
Abstract
Background:
The Hong Kong Poison Information Centre has provided consultation service to healthcare professionals and collected epidemiological data on poisoning in Hong Kong since 2005.
Objective:
To analyse and report the poisoning data of Hong Kong Poison Information Centre in 2020 during the COVID-19 pandemic.
Methods:
A retrospective review of all poisoning cases recorded in the Poison Information and Clinical Management System of Hong Kong Poison Information Centre in 2020.
Results:
A total of 3633 poisoning cases were analysed. Compared to 2019 (pre-COVID era), there was a reduction of ~10% of total poisoning cases recorded (383 cases), with a majority (> 90%) of reduction from poisoning cases with no clinical effect (353 cases). A greater proportion of reduction was observed among the children (0–12 years), patients with general unintentional poisoning, poisoning due to therapeutic error and food poisoning. An increased number of cases was noted from abusive use, adverse herb/proprietary Chinese medicine reaction and poisoning related to household bleaches. Teenage (13–19 years) poisoning seemed to be unaffected by the COVID-19 pandemic and the previously observed increasing trend continued (up to 11.8% of total poisoning cases this year). Despite a total reduction in poisoning cases recorded, the number of deaths increased by 37% from 35 in 2019 to 48 in 2020 (mortality rate 1.5%). A total of seven interesting cases were discussed.
Conclusion:
This 15th annual report provides updated epidemiological information on poisoning patterns in Hong Kong during the COVID-19 pandemic. It also highlighted important changes and possible effects of the COVID-19 pandemic on poisoning in Hong Kong in comparison with our previous reports.
Introduction
The Hong Kong Poison Information Centre (HKPIC) located in United Christian Hospital (UCH) was established in 2005. It provides round-the-clock phone consultation service to healthcare professionals in Hong Kong for poison information and advice on patient management on poisoning. It also provides onsite clinical toxicology service to poisoned patients in UCH and postgraduate diploma and fellowship training in clinical toxicology in Hong Kong. HKPIC routinely collects local epidemiological data on poisoning through voluntary reporting from all the Accident and Emergency Departments (AEDs) from the Hospital Authority (HA).
HKPIC has started to publish annual reports on poisoning since 2006. It continues to provide updated information on the poisoning epidemiology and the changing poisoning trend in Hong Kong. This 15th annual report of HKPIC covers the data in 2020, focuses on the latest poisoning pattern and reviews the effects of the COVID-19 pandemic on poisoning in Hong Kong. We also discuss seven cases of poisoning with educational value to healthcare professionals.
Methods
We retrieved all cases received by HKPIC in 2020 from our database, Poison Information and Clinical Management System (PICMS), for analysis. Notification of poisoning is received by HKPIC primarily from two sources: consultation and reporting. Consultation cases are defined as poisoning cases healthcare professionals consult HKPIC for poison information and management advice. Reporting cases are defined as poisoning cases reported through HA, mostly from all public AEDs.
Data collected include patient demographic data, poison data (poison type and dose, route, time, place and reason of exposure), clinical data (clinical features, investigation results), management data (use of decontamination, antidotes and other specific treatment) and outcome data (disposition for AED patients, outcome and its relationship with the poison exposure) for consultation cases, while only patient demographic data, poison data and outcome data are inputted for reporting cases. We input all the data of each poisoning case into PICMS according to the information obtained from the consulting healthcare professionals, medical records, electronic patient record (ePR) of HA and other relevant sources.
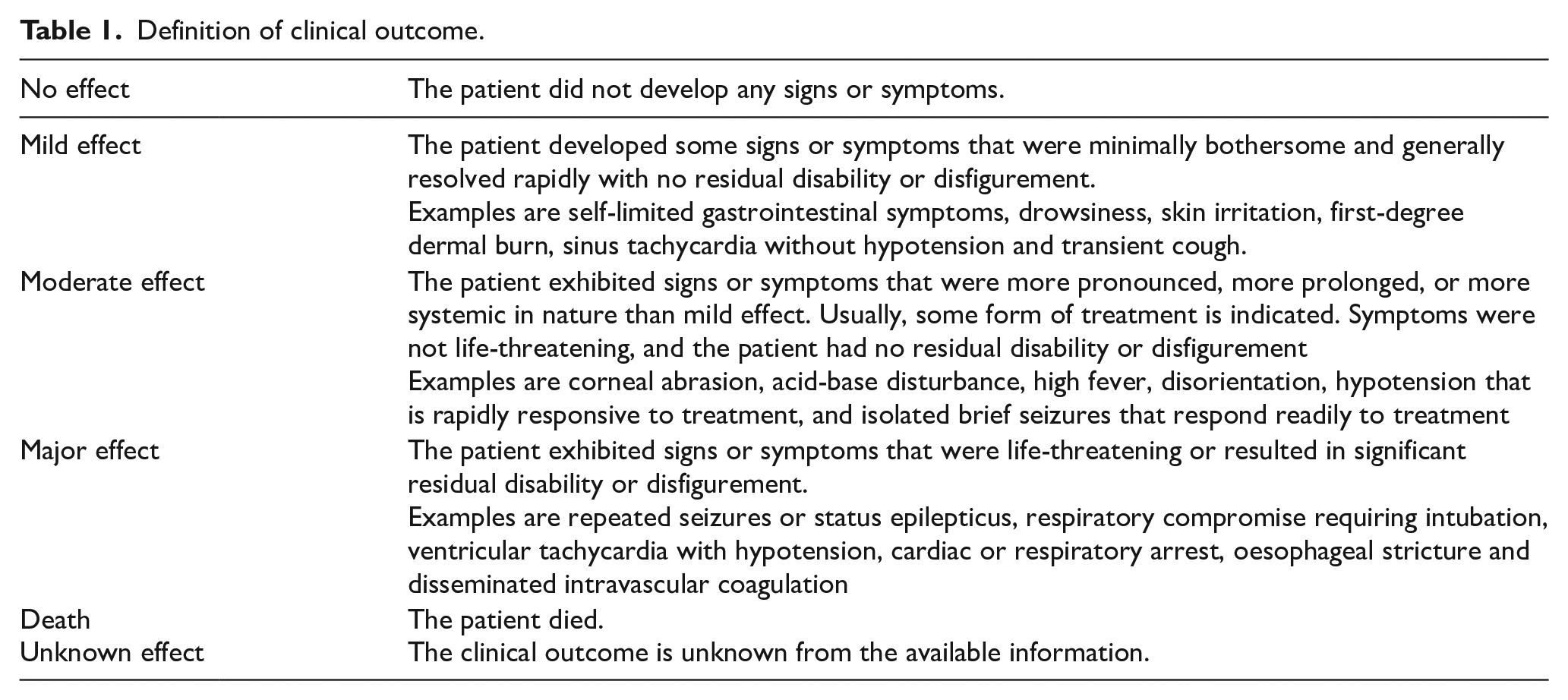
The outcome of the cases is classified by senior doctors in HKPIC into five categories: no effect, mild effect, moderate effect, major effect, or death with reference to the American Association of Poison Control Centres’ National Poison Data System (Table 1). 1 The relationship between poison exposure and clinical outcome is graded as definite, probable, possible, not related or undetermined/not applicable according to the available information. A second senior doctor further reviews all death or major effect cases to ensure appropriate grading.
Definition of clinical outcome.
All information used in this annual report was considered as a part of the usual clinical data routinely collected by HKPIC. Research ethical approval was applied and judged to be not required by the Research Ethics Committee of Kowloon Central/East Cluster (REC (KC/KE)) of HA.
Results
We identified 3633 valid cases in PICMS in 2020 after the exclusion of duplicate and invalid cases, including 2001 (55.1%) consultation cases and 1632 (44.9%) reporting cases for analysis.
There were 1581 male patients (43.5%), 2047 female patients (56.3%) and five sex-unspecified patients (0.1%). Female predominance was present in all age groups except for the children of age 0–12 years and elderly patients from age 60 to 79 years (Figure 1). The age distribution is shown in Figure 1. Of note, 11.8% of all cases were teenagers aged 13–19 years and 5.8% aged 80 years or above.
