
Abstract
Background:
An outbreak of coronavirus disease 2019 (COVID-19) took place in Wuhan, China, by the end of 2019, and the disease continues to spread all over the world. The number of patients is increasing rapidly, a large number of infected patients is critically ill, and the mortality is high. However, information on COVID-19 patients is limited, and its clinical characteristics have not been fully studied.
Objectives:
To compare the performances of point-of-care lung ultrasound (LUS) and bedside chest X-ray in assessing the condition of COVID-19 patients with acute respiratory distress syndrome (ARDS).
Methods:
This observational study enrolled 42 COVID-19 patients with ARDS who were admitted to the Department of Critical Care Medicine of the Wuhan Union Hospital from February to April 2020. The point-of-care LUS characteristics of the COVID-19 patients with ARDS were summarized, and the performances of LUS and bedside chest X-ray in assessing the patient’s condition were compared.
Results:
Most of the 42 patients were elderly individuals with chronic clinical diseases. The proportion of patients older than 60 years old was 85.7%. All patients were given invasive mechanical ventilation; eight (19.0%) of them received venovenous extracorporeal membrane oxygenation support. LUS has evident advantages in detecting lung consolidation, patchy shadows, and pleural thickening, and pleural line changes in particular. The receiver operating characteristic analysis indicated that the sensitivity, Youden index, and kappa value for detecting COVID-19 patients with ARDS were higher for LUS than the chest X-ray.
Conclusion:
LUS has better diagnostic accuracy and sensitivity in COVID-19 patients with ARDS than the chest X-ray.
Background
The severity of the outbreak of the coronavirus disease 2019 (COVID-19) in Wuhan, China, has been increasing since December 2019, and the disease has spread rapidly to other parts of mainland China.1–3 So far, the number of COVID-19 patients continues to rapidly rise worldwide. A large number of infected patients are in critical condition. A recent single-center clinical study published in The Lancet Respiratory Medicine 3 documented that severe cases of COVID-19 are characterized by a 61.5% mortality rate. The 61.5% mortality rate is often associated with acute respiratory distress syndrome (ARDS). Some studies call the COVID-19 associated with ARDS as “CARDS,” and these patients can be assigned in a simplified phenotype, “L” (low lung elastance, low recruitability), 4 but the clinical characteristics of CARDS patients still remain not very clear. Moreover, frequent pulmonary imaging of these patients is very difficult, necessitating the development of a convenient, fast, and rapid new diagnostic strategy for severe COVID-19.
Point-of-care lung ultrasound (LUS) is a noninvasive, convenient tool for real-time imaging of the lung. Since the application of LUS in the diagnosis and treatment of pulmonary diseases in 1997, it has been widely used in Western countries in the diagnosis and treatment of respiratory failure and other pulmonary diseases in critically ill patients. Moreover, it can be applied in early diagnosis and screening of pneumonia patients, as well as in the evaluation of the effects of the treatment.5,6 This technology is highly practical and can be easily mastered by clinicians after rather simple training. It has been documented that in an under-resourced setting, LUS had greater diagnostic accuracy in patients with pneumonia than chest X-ray.7,8 Thus, the use of LUS can solve the problems inherent in currently used imaging examination and auscultation for severe COVID-19 patients.
The present study summarizes the LUS characteristics of patients with ARDS due to COVID-19, admitted to the Department of Critical Care Medicine (CCM) in the Wuhan Union Hospital from February to April 2020. The performances of LUS in assessing the patient’s condition are compared with those of bedside chest X-rays. It is expected that these results will be valuable for the first-line physicians and help them in the care of severely ill COVID-19 patients.
Methods
Study design and setting
This investigation was designed as an observational study of COVID-19 patients admitted to the Department of CCM at the Wuhan Union Hospital (Wuhan, China), and approved by the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (ClinicalTrials. 0027). Patients diagnosed with CARDS were followed from February to April 2020. All examinations and data collection during this period were with the consent of the patient’s relatives by telephone. All patients were diagnosed according to the World Health Organization (WHO) interim guidelines. 9 The diagnosis of ARDS was based on an international consensus criterion, the Berlin definition. 10 The exclusion criteria were severe heart failure (unable to engage in any physical activity, heart failure can occur at rest), interstitial pneumonia, obesity (body mass index (BMI) ≧ 28), and age <18 years.
Data collection
Electronic medical records, nursing records, laboratory findings, radiological examinations, ultrasound imaging, and data obtained at the admission were analyzed. All included patients had COVID-19 confirmed by laboratory tests (detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) nucleic acid by reverse transcription polymerase chain reaction (RT-PCR)) and clinical symptoms.
