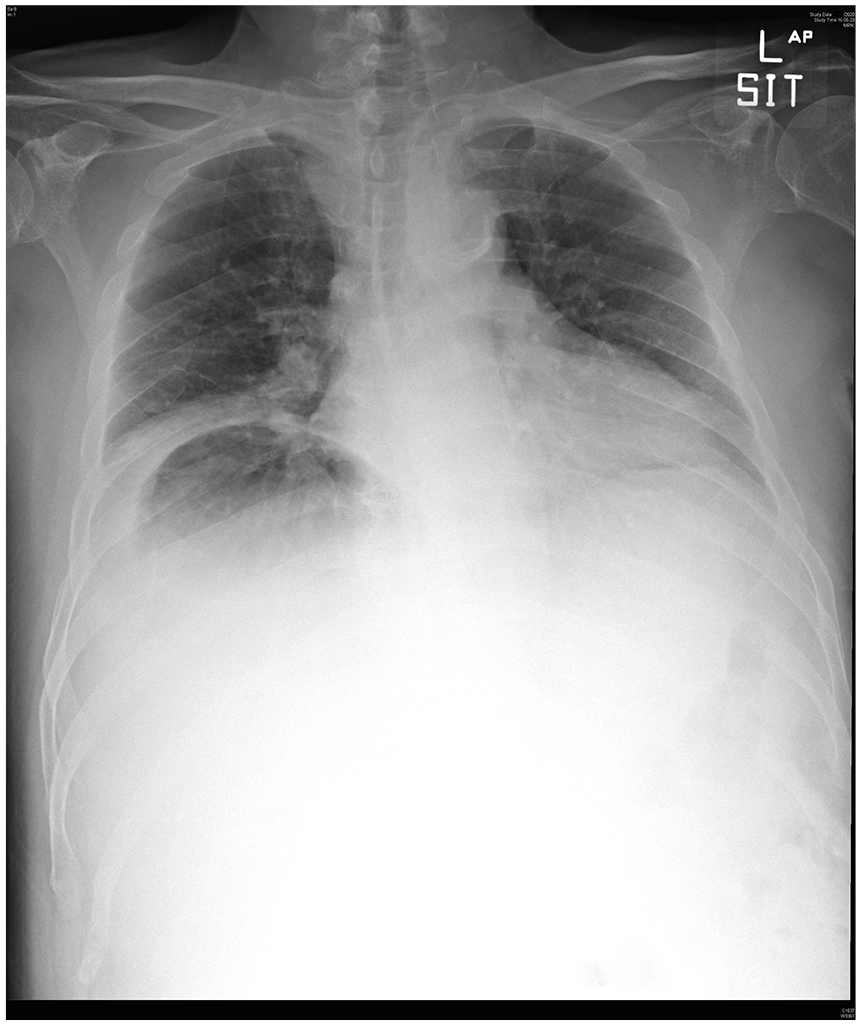
Portable chest radiograph of this patient.
Questions
1. Describe the abnormal findings on the chest radiography.
2. (a) What are the differential diagnoses?
(b) In hindsight, the patient was admitted to the medical ward about 6 weeks ago prior to this event due to hypoglycemia (H’stix 2.5 mmol/L) and fever (37.8°C). Empirical augmentin was prescribed. He was discharged with a diagnosis of right ankle gouty attack. Because of incidental deranged liver function (ALT 133 IU/L, AST 97 IU/L, GGT 146 IU/L), a hepatobiliary ultrasound was performed 2 weeks after discharge which illustrated a 13.1 cm × 9.6 cm × 7.7 cm anechoic lesion with thick and irregular wall in the right lobe of the liver. Differential diagnosis on the report included complicated liver cyst or cystic neoplasm.
What is the likely diagnosis given the above history and clinical picture?
3. What are the risk factors of such a complication?
Answers
1. This expiratory sitting chest radiograph showed a large dome-shaped radiolucency below the right hemidiaphragm, characterized by a well-defined upper margin and an ill-defined lower margin. Right hemidiaphragm elevation and right lower zone haziness were also visualized.
2(a). The differential diagnoses include pneumoperitoneum caused by perforated hollow viscus, Chilaiditi’s syndrome, liver abscess, subphrenic abscess and colonic volvulus.
(b). Ruptured gas-forming pyogenic liver abscess.
3. The risk factors for spontaneous rupture of liver abscess are abscesses greater than or equal to 6 cm in diameter, liver cirrhosis, gas-forming abscesses and the presence of other septic metastases. 1
Discussion
At first glance, one may consider the radiolucency on this radiograph was free gas under the diaphragm. In pneumoperitoneum, however, both upper and lower margins of the radiolucency on an erect chest radiograph are expected to be well defined. Moreover, one may anticipate the appearance of free gas below the left hemidiaphragm as well in a massive pneumoperitoneum. Chilaiditi’s syndrome was unlikely in this case as haustra was not seen in the lucency. Careful interpretation of the chest radiograph is paramount for the initial management of our patient.
