
Abstract
Background:
Optimal cut-offs for B-type natriuretic peptide (BNP) for the diagnosis of heart failure differ based on ethnicity. There are no data for Southeast Asian patients. We aimed to define the optimal cut-off points and the strength of B-type natriuretic peptide as a predictor of heart failure in Southeast Asian multiethnic population.
Methods:
Bedside B-type natriuretic peptide (SOB panel (Biosite®)) was measured for patients (>50 years) presenting with dyspnea. Emergency physicians (blinded to B-type natriuretic peptide result) assessed the probability of acute heart failure on a scale of 0%–100%. Heart failure diagnosis was adjudicated by two cardiologists.
Results:
In all, 43% (n = 87) of the 203 dyspneic patients (54.7% males, 453% females) had a final diagnosis of acute heart failure. B-type natriuretic peptide values ranged from 3.2 to 4960 pg/mL (median, 189 pg/mL). Median B-type natriuretic peptide values of patients with the final diagnosis of “acute heart failure,” “no acute heart failure but history of heart failure,” and “no heart failure” were 600, 301, and 68 pg/mL, respectively. The optimum cut-off was 186 pg/mL. The receiver operating characteristic curve of the emergency physician’s assessment of the probability of heart failure based on clinical assessment had an area under the curve of 85% (95% confidence interval: 80%–90%). Combining receiver operating characteristic curves of physician assessment and B-type natriuretic peptide values yielded an area under the curve of 96% (95% confidence interval: 93%–98%). B-type natriuretic peptide levels less than 100 pg/mL were the strongest predictor of heart failure (odds ratio: 26.36; confidence interval: 6.85–101.41), followed by upper lobe diversion and cardiomegaly.
Conclusion:
The accuracy of bedside B-type natriuretic peptide was validated in a multiethnic Asian population. Optimum cut-off is 186 pg/mL. A B-type natriuretic peptide >100 pg/mL is the single strongest independent predictor of heart failure.
Introduction
Heart failure is a major health problem affecting 23–26 million people globally. 1 An increasing prevalence has been noted over the past decades, particularly in Asian countries.1–4 Acute heart failure accounts for 0.77% of all emergency department (ED) visit and about 5%–10% of all hospital admissions. 5
The diagnosis of acute heart failure particularly in the emergency setting is challenging as only about 65% of patients present with the hallmark symptom of acute dyspnea. 6 Novel diagnostic categories comprising heart failure with preserved ejection fraction (HFpEF) and heart failure with mid-range ejection fraction (HFmrEF) complicate matters further.7,8 There is no single definite “gold standard” diagnostic test to confirm a heart failure diagnosis. Natriuretic peptides have been widely studied as markers of heart failure and have been shown to be of diagnostic value in dyspneic patients with an uncertain diagnosis. Major guidelines incorporated the use of natriuretic peptides into their diagnostic algorithms.9,10 A B-type natriuretic peptide (BNP) value of less than 100 pg/mL is accepted as the threshold, below which heart failure can generally be ruled out. 11 Optimal cut-off points have, however, been shown to differ based on ethnicity.12–14 There are no published data regarding the point-of-care (PoC) BNP testing in a Southeast Asian multiethnic population.
The study at hand explores two questions. First, it defines the accuracy and optimal cut-off points of the BNP assay in a multiethnic Asian population. Second, it assesses the strength of BNP as a predictor of heart failure in patients presenting with acute onset dyspnea compared to history, clinical findings, chest radiography, and electrocardiogram.
Methodology
The study was approved by the institutional ethics committee. All patients aged 50 years and above presenting to the ED with the chief complaint of shortness of breath were prospectively recruited for the study over a 1-year period in 2012. Patients whose dyspnea was related to trauma, pneumothorax, cardiac tamponade, acute coronary syndrome, or a history of renal impairment (estimated glomerular filtration rate of <60 mL/min/1.73 m2) were excluded from the study. Informed consent was obtained verbally from all study subjects. The bedside BNP measurement was performed with the SOB panel (Biosite® Diagnostics Inc., San Diego, CA) following the patient’s clinical examination. 15
The treating emergency physician assessed the probability of acute heart failure on a scale of 0%–100% for each patient based on history, clinical findings, and routine blood test and chest X-ray results. This clinical judgment of probability of heart failure was categorized as low, uncertain, and high in the following ranges: 0%–20%, 21%–79%, and 80%–100%, respectively. The assessor was blinded to the result of the BNP measurement.
