
Abstract
Introduction:
The aim of this study was to determine the risk assessment of acute coronary syndrome and prediction of major adverse cardiac events by HEART (History, ECG, Age, Risk factors, Troponin) and HEARTS3 (HEART + 3S = Sex, Serial 2-h ECG, and Serial 2-h delta Troponin) scoring systems in patients admitted to the emergency department with chest pain.
Methods:
This is a single-center prospective cohort study. This study was conducted in patients admitted to the emergency department with chest pain, without ST-elevation myocardial infarction, who were 18 years or older, and agreed to participate in the study. The primary endpoint is the occurrence of major adverse cardiovascular events within 30 days. The receiver operating characteristic curve was used to assess the power of HEART and HEARTS3 scores to predict major adverse cardiovascular events.
Results:
The mean age of 239 patients was 47.91 ± 13.93 years and 72.4% (173) were male. Major adverse cardiovascular events developed in 20.1% (48) of the patients. The mean HEART and HEARTS3 scores of the patients with major adverse cardiovascular events (5.67 ± 1.46 and 9.38 ± 3.91, respectively) were both statistically and significantly higher than the scores of the patients without major adverse cardiovascular events (2.33 ± 1.44 and 2.22 ± 1.39; p = 0.001). The area under the curve values of HEART and HEARTS3 scores were found to be 0.943 (95% confidence interval: 0.905–0.968) and 0.990 (0.968–0.999), respectively.
Conclusion:
In our study, the power of HEARTS3 score to predict major adverse cardiovascular events was better in the risk assessment of acute coronary syndrome in patients admitted to the emergency department with chest pain compared to the HEART score. We think that patients with a low HEARTS3 score can be safely discharged from emergency department without further cardiac examination.
Introduction
Chest pain is one of the most common reasons for admission to emergency department (ED). 1 It is crucial to differentiate acute coronary syndrome (ACS) from other non-fatal causes of chest pain.2,3
Patients presenting with ST elevation on the electrocardiogram (ECG) are rapidly receiving the necessary treatment. On the contrary, the diagnosis process of patients presenting with suspected ACS without ST elevation on the ECG is prolonged. 4 Physicians have a tendency to unnecessarily monitor these patients and initiate ACS treatment. This situation causes unnecessary patient load, extra diagnostic processes, and unnecessary treatments resulting in high costs. 5 The primary aim of the ED physician should be to identify patients with low-cardiac risk in a short time. 6
According to the literature, it is suggested to use scoring systems to determine the risk status of ACS, such as PURSUIT (Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor Suppression Using Integrilin Therapy), TIMI (Thrombolysis in Myocardial Ischemia), and GRACE (Global Registry of Acute Coronary Events). However, most of these scoring systems were designed for patients in intensive care units and none of these weren’t developed for patients with chest pain in ED. 1
In recent years, HEART (History, ECG, Age, Risk factors, Troponin) and HEARTS3 (HEART +3S = Sex, Serial 2-h ECG, and Serial 2-h delta Troponin) scoring systems were developed to determine the risks of patients with chest pain in ED and to discharge patients without further cardiac tests.7,8 Although there are several studies in the literature regarding HEART score, there aren’t any studies about HEARTS3 score except the original study to the best of our knowledge. On the contrary, these two scores weren’t compared with each other except the original HEARTS3 study.
The aim of this study is to determine the ability of HEART and HEARTS3 scores to predict ACS risk and major adverse cardiac events (MACE) in patients admitted to ED with chest pain.
Methods
Our study is a prospective observational cohort study and performed in Medipol Mega University Hospital Adult Emergency Department (annually 25,000 patients) from 9 October 2015 to 13 July 2016 (Istanbul Medipol University Non-Interventional Clinical Research Ethics Committee approval date/decision-no.: 15/09/2015–450). It is a tertiary university hospital with 380-bed capacity. Primary percutan coronary intervention (PCI) and all other kinds of cardiovascular invasive interventions can be performed in Medipol Mega Hospital for 24 h-a-day.
Patients were managed with “usual care.” Usual care is defined as “daily practice of the cardiologist or attending emergency doctor to diagnose a patient with chest pain.” In this period, attending doctors assess the risk based on their clinical skills, previous experiences, and current internatinal guidelines recommendations.
Inclusion criteria
Patients who were 18 years or older, admitted to ED with chest pain, and accepted the informed consent form were included in the study.
Exclusion criteria
Patients presenting with chest pain due to trauma, ST-elevation myocardial infarction (STEMI), tachyarrhythmia (supraventricular tachycardia (SVT), atrial fibrillation (AF), ventricular tachycardia (VT)), acute pulmonary thromboembolism, pericarditis, pneumonia, vascular pathologies such as thoracic aortic dissection, esophageal reflux, spasm, chest pain due to esophageal pathologies, sepsis, impaired renal function, acute cerebrovascular disease, pulmonary edema requiring mechanical ventilator were not included in the study. Moreover, patients who refused to participate in the study, who had chest pain without cardiac testing, who were transferred to ED as cardiac arrest, less than 18 years old, unable to speak, and unconscious were excluded.
Data collection
Patients were evaluated by emergency medicine specialist and research assistant in ED and standard form was prepared for each patient. After taking anamnesis and physical examination of each patient admitted to ED with chest pain, 12-lead ECG was taken and evaluated by emergency medicine specialist. Afterwards, blood analysis (complete blood count, creatine kinase MB (CK-MB), Troponin-I) was performed and chest radiograph was taken. Control ECGs were taken at the time of admission, at the 30th-min, first and second hours of the examination. The ECG samples were also re-evaluated by two cardiologists, one of whom was blindly consulted as cardiologist and the other one was part of study. Two Troponin-I levels were measured at the time of admission and 2 h after admission.
While patients diagnosed with non-ST-elevation myocardial infarction (NSTEMI) and unstable angina pectoris (USAP) in ED were admitted to coronary unit, patients without ACS were discharged to cardiology outpatient clinic for further examination and treatment.