LUS examination
A series of point-of-care LUS examinations were conducted on the first day of admission to Department of CCM and every day thereafter. LUS was performed according to a standard operating procedure 11 using a Wisonic Clover 60 ultrasound instrument (Shenzhen Wisonic Medical Technology Co., Ltd, Shenzhen, China). A convex abdominal probe (5 MHz) was employed, and the views were obtained according to the bedside lung ultrasound in emergency (BLUE) protocol.12,13 The LUS examinations were completed by two senior POCUS (point-of-care ultrasound) trainers of Department of CCM of our hospital. Lung sliding and pleural thickness were determined using the linear vascular probe (>10 MHz). Patients were examined in the supine and discontinuous prone position, except for those on mechanical ventilation when the prone position was necessary. Ultrasonography data were stored in real time for post hoc quality assurance.
LUS outcomes interpretation
Each BLUE point and posterolateral alveolar or pleural syndrome (PLAPS) point of both hemithoraces were determined as follows: N (normal); B1, B2, S (shred sign); or C (consolidation). Specifically, N corresponded to predominantly A-lines, that is, the image of normal lung tissue; B1 reflected predominantly multiple diffuse B-lines, representing a mild/moderate interstitial edema of lung tissue; and B2 corresponded to predominantly multiple diffuse coalescent B-lines, representing severe interstitial edema/alveolar edema. S-profile indicated the presence of the shred sign, also called rag sign; the shred sign is typically absent in a larger whole-lobe consolidation and is the primary sign of localized pneumonia. C-profile indicates pulmonary consolidation. 14
Radiologic examination
Chest X-rays were administrated on days 0, 3, and 6 after the admission using a portable chest X-ray machine in AP (anteroposterior) position. During this period (on days 0–6), chest computed tomographic (CT) scans were performed one time on patients from the level of the thoracic inlet to the diaphragm. The images were reviewed by senior radiologists who were unaware of the LUS findings and the condition of patients. The chest X-ray and CT were read by the different radiologist. Chest CT images were considered the gold standard for composite reference.
Statistical analysis
Categorical variables are presented as counts and percentages, and continuous variables as mean ± standard deviation (SD). The statistical significance of the differences was determined by a two-sample t-test for continuous variables and Fisher’s exact test for categorical variables. The receiver operating characteristic (ROC) curve was used for the sensitivity and specificity analysis. Data were analyzed using SPSS 22.0 software (IBM SPSS, Chicago, IL, USA). The p value of less than 0.05 was considered statistically significant.
Results
Patient characteristics
In total, 42 patients were enrolled in the study between February and April 2020 (Table 1). All the patients are local residents of Wuhan, no tourist, and seven of whom are medical staff or retired staff of our hospital. Their mean age was 68.1 years (range: 28–86 years), 18 patients (42.9%) were male, and 24 patients (57.1%) were female. The proportion of patients older than 60 years old was 85.7%. Eight patients (19.0%) were treated with venovenous extracorporeal membrane oxygenation (VV-ECMO), all patients (100%) received endotracheal intubation and mechanical ventilation, 15 patients (35.7%) received intermittent prone position ventilation, 3 patients (7.1%) received the recruitment maneuver (RM), and a tracheotomy was administered to 11 patients (26.2%); 88.1% patients had chronic diseases, including hypertension in 30 (71.4%) patients, type 2 diabetes mellitus in 14 (33.3%) patients, chronic cardiac disease (except hypertension) in 12 (28.6%) patients, and chronic pulmonary disease in 9 (21.4%) patients. Lower fractions of patients suffered from hypothyroidism, hyperuricemia, cerebral infarction, hyperlipidemia, and chronic renal insufficiency.
Baseline characteristics of COVID-19 patients with ARDS..