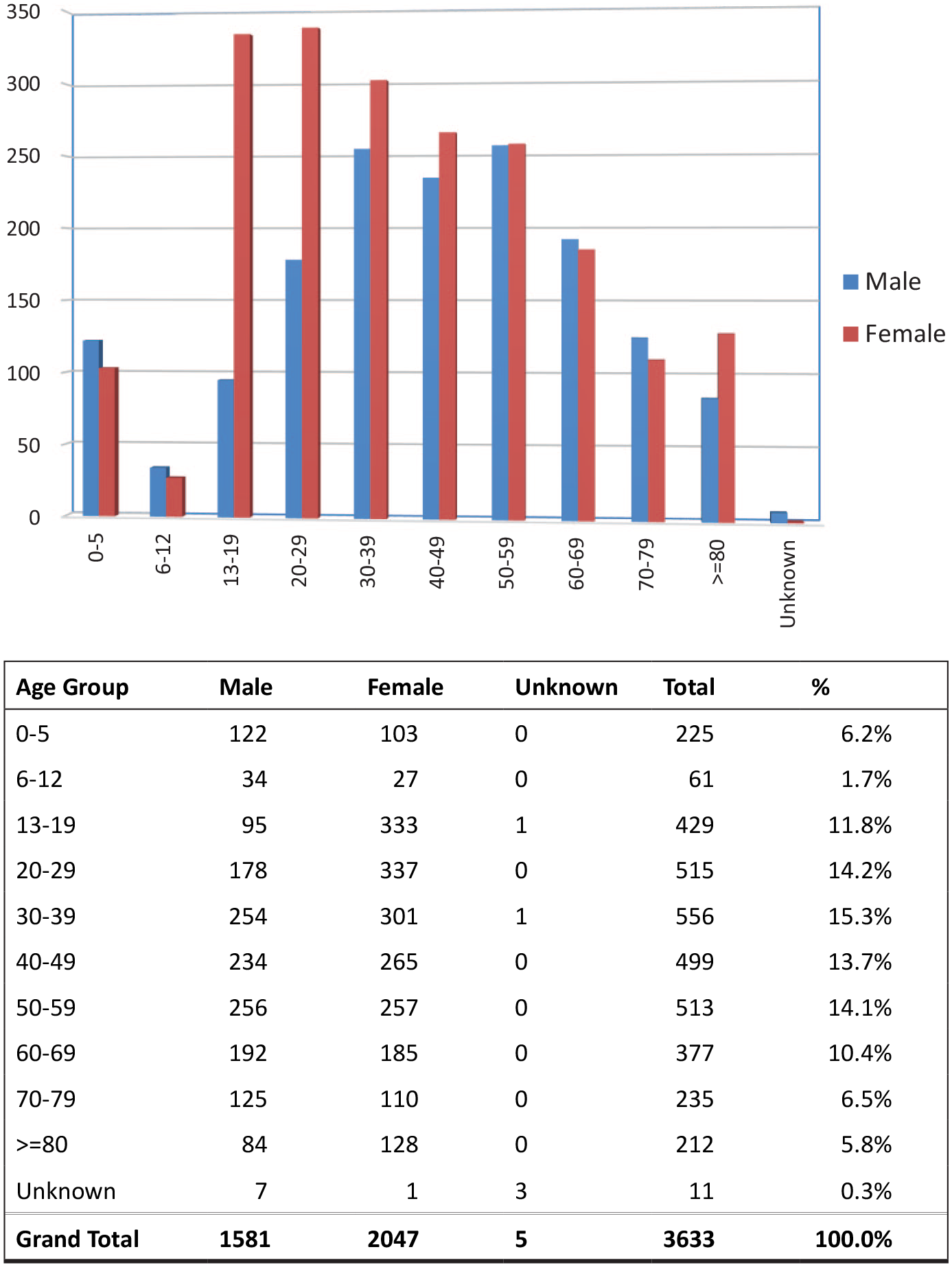
Age and gender distribution.
Figure 2 listed the reasons for poisoning. Suspected self-harm, being the most frequent reason, accounted for 41.6% of the poisoning cases, followed by unintentional exposure (15.3%), abusive use (14.1%), adverse herbal or proprietary Chinese medicine (PCM) reactions (8.1%) and venomous bites and stings (7.4%). Altogether these five commonest reasons for poisoning contributed to the vast majority (86.5%) of the cases. Residential place (66.6%) was the commonest place of exposure (Figure 3). Oral exposure (84.7%) was the commonest route of poisoning, followed by inhalational (6.2%) and dermal exposure (5.6%) (Figure 4).
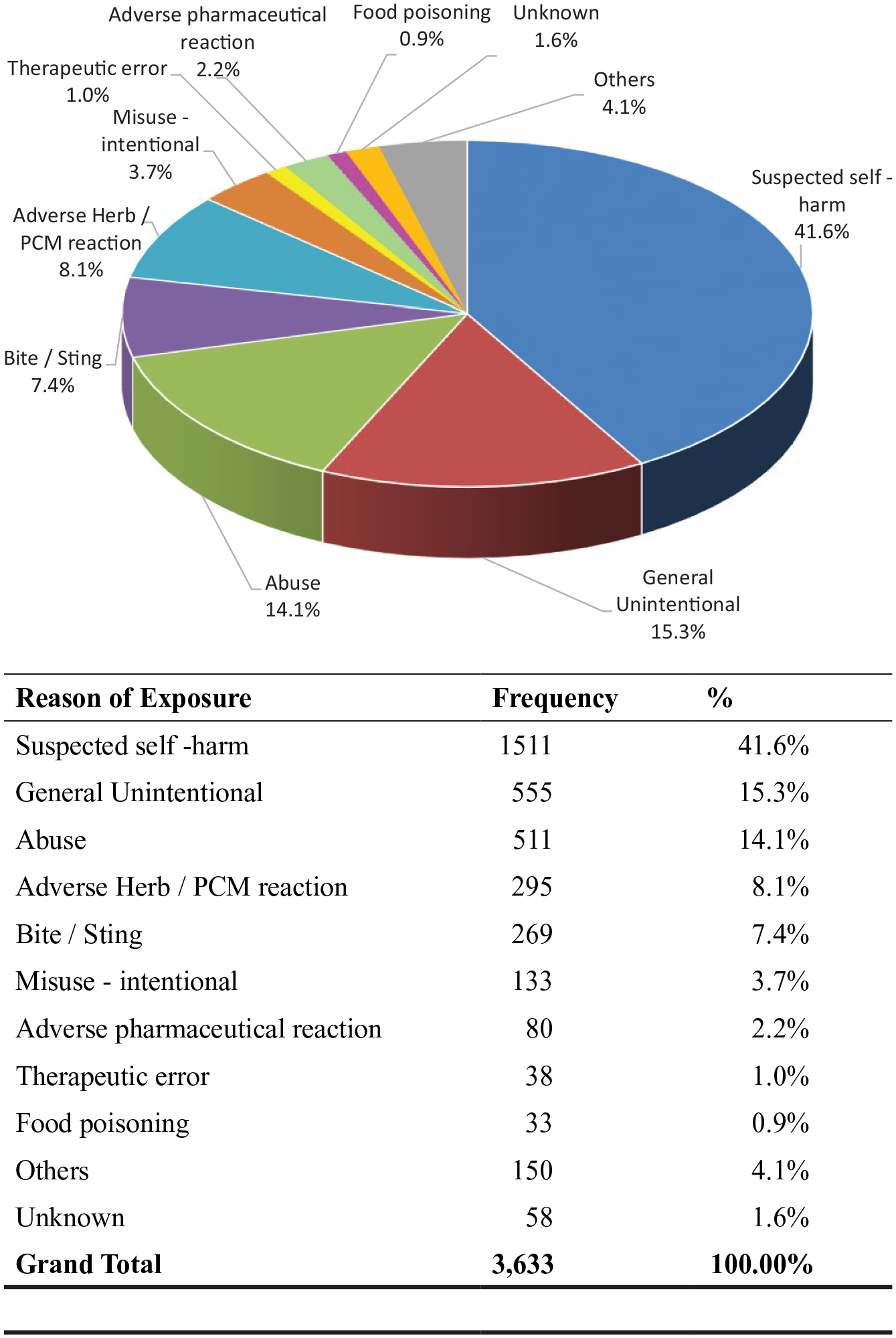
Reason of exposure.
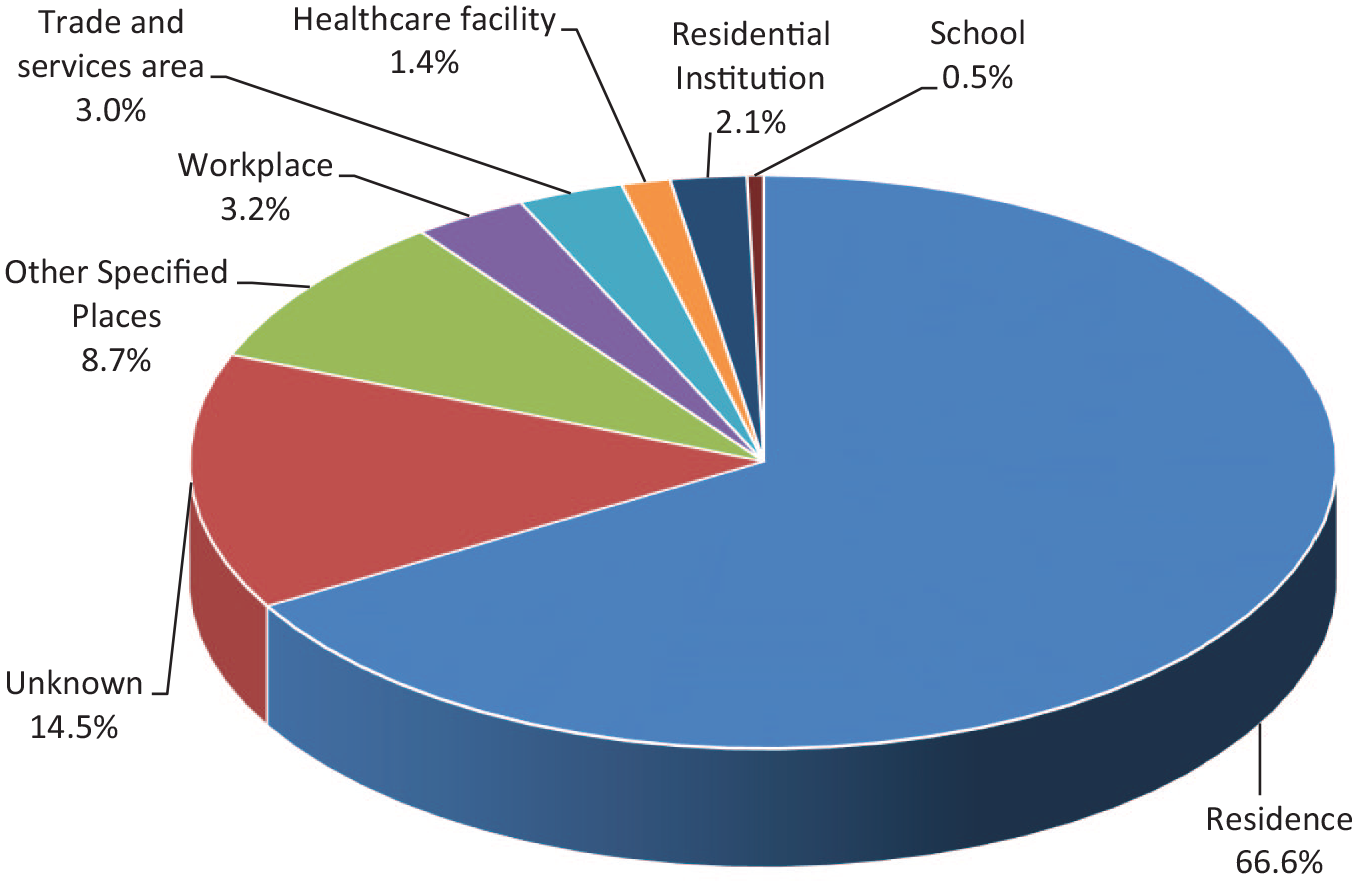
Place of exposure.