The final diagnosis was determined by two cardiologists. The cardiologists independently reviewed all data including demographic factors, history of presenting complaints, physical examination findings, blood test results, electrocardiograms, chest radiographs, and echocardiograms. Formal echocardiography was requested for all patients recruited into the study. The cardiologists were blinded to the patient’s BNP levels. Patients were categorized as (a) dyspnea due to acute heart failure, (b) dyspnea due to non-cardiac causes, but with a history of heart failure, and (c) dyspnea due to non-cardiac causes. If there was disagreement, a third cardiologist reviewed the case.
Statistical analysis was performed using SPSS version 18 for windows (SPSS, Inc., Chicago, IL). Baseline characteristics are reported in counts and percentage or mean ± standard deviation. Group comparison was performed using independent t-test and Mann–Whitney test as appropriate. For further statistical analysis, the patients without heart failure were grouped together with the patients with a history of heart failure but no current heart failure. Pearson’s chi-square test was used to test the association of independent categorical variables with heart failure and t-test for comparison of continuous data. Multiple logistic regression analysis was used to evaluate the ability of BNP (at a cut-off level >100 pg/mL) as an independent predictor of heart failure when compared to history and clinical findings in one model and to electrocardiographic and roentgenographic findings in another separate model. A final multiple logistic regression model was presented when combining all independent variables associated with heart failure to determine the most parsimonious combination to predict heart failure. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV), and accuracy of bedside BNP values were calculated for a selection of cut-off points using receiver operating characteristic (ROC) analysis. The optimal cutoff point was derived from the point on the ROC curve at which the sum of sensitivity and specificity was maximal. The ROC curve analysis was performed for the bedside BNP levels and the emergency doctors’ evaluation of the probability of heart failure using the cardiologist’s final diagnosis as the criterion standard. The areas under the curve (AUCs) were calculated and used to compare the diagnostic accuracy of BNP tests, emergency physicians’ assessment of the probability of heart failure, and the combination of the bedside BNP and the emergency physicians’ evaluation of the probability of heart failure to determine whether there is any significant improvement in the diagnostic accuracy of the emergency physicians’ evaluation of heart failure by adding bedside BNP results to the clinical findings. A value of p < 0.05 was considered statistically significant.
Results
A total of 203 patients with the presenting complaint “dyspnea” were recruited. The study population comprised 111 males (54.7%) and 92 females (45.3%). The final diagnosis, adjudicated by at least two cardiologists, was dyspnea due to heart failure in 87 (43%) patients, dyspnea due to non-cardiac causes but with a history of heart failure in 12 (6%) patients, and dyspnea due to non-cardiac causes in 104 (51%) patients, resulting in an acute heart failure diagnosis in 43% and a non-acute heart failure diagnosis in 57% of the patients. One hundred seventy-four (85.7%) patients were admitted to the wards and 29 (14.3%) patients were discharged directly from the ED. Of the 174 admitted patients, 132 (75%) received a formal echocardiogram. Sixteen (55%) of the 29 patients discharged directly from the ED received a formal echocardiogram prior to discharge. Demographic details as well as comorbidities, symptoms, and findings on clinical examination are presented in Table 1.
Demographics and clinical findings.