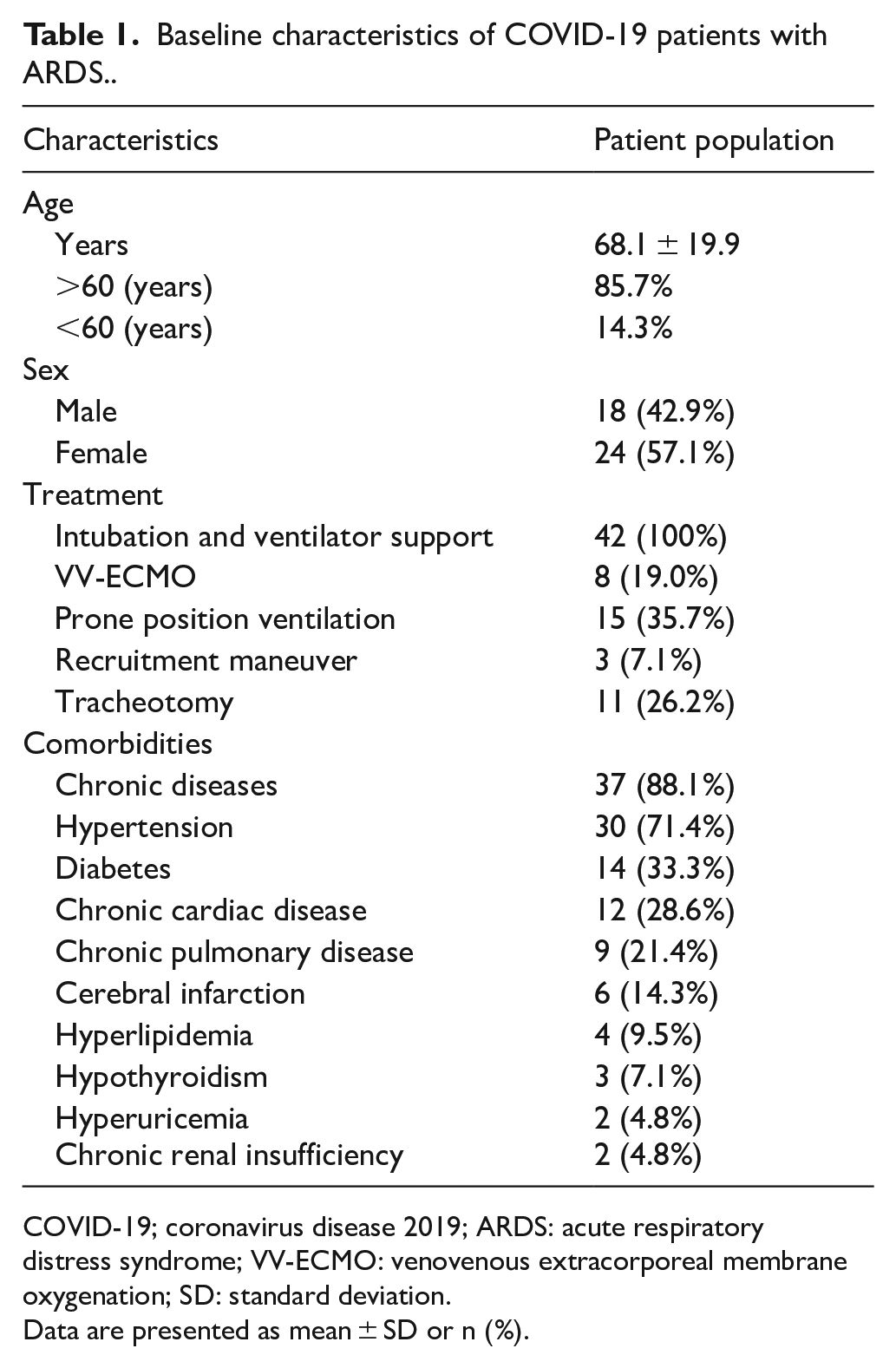
COVID-19; coronavirus disease 2019; ARDS: acute respiratory distress syndrome; VV-ECMO: venovenous extracorporeal membrane oxygenation; SD: standard deviation.
Data are presented as mean ± SD or n (%).
Presence of CARDS based on LUS and chest X-ray
The Berlin definition of ARDS is widely used in clinical practice, but it does not provide a precise evaluation standard for chest X-ray, making the diagnostic reliability of ARDS poor. 15 The current clinical observations (Table 2) have shown that COVID-19 patients with ARDS consistently manifest alveolar interstitial syndrome (AIS) in the front chest wall (85.7%–100%) indicated by multiple diffuse coalescent B-lines (Figure 1), a large area of pulmonary consolidation (71.4%–95.2%) with the shred sign (80.9%–95.2%) on the PLAPS point (Figure 2) accompanied by general pleural thickening (Figure 3) in the anterior and posterior regions (76.2%–95.2%). In addition, part of the patients had a small amount of pleural effusion (23.8%–47.6%; Figure 4), and a few had a pneumothorax (9.5%).
The outcome of LUS and chest X-ray on days 0, 3, and 6 after the admission to Department of CCM.
