
Abstract
Objective
To compare the endotracheal intubation skill retention of the McGRATH™ MAC video laryngoscope with that of the Macintosh laryngoscope in first-year residents rotating at an anaesthesiology department.
Methods
This randomized controlled study enrolled first-year residents who completed a 2-month rotation at an anaesthesiology department. Each rotation group was randomly assigned to the Macintosh laryngoscope (ML) or McGRATH™ MAC video laryngoscope (MML) group. Endotracheal intubation skills were evaluated on a mannequin after the rotation and at 3 and 6 months later. The primary endpoint was the time required for intubation. The secondary endpoint was the percentage of glottic opening (POGO) score.
Results
Forty-six residents participated in this study and were assigned to the ML group (n = 23) or the MML group (n = 23). There were no significant differences between the sex, age and the number of endotracheal intubation procedures performed between the two groups. The time required for intubation was significantly shorter in the MML group compared with the ML group. The POGO scores did not show any significant differences between the two groups.
Conclusion
Compared with endotracheal intubation training using the Macintosh laryngoscope, the McGRATH™ MAC video laryngoscope shortened the intubation procedure and its effect remained even after 6 months.
Trial Registration
UMIN-CTR Clinical Trials, UMIN000036643, URL: https://www.umin.ac.jp
Introduction
The Macintosh laryngoscope, a device commonly used for endotracheal intubation education, allows only the operator to visualize the larynx inside directly. For this reason, it is difficult for the staff of the anaesthesiology department to provide detailed feedback to residents during training. In addition, despite successful intubation, the quality of the intubation process cannot be verified, which further makes it difficult to provide feedback for improvement.
On the other hand, video laryngoscopes allow residents and the anaesthesiology staff to verify real-time images on the video monitor. Several studies have reported that using a video laryngoscope reduced the endotracheal intubation time and improved the view of the larynx.1–4 However, few studies have investigated the level of endotracheal intubation skill retention when using a video laryngoscope.5,6
This current study hypothesized that if the anaesthesiology staff could provide sufficient and precise feedback of the larynx through the video monitor, the residents’ intubation skills would be retained for a more extended period. To test this hypothesis, this randomized control trial was conducted to compare the endotracheal intubation skill retention of the McGRATH™ MAC video laryngoscope with that of the Macintosh laryngoscope in first-year residents rotating at the Department of Anaesthesiology.
Materials and methods
Study design and population
This randomized controlled study included first-year residents who started a 2-month rotation at the Department of Anaesthesiology, The Jikei University School of Medicine, Kashiwa Hospital, Chiba, Japan between May 2019 and March 2020. The first-year residents had not received training in endotracheal intubation before the anaesthesiology rotation and performed endotracheal intubation on an actual patient for the first time during the anaesthesiology rotation.
This was a cluster randomized control trial because each group consisted of two to four residents who rotated every 2 months. Randomization was performed with a balanced randomization schedule and a predefined random number table. Each rotation resident was assigned to either the Macintosh (Heine Standard Fibre Optic LED laryngoscope handle and Heine Classic+ Macintosh Fibre Optic blade, Heine Optotechnik GmbH & Co. KG, Herrsching, Germany) laryngoscope (ML) group or the McGRATH™ MAC video laryngoscope (Covidien Inc. Medtronic, Tokyo, Japan) laryngoscope (MML) group based on the type of laryngoscope used to perform endotracheal intubation on clinical training during the 2-month anaesthesiology rotation. This study adhered to the applicable Consolidated Standards of Reporting Trial Statement (CONSORT) 7 and The Ottawa Statement on the Ethical Design and Conduct of Cluster Randomized Trials.
This study was approved by the Ethics Committee of The Jikei University School of Medicine, Tokyo, Japan (approval number, 26-044 (7549); registration date: 2014/06/02). The trial was registered before patient enrolment at the Clinical registry (trial number: URL: https://www.umin.ac.jp, UMIN000036643; registration date: 2019/05/03). The study received ethical approval for the use of an opt-out methodology for patients, however written informed consent was obtained from the first-year residents before enrolment in this study.