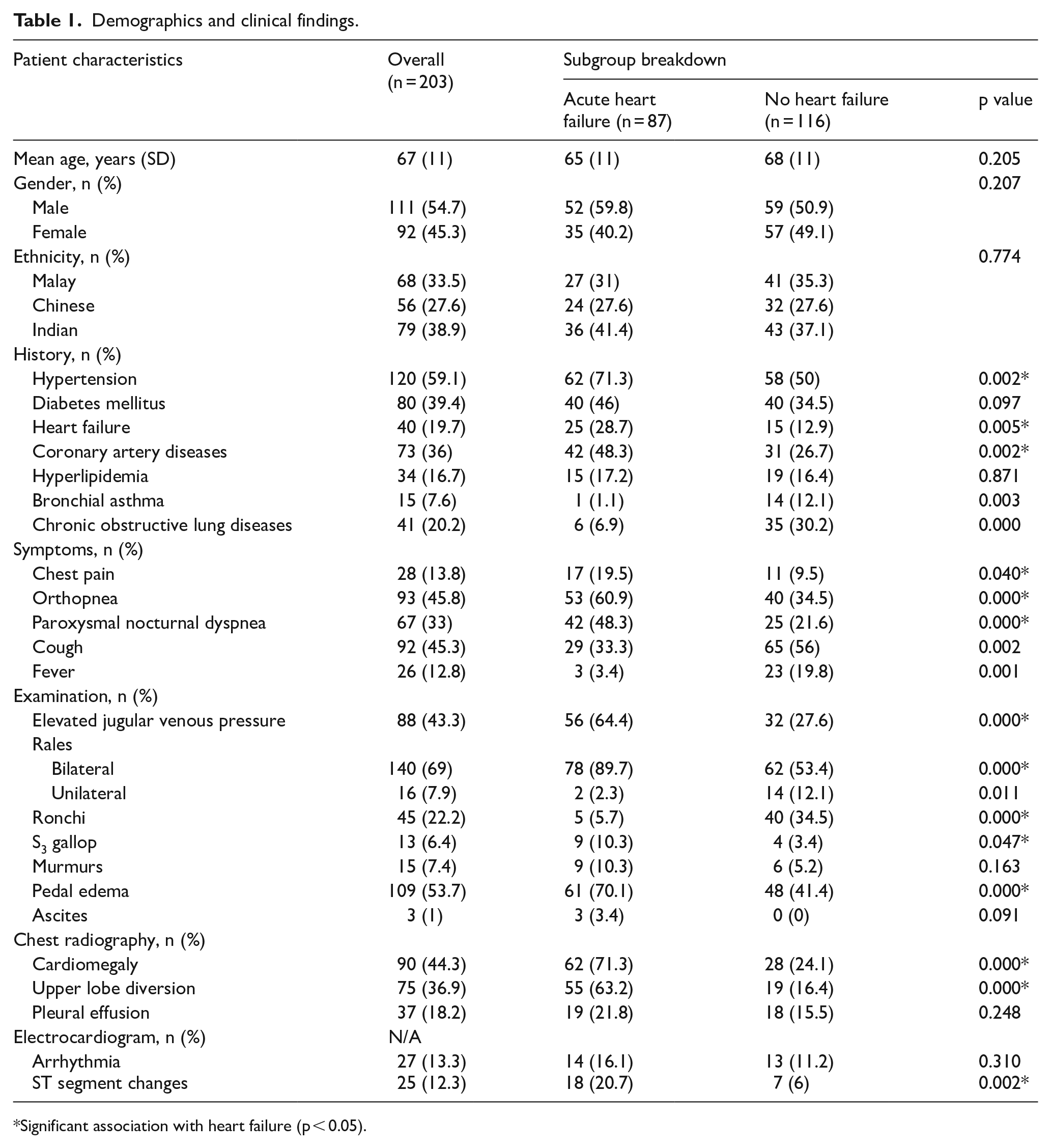
Significant association with heart failure (p < 0.05).
The PoC BNP values ranged from 3.2 to 4960 pg/mL. The median BNP value was 189 pg/mL. The median BNP value of patients with the final diagnosis of “acute heart failure,” “no acute heart failure but history of heart failure,” and “no heart failure” was 600, 301, and 68 pg/mL, respectively (p < 0.05).