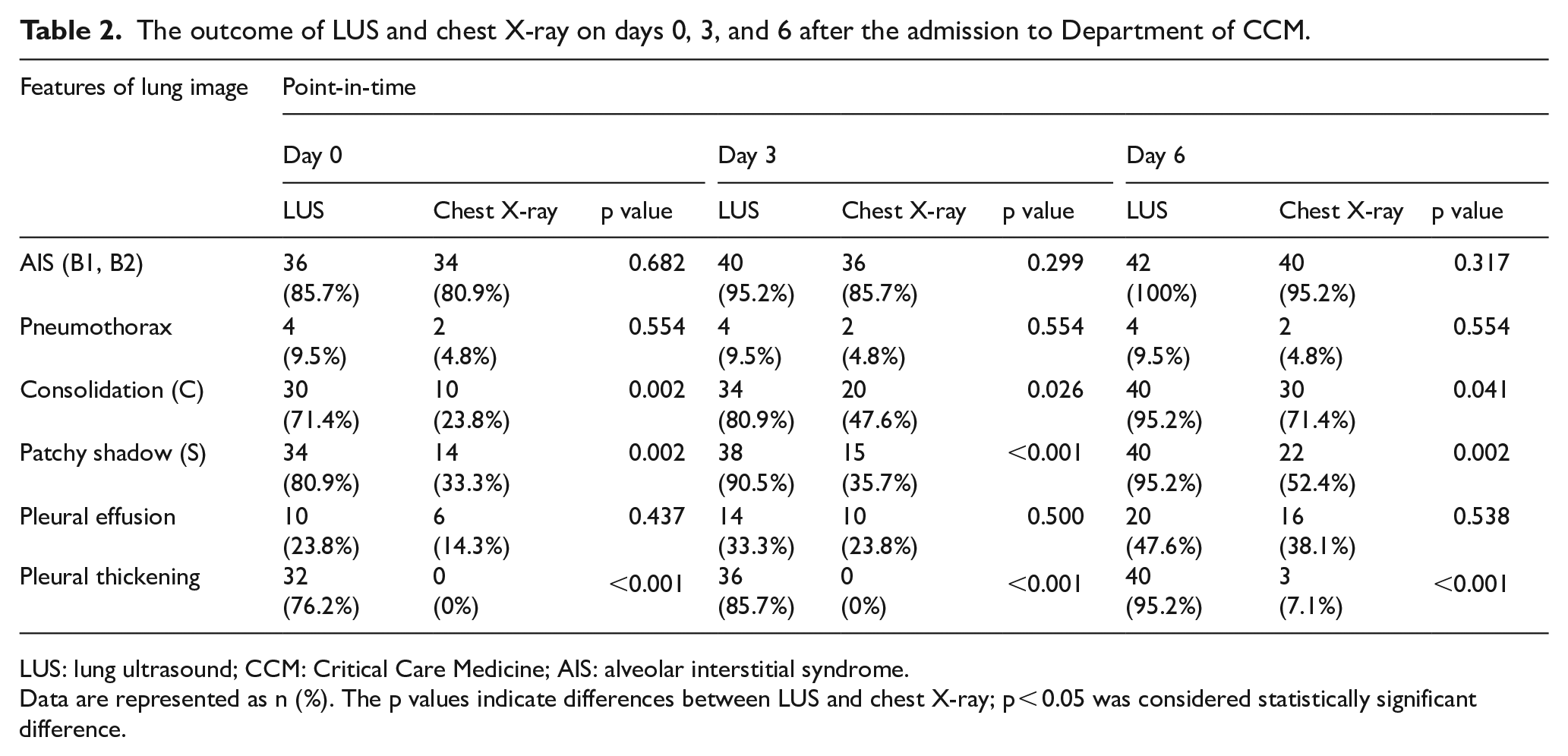
LUS: lung ultrasound; CCM: Critical Care Medicine; AIS: alveolar interstitial syndrome.
Data are represented as n (%). The p values indicate differences between LUS and chest X-ray; p < 0.05 was considered statistically significant difference.
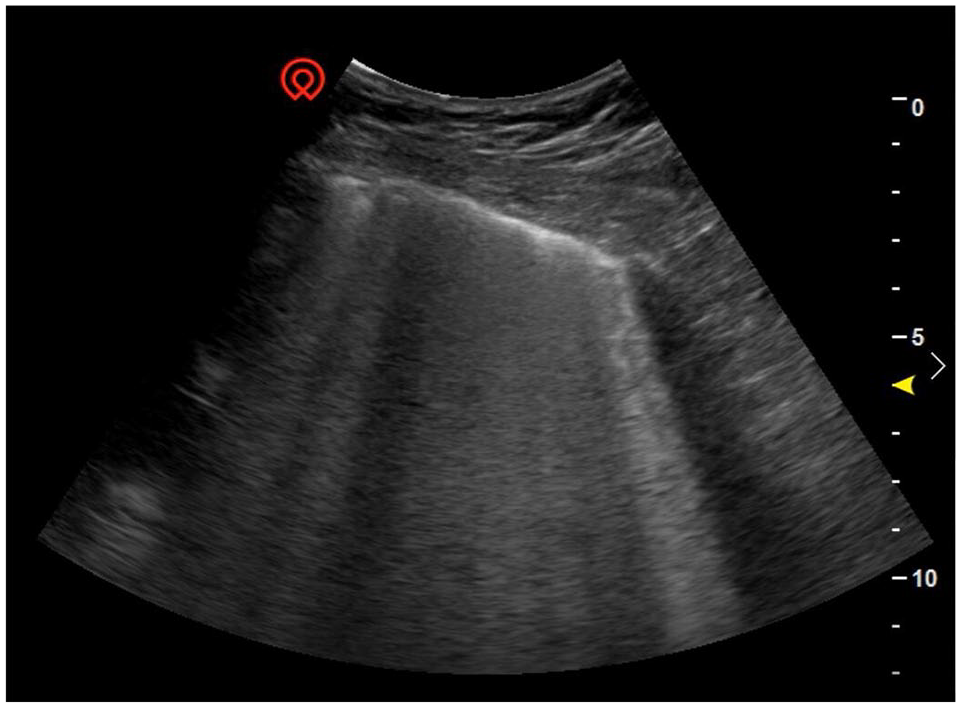
The presence of multiple diffuse coalescent B-lines in the front chest wall represents alveolar interstitial syndrome.