Study protocol
In the ML group, the conventional Macintosh laryngoscope was used for clinical training and the larynx could only be viewed by residents during the actual intubation. The residents explained their field of view and the anaesthesiology staff provided feedback based on their explanations. In the MML group, the residents were encouraged to look at the video monitor of the McGRATH™ MAC video laryngoscope while the anaesthesiology staff provided timely feedback through the video monitor.
Endotracheal intubation skill retention was investigated immediately after completing the rotation at the Department of Anaesthesiology and at 3 and 6 months later. To standardize the evaluations, first-year residents performed the intubations on a mannequin rather than a human. The evaluation used an endotracheal intubation device that was not used in both groups during the rotation period. The high-fidelity simulator SimMan® 3G (Laerdal Medical Japan Co., Ltd., Tokyo, Japan) and a C-MAC® video laryngoscope (KARL STORZ Endoscopy Japan K.K., Tokyo, Japan) were selected for the evaluation of endotracheal intubation skill retention. The SimMan® 3G simulator was used for the following reasons: (i) intubation conditions can be standardized while the laryngeal exposure varies during patient intubation, thus influencing the difficulty; (ii) an evaluation environment similar to the actual clinical setting can be created because it is a whole-body mannequin with an intricate laryngeal structure. The height of the SimMan® 3G head was set at 6 cm and the neck flexion was set at the same angle as the pillow. The SimMan® 3G airway setting was kept at the default status and did not require any adjustments. A 7.5-mm Mallinckrodt™ Hi-Lo tracheal tube (Mallinckrodt Inc., Covidien Japan Inc., Tokyo, Japan) was made to shape and standardized with an intubating stylet following a photograph of the actual size. The C-MAC® video laryngoscope was used as the intubation device because it has a Macintosh-type blade and allows faculty members to verify the field of view on the monitor through a camera attached at the tip of the blade. The monitor is separated from the blade and completely shielded from the view of first-year residents.
Outcome measures
The primary outcome was a retention of endotracheal intubation skills evaluated as endotracheal intubation time. The time required for intubation was measured from when the resident touched SimMan® 3G until the tip of the endotracheal tube passed through the glottis. The secondary outcome was the percentage of glottic opening (POGO) scale scores over the observation period. 8
Intubation was considered a failure if the tube was not passed through the glottis within 60 s. In cases of failure, data from the second successful intubation were analysed. In addition, the POGO scale was visually evaluated by faculty members based on the image displayed on the C-MAC® video laryngoscope monitor.
Statistical analyses
A sample size calculation was performed using G*Power version 3.1.9.3 for Macintosh (Heinrich-Heine-Universität, Düsseldorf, Germany). The parameters were based on our experience and data from past studies: α = 0.05, power of test = 0.8, effect size f = 0.25, which is estimated to be moderate, and the absence of correlation among repeated measures (Corr.≈0). Repeated-measures analysis of variance (ANOVA) was performed for statistical analysis of the primary endpoint.9,10 As a result, the calculated sample size was 44 subjects (22 in each group). The number of dropouts was estimated to be 1 in each group. Moreover, the researchers of this study confirmed the inclusion and exclusion criteria and assignment. Thus, the final sample size was 46 subjects (23 in each group).
All statistical analyses were performed using JMP® Pro version 13.1.0 for Macintosh (SAS Institute Inc., Cary, NC, USA). The background characteristics of both groups are expressed as medians and interquartile ranges for continuous variables and as numbers and percentages for frequencies. Data used in the primary and secondary analyses are expressed as mean ± SD and 95% confidence intervals. A repeated-measures ANOVA was conducted for both primary and secondary analyses. Continuous data were compared using Mann–Whitney–Wilcoxon test. Categorical data were compared using Fisher’s exact test. The data were blinded before analysis by a trial statistician. A P-value < 0.05 was considered statistically significant.
Results
Forty-six residents participated in this study. With cluster randomization, 23 residents were assigned to either the ML or the MML groups (Figure 1). There were no dropouts after the randomization. The sex, age and the number of endotracheal intubation procedures performed during rotation at the Department of Anaesthesiology did not differ between the two groups (Table 1).