Scoring system
The parameters measured in the HEART score are anamnesis (type of chest pain), age, ECG findings, number of coronary artery disease (CAD) risk factors and troponin level.1,9 In the HEART score, each item receives a score of 0–1–2, so total score should be between 0 and 10 points. Patients are divided into three groups as low risk (0–3 points), moderate risk (4–6 points), and high risk (7–10 points)1,9 (Table 1).
The HEART score for chest pain patients at the emergency department.
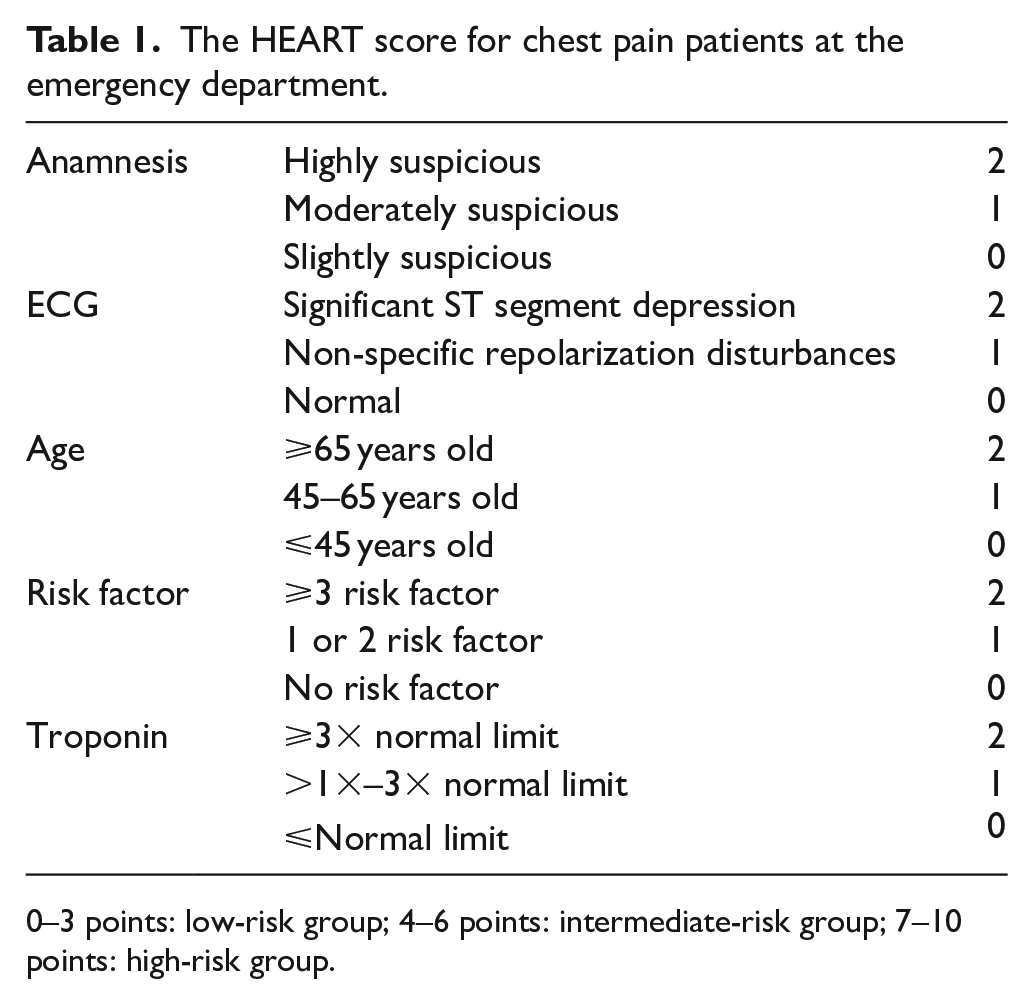
0–3 points: low-risk group; 4–6 points: intermediate-risk group; 7–10 points: high-risk group.
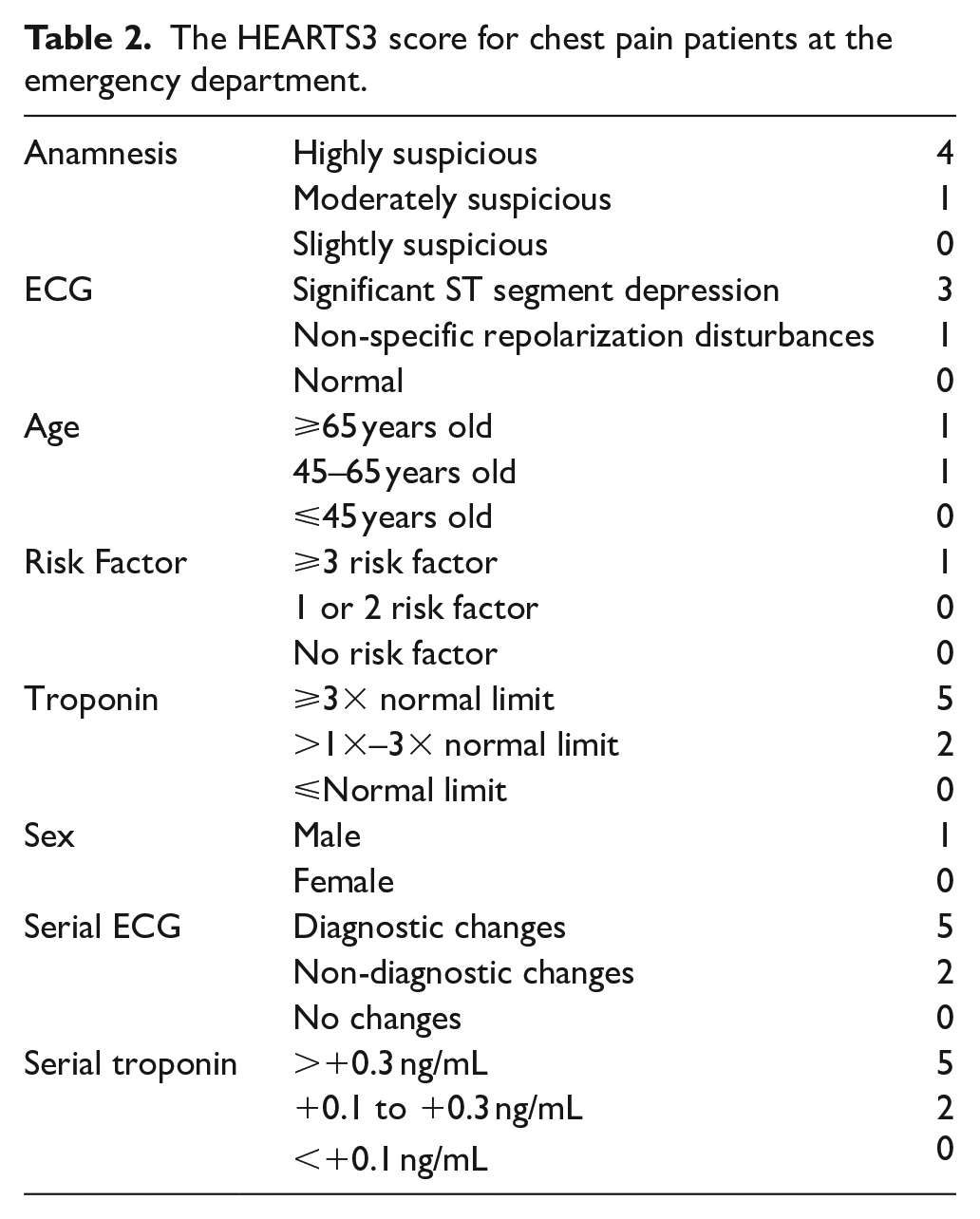
HEARTS3 score is obtained by adding sex, serial ECG, and serial troponin levels abbreviated as 3S to the parameters in HEART score (Table 2).
The HEARTS3 score for chest pain patients at the emergency department.
Anamnesis
Specific elements of chest pain such as onset, character, localization, accompanying symptoms, and response to sublingual nitrate were questioned and in their absence the pain was classified as “non-specific” and scored zero. If patient’s history isn’t specific but includes suspicious elements, it is classified as “moderate-suspect” and given 1 point. If story contains the elements mentioned, it is classified as “high-suspect” and given 2 points in HEART score and 4 points in HEARTS3 score.8,9
Coronary risk factors
The risk factors for ACS were determined by the emergency medicine specialist using patient’s own statements and old information in patient file. Being under treatment for diabetes-mellitus (DM), smoking, diagnosed and/or being under treatment for hypertension (HT), diagnosed with hyperlipidemia, family history of CAD and obesity (body mass index (BMI) calculated by measuring the height and weight >30 were defined as obese) are accepted as risk factors.8,9 According to the HEART score, patients who had no risk factors were given 0 point, who had one to two risk factors were given 1 point, and who had three or more risk factors were given 2 points. For HEARTS3 score; 0 point was given if patient had two or less risk factors, and 1 point was given for three or more risk factors.8,9
ECG
Minnesota ECG Criteria were used to evaluate the ECG. 10 When it was found to be “normal” according to Minnesota criteria, 0 point was given. In case of repolarization abnormalities without significant ST segment depression, 1 point was given. In addition, 1 point was again given for branch blocks, left ventricular hypertrophy, repolarization abnormalities due to possible digoxin use, or already known repolarization