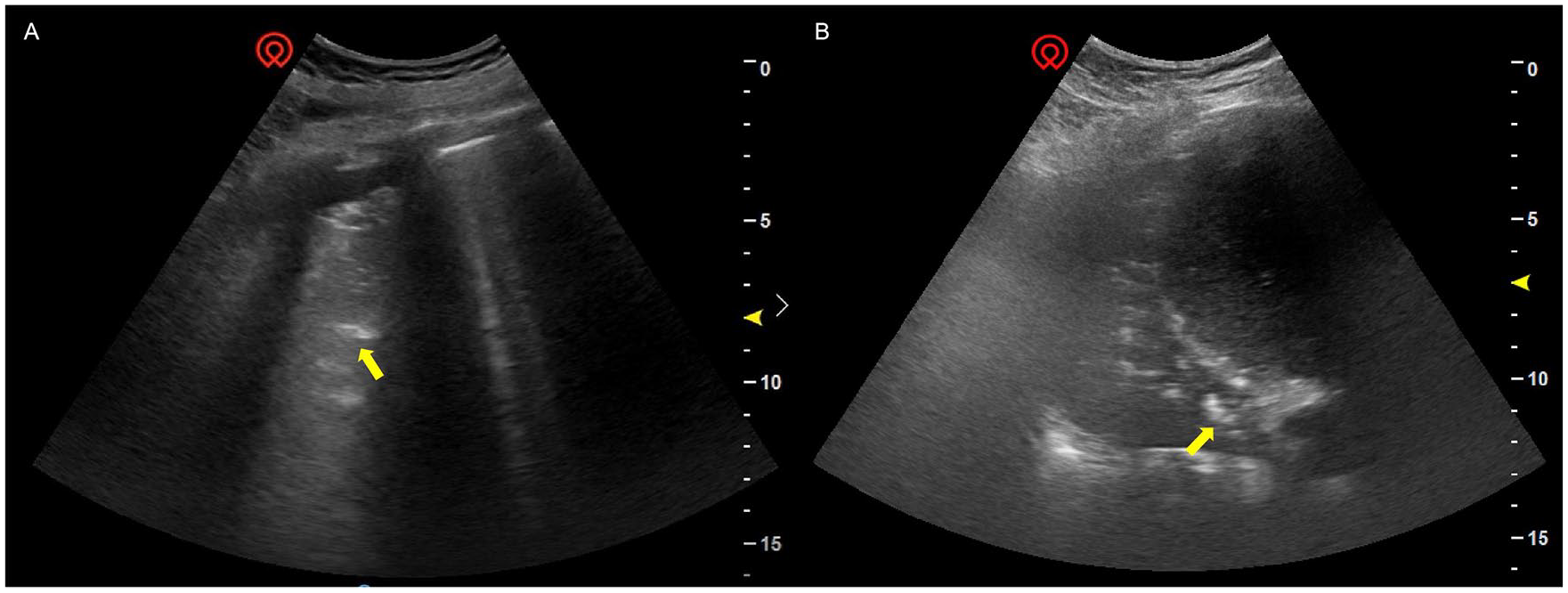
The sonographic sign of lung consolidation and shred sign (yellow arrow) which reflects a tissue-like echotexture in the PLAPS point (A: longitudinal section, B: transverse section).
