
Abstract
Introduction:
Pulmonary and cardiac disorders are diagnosed in most patients presenting to the emergency department with dyspnea. Discrimination of pulmonary and cardiac pathologies from each other and early intervention have vital importance. Various methods have been used for assessment of peripheral perfusion, and the peripheral perfusion index) has gained popularity in recent years. This study aimed to investigate the contribution of peripheral perfusion index to the evaluation process in patients presenting with the complaint of dyspnea and diagnosed with either a pulmonary or cardiac pathology.
Materials and Methods:
We retrospectively reviewed the charts of patients who presented to emergency department with dyspnea between 1 July 2018 and 1 July 2019. Patients in whom the cause of dsypnea was determined to be a cardiac or pulmonary pathology were included in the study. The age, gender, peripheral perfusion index value at admission, the diagnosis, and the hospitalization status were recorded.
Results:
One hundred and ninety patients consisting of 106 (55.8%) males and 84 (44.2%) females were included in our study. While a pulmonary pathology was determined in 141 (74.2%) patients and a cardiac pathology in 49 (25.8%) patients, 72 (37.9%) patients were decided to be hospitalized. No difference was determined between patients with pulmonary and cardiac pathologies regarding peripheral perfusion index. When the patients were compared regarding hospitalization status and discharge from the emergency department, no significant difference was found to be present between the groups.
Conclusion:
Since peripheral perfusion index is a noninvasive, easy-to-perform, rapid, and reproducible test, it has been promising as a prognostic and diagnostic parameter. However, it has been realized that PPI was unsuccessful in the evaluation of patients with dyspnea, in the differential diagnosis of cardiac and pulmonary pathologies and prediction of hospitalization status in the emergency department.
Introduction
Dyspnea is one of the most common causes of admission to emergency department (ED), and its differential diagnosis involves severe disorders that may have a fatal course. However, pulmonary and cardiac pathologies are determined in most patients presenting to ED with dyspnea. 1 Even though various clinical approaches for differential diagnosis and determining the severity of dyspnea have been studied in the literature, emergency physicians still encounter clinical difficulties in the management of patients with dyspnea.1–3 The discrimination of particularly the underlying pulmonary and cardiac pathologies and to intervene during the early period carries vital importance.
In many severe clinical pathologies, such as shock, the reflex response of the body is the reduction of the peripheral perfusion for the preservation of the perfusion of vital organs. The clinically impaired peripheral perfusion has been well-known to reveal the severity of the underlying disorder. 4 Even though various methods have been used for assessment of peripheral perfusion up to now, the peripheral perfusion index (PPI), which can be measured using the pulse oximetry waveform amplitude, has gained popularity in recent years since it is a noninvasive, easy to perform, rapid and reproducible test. Various devices such as Masimo Radical SET (Masimo Corporation, Irvine, CA) calculate PPI value by proportioning the pulsatile and non-pulsatile signal alterations in the vascular bed to each other through a pulse oximetry probe placed at the fingertip. 5 In conditions with a broad spectrum of differential diagnoses, such as dyspnea, we had the opinion that PPI might have serious contributions for patient evaluation in the ED.
This study aimed to determine the contribution of PPI measurement to the clinical evaluation process in patients presenting to ED with the complaint of dyspnea and diagnosed with either a pulmonary or cardiac pathology.
Material and method
This study was performed following the Declaration of Helsinki, and ethical approval was obtained from the local ethics committee (29 Nov 2019/313). Written informed consent was not necessary because no patient data has been included in the manuscript. A trained triage nurse performed PPI measurements at the time of admission in all patients admitted to the ED of Suleyman Demirel University Research and Training Hospital between 1 July 2018 and 1 July 2019. PPI was measured by Masimo Radical SET (Masimo Corporation, Irvine, CA). The upper and lower limits of PPI reported by the manufacturer were 0.02% and 20.2%, respectively. The oximeter probe used for measuring PPI was placed at the index fingertip of the right hand, and the value was recorded after a value fixed on the monitor or after waiting for 30 s. Triage nurses working in the ED are regularly trained on PPI measurement and using the device.
