
Abstract
Objective
We aimed to examine the role of the HEART (history, EKG, age, risk factors, and troponin) score in the evaluation of six clinical outcomes among three groups of patients in the emergency department (ED).
Methods
We performed a retrospective observational study among three ED patient groups including White, Black, and Hispanic patients. ED providers used the HEART score to assess the need for patient hospital admission and for emergent cardiac imaging tests (CITs). HEART scores were measured using classification accuracy rates. Performance accuracies were measured in terms of HEART score in relation to four clinical outcomes (positive findings of CITs, ED returns, hospital readmissions, and 30-day major adverse cardiac events [MACE]).
Results
A high classification accuracy rate (87%) was found for use of the HEART score to determine hospital admission. HEART scores showed moderate accuracy (area under the receiver operating characteristic curve 0.66–0.78) in predicting results of emergent CITs, 30-day hospital readmissions, and 30-day MACE outcomes.
Conclusions
Providers adhered to use of the HEART score to determine hospital admission. The HEART score may be associated with emergent CIT findings, 30-day hospital readmissions, and 30-day MACE outcomes, with no differences among White, Black, and Hispanic patient populations.
Keywords
Introduction
The HEART (history, EKG, age, risk factors, and troponin) score was initially developed to predict short-term major adverse cardiac events (MACE) and has been broadly used to risk-stratify patients with undifferentiated chest pain in the emergency department (ED).1–3 A HEART score of 0 to 3 is assigned to patients with a low risk of acute coronary symptoms. Use of the HEART score provides ED physicians with guidance on the safe disposition of patients in the ED with chest pain. 4 Low-risk patients can be directly discharged from the ED whereas non-low-risk patients are recommended to be admitted to the hospital for further evaluation and treatment.5,6 In recent years, with extended use, the HEART score has been reported as able to predict other clinical outcomes. When patients are admitted to the hospital, the HEART scores had been used to determine the need to perform emergent cardiac imaging tests (CITs). 7 Previous studies have found that patients with low HEART scores tend to have negative emergent CITs, thereby potentially avoiding CITs in these patients,7,8 which could result in shortened hospitalization. Low-risk patients also tend to have fewer ED returns and hospital readmissions; however, the findings are controversial in the literature.9–11 Overall, the HEART score seems to be associated with different clinical outcomes during different phases of chest pain management. However, these major clinical outcomes have mainly been studied independently among different patient populations in previous studies. Without simultaneous comparisons in the same patient population, usefulness of the HEART score for ED providers and the performance accuracy of using HEART criteria to predict clinical outcomes remain uncertain.
Apart from this, health care disparities persist in clinical presentation, evaluation, and outcomes among minorities who present to the ED with chest pain suggestive of acute coronary syndrome.12,13 The study ED has a mixed patient population including White, non-White non-Black Hispanic/Latino (hereinafter referred to as Hispanic/Latino), and African American. In the current literature, non-White patients were reported to have delays in seeking care 14 and Hispanic/Latino patients are less likely to be triaged emergently. 15 Under pressurized time constraints like emergent care settings, minority patients with chest pain might receive a less serious diagnosis. 16 When hospitalized, these patients often have more stress tests ordered, among which most test results are normal.13,17 After discharge, Hispanic/Latino and African American patients with chest pain have increased odds of multiple ED returns. 18 At present, we are uncertain as to discrepancies in using HEART score to predict different clinical outcomes among different ED patient populations. Using the HEART score could potentially minimize health care disparities among different patient populations in the ED with chest pain if it is proven that there are no differences by patient group.
It is challenging to resolve the above uncertainties simultaneously. Clinical practice patterns also differ among clinicians, making it harder to determine associations based on the results of previous studies. Therefore, it is critical to examine the clinical practice patterns of using the HEART score in different ED patient populations (such as to assess the need for hospital admissions and CITs) and furthermore, to determine the performance accuracy of using the HEART score to predict different clinical outcomes (such as CIT findings, ED returns, hospital readmissions, and MACE) in one study. With the use of electronic health records (EHR) within the same system, it is now feasible to follow the entire care process of each patient longitudinally, from ED disposition to hospital admission, to ED/hospital discharge, and finally to clinical follow-up or ED/hospital revisits. Therefore, we aimed to 1) determine the role of the HEART score in terms of six clinical outcomes including ED disposition, need to perform emergent CITs, emergent CIT results, short-term ED returns, hospital readmissions, and short-term (30-day) MACE outcomes; and 2) compare any associations among different ED patient populations.