disorders. A total of 2 points in HEART and 3 points in HEARTS3 were given for significant ST segment depression or elevation, in the absence of a branch block, absence of left ventricular hypertrophy, or absence of digoxin use. For HEARTS3 score, the second ECG was taken at least 2 h later, evaluated in the same way, and according to same findings 0, 2, or 5 points were given, respectively.8,9
Troponin
Troponin-I levels were measured (Radiometer AQT90Flex, Denmark) at the time of admission and at the second hour. If troponin-I level was below the threshold value, 0 point was given. If troponin level was elevated up to 2 times of the threshold value, 1 point in HEART score and 2 points in HEARTS3 score were given. If troponin level was elevated 3 times or higher, 2 points in HEART and 5 points in HEARTS3 score were given.8,9
Outcome
The endpoint of our study was to detect development of MACE within 30 days in patients admitted to ED with chest pain. MACE is defined as acute myocard infarction (AMI), revascularization with PCI and coronary stenting, coronary artery bypass graft surgery (CABG), or cardiovascular mortality.1,8,9
The results of all patients were checked 30 days later from hospital information system, and examination reports and MACE results were recorded on the form. In addition, these patients were phoned on the 30th day after first admission and verbal information (such as effort test, echocardiography, coronary angiography, advanced cardiac examination results, etc.) was obtained for MACE.
Statistical analysis
IBM-SPSS Statistics22 (IBM-SPSS, Turkey) and Medcalc12.7.5 (MedCalc Software, Turkey) were used for statistical analysis. The suitability of the study parameters to the normal distribution was evaluated using ShapiroWilks test. In addition to descriptive statistical methods (mean, standard deviation, frequency), Student t test was used for comparison of normal distribution parameters between two groups and Mann–Whitney U test was used to compare non-normal distribution parameters. The chi-square test and Continuity (Yates) Correction were used to compare the qualitative data. In addition, receiver operating characteristic curve (ROC) was also used to compare diagnostic performance of HEART and HEARTS3 scores to differentiate patients with MACE. All p values less than 0.05 were considered to be statistically significant.
Results
During our study period, 18,162 patients applied to our ED. A total of 937 of them were eligible for the study. In line with the exclusion criteria, 698 patients were excluded from the study and 239 patients were included in the study (Figure 1).