Given the ultrasound findings (Figure 2), together with a recent admission for low-grade fever with deranged liver function and hypoglycemia, the reported liver lesion was likely a liver abscess. Thus, along with a clinical presentation of acute abdomen, the most likely diagnosis was ruptured liver abscess.
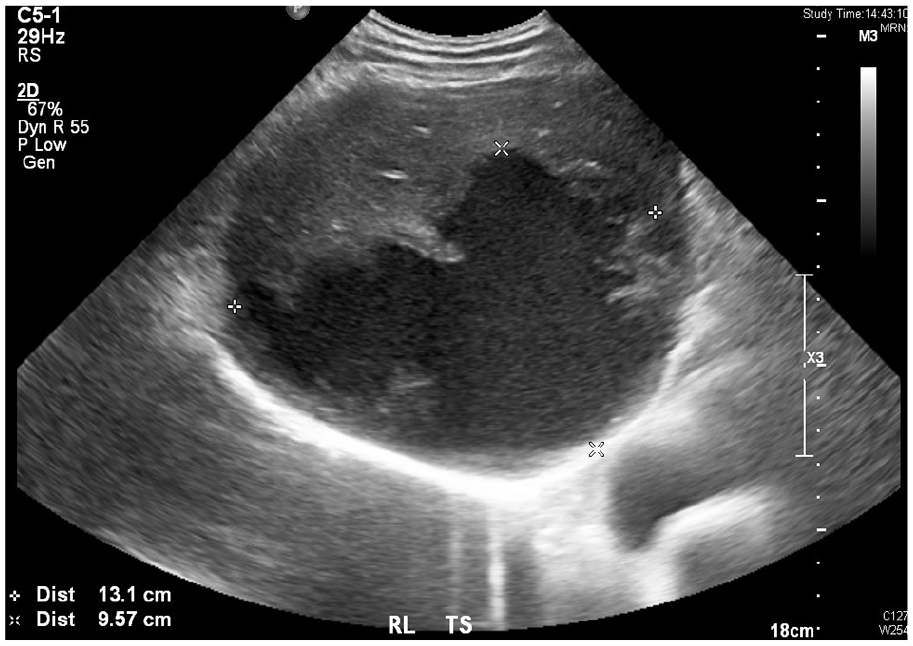
Ultrasound of the right lobe of the liver of the patient in transverse view about 4 weeks prior to the event. A 13.1 cm × 9.6 cm × 7.7 cm anechoic lesion with thick and irregular wall was demonstrated.
Comorbidities such as diabetes mellitus, cirrhosis, malignancy, alcoholism, biliary stones and cardiopulmonary disease increase the risk of developing liver abscess; and rupture of liver abscess occurs in only 5% of cases. 2 Klebsiella pneumoniae (cultured in this patient) and Escherichia Coli account for 77% of gas-containing pyogenic abscesses, 3 thus guiding the choice of empirical antibiotics. In case of rupture, surgery is vital to decontaminate the abdominal cavity and drain the abscess as mortality was reported to be 43.5%. 2
Large gas-forming liver abscess is not uncommon in diabetic patients. They have an impaired immune response and are more susceptible to infections. Mechanisms of poor immune response include reduced inflammatory cytokines release and impaired chemotaxis of white blood cells. Diabetic microangiopathy worsens tissue perfusion and results in anaerobic conditions. 4 In a hyperglycemic, ischemic and acidic environment, enterobacteria thrive and their mixed-acid fermentation of glucose generates hydrogen and carbon dioxide gas via pyruvic acid and formic acid. As the inflammatory site continues to build up gas and other end-products from tissue damage, their removal is simultaneously impaired because of the microangiopathy. A vicious cycle ensues and results in a rapid and massive appearance of gas in the abscess.
In our patient, an emergency operation was immediately arranged based on the diagnosis of pneumoperitoneum. Pre-operative imaging was not conducted. It was converted to laparotomy upon revealing 3 L of pus after removing the omentum from the right liver surface. No abdominal free gas was noted. On-table upper endoscopy revealed no ulcer or leak down to the second part of duodenum. Five abdominal drains were inserted after deloculating the ruptured liver abscess cavity and lavaging the peritoneum.
All in all, this case illustrates that the integration of meticulous history taking and analysis of simple imaging can come a long way to arriving at an accurate diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was not necessary because no patient data have been included in the manuscript.