The ability of BNP to diagnose acute heart failure as the cause of dyspnea was assessed with ROC curve analysis for various cut-off points. The guideline-recommended cut-off of 100 pg/mL had a sensitivity of 97%, specificity of 54%, accuracy of 72%, PPV of 61%, and NPV of 95% in the study population. The sum of sensitivity and specificity was maximized at 186 pg/mL and hence is considered the optimum cut-off value for BNP in this study (Table 2).
Diagnostic performance of various cut-off points of PoC BNP.
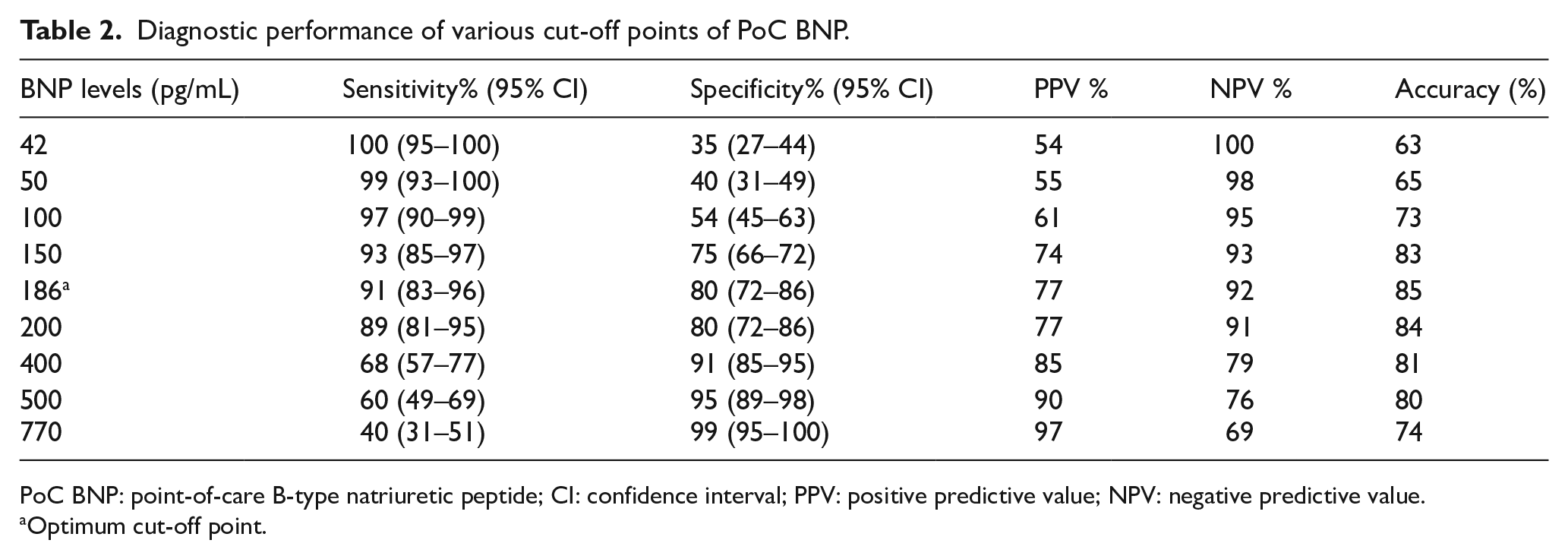
PoC BNP: point-of-care B-type natriuretic peptide; CI: confidence interval; PPV: positive predictive value; NPV: negative predictive value.
Optimum cut-off point.