Methods
Study design and setting
This was a retrospective single-center observational study. This study was approved by the local Institutional Review Board with a full waiver of the requirement for informed consent (#1541042 approved on 16 January 2020 by UNTHSC regional IRB). The study hospital is a publicly funded tertiary referral center, a level one trauma center, chest pain center, and a comprehensive stroke center. The study hospital ED has approximately 120,000 to 130,000 patient visits per year and chest pain is one of the most common problems in the study ED. Our entire health care system, including the ED, all outpatient clinics, and in-patient services, uses the same EHR system.
Study participants
All patients aged 18 or older who presented to the study ED with a chief complaint of chest pain or chest pain equivalent from 1 January 2017 to 31 December 2019 were enrolled. We screened all patients whose HEART score had been calculated prospectively (i.e., HEART scores calculated while patient was initially evaluated in the ED). Owing to potential changes in the patients’ condition during their hospital stay (in the ED or observation unit, or hospitalization), such changes could have resulted in multiple HEART scores being reported. In this study, as we focused on HEART score use among ED patients with chest pain, only HEART scores assessed by ED providers and documented in the ED notes were used in the data analysis. We excluded patients who 1) left the ED against medical advice (AMA), eloped, or left without being seen (LWBS); 2) were directly transferred to other facilities, immediately transferred to the heart catheterization lab, or who died in the ED; and 3) were clearly non-cardiac chest pain in the final diagnoses and did not have troponin testing during their ED visit. Additionally, we classified patients into four groups: White, Hispanic/Latino (non-White non-Black Hispanic/Latino), African American, and other. Other included Asian, Native American, Alaska Native, Hawaiian and other Pacific Islander, and unknown. Patients of other ethnicities were excluded as there was a very small number of patients (509 patients in total) classified as other race/ethnicity in this study ED. We retrieved patients’ EHR data from 1 January 2017 to 1 February 2020, including all follow-up information after patients’ index ED visit for the given study period.
Data retrieval and validation
The study health care system has been using an EHR system since 2012. Patient EHR data were retrieved by two assistants from the hospital’s Information Technology (IT) department who were trained in data management. To validate the accuracy of data retrieval, we randomly chose 20 patient charts and manually reviewed individual patient EHR data, to ensure that all reported variables were included. Subsequent validation was performed in triplicate for 60 patients, and all variables correctly matched the manual evaluation.
Study variables
The basic demographics of patients included age, sex, and ethnicity. Patient clinical variables included patient mode of arrival to the ED, level of acuity, insurance type, ED disposition, and total ED length of stay in minutes. We reported patients’ level of acuity using the emergency severity index (ESI) as documented by triage nurses. Patient mode of arrival included health care assisted (ambulance, ground/air, or hospital-based transportation), private (private car or other private vehicle), and other (including ambulatory, wheelchair, taxi, and public transportation). Patient insurance included hospital sponsored (e.g., study hospital-sponsored health insurance plan for low-income individuals), Medicare, Medicaid, patients with no insurance coverage (self-insured), and other (including different commercial insurance, Tarrant County Jail, TRICARE, Cook Children’s, other veterans insurance, and workers’ compensation insurance).
Outcome measures
Six clinical outcomes were measured in this study, including (1) ED disposition, (2) need to perform emergent CITs, (3) emergent CIT results, (4) short-term ED returns, (5) short-term hospital readmissions, and (6) short-term (30 day) MACE outcomes. Further definitions of the six outcome measures are given below.
ED disposition: Discharge dispositions to outside of the hospital (e.g., home, nursing facility) or to units within the hospital. Patient disposition was completely determined by individual physicians. Need for emergent CITs: This outcome is a binary variable (retrieved by an IT person using procedure codes) that is only applied to patients admitted to the hospital when emergent CITs are performed during the index hospitalization for individual patients. CIT results: The test result has two values, positive and negative, derived from the following CITs: a) cardiac stress test to determine the risk of acute coronary syndrome with acute cardiac ischemia (i.e., wall motion abnormalities, cardiac perfusion abnormalities, significant EKG ischemic patterns during the stress test, and others) where positive results are often indicated as a moderate to high risk; and/or b) reported heart catheterization interventions (such as stent placement, high pressure balloon angioplasty, balloon dilatation, thrombus extraction, regional medication perfusion, and others) or recommendation for coronary artery bypass graft surgery (CABG). Two individuals involved in conducting the study, who received adequate training on CIT result interpretation, independently reviewed CIT results documented in the EHR. If discrepancies occurred, a third person (the principal investigator) reviewed the CIT findings and made the final decision. Short-term ED returns: A binary variable that indicates whether the patient had any ED revisits within 30 days since the last ED or hospital discharge, regardless of their complaints on ED return. Short-term hospital readmissions: A binary variable that indicates whether patients had any hospital admissions within 30 days since their previous hospital admission. The 30 days were calculated from the date of previous hospital discharge to the date of hospital readmission, regardless of the diagnoses on hospital admission. Short-term MACE outcomes: A binary variable used to indicate whether any MACE occurred within 30 days of the index ED/hospital discharge. MACE refers to acute myocardial infarction (AMI), coronary revascularization by percutaneous coronary intervention (PCI) with or without additional interventions, CABG, and all-cause mortality. We used the International Classification of Disease Tenth Revision (ICD-10) code to determine AMI and procedure codes were used for PCI/CABG determination.