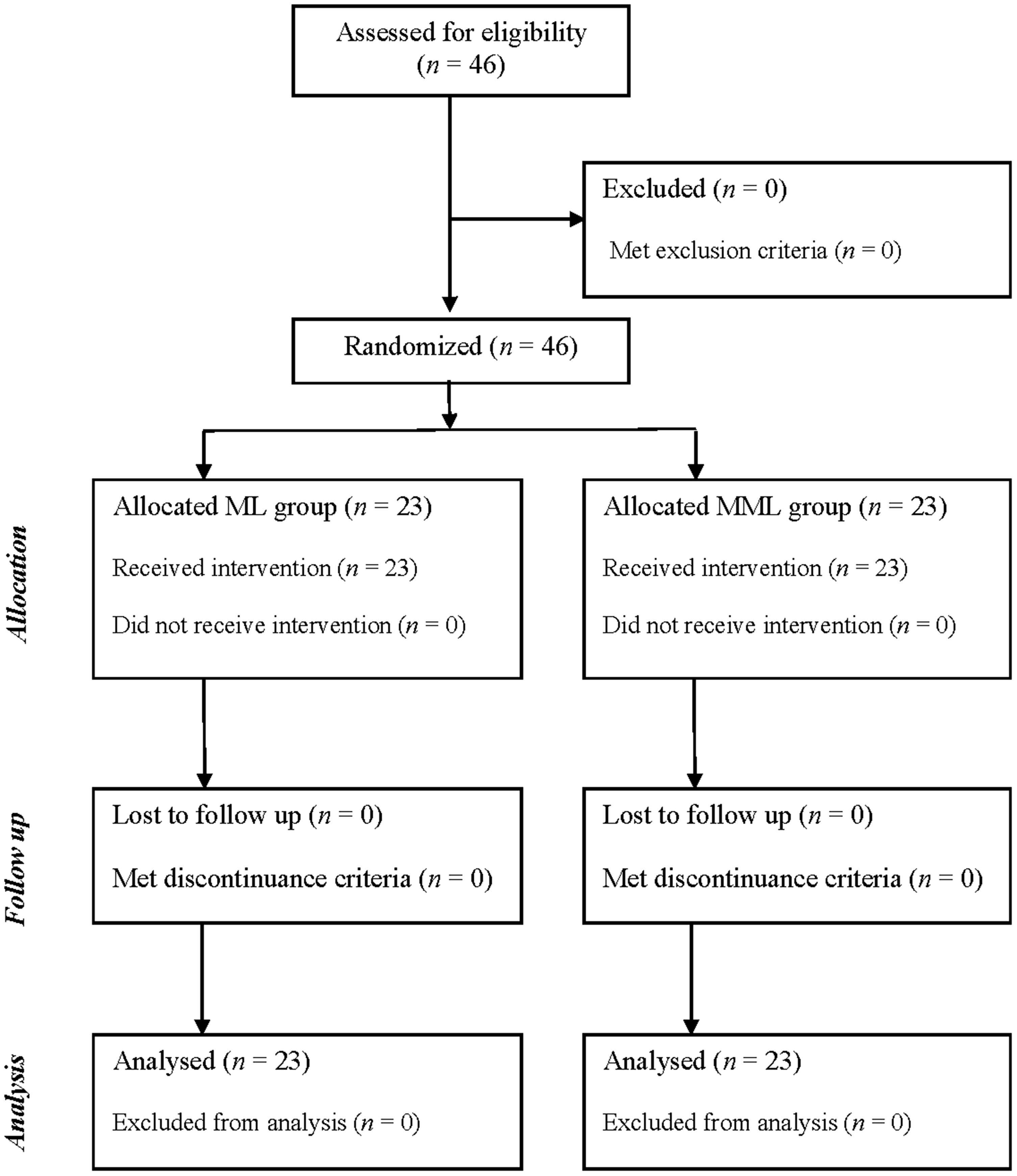
Flow chart showing progress through enrolment, randomization and analysis of first-year residents that participated in a randomized controlled trial conducted to compare the endotracheal intubation skill retention of the McGRATH™ MAC video laryngoscope with that of the Macintosh laryngoscope.
Demographic characteristics of first-year residents (n = 46) that participated in a randomized controlled trial conducted to compare the endotracheal intubation skill retention of the McGRATH™ MAC video laryngoscope (MML Groups) with that of the Macintosh laryngoscope (ML group).