The ROC curve of the emergency physician’s assessment of the probability of heart failure based on clinical assessment had an AUC of 85% (95% confidence interval (CI): 80%–90%). Combining the ROC curves of the physician’s assessment of the probability of heart failure with that of the BNP values yielded an AUC of 96% (95% CI: 93%–98%), which is significantly better than the AUC of the clinical probability and BNP values alone (p < 0.05) (Figure 1)
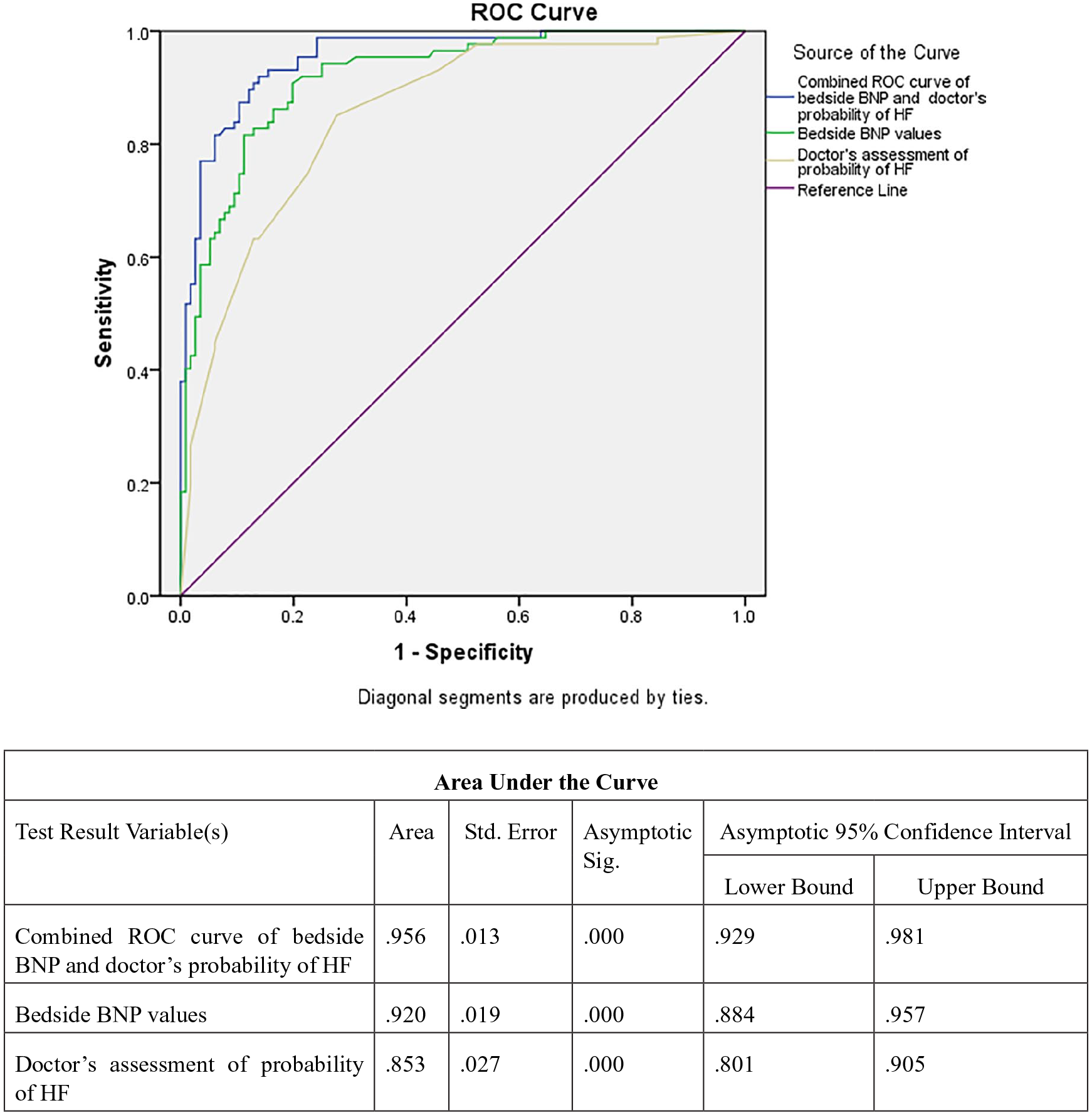
Comparison of receiver operating characteristic (ROC) curves of bedside BNP versus doctor’s assessment of probability of heart failure versus the combination of these assessments to evaluate the accuracy of BNP to diagnose heart failure as the cause of dyspnea.