Approximately 32% of the patients in our data sample had no follow-up information and because their 30-day MACE outcomes were not observed, we manipulated the missing values in the following three ways:
The relevant data of patients without follow-up records were excluded from the analysis for predicting MACE outcomes. All missing MACE outcome values were indicated with a zero (0), (i.e., no major cardiac adverse events). This could be the best scenario because it indicates that no MACE occurred among patients that were not followed up. Missing MACE outcome values were imputed based on the distribution of the outcome among patients during follow-up, stratified by the three study populations and the two heart risk groups (i.e., low risk versus non-low risk). This imputation assumed that the likelihood of having MACE among non-follow-up patients was similar to that among follow-up patients in the same population and heart risk group (see Appendix for details).
Different methods for imputing the missing values allowed us to examine the robustness of the prediction models.
Cardiac imaging tests (CITs)
CITs consisted of stress tests and heart catheterizations in this study. All stress tests and heart catheterization results were reviewed by two independent reviewers after they had completed training on how to review the test reports.
Stress tests included exercise stress echocardiography, dobutamine stress echocardiography, pharmacologic nuclear Lexiscan (regadenoson) examination, and nuclear exercise stress testing with myocardial perfusion imaging. There are four possible stress test results: 1) low risk of acute cardiac ischemia, 2) moderate risk; 3) high risk; and 4) inconclusive (i.e., unable to complete the test or unable to reach the ideal heart rate). Positive stress test findings refer to test results of moderate and high risk (groups 2 and 3).
Heart catheterization tests have three possible results: 1) normal with no treatment or medical treatment with no intervention; 2) interventions including stent placement, high pressure balloon angioplasty, dilatation, or thrombus retrieval; and 3) no intervention but recommend consultation with cardiothoracic surgery for further procedures (such as CABG or valve replacement). Positive heart catheterization findings refer to performing interventions or a recommendation for CABG (groups 2 and 3).
Data analysis
The data analysis was focused on examining the role of the HEART score in specific clinical outcomes among three ED patient populations: White, Hispanic/Latino, and African American. Descriptive analysis was conducted including patient demographics and clinical information, as well as the six clinical outcomes mentioned above, among the three patient populations. The kappa statistic (
Reporting guidelines
The reporting of this study conforms to the STARD statement (STAndards for Reporting Diagnostic accuracy studies). 20
Results
Descriptive analysis
We prospectively calculated HEART scores among 9763 patients with chest pain in the study ED between 1 January 2017 to 31 December 2019; among them, 9419 patients completed their ED care. In further screening, we excluded patients who were transferred directly to an emergent catherization laboratory or other facility, patients who died in the study ED, and those who signed an AMA, eloped, or LWBS. Owing to the focus of this study, we further excluded 11 patients with unknown race/ethnicity and 509 patients with other race/ethnicity, as indicated in the methods section. A total of 8899 patients were enrolled in the final analysis (see Figure 1).