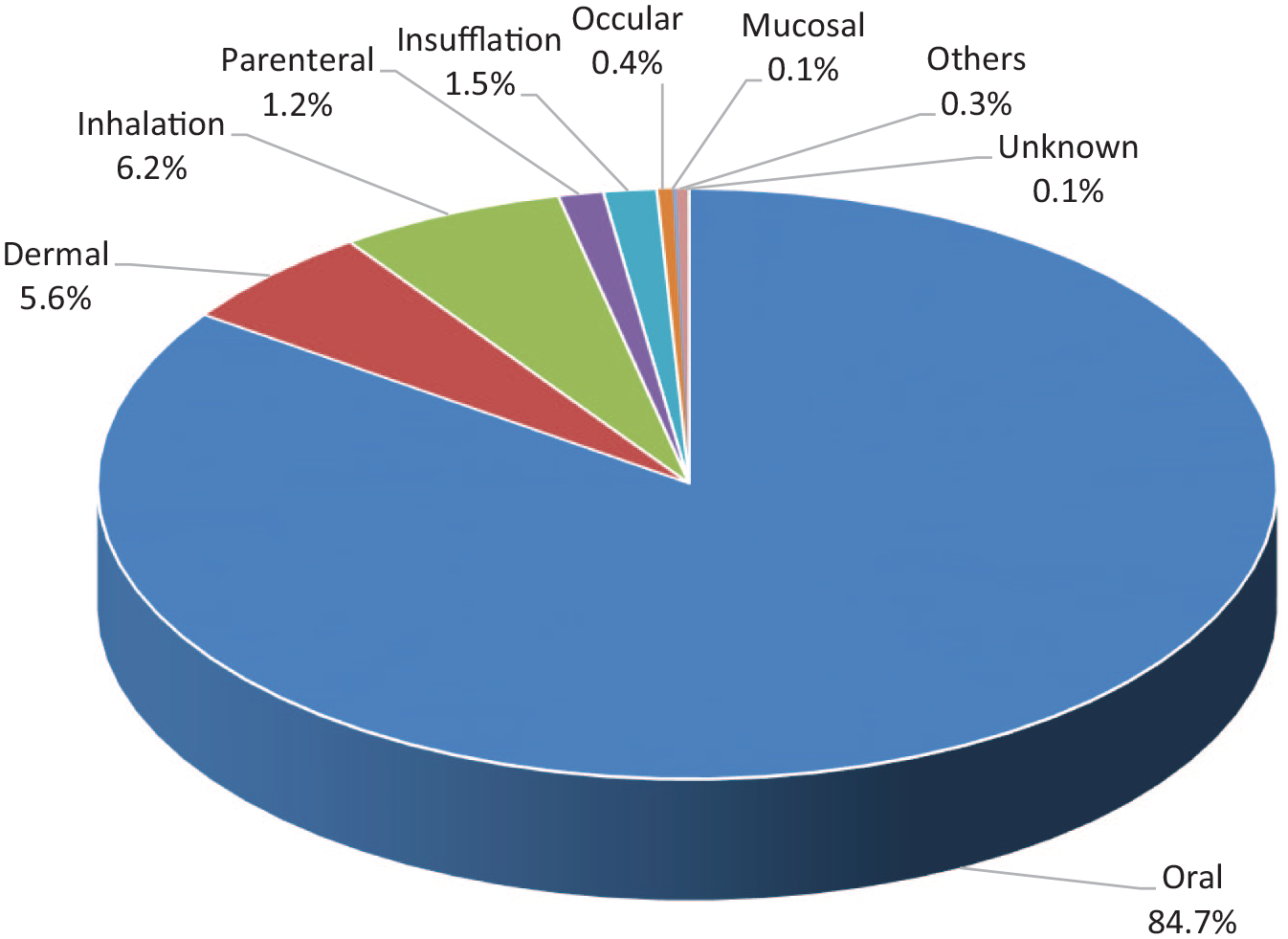
Route of exposure.
In the 3633 cases, a total of 5929 poisons were involved. About two-thirds (67.4%) had been exposed to a single poison and one-third (32.6%) had been exposed to multiple poisons. Figure 5 shows the types of poison exposure. Excluding the commonly involved co-ingestant ethanol, benzodiazepines (408 cases), paracetamol (317 cases), household products, Chinese herbal medicine (both 306 cases) and zopiclone (304 cases) were the five commonest.
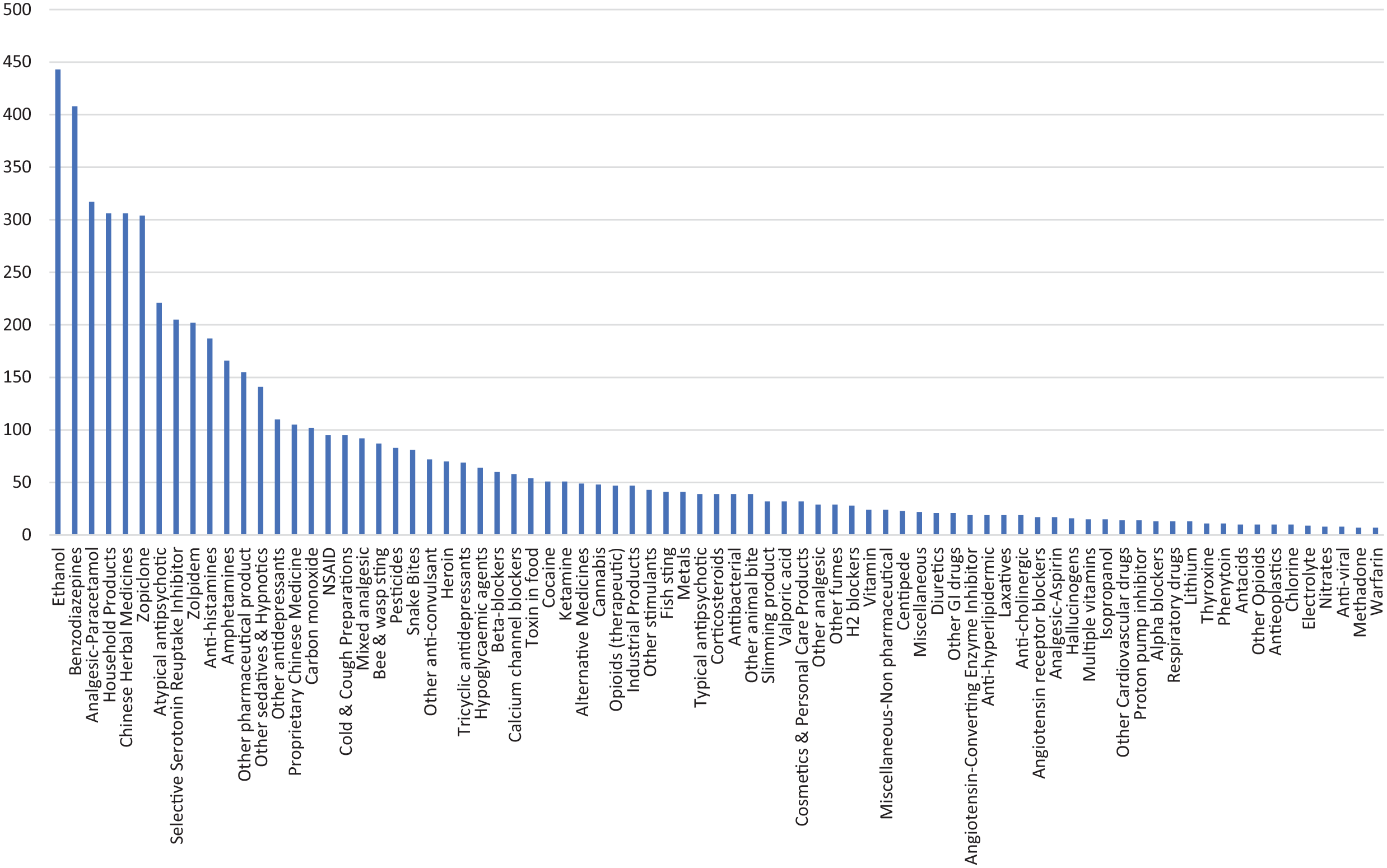
Type of poison exposed.