A multiple logistic regression analysis was performed for factors found to be associated with the correct diagnosis of “acute heart failure” on univariate analysis. A BNP level of 100 pg/mL was the strongest independent predictor of heart failure with an odds ratio of 26.36 (95% CI: 6.85–101.41, p < 0.05) followed by upper lobe diversion and cardiomegaly on chest radiography (Table 3).
Multivariable model evaluating the ability of BNP (⩾100 pg/mL) to identify heart failure when compared to patient’s demographic characteristics, history, clinical findings, and chest radiography.
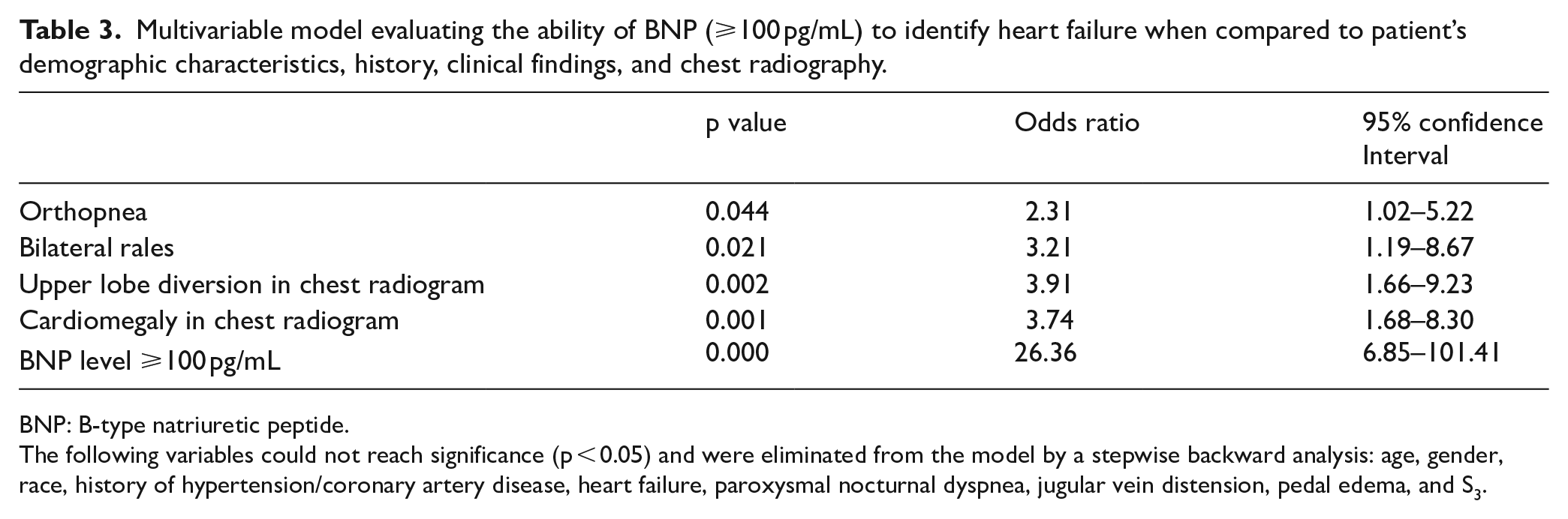
BNP: B-type natriuretic peptide.
The following variables could not reach significance (p < 0.05) and were eliminated from the model by a stepwise backward analysis: age, gender, race, history of hypertension/coronary artery disease, heart failure, paroxysmal nocturnal dyspnea, jugular vein distension, pedal edema, and S3.
Discussion
In our specific study population (patients 50 years and above, presenting with acute onset shortness of breath to the ED), heart failure was the final diagnosis in 43% of cases. The vast majority of patients (85.7%) regardless of the final diagnosis required admission to hospital.