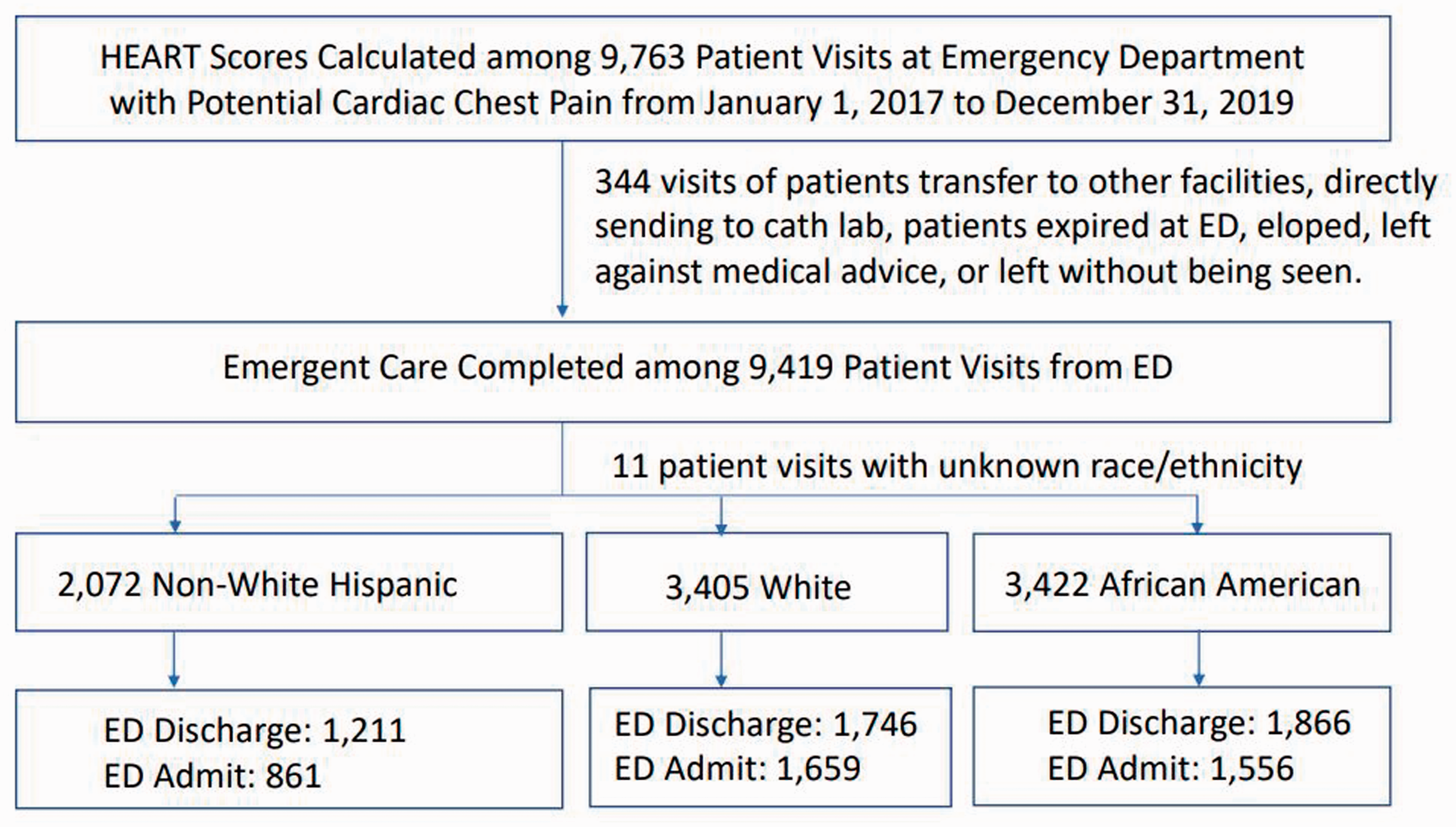
Study flow diagram
Table 1 shows the general characteristics of the study patients. In our cohort, Hispanic/Latino and African American patients were slightly younger and had more female patients compared with White patients (age:
Patients’ general characteristics

ED, emergency department; IQR, interquartile range; ESI, emergency severity index.
Classification accuracy analysis
The classification accuracy rate was measured on two clinical outcomes, hospital admissions and performing CITs if hospitalized. Among patients with non-low-risk HEART scores (4–10), we found no difference in the rate of admission to the hospital among Hispanic/Latinos in comparison with White and African American patients (Table 2). The classification accuracy rates were all 87% regardless of patient population, indicating high adherence of ED providers to using HEART score to assess patient hospital admission. Among all patients who were admitted to the hospital, those with non-low-risk HEART scores were more likely to have CITs performed during hospitalization (
Comparison of classification accuracy rate using HEART score (0–3) to determine hospital admission and cardiac imaging tests while hospitalized among emergency department patients
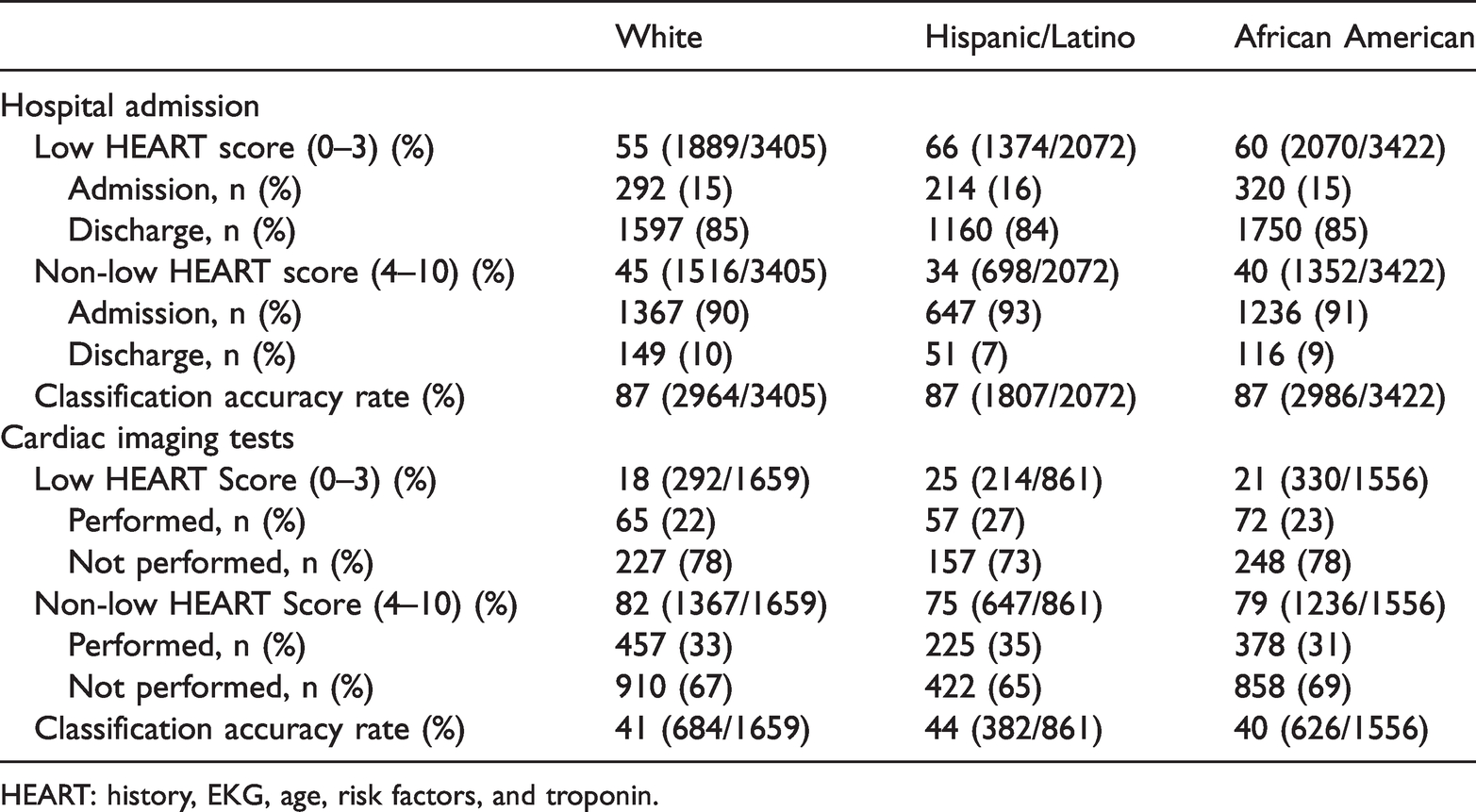
HEART: history, EKG, age, risk factors, and troponin.
Analysis of HEART score performance accuracy
Four other clinical outcomes were measured in this study. Two independent assistants reviewed the CIT results, and the kappa was high (