The investigators reviewed the charts of patients who presented to the ED with dyspnea between the specified dates. Patients in whom the cause of dyspnea was determined to be a cardiac or pulmonary pathology were included in the study. The cardiac and pulmonary pathologies determined in the study were shown in Figure 1. Trauma patients, pregnant patients, patients in whom the cause of dyspnea was determined to be disorders other than the cardiac and pulmonary systems, patients aged under 18 years, patients with peripheral arterial diseases, patients whose chart data were unavailable, and patients who had both cardiac and pulmonary pathologies at the time of admission were excluded from the study. The age, the gender, the PPI value at admission, the ED diagnosis, and the hospitalization status of the patients included in the study were recorded.
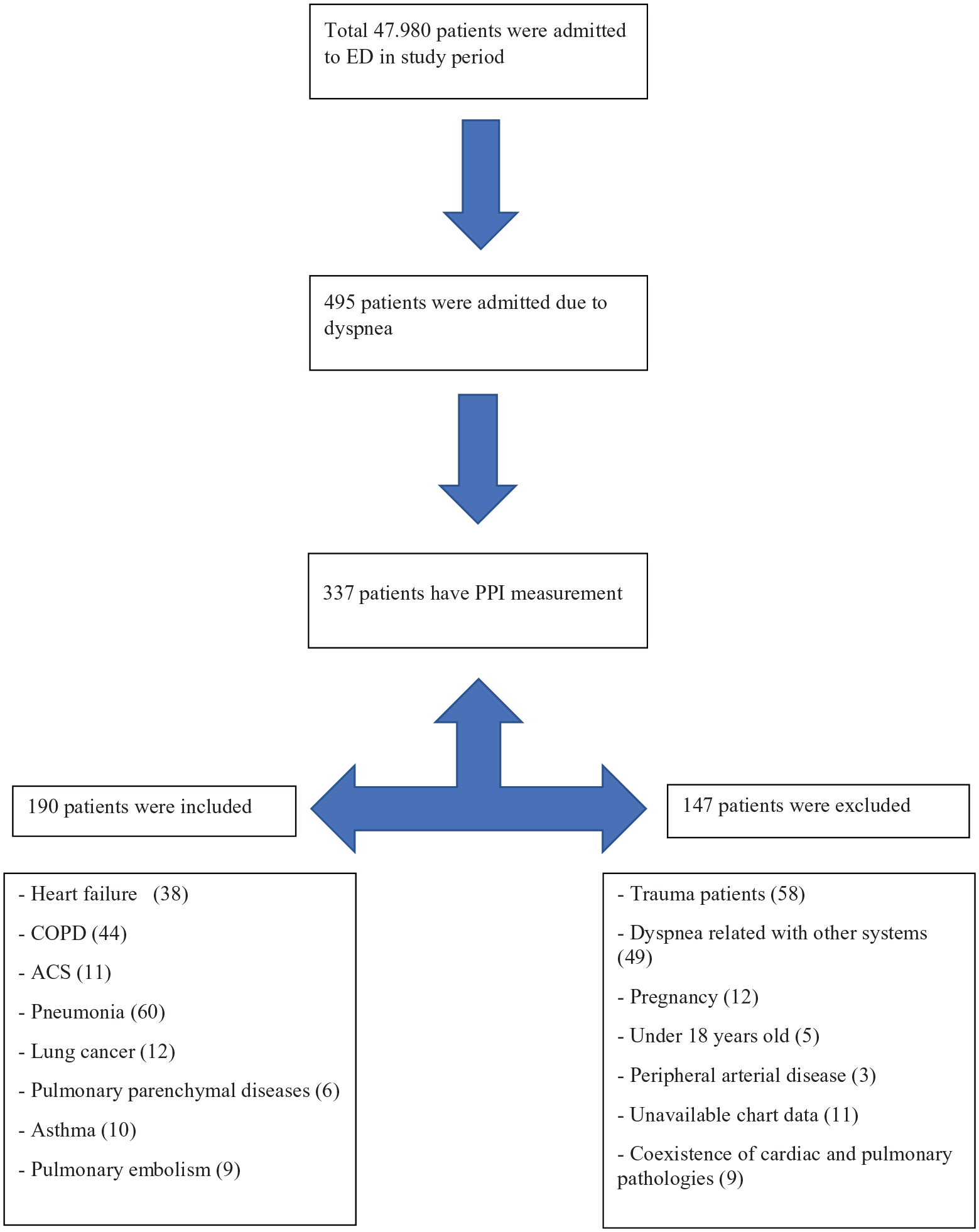
Flow chart of the study.