The main strength of this study is the confirmation of the overall good accuracy of PoC BNP testing and the definition of an optimal cut-off point for BNP in the diagnosis of acute heart failure in a multiethnic Asian population. This optimal cut-off point of 186 pg/mL was derived from the ROC curve of BNP against the final diagnosis and had 91% sensitivity, 80% specificity, 77% PPV, 92% NPV, and 85% accuracy. The cut-off point was higher in our study population when compared to Maisel’s landmark study “Breathing Not Properly.” 15 There are possible explanations for this difference: (1) our study population was older. The most common reason for acute dyspnea in younger patients is respiratory disease. We intentionally excluded patients younger than 50 years to address the middle to higher age dyspneic patient population where diagnostic ambiguity is much greater. It is well established that BNP levels increase with age. (2) Our patients had a high rate of comorbidities: 59%, 36%, and 20% had hypertension, coronary artery disease, and congestive heart failure, respectively. Studies suggest higher BNP levels in patients with a history of hypertension.16,17 (3) Ethnic differences most certainly also contribute to the difference observed. Deepak found generally lower natriuretic peptide (NP) levels in Black individuals. 13 Korean and Japanese studies identified even higher cut-off points at 296 and 234 pg/mL and explained the difference with ethnic factors and the generally lower body mass index in Asians.12,14 Generally, BNP cut-off values are greatly dependent on the type of BNP assay used and the study population, and efforts should be made to establish suitable parameters in different ethnic groups.4,13,18
We also examined the performance of the optimal cut-off point of 100 pg/mL as recommended by guidelines for our study population. The study found that it had a higher sensitivity (97% vs 90%), lower specificity (54% vs 76%), and lower accuracy (72% vs 83%) than reported in the “Breathing Not Properly” study. 15 The PPV and NPV were 61% and 95%, respectively. Therefore, the cut-off point at 100 pg/mL still has a useful role in ruling out acute heart failure when used in our local population.
The AUC for the emergency physician’s clinical judgment was 0.85 (95% CI: 0.80–0.90), whereas the AUC for the BNP results alone was 0.92 (95% CI: 0.88–0.96). However, when BNP results and clinical probability percentage of heart failure were statistically combined, the AUC improved further to 0.96 (95% CI: 0.93–0.98) Therefore, our study adds to the body of evidence of the utility of BNP levels in conjunction with clinical judgment and the consideration of cardiac and non-cardiac factors that can affect it. Without doubt, patients presenting with acute dyspnea who could benefit the most from BNP testing are those whose diagnosis of “heart failure” is uncertain. Clinical uncertainty has been shown to be associated with increased morbidity and mortality. 19
Limitations and strengths
The study is limited by the rather small sample size. The study population is older than that of comparable studies with a higher rate of comorbidities. The findings might not be applicable to a younger population. One of the strengths of this study is the fact that the multiethnic population studied might be highly representative of Southeast Asian patients in general than a monoethnic study possibly could be. We used a convenience sample collected in a single center which is subject to sampling and selection bias. While two blinded cardiologists used all possible information in making the final heart failure diagnosis as our criterion standard in this study, we acknowledge that misclassification bias is possible and difficult to quantify.
Conclusion
The accuracy of the bedside BNP (Biosite) was validated in a multiethnic Asian population and an optimum cut-off point of 186 pg/mL was defined for PoC BNP in the diagnosis of heart failure in dyspneic patients who presented to the ED. A BNP >100 pg/mL was found to be the single strongest independent factor in predicting heart failure when compared to demographic characteristics, past medical history, clinical findings, and chest radiography. The bedside BNP test improved the diagnostic accuracy, especially for those patients whose diagnosis of acute heart failure is uncertain.
Footnotes
Authors’ contribution
M.Y. and S.S.J. collected and analyzed the data. M.I.Z. reviewed the manuscript. M.Y., A.L., and K.S. prepared the manuscript and are responsible for the overall content as guarantor. All authors have seen and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets used and/ or analyzed during the current study are available from the corresponding author on reasonable request.
Informed consent
Verbal informed consent was obtained from all subjects before the study. Written informed consent was not obtained because the ethics committee did not require informed written consent as for the observational nature of the study.
Ethical approval
The study was approved by the University of Malaya Medical Centre Ethics committee (No: 201782-5459).