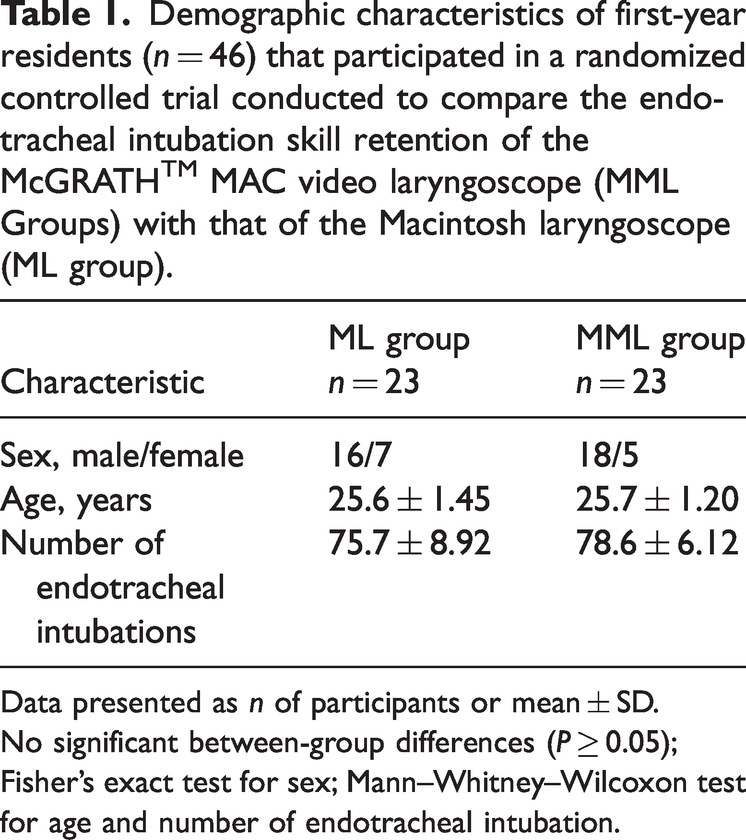
Data presented as n of participants or mean ± SD.
No significant between-group differences (P ≥ 0.05); Fisher’s exact test for sex; Mann–Whitney–Wilcoxon test for age and number of endotracheal intubation.
The time required for intubation was significantly shorter in the MML group than in the ML group at all time-points (immediately after completing the rotation in the Department of Anaesthesiology, 6.0 s, P = 0.0305; at 3 months, 10.2 s, P = 0.0014; at 6 months, 10.2 s, P = 0.0064) (Table 2). A repeated-measures ANOVA was performed to confirm whether the individual’s ability to perform the intubation was retained over time, demonstrating that the intubation time was significantly shorter in the MML group than in the ML group (P = 0.0017) (Figure 2). Intubation was re-attempted by three residents in the ML group and one resident in the MML group immediately after completing the rotation in anaesthesiology; and by two residents in the ML group at 3 months. There were no re-attempts at 6 months.
Intubation time for first-year residents that participated in a randomized controlled trial conducted to compare the endotracheal intubation skill retention of the McGRATH™ MAC video laryngoscope (MML group) with that of the Macintosh laryngoscope (ML group).

Data presented as mean (95% confidence interval).
Mann–Whitney–Wilcoxon test.

Intubation time for first-year residents that participated in a randomized controlled trial conducted to compare the endotracheal intubation skill retention of the McGRATH™ MAC video laryngoscope (MML group) with that of the Macintosh laryngoscope (ML group). Data presented as mean ± 95% confidence interval (CI). #P < 0.05 between the two groups by repeated-measures analysis of variance; *P < 0.05 at each time-point by Mann–Whitney–Wilcoxon test.
The POGO is a scale used for assessing airway visualization during tracheal intubation and represents the percentage glottis opening, ranging from 0% to 100%. A higher percentage indicates that the operator can observe more vocal cords. The mean POGO scores were not significantly different between the two groups at any time-point (Figure 3).

