
Abstract
Introduction:
Flood syndrome is a rare and potentially fatal complication of liver cirrhosis with gross ascites.
Case presentation:
We present a case of Flood syndrome in a gentleman with alcoholic cirrhosis and ascites who had sudden spontaneous rupture of umbilical hernia, resulting in sudden gush of ascitic fluid from the hernia. The wound was cleaned and covered in sterile dressing and was admitted for further management. His umbilical hernia wound was closed at bedside by General Surgery team and he underwent ultrasound-guided ascitic drain insertion by Interventional Radiology. His stay was complicated by bacterial peritonitis which was treated with intravenous antibiotic. Patient eventually recovered and was discharged well.
Discussion:
Flood syndrome has high complication and mortality rate. Recent reported cases were reviewed, focusing on the causes of cirrhosis, complications of Flood syndrome, treatments provided and the outcomes.
Conclusion:
There is currently no standard guideline for the management of Flood syndrome which falls in the grey area between medical and surgical management. Proper medical management with early surgical consultation is important to reduce the morbidity and mortality for these patients.
Introduction
Ascites is a common event in the natural disease progression of liver cirrhosis, and is associated as a marker of morbidity and mortality in patients with liver cirrhosis. The increased intra-abdominal pressure from ascites pushes the peritoneum through the umbilical ring into the subcutaneous space, leading to the formation of umbilical hernia. 1 The prevalence of umbilical hernia in cirrhotic patients with ascites is about 20%. 2 The ascites filled subcutaneous peritoneal sac which is in direct contact with the skin causes the attenuation of the skin, leading to ulceration and possible rupture. 1
Within this subgroup of patients with umbilical hernia, spontaneous rupture of umbilical hernia may occur infrequently. First described by Johnson in 1901, 3 this rare and potentially life-threatening condition is also known as ‘Flood syndrome’, named after Frank B. Flood who described five such cases in 1961. 4 Flood syndrome, albeit rare, carries with it various complications and a high mortality rate. Among the complications of Flood syndrome that has been reported include peritonitis, cellulitis, sepsis, bowel strangulation, evisceration and death. We present a rare case of Flood syndrome in a man who presented to our emergency department and discuss its management.
Case report
A 77-years-old gentleman presented to our Emergency Department with a sudden gush of approximately 3–4 L of fluid from his pre-existing umbilical hernia about 1 h prior to his presentation. He complained of a very tense and distended abdomen which was relieved with the spontaneous leakage of fluid from the umbilical hernia. He denied any prior trauma, abdominal pain, bleeding or fever. He had a background of Child’s B alcoholic liver cirrhosis (Model for End-stage Liver Disease score = 18) complicated by esophageal varices, portal hypertension and diuretic intolerant recurrent ascites. This patient had been requiring bi-weekly paracentesis for ascites drainage, and was due for his next paracentesis in 3 days. He had also previously declined transjugular intrahepatic portosystemic shunt (TIPS).
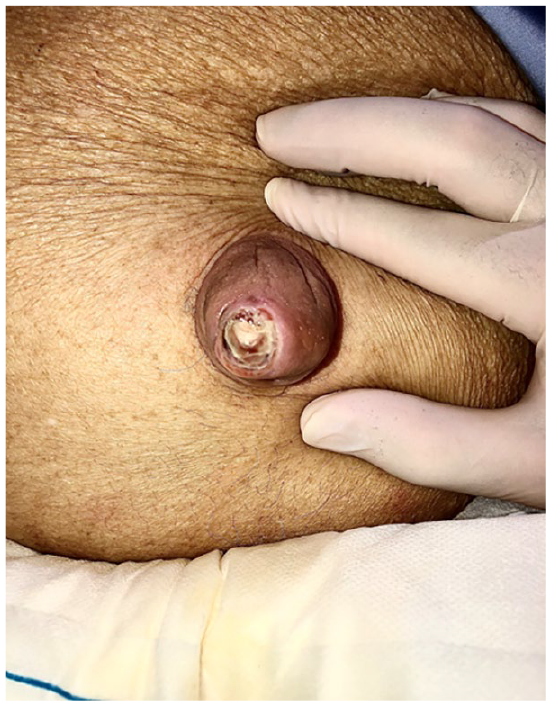
Physical examination revealed a soft, mildly distended and non-tender abdomen with splenomegaly 8 finger-breadths below the left subcostal margin. There was an erythematous umbilical hernia with a non-bleeding ulcer at the tip of the hernia from which straw-coloured ascitic fluid was actively draining. He had bilateral lower limb pitting edema with scrotal and penile skin edema. Otherwise, he was hemodynamically stable and afebrile without any signs of hepatic encephalopathy and asterixis. His white blood cell count was 5.56 × 109/L (reference range 4–10 × 109/L), Hb 9.2 g/dL (reference range 14–18 g/dL) and platelet count of 164 × 109/L (reference range 140–440 × 109/L). Other significant results include serum urea level of 20.8 mmol/L (reference range 2.7–6.9 mmol/L) and serum creatinine level of 185 µmol/L (reference range 54–101 µmol/L). His liver function test was normal apart from serum albumin level of 36 g/L (reference range 40–51 g/L).