SPSS software v.25 was used for statistical analysis. The Kolmogorov-Smirnov test evaluated the conformity of quantitative data with a normal distribution. The T-test was used for statistical comparisons of data showing a normal distribution, and the Mann Whitney U test was used for data without normal distribution. Descriptive statistics were presented as “mean (standard deviation).” Pearson’s Chi-Square analysis was used in statistical comparisons of categorical variables, and descriptive statistics were presented as “number (%).” p < 0.05 was considered statistically significant.
Results
It was determined that there were 47,890 patient admissions to the ED between the specified dates, and PPI measurement was performed in 337 out of 485 patients having a complaint Of dyspnea. One hundred and ninety patients consisting of 106 (55.8%) males and 84 (44.2%) females were included in our study (Figure 1). The mean PPI and age were calculated as 3.6 ± 2.6 and 65.0 ± 17.3 years, respectively, in the entire patient group, 3.4 ± 2.5 and 67.4 ± 13.3 years, respectively, in male patients, and 3.8 ± 2.6 and 61.9 ± 13.3 years, respectively, in female patients. While no significant difference was found to be present between the male and female patients regarding the mean PPI value (p = 0.306), it was determined that male patients were older than female patients, the difference between the two groups was statistically significant (p = 0.029)(Table 1).
Comparison of patients according to gender, pathology, and outcome.
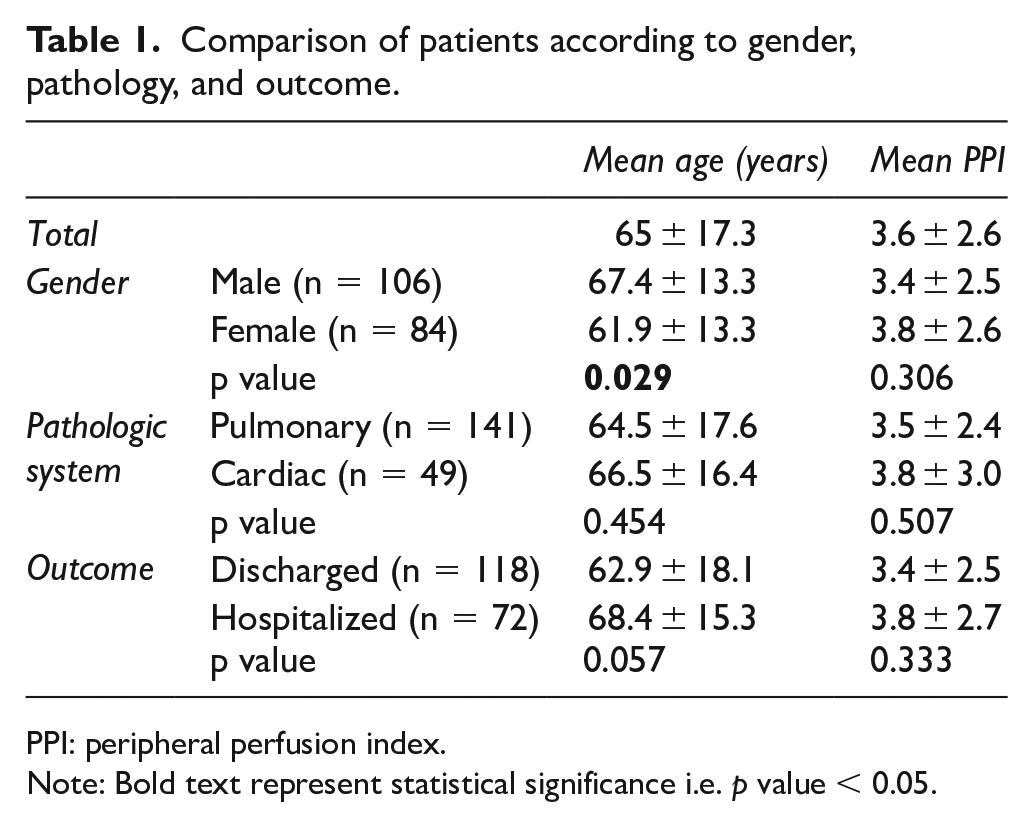
PPI: peripheral perfusion index.