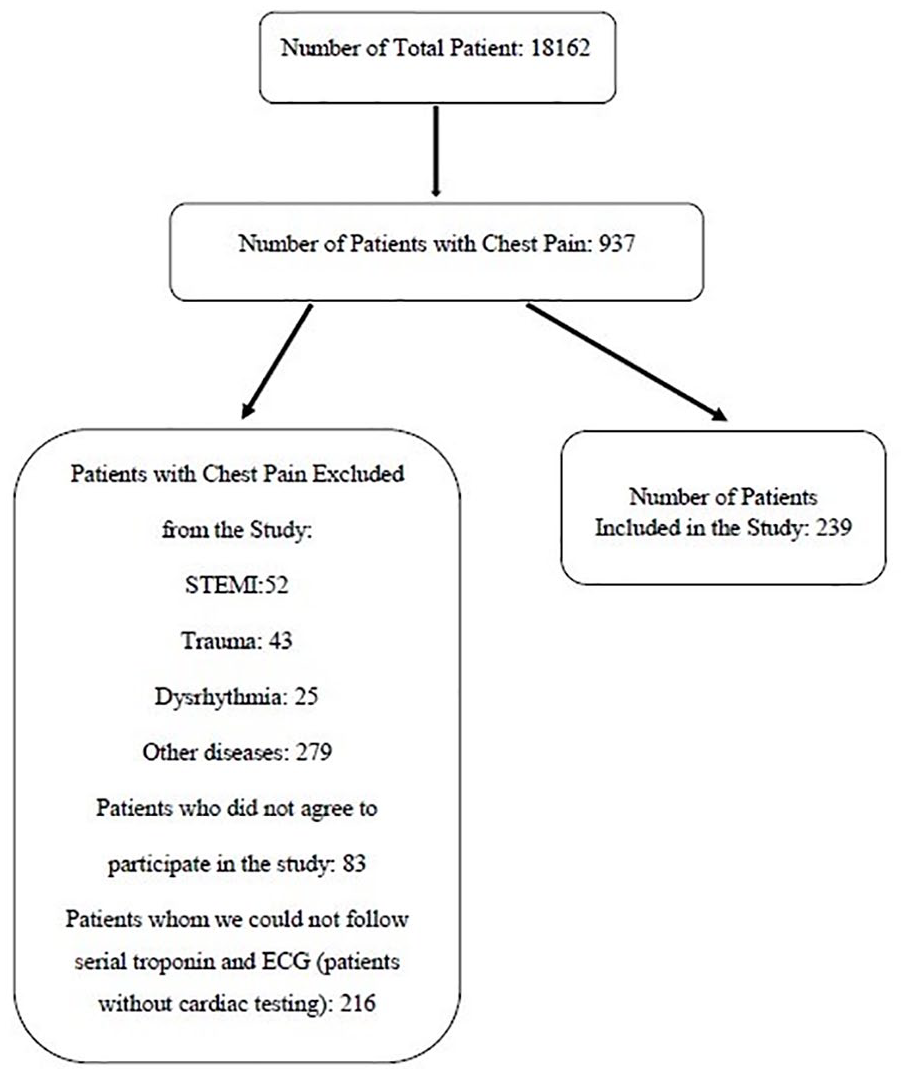
Flow diagram of patients in our study.
Total number of patients was 239 and 72.4% (n = 173) were male. The mean age was 47.91 ± 13.93 years (19–86 years). MACE developed in 20.1% (n = 48) of patients.
The general characteristics of patients according to MACE development are given in Table 3. The mean age of patients with MACE was significantly higher than those without MACE (p = 0.001). The incidence of MACE was 87.8% in patients with high suspected chest pain in their anamnesis (p = 0.001). Among the risk factors, hypertension, dyslipidemia, and family history of CAD were found to be 58.3%, 37.5%, and 28.9%, respectively, in MACE patients, and were both statistically and significantly higher.
Demographic features of patients according to major adverse cardiac events (MACE) outcome.
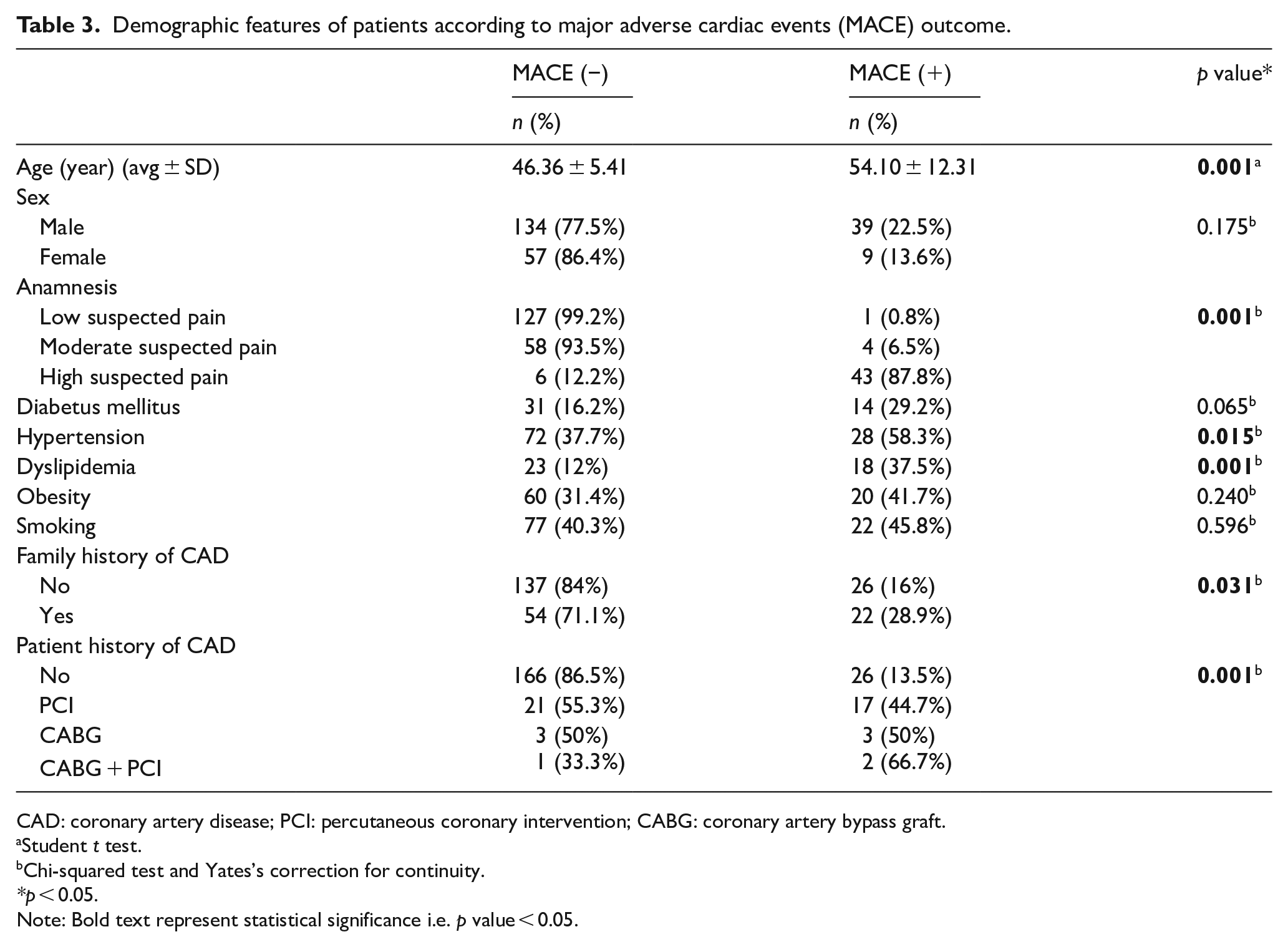
CAD: coronary artery disease; PCI: percutaneous coronary intervention; CABG: coronary artery bypass graft.