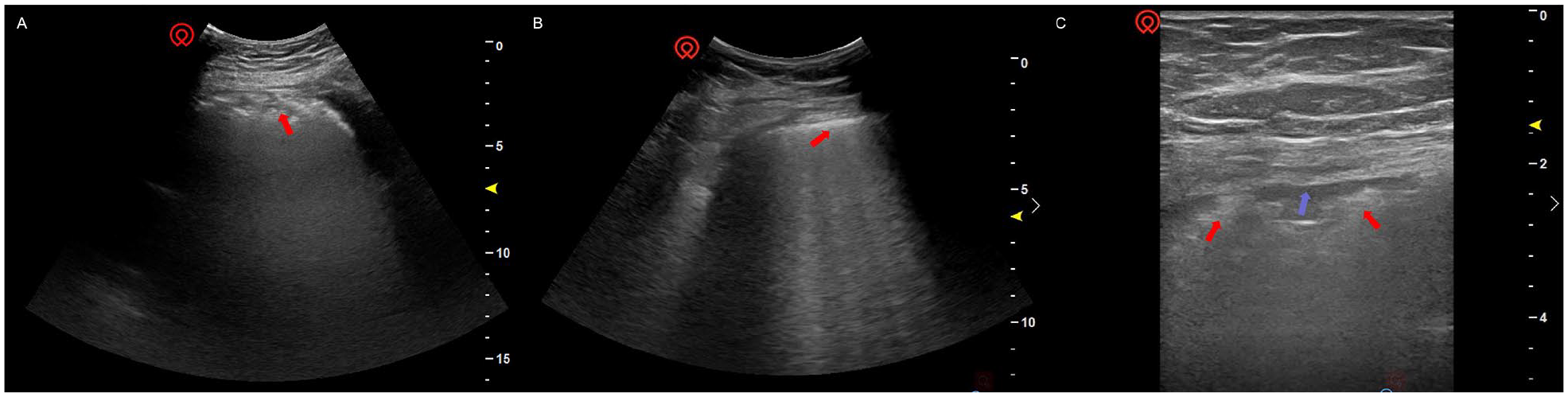
Irregularly thickened and rough pleural line obtained with a convex abdominal probe (A, B) and linear vascular probe (C) (red arrow), accompanied by a small amount of pleural effusion (blue arrow).
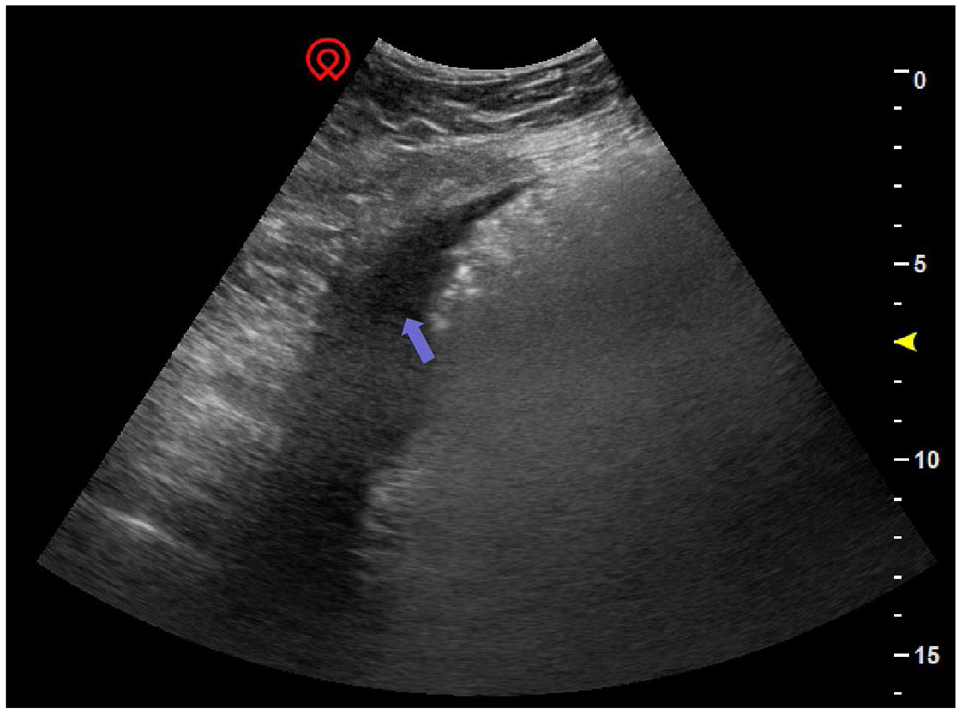
The presence of a small amount of pleural effusion (blue arrow) in the PLAPS point.
The radiological examination of ARDS by the chest X-ray was conducted on days 0, 3, and 6 after the admission. As shown in Table 2, although LUS identified more patients with AIS than chest X-ray, there was no statistical difference between the two methods (p = 0.682 on day 0, p = 0.299 on day 3, and p = 0.317 on day 6). However, LUS detected significantly higher number of cases of consolidation (p = 0.002 on day 0, p = 0.026 on day 3, and p = 0.041 on day 6), patchy shadow (S) (p = 0.002 on day 0, p < 0.001 on day 3, and p = 0.002 on day 6), and pleural thickening (p < 0.001 on day 0, p < 0.001 on day 3, and p < 0.001 on day 6) than the chest X-ray. The detection of pleural effusion by LUS on days 0, 3, and 6 was consistent with the chest X-ray results, with p values of 0.437, 0.500, and 0.538, respectively. LUS and chest X-ray on the pneumothorax were similar at all three time points, with a p value of 0.554. There was a higher prevalence in the pleural line detected using LUS compared with chest X-ray, with the rate of 76.2% versus 0% on day 0 (p < 0.001), 85.7% versus 0% on day 3 (p < 0.001), and 95.2% versus 7.1% on day 6 (p < 0.001).