Note: Bold text represent statistical significance i.e. p value < 0.05.
Of the patients, 72 (37.8%) were hospitalized. When the hospitalized patients were compared to those discharged from the ED, no significant difference was determined between the two groups regarding the mean PPI value and age (Table 1).
In 141 (74.2%) patients, the cause of dyspnea was found to be pulmonary-related pathologies, whereas, in 49 (25.7%) -patients, dyspnea was caused by cardiac pathologies. Even though the mean age and PPI value of the patient group with pulmonary pathologies were lower compared to the group with cardiac pathologies, the difference was not statistically significant (Table 1).
When 72 hospitalized patients were investigated, it was found that 52 (72.2%) were admitted to the Pulmonary Clinic, 20 (27.8%) to the Cardiology Clinic, and in 15 (20.8%) patients, the outcome was fatal. The mean age and PPI value of the patients admitted to the Pulmonary Clinic were 68 ± 15.8 years and 3.5 ± 2,2, respectively, whereas these values were 69.5 ± 14.0 years and 4.7 ± 3.7, respectively, in the patient group admitted to the Cardiology Clinic. No significant differences were determined between the two groups regarding the mean PPI value and age (p = 0.816, p = 0.414, respectively).
When 141 patients in whom a pulmonary pathology was diagnosed in the ED were investigated, it was found that 52 (36.8%) patients were decided to be hospitalized. When the hospitalized and discharged patients were compared, no significant differences were found regarding distributions of age, gender, and PPI value. Similarly, when the hospitalized and discharged patients among those admitted due to a cardiac pathology were compared, no significant differences were found regarding distributions of age, gender, and PPI value. The statistical data of the two groups were presented in Table 2.
Comparison of hospitalized and discharged patients according to pathologic system.
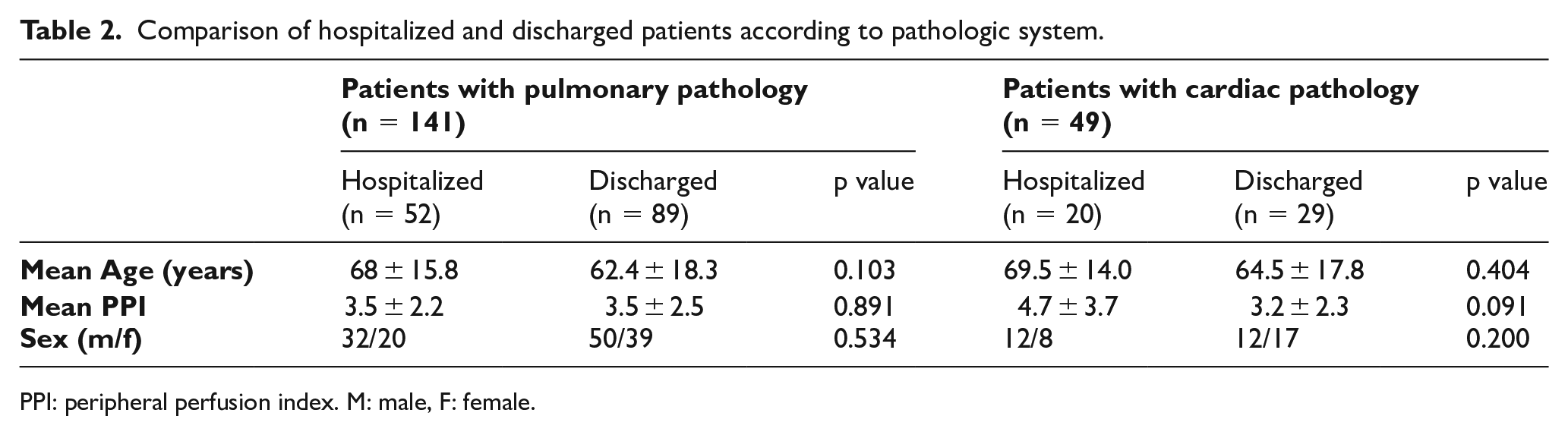
PPI: peripheral perfusion index. M: male, F: female.