Percentage of glottic opening (POGO) score for first-year residents that participated in a randomized controlled trial conducted to compare the endotracheal intubation skill retention of the McGRATH™ MAC video laryngoscope (MML group) with that of the Macintosh laryngoscope (ML group). Data presented as mean ± 95% confidence interval (CI).
Discussion
This current randomized controlled study demonstrated that endotracheal intubation training using a McGRATH™ MAC video laryngoscope significantly shortened the endotracheal intubation time and facilitated long-term skill retention compared with the traditional Macintosh laryngoscope. A previous study reported that the endotracheal intubation skill of novice medical students deteriorated more when using an Airtraq® laryngoscope on a mannequin compared with the Macintosh laryngoscope. 6 Another study examined the endotracheal intubation skill retention of novice medical students using video laryngoscopes after simulation training on a mannequin. 5 The authors reported that there was no significant difference in the median intubation time at the end of the initial training between video laryngoscopy and Macintosh laryngoscopy; however, the median intubation time after 1 month was longer when using a video laryngoscope compared with Macintosh laryngoscope. 5 These studies examined endotracheal skill retention on a mannequin after simulation training.5,6 On the other hand, this current study examined the endotracheal skill retention of novice residents who completed a 2-month anaesthesiology department rotation. Then, endotracheal skill retention was assessed on a mannequin over 6 months.
Endotracheal intubation is an essential technique in life-threatening situations. Physicians are required to maintain this skill despite only performing it occasionally. Therefore, this current study protocol aimed for novice first-year residents to master this skill using deliberate practice. The process of deliberate practice requires focused repetitive practice and receiving informative feedback. 11 A prior study in novice medical students demonstrated that the minimal number of encounters required to achieve a 90% success rate under the supervision of attending anaesthesiologists was 17. 12 In this current study, the residents performed a mean of 75 endotracheal intubations during their anaesthesiology department rotation. The number of repetitive practices was sufficient for novice residents; 13 however, this number alone may not explain the better skill retention observed in the MML group. In addition, the process of providing feedback during endotracheal intubation contributed to better skill retention. The residents in the MML group received precise feedback from anaesthesiology faculty member who constantly monitored the view of the larynx. Receiving feedback with the aid of the viewing monitor enabled residents to identify areas that required further improvement and set goals for improvement. The goal-orientated and informative feedback using a video laryngoscopy resulted in superior skill retention in the MML group, even 6 months after completing the anaesthesiology rotation. These current findings demonstrate that the MML group acquired and retained better endotracheal intubation skills, as shown by the intubation time still being more than 10 seconds faster after 6 months; and this was despite the skills of beginners potentially declining rapidly to novice levels based on the deliberate practice concept.11,14 Acquiring and retaining good endotracheal intubation skills are clinically significant in the long run.
The laryngeal opening was also investigated using the POGO scale. 8 A previous study reported that laryngeal opening was better in group training with a video laryngoscope compared with a Macintosh laryngoscope. 15 However, there was no significant difference in the POGO scores between the two groups in this current study. The mean POGO scores in the MML group was approximately 70% over 6 months, which were comparable to the results of other research on mannequins. 16
This study had several limitations. First, the group assignments of the first-year residents were randomized but not blinded to the anaesthesiology faculty members. Secondly, a prior study investigated the emergency endotracheal intubation skill retention of residents, which indicated that residents needed to perform approximately three or supervise approximately five endotracheal intubations per year to maintain procedural proficiency and skill retention. 17 The residents in this study also had some opportunities to perform intubations 6 months after the anaesthesiology department rotation, which might have caused bias and affected their endotracheal skill retention.
In conclusion, intubation training with the McGRATH™ MAC video laryngoscope in first-year residents facilitated long-term skill retention compared with the traditional Macintosh laryngoscope.
Footnotes
Acknowledgements
We would like to thank all the residents that participated in this study.
Author contributions
Each of the authors significantly contributed to this manuscript. All authors are responsible for the content and have read and approved the manuscript for submission. Takanori Hiroe is a statistician and participated in the design phase of the study. Takako Terui, Shohei Kimura and Hideki Kuniyoshi supervised data collection. Yu Yamamoto wrote the first draft of the manuscript. Yoichi Kase guided the analysis and critically revised and reviewed the manuscript.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.