Diagnostic accuracy of LUS and chest X-ray in detecting CARDS
Chest CT images were considered the gold standard for composite reference. Table 3 lists the results of the ROC analysis showing sensitivity, specificity, Youden index, and kappa and p values for the diagnostic consistency between LUS and chest X-ray in the diagnosis of CARDS. AIS, lung consolidation, and patchy shadow in the bilateral lung were the major clinical features that occurred at sufficient frequency to allow the calculation of the sensitivity, specificity, and the Youden index in the diagnosis of CARDS by LUS. The respective values were 94.4% (sensitivity), 66.7% (specificity), and 61.1% (Youden index) in detecting AIS; 93.8% (sensitivity), 60.0% (specificity), and 53.8% (Youden index) in detecting consolidation; and 94.1% (sensitivity), 75.0% (specificity), and 69.1% (Youden index) in detecting patchy shadow. The analysis of the application of the chest X-ray to diagnose CARDS showed that the sensitivity, specificity, and the Youden index were 62.5%, 60.0%, and 22.5% in detecting AIS; 75.0%, 40.0%, and 15.0% in detecting consolidation; and 52.9%, 50.0%, and 2.9% in detecting patchy shadow, respectively. In the detection of CARDS, the sensitivity and the Youden index were higher for LUS than for the chest X-ray. LUS had higher diagnostic consistency for CARDS with the kappa and p values of 0.611 and 0.005 (AIS), 0.577 and 0.008 (consolidation), and 0.691 and 0.002 (patchy shadow) compared to chest X-ray for CARDS with the kappa and p values of 0.176 and 0.375 (AIS), 0.140 and 0.517 (consolidation), and 0.019 and 0.916 (patchy shadow), respectively.
Diagnostic accuracy of LUS and chest X-ray in the diagnosis of CARDS..
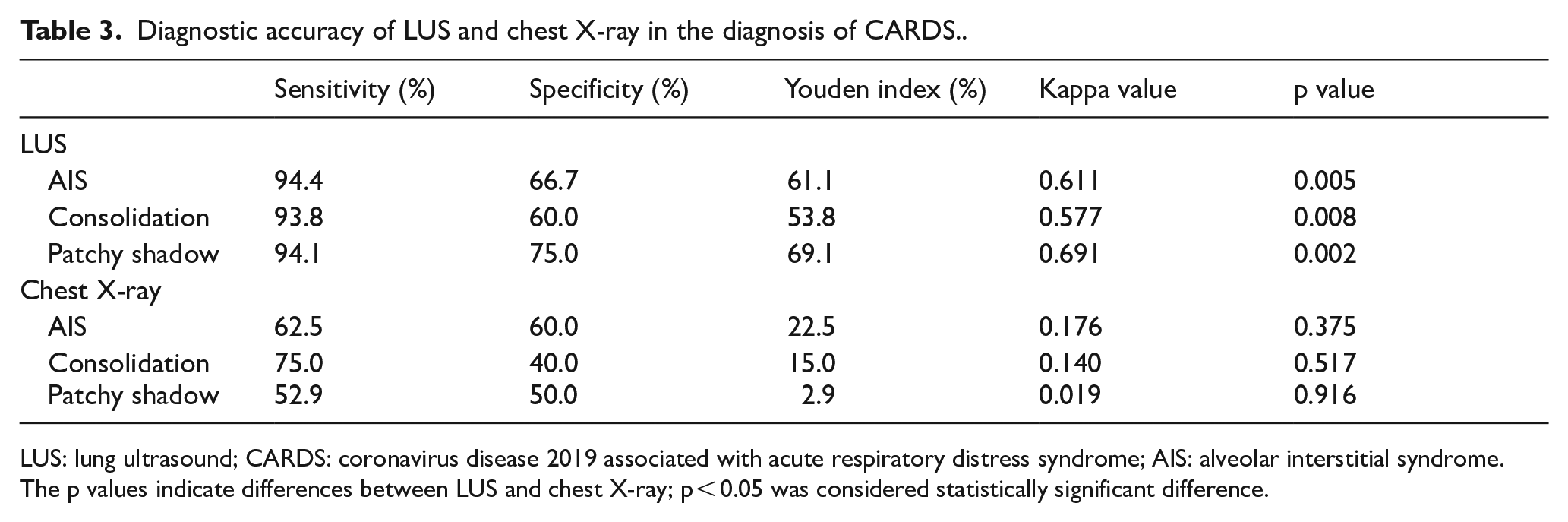
LUS: lung ultrasound; CARDS: coronavirus disease 2019 associated with acute respiratory distress syndrome; AIS: alveolar interstitial syndrome.
The p values indicate differences between LUS and chest X-ray; p < 0.05 was considered statistically significant difference.