Comparison of performance accuracy of HEART criteria to predict clinical outcomes among patient populations
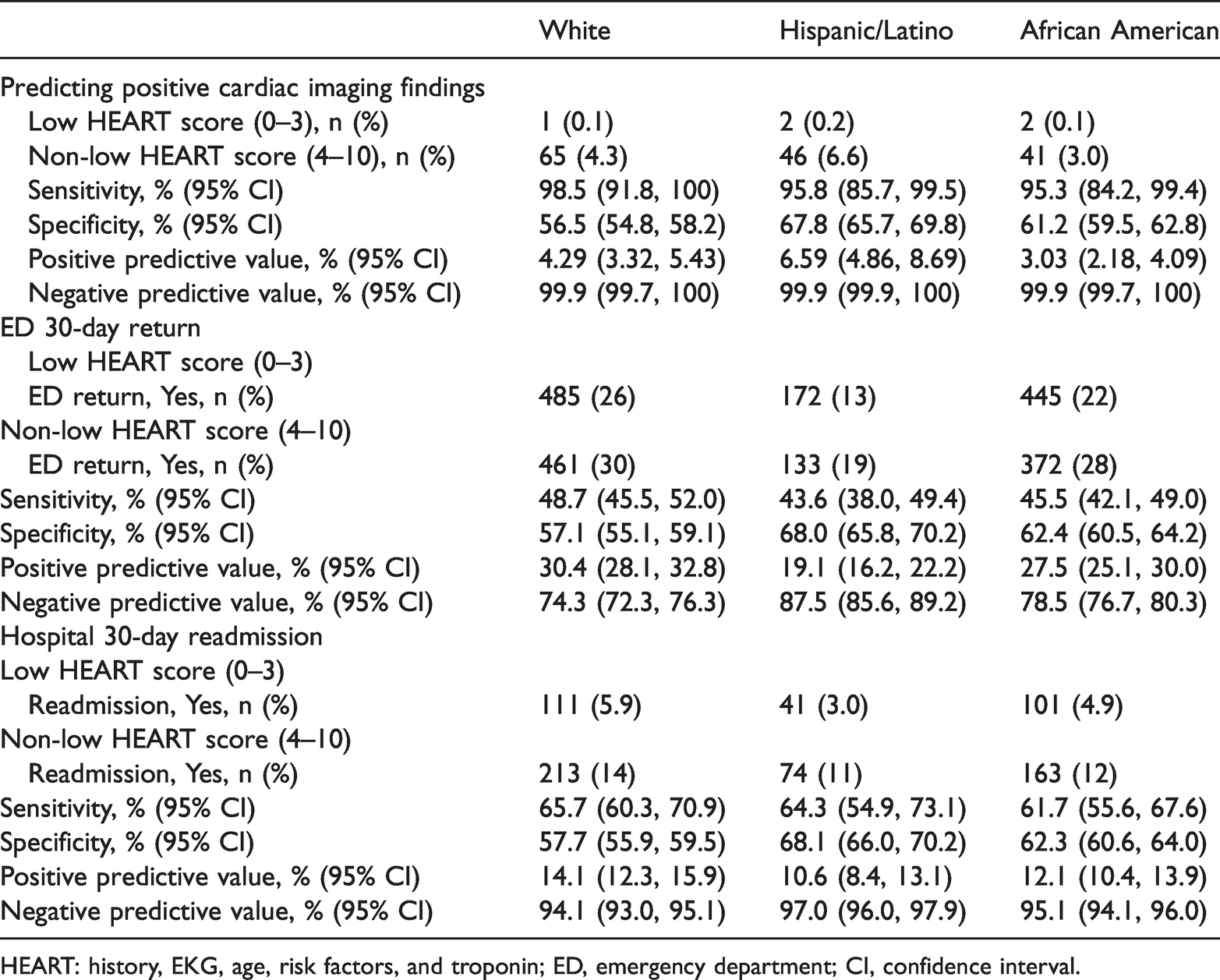
HEART: history, EKG, age, risk factors, and troponin; ED, emergency department; CI, confidence interval.
In comparison with White and African American patients, Hispanic/Latino patients with low-risk HEART scores (0–3) tended to have fewer 30-day ED returns (
Regarding short-term MACE outcomes, MACE occurrences ranged from 0.2% to 1.2% in patients of different ethnicities with chest pain. Consistently high NPV was found, regardless of patient population (Table 3). Additionally, MACE outcomes were estimated under other assumptions: 1) no MACE occurring among patients without follow-up; and 2) imputed MACE outcomes among patients without follow-up. Both assumptions showed no statistically significant differences among the three patient populations studied, with consistently high NPVs (Table 4). This indicates that patients with low-risk HEART scores had a lower risk of having short-term MACE outcomes.
Comparison of performance accuracy using HEART criteria to predict MACE outcomes under three scenarios in emergency department patients
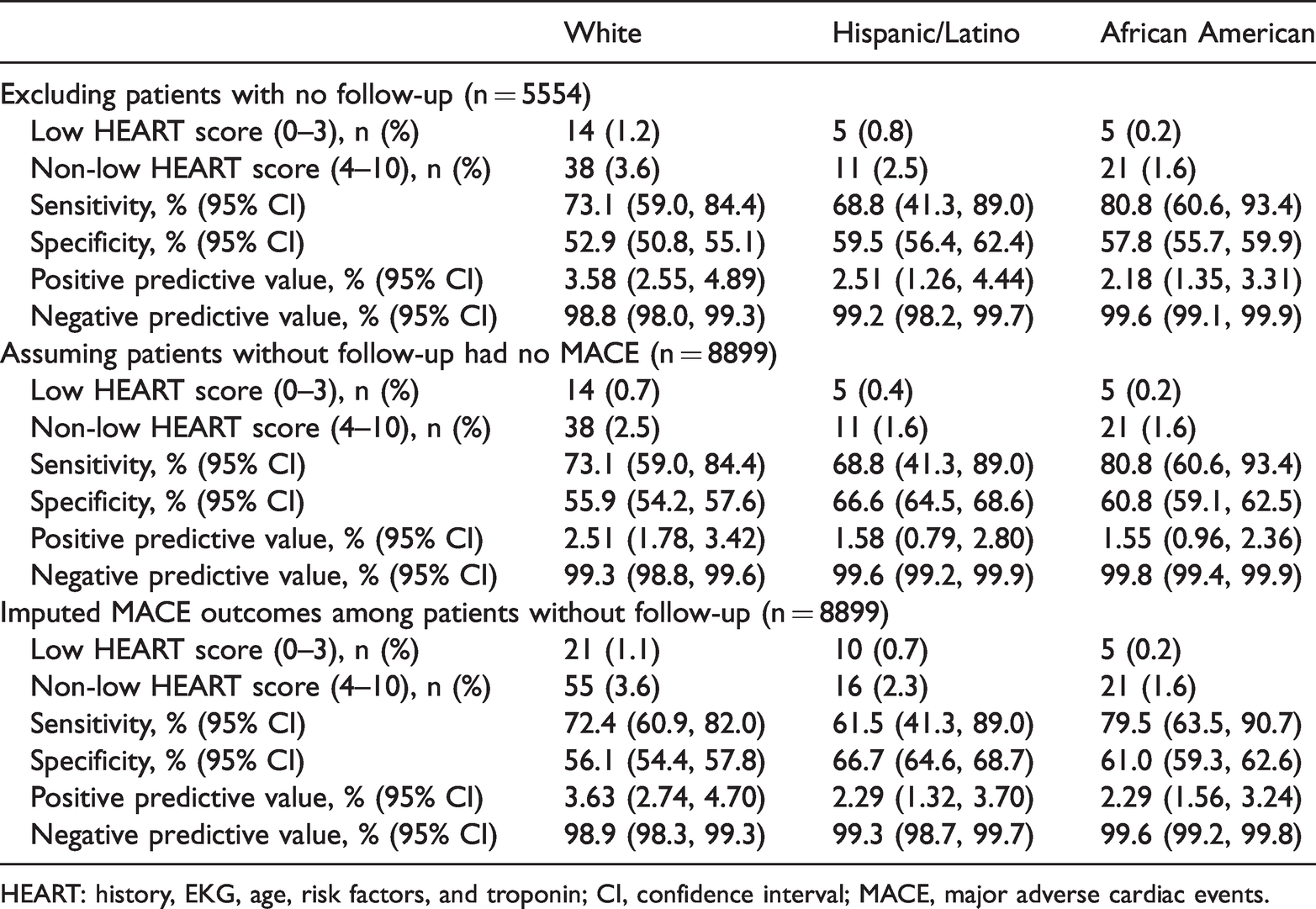
HEART: history, EKG, age, risk factors, and troponin; CI, confidence interval; MACE, major adverse cardiac events.