Only the consultation cases were included for analysis on the use of decontamination and antidote. Among the 2001 consultation cases, decontamination was performed in 325 (16.2%) patients and 18 of them had multiple decontaminations. Single-dose activated charcoal (AC) (93.5%) was the commonest method, followed by gastric lavage (4.3%) and multiple-dose activated charcoal (MDAC, 3.1%) (Table 2). There were 328 patients (16.4 %) treated with antidotes and more than one antidote were required in 48 of them. N-acetylcysteine (NAC), benzodiazepines, hyperbaric oxygen, sodium bicarbonate and snake antivenin were the five commonest antidotes used (Table 3).
Decontamination.
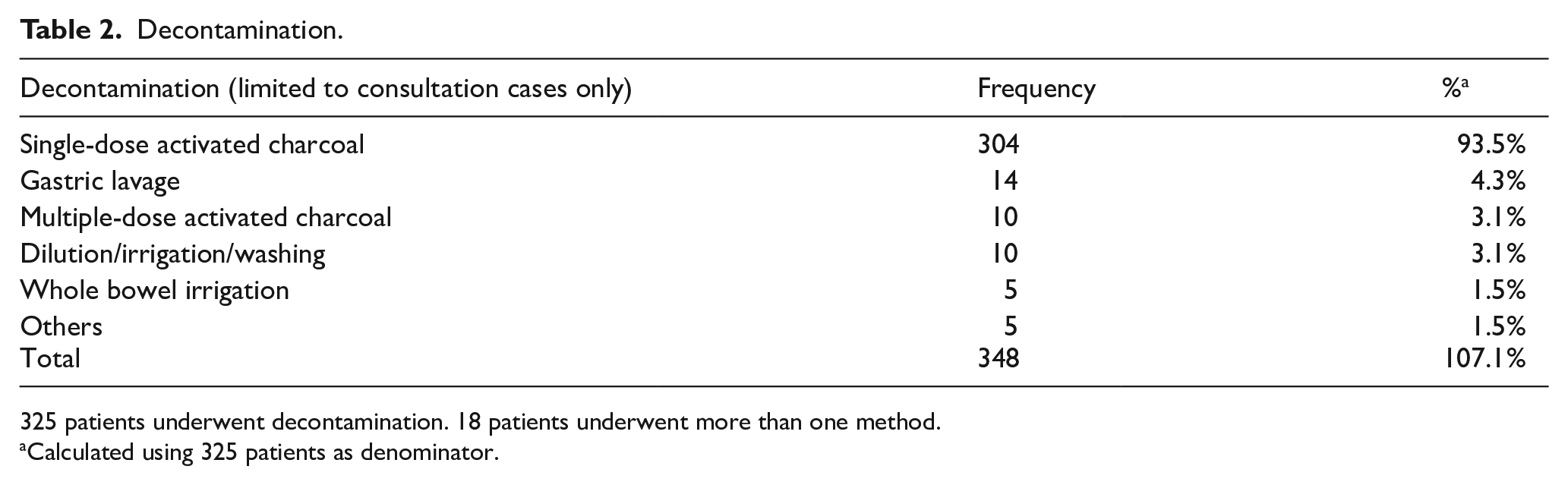
325 patients underwent decontamination. 18 patients underwent more than one method.
Calculated using 325 patients as denominator.
Antidote.
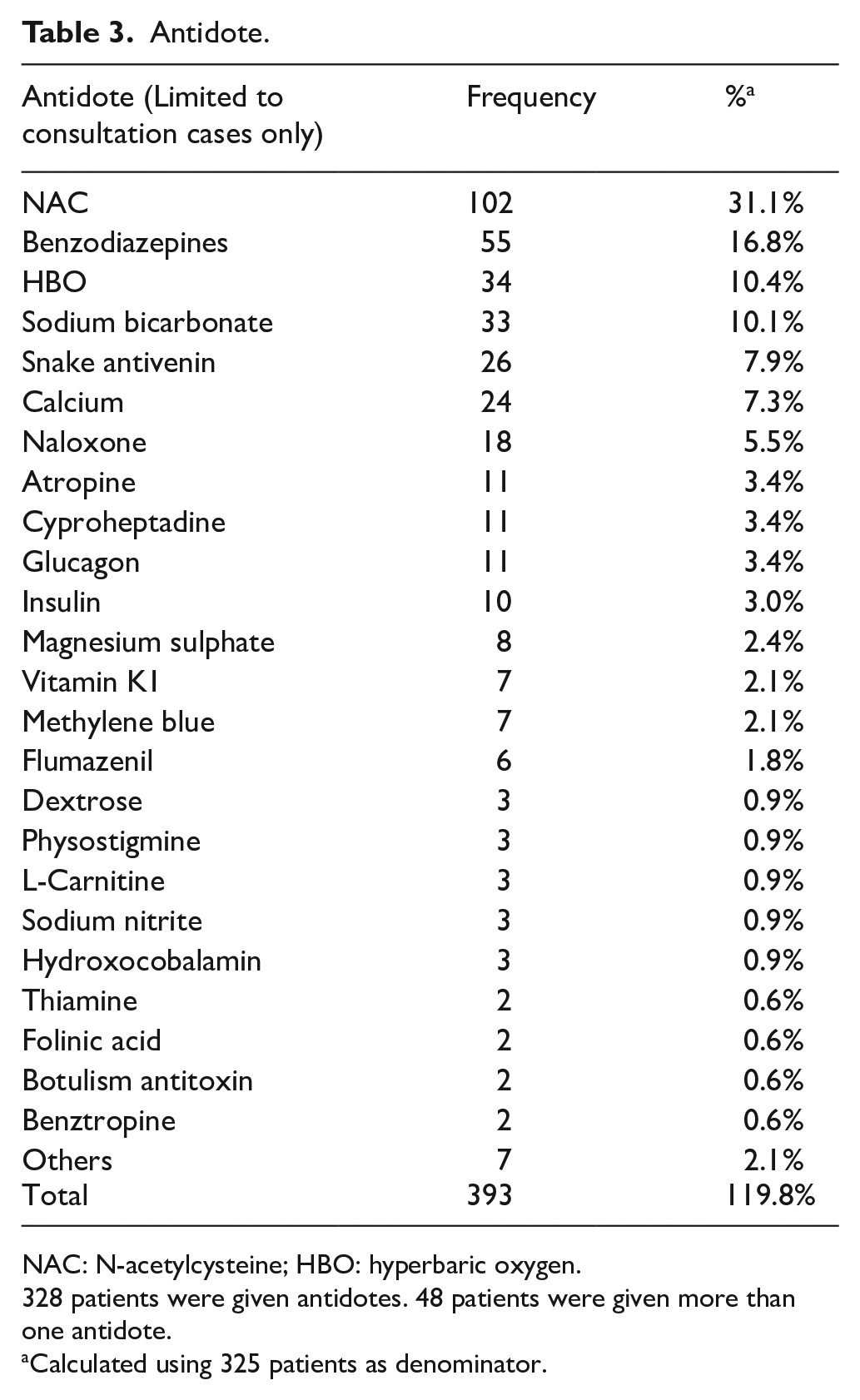
NAC: N-acetylcysteine; HBO: hyperbaric oxygen.
328 patients were given antidotes. 48 patients were given more than one antidote.
Calculated using 325 patients as denominator.
After excluding 365 cases in which the clinical outcomes were graded as not related to the poison exposure, or clinical outcome could not be assessed from the available information, there were 3268 remaining cases for the outcome analysis. There were 48 deaths (1.5%), 162 cases with major effects (5.0%), 561 cases with moderate effects (17.2%), 1993 cases with mild effects (61.0%) and 504 cases with no effects (15.4%) (Table 4), of which 44.4% of the outcomes were graded as definitely, 34.2% as probably and 21.3% as possibly related to the poison exposure.
Clinical outcome in 2020, and 2019 for comparison.