Discussion
The mortality and morbidity of COVID-19 critically ill patients were very high in the world.3,16,17 For these COVID-19 patients, performing the auscultation and CT imaging outside the Department of CCM is very difficult, and bedside chest X-ray has its diagnostic limitations. Based on these constraints, we have chosen LUS, a noninvasive, convenient, real-time detection instrument, as the tool for the daily examination and functional assessment of lung and other organs. The present observational study of 42 critically ill COVID-19 patients with ARDS lists the main pulmonary ultrasound signs and compares the sensitivity and specificity of LUS and bedside chest X-ray in the diagnosis and assessment of this type of patients.
The patients were mostly older people with chronic diseases, most commonly hypertension, diabetes, and chronic cardiac disease. The high proportion of patients over 60 years old, 85.7%, may be attributed to the presence of acute or chronic comorbidities and lower reserve capacity in most important organs and systems, which can reduce the ability to cope with physical stress.6,18 All patients were given invasive mechanical ventilation, but only eight (19.0%) received VV-ECMO support. The reasons for this relatively low number were mostly insufficient availability of ECMO machines and the old age of the patients, which is a contraindication for ECMO. Prone position ventilation for more than 12 h/d was provided to 35.7% of the patients, but the clinical observations indicated that its benefit was very limited. Only a small number of patients underwent the RM, mainly because most patients had poor lung compliance and were prone to barotrauma. These findings will be analyzed in more detail in subsequent studies.
Together with sepsis, septic shock, respiratory failure, and heart failure, ARDS is a frequently observed complication in COVID-19 patients and is also a major cause of high mortality. 18 At present, the methods for improving the accuracy of CARDS diagnosis are limited, and the dynamic assessment of the progress in its treatment is challenging.19,20 Typically, elderly patients have a higher number of complications and poorer self-repair ability. The diagnosis and assessment of CARDS in this patient population are even more difficult. 21 Therefore, improvement is necessary in early and precise diagnosis, and assessment and intervention are critical for the improvement of prognosis and survival rate of COVID-19 patients with ARDS to ensure a better prognosis and survival rate.
Since the outbreak of the novel coronavirus, the diagnosis and treatment of COVID-19 patients with ARDS at our department are largely based on the changes in the lungs observed using LUS, a novel way imaging method for CARDS diagnosis. The present observational study documented clear advantages of LUS in detecting lung consolidation, patchy shadows, and pleural thickening. In particular, by detecting the changes in pleural line changes, LUS can provide accurate information on pleural thickening, roughness, and associated localized pleural effusion. This information helps us understand the condition of the patient’s lungs in more detail, so that we can take further treatment measures. For example, the patients with large areas of consolidation and patchy shadows may be considered for prone position ventilation or sputum aspiration and alveolar lavage under bronchoscope. Diffuse pleural thickening often indicates poor lung compliance, and more rigorous pulmonary protective ventilation should be implemented. Autopsy of deceased COVID-19 patients revealed that pleural thickening widely adheres to the lung tissue; there are fibrous cords in the lung, gelatinous mucus in the bronchi, and a small amount of yellow pleural effusion on both sides. 22 These findings are fully consistent with clinical observations by LUS, demonstrating the accuracy of this technology. Of relevance, these advantages are not available in the bedside chest X-ray.
The collected data suggest that LUS might be an essential diagnostic modality to optimize the postoperative imaging strategy in COVID-19 patients. LUS can facilitate prompt diagnosis of CARDS and help in understanding the changes taking place in the lung tissue. These factors can enable an early start of the therapy and ensure proper treatment. In addition, the ROC analysis suggested that the sensitivity, Youden index, and kappa value for detecting CARDS were higher for LUS than chest X-ray. Therefore, we suggest using LUS as an addition to the physical examination in COVID-19 patients with ARDS.
The current study has some important limitations. First, the number of admitted patients was very small, which could have influenced the results of the performed analysis. Second, the enrolled COVID-19 patients were already screened for ARDS, which may have affected the results of the ROC analyses for LUS and chest X-ray. Third, LUS was performed by different first-line clinical doctors with different levels of experience, which may have produced differences in the detection results since the detection standards are difficult to control. 23
In conclusion, LUS has a greater diagnostic accuracy and sensitivity in COVID-19 patients with ARDS than the portable chest X-ray. The obtained results suggest that LUS can be used as the primary imaging technique to detect COVID-19 patients and can improve bedside decision-making.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The raw data required to reproduce these findings cannot be shared at this time as the data also form part of an ongoing study.
Informed consent
The data and images were collected with the consent of the patients’ family members.
Ethical approval
This investigation was approved by the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (ClinicalTrials. 0027). The ethical proof of this study is attached to the letter. It is a form in Chinese.
Human rights
Human rights were guaranteed throughout the data collection process.