Student t test.
Chi-squared test and Yates’s correction for continuity.
*p < 0.05.
Note: Bold text represent statistical significance i.e. p value < 0.05.
The mean Troponin-I levels at the time of admission were 0.022 ± 0.076 (0.010–0.860) and the second Troponin-I levels were 0.039 ± 0.178 (0.010–2.300).
At the time of admission, 70.3% (n = 168) of patients had normal ECG, 23.4% (n = 56) had atypical ECG and 6.3% (n = 15) had ischemic ECG. While performing serial ECG analysis it was found that 95.8% (n = 229) of patients had no change, 2.5% (n = 6) had non-diagnostic changes, and 1.7% (n = 4) had ischemic changes.
MACE didn’t develop for any patient with HEART score of 0–2 and HEARTS3 score of 0–3. MACE developed in all patients with HEART score of 7 and above and in all patients with HEARTS3 score of 8 and above (Table 4).
Distribution of 239 patients’ HEART and HEARTS3 scores.
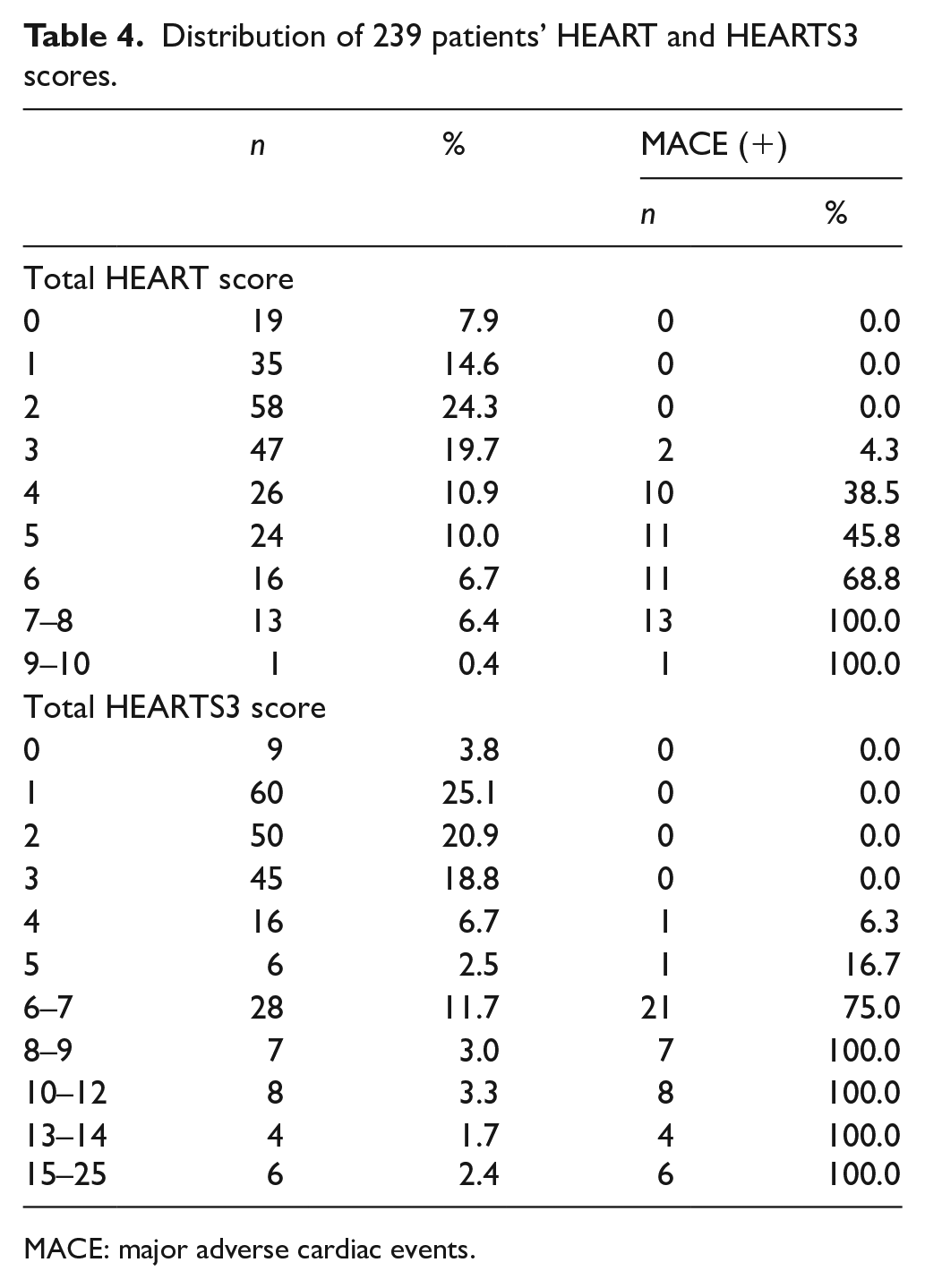
MACE: major adverse cardiac events.