The wound was cleaned and covered in a sterile gauze dressing, and he was admitted to Gastroenterology department for further management. Urgent non-contrasted Computed Tomography of the abdomen and pelvis was done, which reported cirrhotic liver with associated changes of portal hypertension. There was gross ascites with umbilical hernia containing fluid and no bowel seen within the hernia. He was reviewed by the General Surgery team who deemed that his risk for emergency operation was too high and proceeded with closure of the umbilical hernia ulcer at bedside. Patient underwent ultrasound-guided ascitic drain insertion by interventional radiology and drained a total of 8.5 L of ascitic fluid. His stay was complicated by bacterial peritonitis (ascitic fluid cell count reported 2139 neutrophils/mm3) for which he was treated with IV Ceftriaxone and IV Metronidazole. Patient eventually improved and the ascitic drain was removed and he was discharged well after 6 days. Follow-up 1 week later revealed that the ulcer had healed completely.
Discussion
Flood syndrome, described as a sudden gush of fluid from spontaneous umbilical hernia rupture, is a rare and potentially life-threatening complication of chronic ascites and end-stage liver disease. 5 Mortality rate as high as 30% has been reported. 6 Although it was first described by Johnson in 1901, 3 there has been little data since then regarding its management. About 20% of cirrhotic patients with ascites will develop umbilical hernia during the course of their disease. 7 This is due to the interruption of linea alba at the umbilicus resulting in a site of weakness at the anterior abdominal wall, 8 allowing protrusion of peritoneum, fluid, omentum or even bowels from the raised intra-abdominal pressure. In these patients, the peritoneum and the overlying skin of the umbilical hernia can breakdown completely, resulting in expulsion of intra-abdominal contents. In 81% of the cases, ulceration of the skin overlying the umbilical hernia was reported prior to the rupture. 9 Spontaneous rupture of the umbilical hernia may result in drainage of ascitic fluid, also known as ‘spontaneous paracentesis’, and in rarer cases, may even result in evisceration of bowel or omentum.10,11
Complications that may arise from Flood syndrome include bacterial peritonitis, cellulitis of abdominal wall, sepsis, incarceration or strangulation of bowel and renal or hepatic failure. 11 Loss of large volume of ascitic fluid may also lead to hemodynamic instability and death. 12 The main aim of management in ED should focus on hemodynamic stabilization and prevention of infectious complications. 10 The wound should be cleaned and covered in sterile dressing. Patient should be started on a broad-spectrum antibiotic covering skin flora and organisms causing bacterial peritonitis as per local hospital guidelines. 13 Patient should also receive IV fluids if large volume spontaneous paracentesis has occurred due to risk of hemodynamic instability.
Although there has been case reports and studies done looking at the management of Flood syndrome, standard treatment protocol is yet to be developed as the cases are so rare. The decision for delayed hernia repair after medical optimization versus emergent herniorrhaphy is still made on an individual basis. 13 The various etiologies, complications, treatments and outcomes of cases published since 2000 are listed in Table 1.
Cases of Flood syndrome published since 2000.