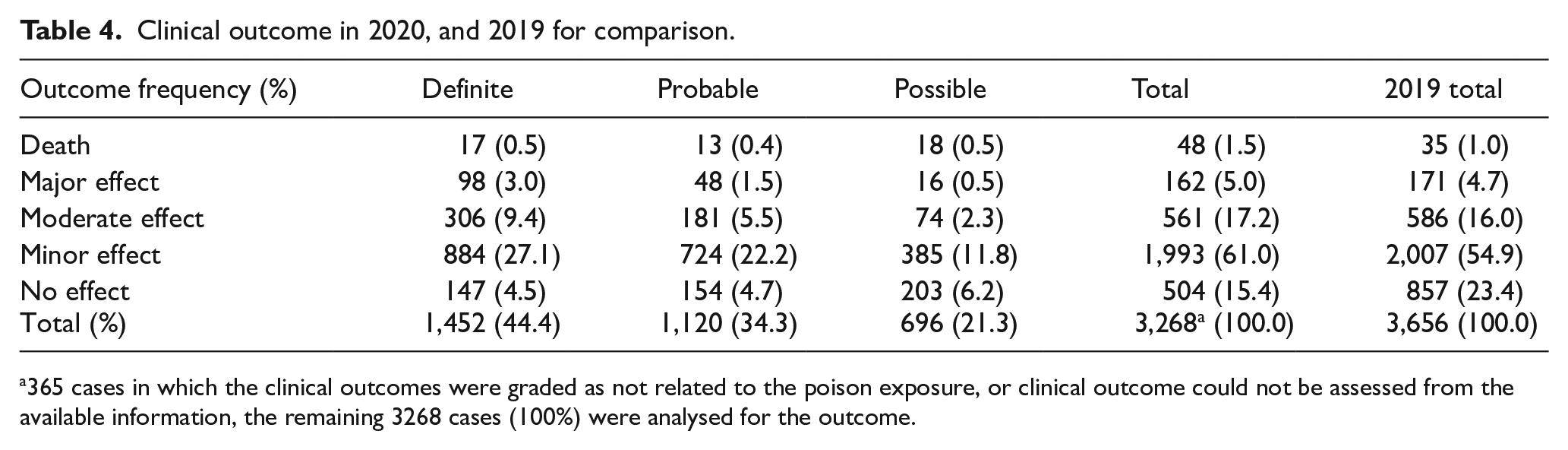
365 cases in which the clinical outcomes were graded as not related to the poison exposure, or clinical outcome could not be assessed from the available information, the remaining 3268 cases (100%) were analysed for the outcome.
We received 317 consultations on pre-hospital AC administration. AC was given in 187 (59.0%) patients and the remaining 130 (41.0%) patients were either not indicated for AC administration, or judged to be not suitable for AC administration during the ambulance transfer.
Discussion
This 15th annual report of HKPIC analysed the data of 3633 poisoned cases in 2020, which represented the most updated poisoning pattern in Hong Kong.
Although reporting of poisoning to HKPIC is not compulsory in Hong Kong which remains an intrinsic limitation to our data, HKPIC recorded around 4000 cases every year over the past, with comparable figures of death and major outcomes in recent years (Table 5). We believe the majority of poisoning cases have been captured for analysis by the current method.
The HKPIC annual reports important figures in the previous 5 years.
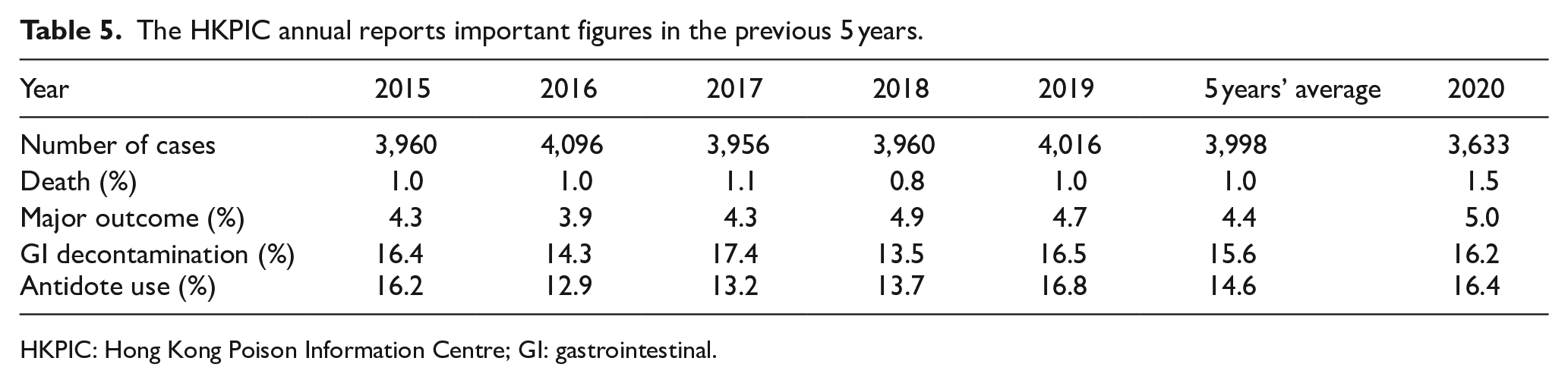
HKPIC: Hong Kong Poison Information Centre; GI: gastrointestinal.
As mentioned in our previous reports, the following patterns of poisoning were similar to previous years: the age and sex distribution (Figure 1); the three commonest reasons of exposure (Figure 2), the five commonest types of poisons excluding ethanol (Figure 5); and the decontamination and antidotes usage pattern for consultation cases (Tables 2 and 3). 2 As noted in previous years, the proportion of teenage (13–19 years) poisoning continued to increase from 6.3% in 2016 to 11.8% in 2020. However, for the elderly group (>80 years), the previously observed rising trend from 2016 plateaued in 2020, with a similar proportion in 2019 (5.9%) and 2020 (5.8%).
The year 2020 also witnessed the first year of the COVID-19 pandemic in Hong Kong, with the first case confirmed on 23 January 2020, followed by three waves of local outbreaks. We recorded several major changes which might be related to the COVID-19 pandemic effect. There was a drop in the number of poisoned cases from 3998 cases of the previous 5 years’ average and 4016 cases in 2019 to 3633 this year, which represented around 10% reduction (365 cases and 383 cases fewer, respectively). 2 Comparing with 2019, the reduction was similar for all age groups except for children (0–12 years) where a greater percentage of reduction by 32% was observed and for teenagers (13–19 years) where an increase of 2% was noted. For the reasons of exposure, a similar percentage of reduction was observed for suspected self-harm (11%), adverse pharmaceutical reaction (5%) and bite and sting (4%). A greater percentage of reduction was observed for general unintentional (24%), food poisoning (47%) and therapeutic error (66%). There was an increase in abusive use by 15% and adverse herb/PCM reactions by 5% (Table 6). Although the total number of poisoning due to household products remained similar (292 cases in 2019 vs 306 cases in 2020), the number of poisoning related to household bleaches increased by 55% from 56 to 87 cases.
Reasons of exposure in details (sort according to the percentage of change in absolute number in 2020 compared with 2019).
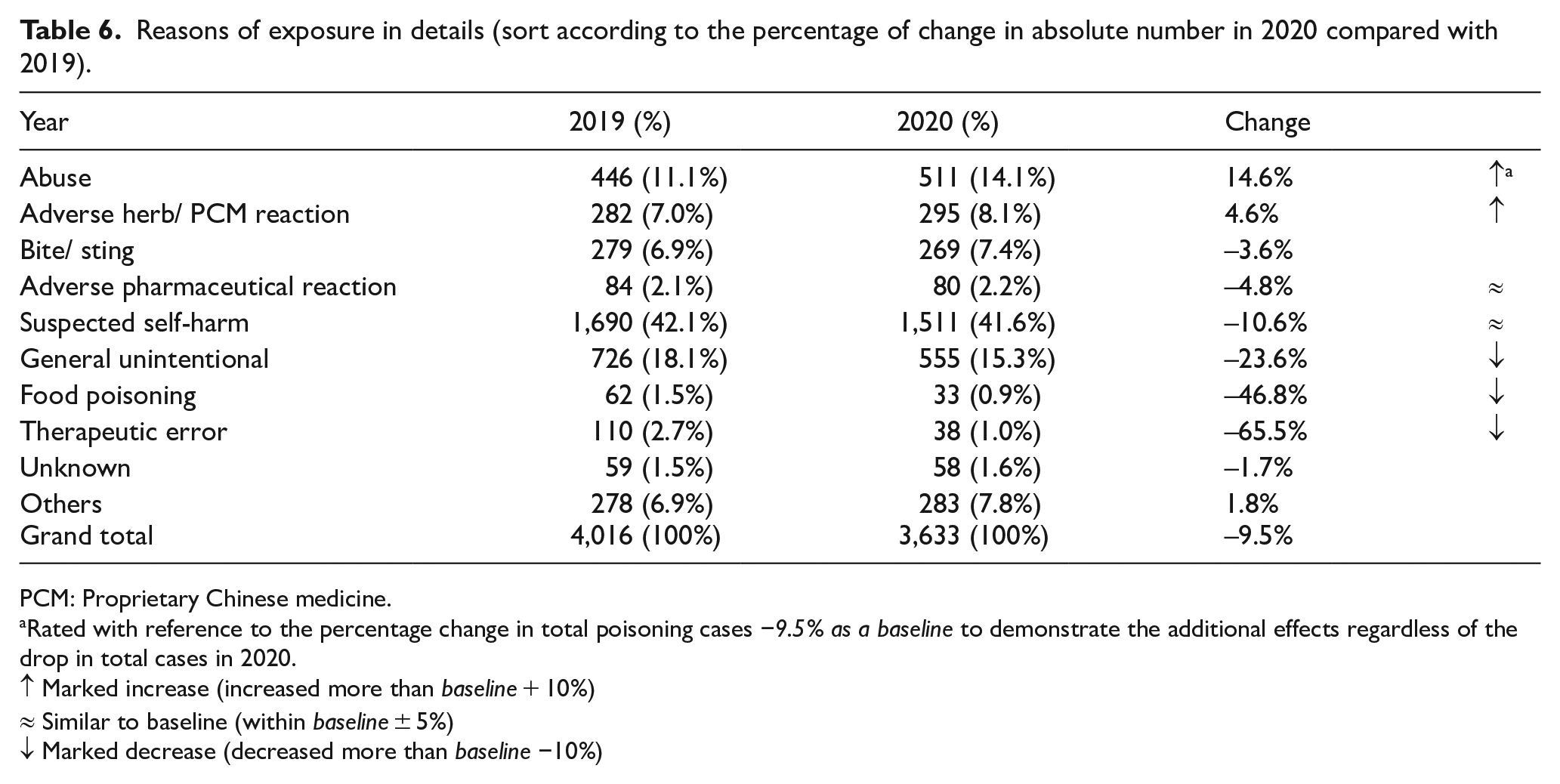
PCM: Proprietary Chinese medicine.