HEART and HEARTS3 scores of patients who developed MACE (mean scores were 5.67 ± 1.46 and 9.38 ± 3.91, respectively) were significantly higher than HEART and HEARTS3 scores of patients without MACE (mean scores were 2.33 ± 1.44 and 2.22 ± 1.39, respectively; p = 0.001).
When the distribution of 48 patients with MACE was examined, 31 of them (64.6%) had PCI and 16 of them (33.3%) had AMI (Table 5).
Major adverse cardiac events (MACE) distributions of patients.
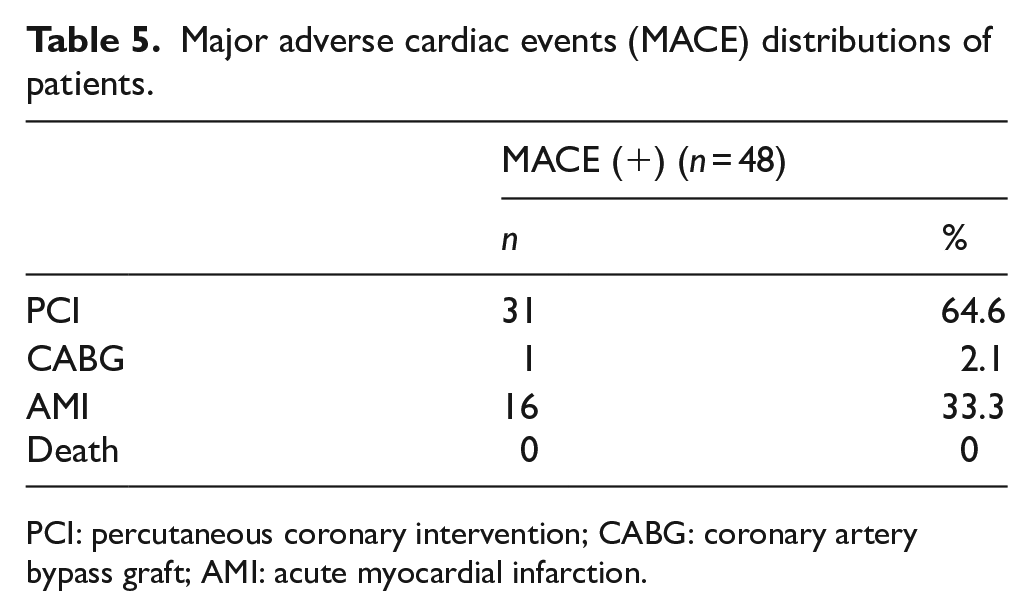
PCI: percutaneous coronary intervention; CABG: coronary artery bypass graft; AMI: acute myocardial infarction.
In the ROC analysis performed to determine MACE predictive power of the HEART and HEARTS3 scores, the predictive power of both scores was found to be high (area under curve (AUC) values for HEART score 0.943 (95%CI 0.905–0.968), for HEARTS3 score 0.990 (0.968–0.999)). However, the AUC value of HEARTS3 score was higher than the value obtained for HEART score (p = 0.001; Table 6 and Figure 2).
Comparison of the diagnostic performance of HEART and HEARTS3 scores to differentiate patients with major adverse cardiac events (MACE).
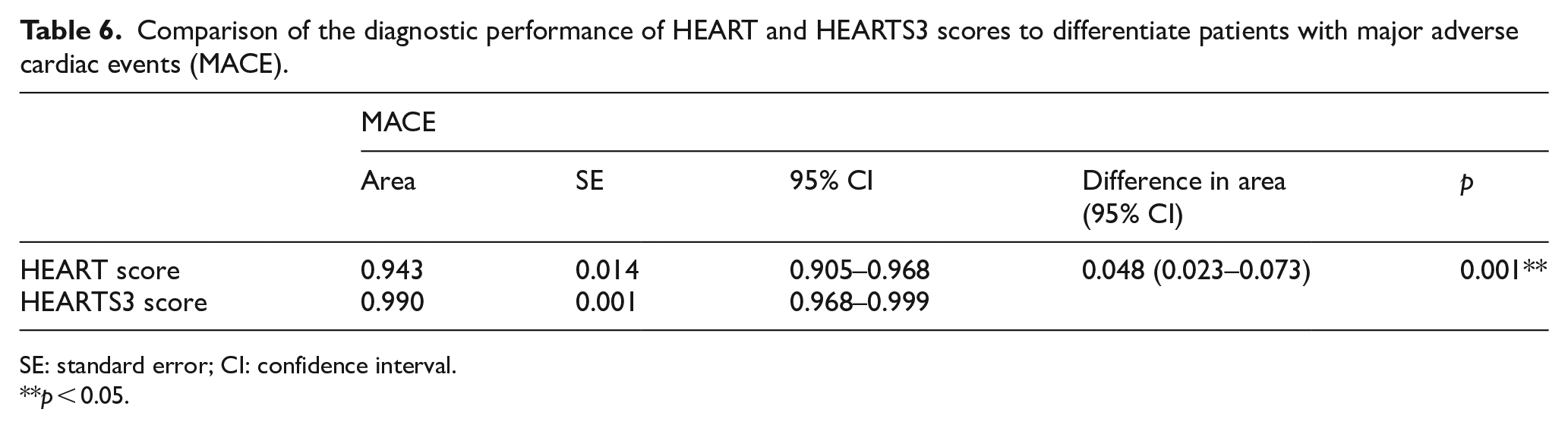
SE: standard error; CI: confidence interval.
p < 0.05.