Discussion
This study aimed to investigate whether PPI measurement contributed to clinical assessment in patients presenting with dyspnea to the ED. According to our knowledge, no other study conducted in this regard is present in the literature, and our study has clinical importance in this aspect. The results of our study revealed that the PPI value was not a valid parameter for the prediction of hospitalization and discrimination of cardiac and pulmonary pathologies in patients presenting with dyspnea to the ED.
PPI has gained popularity as a noninvasive and easy-to-measure parameter about showing impaired peripheral perfusion in critical patients in recent years. Initially, Lima et al. 6 showed in intensive care patients that a PPI value equal to or below 1.4 was a powerful indicator of impaired perfusion. Pirneskoski et al. 7 proposed that the dimensions of the pulse photoplethysmography wave amplitude could be used as a triage parameter for patient evaluation in the ED. Even though such a result might suggest that PPI could serve as a parameter for hospitalization and mortality in ED patients, Oskay et al. 8 reported that PPI was an invaluable parameter for the prediction of hospitalization and mortality in ED patients in the critical area. Although conducted on patients with dyspnea only, our study seemed to support the results of the study conducted by Oskay et al. The fact that the study conducted by Pirneskoski et al. had involved all patients instead of those in the critical area only might have led to such contradictory results.
The differential diagnosis of pulmonary and cardiac pathologies in patients presenting with the complaint of dyspnea is a serious clinical challenge for emergency physicians. Even though the most reliable method for identification of cardiac pathologies is echocardiography, it has various limitations such as not being present in all EDs, the dependency of its results on the person performing the procedure, and its requirement for serious training and experience. Similarly, the computed tomography, arterial blood gas measurements, and the spirometric measurement method, all frequently used for the identification of pulmonary pathologies, have various limitations such as being invasive, involving radiation, and not being commonly available. For this reason, approach methods for rapid assessment of patients presenting with dyspnea to EDs have been under investigation for a long time,9–11 and the search for a reliable method has still been continuing. Boubaker et al., 12 in the study that they reported in 2016, stated that in patients admitted to EDs due to exacerbations of chronic obstructive pulmonary disorder (COPD), the high change rate of the pulse amplitude in plethysmography with the Valsalva maneuver might hide a cardiac functional disorder. In that study, the difference between the patient group with heart failure and the COPD patients without heart failure was determined to be significant regarding the change rate of plethysmographic pulse amplitude. In the direction of this result, we had established the hypothesis of our study on the fact that the PPI value, calculated according to the plethysmographic pulse amplitude, might be a valid parameter for discriminating cardiac and pulmonary pathologies in patients presenting to EDs with dyspnea. However, our study revealed that the PPI value was unsuccessful in this regard.
Our study had various limitations. The most critical limitations were its retrospective and single-center nature, together with not being able to reach a patient number enough to make comparisons among specific diagnoses. Besides, because of its retrospective nature, the opinion of the responsible physician was used instead of objective data such as laboratory and imaging tests for differential diagnosis of pulmonary and cardiac pathologies. Clearer data might be presented with prospective studies depending on more objective diagnostic methods.
In conclusion, since PPI is a noninvasive, easy-to-measure, rapid, and reproducible test, it has been promising as a prognostic and diagnostic parameter for clinicians. However, it has been realized that PPI was unsuccessful in the evaluation of patients with dyspnea, in the differential diagnosis of cardiac and pulmonary pathologies, and prediction of hospitalization status. More comprehensive studies are required in this regard.
Footnotes
Author contributions
K.K. and E.S.G. researched literature and conceived the study. K.K. was involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. K.K. and E.S.G. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availably of material
Can be provided on request.
Informed consent
Written informed consent was not necessary because no patient data has been included in the manuscript.
Ethical approval
Ethical approval was obtained from Süleyman Demirel University Faculty of Medicine Clinical Research Ethics Committee (with the date of Nov 29th, 2019, and number 313).