Table 5 shows the overall performance accuracy of using HEART score to predict the four clinical outcomes. We used the AUC to determine the performance accuracy of HEART scores in predicting each outcome, with comparisons among the three ED patient populations. The findings showed moderate accuracy in predicting positive CIT findings, 30-day hospital readmissions, and short-term MACE outcomes (AUC > 0.65), and that the HEART score was less valuable in predicting 30-day ED returns (AUC < 0.6). However, no differences occurred among the different ED patient populations with respect to using HEART score to predict all four clinical outcomes (
Comparison of performance accuracy using HEART score to predict clinical outcomes among emergency department patients

HEART: history, EKG, age, risk factors, and troponin; MACE, major adverse cardiac events, AUC, area under the receiver operating characteristic curve; CI, confidence interval.
Discussion
We studied the role of the HEART score in the association with clinical outcomes among three ED patient populations and found no statistical differences among White, Hispanic/Latino, and African American patients. We found high provider adherence in using the HEART score to admit patients to the hospital but less reliance on the HEART score when assessing the need to perform CITs while patients were hospitalized. Comparisons of HEART score performance accuracy showed moderate accuracy in predicting CIT results, short-term MACE outcomes, and hospital 30-day readmissions, and poor accuracy in the prediction of 30-day ED returns. We performed these analyses to validate the broader use of HEART scores.
The HEART score plays a very important role throughout the entire course of chest pain evaluation and management. Based on the present analyses, we found minimal health care disparities among ethnic minorities when using the HEART score in chest pain evaluation and management. Our study adds empirical evidence regarding the performance accuracy of HEART scores in relation to different clinical outcomes and comparing such outcomes among different patient populations, which has not been extensively studied.
Six clinical outcomes have been commonly used, measured, and reported in previous chest pain studies.4,6,11 Our study not only revealed findings similar to those reported previously but also showed the extended usefulness of the HEART score. However, previous studies have neither analyzed all clinical outcomes together nor separated ED patients into different populations. This may be partially owing to relatively unequal proportions of certain patient populations in past studies.4,21 Fortunately, our study ED has relatively equal proportions of different patient groups (e.g., White, Hispanic/Latino, and African American) and all our study patients were managed by the same group of ED providers, resulting in less bias. The present study results could further imply improved equity with use of the HEART score criteria in different ED patient populations.