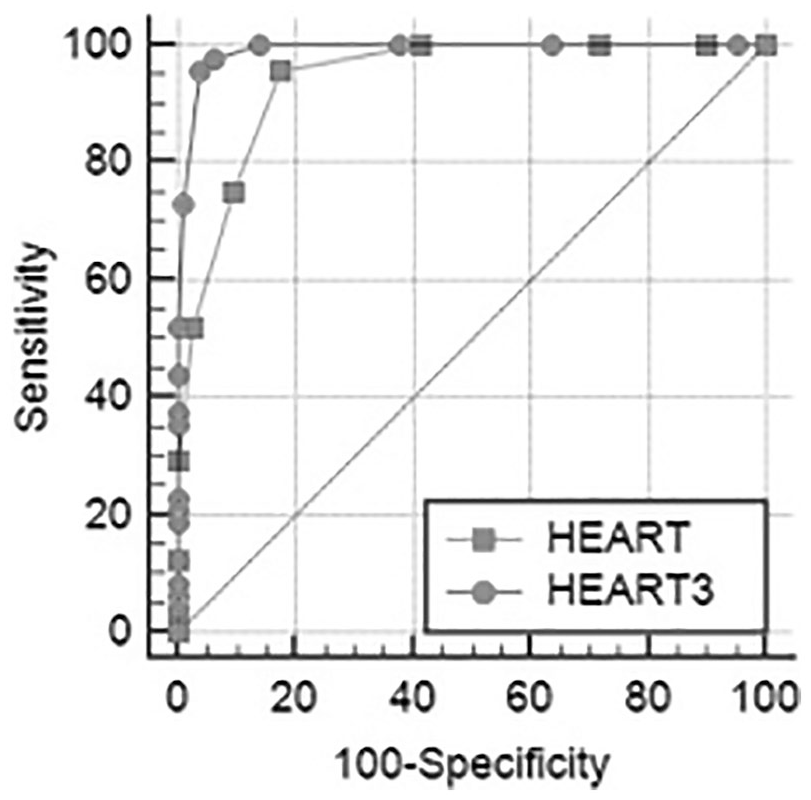
Receiver operating characteristic curves for MACE of the HEART and HEARTS3 scores.
Discussion
The main disadvantage of HEART score developed in 2008 is that individual variables are selected “based on clinical experience and current medical literature” and scores of every variable arbitrarily given without considering the possibility of MACE. For example, the presence of three risk factors or being above 65 years old have the same score with acute ischemic ECG or markedly elevated troponin level. However, these last two findings almost constitute the diagnosis of ACS in patients with chest pain. 8 Due to the lack of appropriate weighting, HEART score has low sensitivity especially in the evaluation of patients with moderate scores. Another limitation of HEART score is that it doesn’t take into account the gender of patient. 8 To improve HEART score by indicating these disadvantages, Fesmire et al. 8 changed the scoring using the probability ratio analysis of HEART elements in 2012 and they added abbreviated 3S as Sex, Serial ECG, and Serial Troponin levels. Probability ratio analysis was performed to create a weighted score for all variables and a new scoring system was developed. In this study, HEARTS3 score performed better than HEART score in risk classification of patients admitted to ED with chest pain. 8
The original study of HEART score by Six et al. 9 was a single-center study involving 120 patients with chest pain and mean HEART scores were 6.51 ± 1.84 and 3.71 ± 1.83 in those with and without MACE, respectively. In the study of 2388 patients by Backus et al., 5 HEART scores were 6.54 ± 1.7 and 3.96 ± 2.0 in those with and without MACE, respectively. In a retrospective study of 880 patients by Backus et al., 3 mean HEART scores were 7.2 ± 1.7 and 3.8 ± 1.9 in those with and without MACE, respectively. In our study, mean HEART scores in patients with and without MACE were 5.67 ± 1.46 and 2.33 ± 1.44, respectively. Similar to other studies in the literature, patients with MACE had a significantly higher HEART score in our study.
In a multicenter prospective study of 2388 patients by Backus et al., 5 MACE developed in 17% of patients (407 patients) and AMI developed in 6.4% of patients, 10.5% underwent PCI, 2.8% underwent CABG, 1.8% underwent conservative treatment, and 0.7% died. In a single-center study of 120 patients with chest pain by Six et al., 9 MACE developed in 24.1% of patients (29 patients), AMI developed in 13.3% of patients, 11.6% underwent PCI, 5% underwent CABG, and 1.6% died. In retrospective and single-center studies of Leite et al., 11 MACE was seen in 9.4% of 233 patients (22 patients) with chest pain. In our study with 239 patients, MACE developed in 20.1% of patients (48 patients), 6.7% were diagnosed with AMI, 12.9% underwent PCI, and 0.4% underwent CABG. None of the patients died within a month of cardiac events. Although MACE rates in different studies ranged from 9.4% to 24.1%, we can say that our rate is similar to the literature.