Rated with reference to the percentage change in total poisoning cases −9.5% as a baseline to demonstrate the additional effects regardless of the drop in total cases in 2020.
↑ Marked increase (increased more than baseline + 10%)
≈ Similar to baseline (within baseline ± 5%)
↓ Marked decrease (decreased more than baseline −10%)
For the clinical outcome, there were 353 fewer cases who had no effects compared with 2019 (Table 4), which comprised 92% of the total reduction (383 cases). Despite the reduction in total poisoning cases in 2020, the number of deaths increased by 37% from 35 to 48 cases. 2
Possible reasons for the above differences include the followings: during the COVID-19 pandemic, people are in general less willing to attend the hospitals or AED where these places are commonly regarded as unsafe and people are worried to get infected by the virus there. Moreover, there are messages from the government to discourage the general public from unnecessary visits to AED. Therefore, people with a minor health problem will not present to AED, including those suffering from poisoning. In a local study, AED attendance was found to have decreased during the COVID-19 pandemic in Hong Kong, with a greater degree of reduction on the semi-urgent and non-urgent patients (-29.5%), comparing with the critical one (−2.2%). 3 From our data, it clearly shows that the COVID-19 pandemic was associated with a reduction in poisoning cases in which more than 90% of them are asymptomatic. Whether this is the result of a true reduction in mild poisoning cases, or just because mild poisoning cases did not turn up in AEDs and therefore they were not captured by us resulting in an apparent decrease in poisoning cases, is difficult to prove from our data.
Several measures were taken by the government in response to the three waves of COVID-19 to limit direct face-to-face contact to control the spread of the disease. This included encouraging people to work from home, limiting the number of people gathering, banning dine-in service from restaurants during dinner time after 6 p.m., closure of public entertainment venues and so on. All these measures encouraged people to stay at home most of the time and therefore parents might have better supervision of their children. Since children (0–12 years) poisoning were in majority accidental in nature, 4 as a result, the number of children (0–12 years) poisoning and general unintentional poisoning had both decreased.
In addition to the above measures, wearing facial masks, and keeping good hand hygiene, together with the closure of schools in an attempt to reduce close contact by children, effectively controlled influenza (and other respiratory diseases) spread compared to the non-COVID era. 5 As a result, poisoning due to own therapeutic error as a result of taking Western medications for flu symptoms might decrease as well.
The lack of entertainment during the COVID-19 pandemic and the increasing stress in coping with the situation might lead to an increase in abusive substance use, as reported in other places in the world. 6 Some Chinese herbal medicine (CHM) or PCM were promoted to be useful in treating COVID-19 or enhancing our health and immune system to fight against the virus. As a result of increasing CHM/PCM use, adverse herb/PCM reactions would also increase. Increasing the use of diluted household bleaches for cleaning and disinfection by people might increase the number of poisoning related to household bleaches, which has also been reported in other poison centres. 1
The reason for an increase in the number of poisoning deaths was unknown. One might suggest its relation to the possible delayed presentation as a result of fear of AED or hospital attendance. Whether there was a delay in poisoning cases to be presented to the hospital and if any, its effect on poisoning outcome needs further study to quantify.
Last but not least, teenage (13–19 years) poisoning seemed to be unaffected by the COVID-19 pandemic. There was an actual increase in the number of teenage poisoning cases in 2020 despite the drop in total poisoning cases which matched the increasing trend observed in the pre-COVID-19 era since 2016. Although this year, we did not record any death related to teenage poisoning and only seven cases (1.6%) were of the major outcome, this increasing trend in teenage poisoning is worrisome and it warrants close monitoring. Further analysis of the data to look into the problem in detail is suggested.
Limitations
This report has limitations as mentioned in our previous annual reports, including the voluntary basis of poisoning reporting in Hong Kong and possibly incomplete data obtained from the consulting healthcare professionals. However, since most poisoning cases are managed in HA hospitals with clinical records accessible in the centralised electronic patient record (ePR), the accuracy and amount of information are expected to be much better than data obtained in other poison centres not having direct access to patient records in their managing hospitals. In cases with limited clinical information, it is difficult to establish the causal relationship between poison exposure and the outcome.
Conclusion
This 15th annual report provides the most updated epidemiological information on poisoning in Hong Kong in 2020. It highlights several changes in poisoning demography as compared with our previous reports and identified some possible effects of the COVID-19 pandemic on poisoning in Hong Kong. Concerning the outcome, 1.5% and 5.0% of the cases resulted in death and major outcome, respectively. HKPIC will continue to monitor the poisoning pattern in Hong Kong to facilitate the formulation of strategies in local poison control and prevention.
Interesting cases
Case 1 ‒ endogenous lead exposure in a patient with end-stage renal failure
A woman in her 70s with a history of end-stage renal failure (ESRF) on haemodialysis was investigated for bilateral hand numbness for 2 years. Electromyography showed moderate-to-severe carpal tunnel syndrome and underlying generalised axonal neuropathy. Upon routine investigation for alternative causes of peripheral neuropathy, she was found to have elevated blood lead level (BLL) 13.9 µg/dL (reference < 10 µg/dL). The elevated BLL was confirmed upon repeating the blood tests 2 weeks later. There was no other clinical feature of lead poisoning. There was no exogenous source of lead exposure identified in detailed history taking. The patient was noted to have an elevated parathyroid hormone (PTH) concentration of 53 pmol/L (reference 1.3–6.8 pmol/L) and a corrected serum calcium concentration of 2.54 mmol/L (reference 2.24–2.63 mmol/L), which is at the high end of the normal range. Blood alkaline phosphatase concentration was elevated to 203 U/L (reference 47–124 U/L). Hyperparathyroidism related to ESRF and renal osteodystrophy was suspected in this patient. Based on the literature review, bone demineralization and mobilisation of lead from the bone store was reported to be a cause of endogenous lead exposure in ESRF patients.7 –10 In patients with renal osteodystrophy, the kidneys fail their function in maintaining normal calcium and phosphate homeostasis. The associated hyperphosphataemia and hypocalcaemia lead to hyperparathyroidism and increased bone turnover. 11 As 95% of environmental absorbed lead is stored in bones in adults, hyperparathyroidism and increased bone turnover cause increased lead mobilisation from the bone in ESRF patients. 7 This will result in a slight elevation of BLL in ESRF patients when compared with the normal population. An exogenous source of lead exposure is typically absent in these cases. 12 This type of endogenous lead exposure was also reported in other physiological states with calcium stress (e.g. pregnancy, lactation and osteoporosis) or calcium deficiency.
The slight elevation of BLL in this case was not compatible with lead neurotoxicity and it is unlikely the cause of peripheral neuropathy. Lead-induced peripheral neuropathy is one of the clinical manifestations of moderate to severe lead poisoning when BLL > 70–100 µg/dL in adults. Typical clinical presentation is primarily a motor weakness, initially in wrist and finger extensors, then other muscular involvements manifest as wrist drop and foot drop. Sensory involvement is generally minimal. 13 Other clinical features of lead poisoning such as anaemia, abdominal colic and encephalopathy are always present in patients with lead-induced peripheral neuropathy.
Case 2 ‒ risk of cyanide poisoning related to excessive bitter almonds consumption
A woman in her 50s attended the emergency department because of dizziness, headache, palpitation and shortness of breath. She had consumed a decoction 2 h ago, which was made by boiling 120 g of bitter almonds (北杏) in water. Cyanide poisoning related to excessive bitter almonds consumption was suspected. She was fully conscious and had stable vital signs upon presentation. Venous blood gas showed normal acid–base status. Serum lactate was not elevated. Based on the stable condition and the absence of lactic acidosis, the patient was unlikely to suffer from clinically significant cyanide poisoning. The use of cyanide antidote was not recommended. Her symptoms gradually resolved within several hours after in-patient observation. Qualitative analysis of cyanide in urine was negative and the patient was diagnosed to have mild bitter almond poisoning.