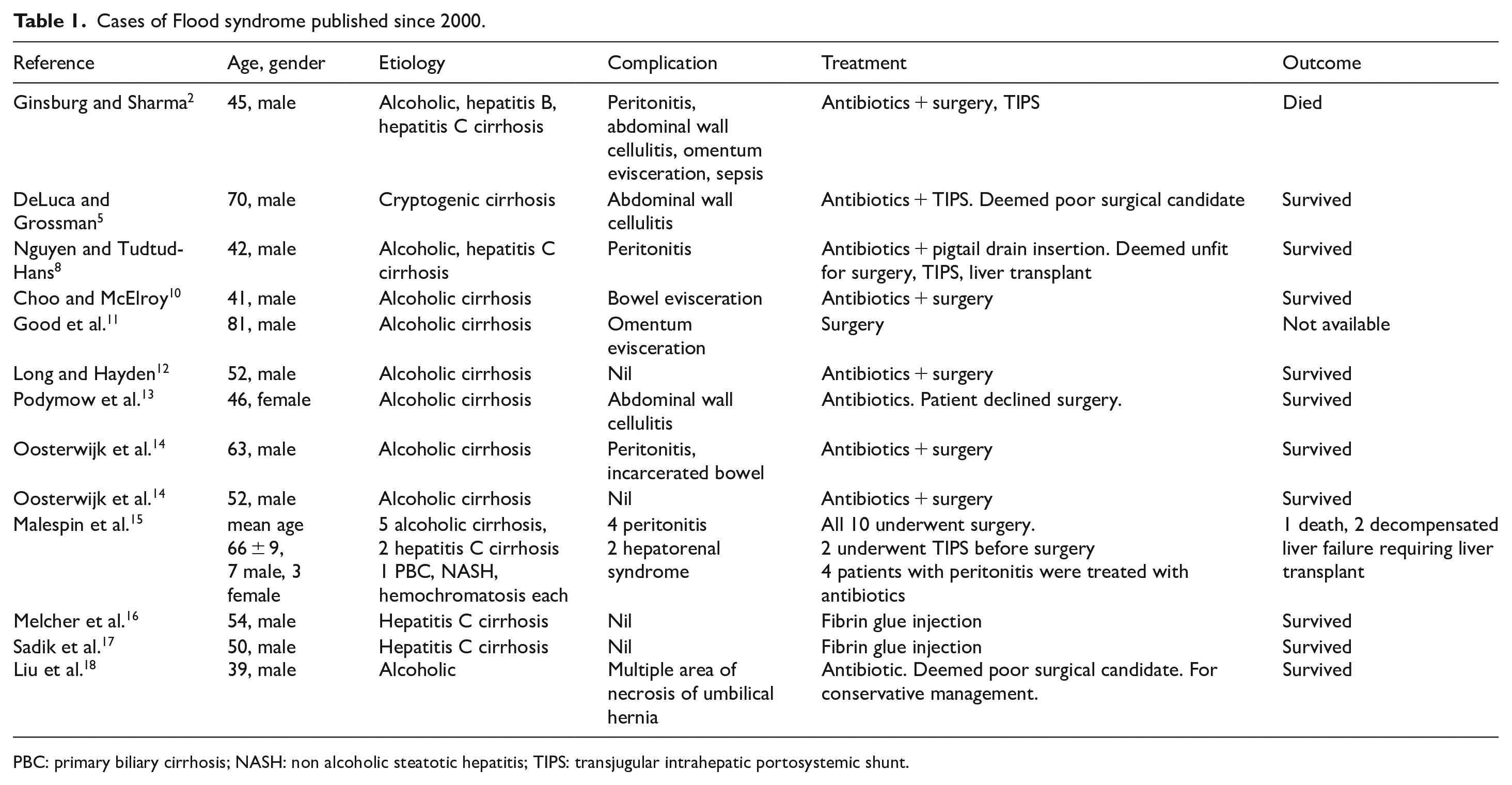
PBC: primary biliary cirrhosis; NASH: non alcoholic steatotic hepatitis; TIPS: transjugular intrahepatic portosystemic shunt.
Traditionally, surgical repair of umbilical hernia has been reserved for patients who had developed complications such as rupture or evisceration due to the high mortality rate.6,7 This is because ascites is a major risk factor for surgery and is associated with high risk of mortality. 2 Besides that, patients with cirrhosis may develop patent umbilical vein which if ligated during umbilical hernia repair, may lead to portal circulation outflow obstruction causing acute portal vein thrombosis and acute liver failure, necessitating emergency liver transplant.14,18
However, a recent study by Triantos et al. 6 has recommended elective hernia repair as it prevents complications and thus avoid the need for an emergency hernia repair which has high mortality. This was supported by Ginsburg and Sharma 2 which stated that elective hernia repair carries 2% risk of mortality, whereas emergency hernia repair due to rupture, strangulation or incarceration is associated with 14% risk of mortality. Oosterwijk et al. 14 also recommended elective hernia repair after optimal management of ascites to prevent spontaneous rupture of umbilical hernia.
A case series by Malespin et al. 15 on 10 liver cirrhosis patients with ruptured umbilical hernia who underwent emergency repair reported poor post-surgical outcome in 30% of the patients (one death and two decompensated liver failure followed by urgent liver transplant). Other alternative management techniques for ruptured umbilical hernia that have been described include injection of fibrin glue into the defect to stop the ascitic leakage,16,17 and placement of pigtail drain to allow the ulcer to heal by itself. 8
Conclusion
Flood syndrome is rare, and it can be potentially fatal if not managed appropriately. There is no standard guideline with regards to the management of Flood syndrome. This presents a difficult conundrum for the emergency physicians with regards to the disposition of such patients as it falls in the grey area between medical and surgical management. Hence, emergency physicians should be aware of this condition and ensure proper medical management and involve early surgical consultation for these patients to reduce morbidity and mortality.
Footnotes
Author contributions
Dr Daniel wrote the first draft of manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Informed consent
Written informed consent was obtained from patient’s son for anonymized patient information to be published in this article.
Ethical approval
As this is a case report, no ethical approval was required to be obtained.