In the study of Six et al. 9 MACE developed in 2.5% (one patient) of 39 patients with HEART score of 0–3, 20.3% (12 patients) of 59 patients with HEART score of 4–6, and 72.7% (16 patients) of 22 patients with HEART score of 7–10. In the study of 233 patients by Leite et al. 11 MACE developed in 2% of 98 patients with HEART score 0–3, in 15.6% of 64 patients with HEART score 4–6, and in 76.9% of 12 patients with HEART score 7–10. In another study of 880 patients performed by Backus et al. 3 in 2010, MACE rates were 0.99% in patients with HEART score of 0–3, 16.6% in patients with HEART score of 4–6, and 65.2% in patients with HEART score of 7–10. In our study, MACE developed in 1.25% (two patients) of 159 patients with HEART scores between 0 and 3, 48.48% (32 patients) of 66 patients with HEART scores between 4 and 6, and 100% of 14 patients with HEART scores between 7 and 10. As HEART score increases, the risk of MACE increases. In our study, although MACE rates of low-risk group were similar to those in the literature, MACE development rate was found to be higher in medium-risk group. It was suggested that low-risk patients could be discharged early without additional advanced diagnostic methods (such as serial troponin, effort testing or imaging studies) in ED, while intensive care unit hospitalization, early invasive strategies and aggressive treatment were recommended for high-risk patients.3,9,12
In study of Fesmire et al., 8 MACE wasn’t observed in any of 304 patients (0.0%) with a HEARTS3 score of 0–1. In addition to this, MACE was observed in 4 (1.0%) of 400 patients with a HEARTS3 score of 2 points, in 24 (4.6%) of 520 patients with 3 points, in 36 (9.5%) of 380 patients with 4 points, in 31 (16.2%) of 191 patients with 5 points, in 42 (35.3%) of 119 patients with 6–7 points (35.3%), in 55 (59.8%) of 92 patients with 8–9 points, in 50 (78.1%) of 64 patients with 10–12 points, in 40 (88.9%) of 45 patients with 13–14 points, in 33 (100.0%) of 33 patients with 15–25 points. In our study, MACE wasn’t observed in any of patients with HEARTS3 score of 0–3 points. In addition to this, MACE was observed in 6.3% of 16 patients with HEARTS3 score of 4, in 16.7% of 6 patients with HEARTS3 score of 5, in 21 (75%) of 28 patients with HEARTS3 score of 6–7, in 25 (100%) patients with HEARTS3 score of 8 or higher. Similar to this study, it was observed that there was linear relationship between increasing HEARTS3 scores and MACE risk. In the same study, MACE rate was found to be 0.6% (4/704) in patients with HEARTS3 score of 0–2, whereas this rate was found to be 0% in patients with score of 0–3 in our study. It can be said that HEARTS3 score detects low-risk patients much better than HEART score. However, since there’s no other study related to HEARTS3 in literature, we couldn’t compare these data.
Fesmire et al. 8 compared the power of HEART and HEARTS3 scores to predict MACE. They detected a significant difference in favor of HEARTS3 both for MI and ACS development in 30 days (AUC values of HEARTS3 and HEART scores for MI were 0.958 and 0.825, respectively; and for risk of developing ACS within 30 days were 0.901 and 0.813, respectively). In our study, the power of HEART and HEARTS3 scores to predict MACE was determined as high (AUC values of 0.943 and 0.990, respectively). However, in our study, AUC value of HEARTS3 score was found statistically significantly higher. This makes HEARTS3 score more valuable for predicting MACE.
There are studies in the literature comparing HEART score with more commonly used scores. In their multi-center, prospective study Backus et al. 5 compared HEART, TIMI, and GRACE scores to predict MACE and found AUC values of 0.83, 0.75, and 0.70, respectively. Thus, they found prediction power of HEART score is statistically significantly higher. Poldervaart et al. 13 compared power of HEART, TIMI and GRACE scores to predict MACE in their multi-center, prospective study including 1748 patients. AUC values were determined as 0.86, 0.80, and 0.73, respectively, and they stated that HEART score was more successful. In the retrospective study including 2906 patients with chest pain, Six et al. 12 found the AUC values of HEART and TIMI scores for predicting MACE as 0.83 and 0.75, respectively. In our study, only HEART and HEARTS3 scores were compared and it was found that both scores had high power to predict MACE (AUC: 0.943–0.990, respectively).
Mahler et al. 14 evaluated power of HEART score to predict MACE using HEART score and serial troponin measurements together in patients with chest pain but low risk for ACS admitted to ED-based observation unit registry. In low-risk (HEART score < 3) patients; MACE rate was found to be 0.5% when only HEART score was used, but when a second troponin was added to HEART score, MACE rate was 0%. In our study we’ve also found the incidence of MACE 0% in patients with HEARTS3 score of 0–3. According to Mahler et al., 7 while the MACE incidence is more than 1% in patients discharged from ED according to HEART or other scoring systems (TIMI and GRACE), it is less then 1% in patients discharged according to HEARTS3 score. Accordingly, it increases reliability of HEARTS3 score.7,14
Patients with symptoms suggestive of ACS often undergo a lengthy assessment in the ED. Prolonged assessment contributes to duplication of work, high costs, and ED overcrowding, which leads to adverse patient outcomes, including increased mortality. HEARTS3 would liberate hospital resources, improve patient flows and reduce the economic burden on the health care system. It may also have a significant effect on ED overcrowding.
A potential implementation difficulty of HEARTS3 is that 2-h delta troponin testing is not a component of the chest pain evaluation protocol at many institutions. In HEARTS3 original study, the serial ECG component was performed using continuous serial ECG monitoring. 8 In our study, we applied serial static ECG. It is unknown how this affects the HEARTS3 score when one uses serial static ECGs in the ED. A final potential implementation difficulty is that the HEARTS3 score is not easily memorized due to the complexity of scoring as compared with the HEART score.
One of the limitations of our study is the low number of patients because it’s a single-center study in a private university hospital. Another limitation is the usage of old generation troponin measurement method. We think that using high-sensitivity troponin can provide more accurate score calculation and diagnosis. Another limitation of our study is that the risk factors of some patients included in the study were recorded according to their own statements. No particular tests have been done to any patient for hyperlipidemia, hypertension, or diabetes. Since further examinations and treatments of some patients after ED were performed in different hospitals according to patient’s preference, MACE results were obtained by calling them over the phone. This can be said as another limitation of our study.
In conclusion, HEART and HEARTS3 scores are easy, fast, and reliable methods in ACS risk assessment of ED patients with chest pain. However, it was found that HEARTS3 score had much better power to predict MACE. Especially, we think that patients having low HEARTS3 score should be discharged from ED without further cardiac examination.
Footnotes
Author contributions
All authors contributed to all stages of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from legally authorized representatives before the study.
Ethical approval
Ethical approval for the study was obtained from Istanbul Medipol University Non-Interventional Clinical Research Ethics Committee approval date/decision-no.: 15/09/2015-450.
Human rights
No human rights have been voilated during the preperation of this report.
Data accessibility statement
The datasets generated and analyzed during the current study are available from corresponding author.