Cyanide poisoning is a rare cause of potentially fatal poisoning in Hong Kong. Cyanide compounds exposure is typically associated with smoke inhalation in fire victims, accidental exposure to laboratory or industrial chemicals and suicidal attempts. Many plant species contain cyanogenic glycosides and are considered as a potential cause of cyanide poisoning upon excessive consumption or improper preparation. The Prunus species consisting of apricots, bitter almonds, cherry and peaches have fruits containing the glycoside amygdalin. 14 When ingested, amygdalin is hydrolysed by intestinal enzymes to give hydrogen cyanide. Bitter almonds or bitter apricot seeds refer to 北杏 or 苦杏仁 in Chinese medicine. They are known to contain a higher amygdalin content when compared with sweet almonds or other Prunus species kernel. Accidental poisonings were well-reported in the literature and ingestion of 5–10 raw bitter almonds can result in severe toxicity in young children.15 –18 Early clinical features of cyanide poisoning are non-specific and may include gastrointestinal disturbances, dizziness, headache and weakness. Severe poisoning will progress to coma, seizures, cardiovascular collapse and severe lactic acidosis. Laboratory confirmation of cyanide poisoning is available in all acute public hospitals in Hong Kong, which includes qualitative cyanide screening and quantitative analysis of urine or blood samples. The turnaround time can be several hours for cyanide qualitative screening tests and two to 4 days for cyanide quantitative analysis. Due to the long turnaround time of cyanide tests, cyanide poisoning is diagnosed and treated clinically before the availability of laboratory confirmation in most circumstances.
According to a local study performed by the Centre for Food Safety, the uncooked bitter almonds contained an average content of 330 mg/kg free cyanide. A 98% reduction of free cyanide content was observed after cooking bitter almonds in boiling water for 15 min. 19 Cyanide poisoning after bitter almonds consumption is considered rare in Hong Kong as bitter almonds are always cooked or boiled before consumption in usual cooking recipes or Chinese herbal medicine practice. Adequate cooking or boiling can release the cyanide from bitter almonds and significantly reduce their toxicity. This observation may also explain the relatively mild symptoms and negative urine cyanide screening in our patient, who reported consumption of a large amount of boiled bitter almonds.
Case 3 ‒ LSD (Lysergic acid diethylamide)
An 18-year-old man was found to be wandering in the street with aggressive behaviour. He was put on physical restraint and brought to the emergency department. On examination, he was confused with irrelevant speech. There was diaphoresis and hyperthermia with a temperature of 37.6℃. His pulse rate was 173 beats per minute (bpm), pupils were 6 mm. Blood pressure could not be recorded initially as the patient was struggling. It was noted to be 115/56 mm Hg 15 min later. He reported to have ingested LSD (lysergic acid diethylamide) given by his friend but the details were not available. A total of 10 mg of midazolam and 50 mg diazepam was given intravenously in the first hour, together with a further 20 mg of diazepam 15 min later to control his sympathomimetic toxidrome. The serum creatine kinase level was peaked at 3982 U/L the next day (reference 39–308 U/L) and his other blood results were unremarkable. The patient’s confusion resolved the next day. In the urine specimen, LSD, diazepam, midazolam and temazepam were detected. Specific screening of novel psychoactive substances was negative.
LSD is a semi-synthetic hallucinogen structurally similar to serotonin (5-hydroxytryptamine; 5HT). 20 It has agonistic effect on the 5HT2A, 5HT1 and dopamine receptors. 21 It is a very potent abusive agent and is most commonly used in the form of small squares of liquid-impregnated ‘blotter’ paper, resembling the appearance of a stamp. It was widely used as a psychotropic drug in the 1960s. Abuse of LSD has resurged in Hong Kong in recent years. 21 A single case of LSD abuse was recorded in our system each year from 2014 to 2016, but the number of cases rose to three, eight and 14 in 2018, 2019 and 2020, respectively.
Although LSD is traditionally classified as a psychedelic and severe toxicity is thought to be rare, significant sympathomimetic features may also result from its abuse. Agitation, violent behaviour, hypertension, tachycardia and rhabdomyolysis after LSD use have been reported in a recent case series in Hong Kong. 22 Another concern in patients presenting with significant toxicities is the possibility of adulteration with other potent hallucinogens such as NBOMes (N-benzyl-oxy-methyl), DOC (dimethoxy-4-chloroamphetamine) and DOI (dimethoxy-4-iodoamphetamine), which may not be detected routinely by urine toxicology. 23 The prompt recovery of our case illustrated the importance of treating the sympathomimetic toxicity early in the emergency department.
Case 4 ‒ tramadol overdose (obtained from give-away of unused medications)
A woman in her 20s with repeated attempts of self-harm by drug overdose was brought to the emergency department for taking 70 capsules of tramadol (50 mg per capsule). She was noted to be semi-conscious, with a Glasgow Coma Score of E3V1M6 and sweaty. Her blood pressure was 122/94 mm Hg, pulse 90 bpm, temperature 37.2℃ and pupil size 3 mm. Her limb tones were increased but there was no ankle clonus. Haemoglucostix was 3.4 mmol/L and 20 g of dextrose was given intravenously followed by a dextrose infusion. The blood glucose level was 3.7 mmol/L and her other biochemistry results were normal. Her condition improved afterward. It was later noted that the tramadol was given to her freely by a member of a ‘self-help recycle group’ on social media who had some unused tramadol. The patient and her family refused psychiatric admission and she was discharged with acknowledgement of medical advice 3 days later.
Tramadol is a centrally acting analgesic that inhibits the reuptake of serotonin and noradrenaline, with a weak µ-opioid receptor agonistic effect. Tramadol overdose may produce nausea, vomiting, agitation, tachycardia, central nervous system and respiratory depression, seizure and serotonin syndrome. 24 Hypoglycaemia of about 2 mmol/L following tramadol overdose has also been reported.25,26 An increase in peripheral glucose utilisation and insulin levels have been proposed as the mechanisms for hypoglycaemia. 27
Giving away unused medicines to a stranger without medical consultation is a dangerous practice. Although most people share medications with good intentions, the danger of misuse of the medications, for example, the risk of improper indications, incorrect dosage, missing proper follow-up and so on would outweigh the benefits. While many thought that analgesics are harmless medications, an overdose of paracetamol and opioid analgesics may produce significant toxicity. Some opioid analgesics also have abuse potential and access to these medications in an unsupervised manner may increase the risk of abuse in some patients.
Case 5 ‒ multiple wasp stings
A man in his 50s enjoying good past health was attacked by wasps while cutting down a tree. He was stung more than 30 times on his scalp, limbs and trunk. He presented immediately to the hospital with itchy and painful swelling over the sting wounds. His vital signs were stable with no sign of anaphylaxis despite having multiple wasp stings. After more than 10-h of observation, he developed a low-grade fever and was found to have coagulopathy with prolonged activated partial thromboplastin time (APTT) > 200 s and prolonged prothrombin time (PT) of 16.3 s with an international normalised ratio (INR) of 1.4. His platelet count and haemoglobin were normal but the white cell count was raised at 13.4 × 109/L. His urea and creatinine concentrations were mildly raised at 9.8 mmol/L (reference 2.8–7.2 mmol/L) and 106 µmol/L (reference 59–104 µmol/L), respectively. His creatinine kinase was normal initially but raised slightly and peaked at 902 U/L (reference 61–399 U/L). He was admitted to the general medical ward with intravenous fluid and antibiotic treatment for the apparently infected pustular sting wounds. His renal function recovered in 24 h but the coagulopathy improved much slowly over the next four days without developing any bleeding complication. Both fibrinogen level and D-dimer concentration were raised on day 1 at 6.31 g/L (reference 1.85–3.83 g/L) and 1566.7 ng/mL (reference < 500 ng/ml), respectively. The platelet count of the patients had been normal during hospitalisation.
Coagulopathy after multiple wasps or bee stings has been well reported before. Many mechanisms have been proposed. One is heparin and tryptase released by mast cell activation as a part of venom-induced anaphylaxis. 28 Heparin exerts its anticoagulant effect by activation of antithrombin III while tryptase increases lysis of fibrinogen that could result in hypofibrinogenaemia. Heavy wasp and bee envenomation can result in disseminated intravascular coagulopathy. 29 Reduction of titres of multiple clotting factors independent of intravascular coagulation has also been reported. 30 Our patient presented with coagulopathy and mild renal function abnormality without clinical evidence of anaphylaxis which was typical for heavy wasp stings. A large review of 1091 wasp-stung patients in Hubei of China documented a 5.1% mortality, about 90% of deaths were due to multi-organ dysfunction instead of anaphylaxis. The envenomation syndrome comprised of coagulopathy, acute kidney injury, haemolysis, liver injury and rhabdomyolysis were observed in the severe cases. Wasp sting more than 10 times was associated with in-hospital mortality. 31 Massive wasp or bee sting can cause multi-organ dysfunction and even death. Clinicians should be aware of the danger of multiple-wasp/bee stings.
Case 6 ‒ cicada flower poisoning
A family of three adults developed dizziness two to four hours after consuming homemade meatball soup prepared with a total of 18 pieces of golden Chanhua (金蟬花), a type of cicada flower. They presented with vertigo, nausea, vomiting, hyperventilation and generalised weakness. Their vital signs were stable but the father and mother had a mildly elevated systolic blood pressure. All three recovered uneventfully after symptomatic treatment overnight. The clustering was highly indicative of a food poisoning event so biological and herb samples were collected for investigation. Similar to the herb Ophiocordyceps sinesis (冬蟲夏草) which was a fungus-infected moth caterpillar, the much less expensive herb golden Chanhua (Isaria cicadae) referred to cicada nymph infected by a specific fungus of the Isaria genus. It might be collectively grouped under the herb name of cicada flower (蟬花) that also included Ophiocordyceps sobolifera (小蟬花) and Ophiocordyceps cicadae (大蟬花). They were the same cicada nymphs but infected by different fungal species. Morphological examination by an expert mycologist on the unused herb revealed the presence of Ophiocordyceps sobolifera and an unexpected species Ophiocordyceps heteropoda that was potentially toxic.