Providers relied less on the HEART score when determining the need to perform CITs for patients admitted to the hospital. This could be partly owing to different chest pain management strategies among health care providers. When patients are admitted to the hospital, patient care is transferred to in-hospital service groups (either hospitalists or internal medicine physicians), among whom the HEART score might not be frequently used. Additionally, in-hospital services might prioritize the completion of chest pain management instead of assessing the need for emergent CITs in admitted patients. Some patients may have poor compliance with regard to outpatient clinic follow-up, thereby rendering clinicians unable to perform outpatient CIT evaluations. 22 Similarly, the HEART score may have less power to predict 30-day ED returns among our study cohort because many risks could affect patient short-term ED returns such as no insurance coverage, poor education, less income, and homelessness.23–26 The present study cohort might have high psychosocial risk, which could potentially prevent accurate prediction of ED returns. Our findings emphasize that the HEART score may be suitable for only certain clinical outcomes.
As for health care disparities among ethnic groups, our findings are consistent with previous reports.13,15 Hispanic/Latino patients with chest pain who attended the ED tended to be younger, most were female patients, and these patients were triaged less urgently than other ethnic groups, resulting in fewer hospital admissions. This might be owing to more atypical clinical presentations among certain patient populations, which could affect triage classification and subsequent hospital admission.12,27,28 Previous reports show that during hospitalization, more Hispanic/Latino patients with chest pain undergo cardiac stress tests, with fewer abnormal findings.13,29 These factors could also partially explain the relatively lower sensitivity and specificity of prediction using HEART score criteria among Hispanic/Latino patients. Although health care disparities exist among different ED populations, these do not affect the overall performance accuracy of the HEART score with respect to different clinical outcomes. Our findings indicate that the HEART score is suitable for use among general ED patient populations.
Limitations
Our study has several limitations. First, this was a single center retrospective analysis. Although all the data were retrieved from the EHR system and were entered prospectively, incomplete, inaccurate, or lost data could not be completely avoided. Second, we only enrolled patients whose HEART scores were calculated prospectively, which could further lead to patient selection bias. Third, in our study population, over 30% of patients had no follow up information; therefore, we imputed MACE outcome data and analyzed the study data under three conditions (see Table 4, and Appendix). Fourth, HEART scores were calculated by individual ED providers; variability could be present among ED providers, especially regarding some subjective elements like patient history and EKG interpretation. The acuity of patients with chest pain might vary among groups (e.g., more White patients than Hispanic/Latino patients had ESI-2) and could be affected by the mode of arrival to the ED (e.g., more White than Hispanic/Latino patients arrived via health care assisted transportation). Patients not arriving via health care assisted transportation may have had lower (or higher) acuity and may have waited longer before being evaluated from ED providers. Because we only measured the ED HEART score without investigating dynamic HEART score changes during patients’ ED stay, inaccuracies may have occurred among patients with a prolonged waiting time. Therefore, a multi-center prospective study is warranted to further validate the findings of this study.
Conclusion
In patients with chest pain who were evaluated in the ED, providers adhered to the HEART score to determine hospital admissions but had less reliance on the HEART score to determine the need to perform CITs. The HEART score may be associated with certain clinical outcomes, including positive emergent CIT findings, 30-day hospital readmission, and 30-day MACE outcomes, with no differences among White, Hispanic/Latino, and African American patient populations.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211010638 - Supplemental material for Role of HEART score in evaluating clinical outcomes among emergency department patients with different ethnicities
Supplemental material, sj-pdf-1-imr-10.1177_03000605211010638 for Role of HEART score in evaluating clinical outcomes among emergency department patients with different ethnicities by Stefan H. Meyering, Chet D. Schrader, Darren Kumar, Yuan Zhou, Naomi Alanis, Sajid Shaikh, Radhika Cheeti, Rebecca Smiley, Chukwuagozie Iloma Hao Wang in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors’ contributions
Stefan H. Meyering: Conceptualization, investigation, writing-review & editing, supervision, project administration
Chet D. Schrader: Conceptualization, methodology, investigation, writing-review & editing, supervision
Darren Kumar: Investigation, resources, writing-review & editing, supervision
Yuan Zhou: Validation, formal analysis, data curation, writing-review & editing
Naomi Alanis: Investigation, resources, data curation, writing-review & editing, supervision, project administration
Sajid Shaikh: Validation, resources, data curation, writing-review & editing
Radhika Cheeti: Validation, resources, data curation, writing-review & editing
Rebecca Smiley: Validation, resources, data curation, writing-review & editing
Chukwuagozie Iloma: Validation, resources, data curation, writing-review & editing
Hao Wang: Conceptualization, methodology, validation, formal analysis, investigation, data curation, writing-original draft, writing-review & editing, supervision, project administration
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.