Ophiocordyceps heteropoda had been identified to be the cause of 60 cases of poisoning after cicada nymph ingestion in Vietnam. 32 All patients in the case series reported dizziness, vomiting and salivation within one hour. About one-third of them developed more severe neurological symptoms that included agitated delirium, hallucination and seizure. Jaw stiffness was an interesting symptom among three patients. About 20% of the cases developed coma and one of them died with respiratory failure, hypotension and cardiac arrhythmias despite intensive care. The psychoactive compound ibotenic acid was detected from Ophiocordyceps heteropoda samples collected in the area. Ibotenic acid is well known to be present in the hallucinogenic mushroom species Amanita muscaria. It is psychoactive and neurotoxic in being a potent glutamate receptor agonist which can explain the spectrum of symptoms in the Vietnamese case series. In our cases, consumption of Ophiocordyceps heteropoda was the likely cause of the poisoning. However, we were not certain if Ibotenic acid was the culprit as subsequent chemical analysis of the unused herb sample did not find Ibotenic acid. Possible explanations included missing the toxic species on laboratory sampling or the presence of other unidentified toxic compounds in Ophiocordyceps heteropoda.
Case 7 ‒ slow K overdose with endoscopic removal of pharmacobezoar
A teenage girl with borderline personality disorder intentionally overdosed 30 tablets of slow K (potassium chloride extended released 600 mg). She remained asymptomatic and presented to the emergency department 1.5 h after ingestion. Her vital signs and physical examinations were normal. Initial blood tests showed hyperkalaemia 5.7 mmol/L, which increased to 6.0 mmol/L on repeated testing. ECG showed normal sinus rhythm with no hyperkalaemic changes. Calcium gluconate 10% 10 mL, sodium bicarbonate 8.4% 50 mL and regular human insulin 10 units with 25 g dextrose infused over 30 min were given intravenously. A dose of activated charcoal was given despite potassium is not adsorbed by charcoal. An abdominal X-ray (Figure 6(a)) showed multiple (more than 20) radio-opaque drug tablets in her stomach. Given the presence of multiple drug tablets in the stomach, gastric lavage was performed after intubation by rapid sequence induction (RSI) using etomidate and suxamethonium for airway protection and yielded one tablet only. Repeat X-ray (Figure 6(b)) showed similar pattern of radio-opaque tablets in the stomach and formation of pharmacobezoar was suspected. She was then transferred to paediatric intensive care unit (ICU) for close monitoring, with a dose of polystyrene sulphonate sodium 15 g given via nasogastric tube. Upper endoscopy was performed by paediatric surgeon after urgent consultation at post-ingestion 8 h during which activated charcoal was seen over her stomach. A total of 23 tablets were retrieved by a basket in multiple attempts. Post-endoscopy X-ray (Figure 6(c)) showed few remaining tablets passed beyond the stomach. The potassium level was peaked at 6.0 mmol/L in the ED and remained normal after admission. Her condition was stable and she was discharged to a psychiatric unit on day 2 after admission.
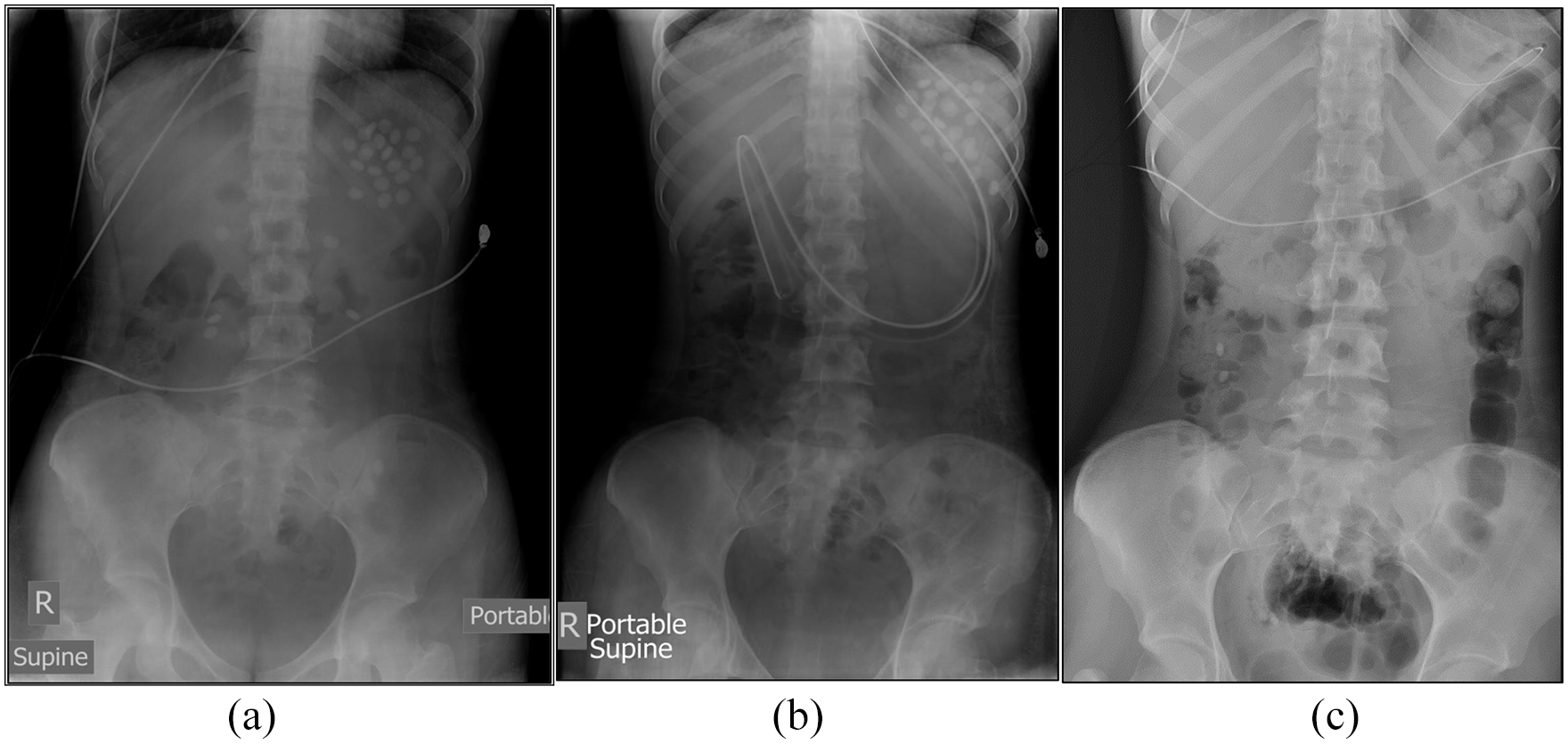
Case 7 abdominal X-ray (AXR): (a) on admission, (b) post-gastric lavage and (c) post-upper endoscopy.
Intentional potassium overdose is not common in Hong Kong. There have been only nine recorded cases related to potassium overdose in PICMS since 2007. The toxic dose of potassium is not well defined. Each tablet of slow K 600 mg contains 8mmol potassium. Dose as low as 2–2.5 mmol/kg (i.e. 2.5–3 tablets of slow K in a 10-kg child) can cause hyperkalaemia in patients with normal renal function. Management mainly includes medical therapy for hyperkalaemia, together with timely and appropriate gastrointestinal (GI) decontamination. Activated charcoal is ineffective in binding potassium. Its use may also obscure the view of endoscopy in case removal of drug clumps by upper endoscopy is required, as in our patient. Gastric lavage is often not useful as the slow K tablets are often too big to pass through the holes of the gastric lavage tube. The formation of pharmacobezoar also limits the usefulness of gastric lavage. Whole bowel irrigation is another GI decontamination option. Since our patient had hyperkalaemia and X-ray showed evidence of drug tablets with suspected pharmacobezoar formation inside the stomach and failed gastric lavage, urgent upper endoscopy was arranged. The successful removal of the slow K tablets by endoscopic technique renders our patient’s subsequent clinical wellness with a short duration of hospital stay. Finally, therapeutic use of suxamethonium during RSI can cause an increase in potassium level of 0.5–1 mmol/L in healthy individuals 33 and therefore should be avoided in case of potassium overdose with risk of hyperkalaemia.
Footnotes
Author contributions
We certify that we have each made a substantial contribution so as to qualify for authorship and that we have approved the contents.
Availability of data and materials
Not applicable. Not required in our previous annual report which is also published in this journal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Since this is an annual report with no patient contact and intervention involved, written informed consent was considered not necessary by our institution and no patient identifiable data has been included in the manuscript. Our previous annual reports were also published in this journal without informed consent.
Ethical approval
Ethical approval was applied and judged to be not required by the Research Ethics Committee (Kowloon Central/Kowloon East). Please see the attached letter for your reference.
Human rights
Patient’s right to privacy was not infringed in this study.