
Abstract
A 65-year-old paraplegic patient just discharged from the medical ward 2 days ago with a negative left lower extremity Doppler study for deep vein thrombosis. He presented to the emergency department for deteriorating lower extremity swelling. Point-of-care ultrasound helped to swiftly arrive at the diagnosis and facilitate prompt management.
Keywords
Case presentation
A 65-year-old man presented to the emergency department (ED) with deteriorating left lower extremity (LE) swelling for several days. His past medical history included diabetes, hypertension, traumatic spine fracture in the 1970s leading to paraparesis and his being wheelchair bound. He was discharged 2 days ago from the general medical ward for an episode of unconsciousness, for which he had stayed as an inpatient for 1 week, undergone extensive workup, had his medication being titrated and a small pressure sore in his left buttock receiving regular dressing. His left thigh and leg was noted by the treating physician to be swollen and an ultrasound Doppler study was arranged on the day of discharge, which showed patent left LE veins and no evidence of deep vein thrombosis (DVT).
He attended the ED because his left LE swelling did not improve after discharge. When assessed by the emergency physician (EP), the patient was afebrile and not in distress. His blood pressure, heart rate, respiratory rate and saturation were all within normal ranges. His left LE appeared swollen with pitting oedema, yet not explicitly warm nor tender on palpation.
The patient was deemed at high risk of having a DVT for his LE immobility. A point-of-care ultrasound (POCUS) examination was therefore performed with a handheld device, originally intending to re-examine his left LE venous system (Figures 1 and 2, Supplemental Video 1). Usually the musculoskeletal or vascular systems are sonographically best assessed with a high frequency linear probe due to its superior temporal and spatial resolution; yet for this patient’s large body habitus and the degree of tissue swelling, a lower frequency curvilinear probe was utilized in order to achieve adequate penetrance. As can be seen in Figures 1 and 2, a depth of 6–8 cm was needed to fully cover the region of interest, which was far beyond the reach of a linear probe. For compression ultrasound exams, a handheld device is often sufficient for the task, but for other exams involving more detailed Doppler assessment or better tissue delineation, a higher end machine, which was not available to the physician then, could be more appropriate.
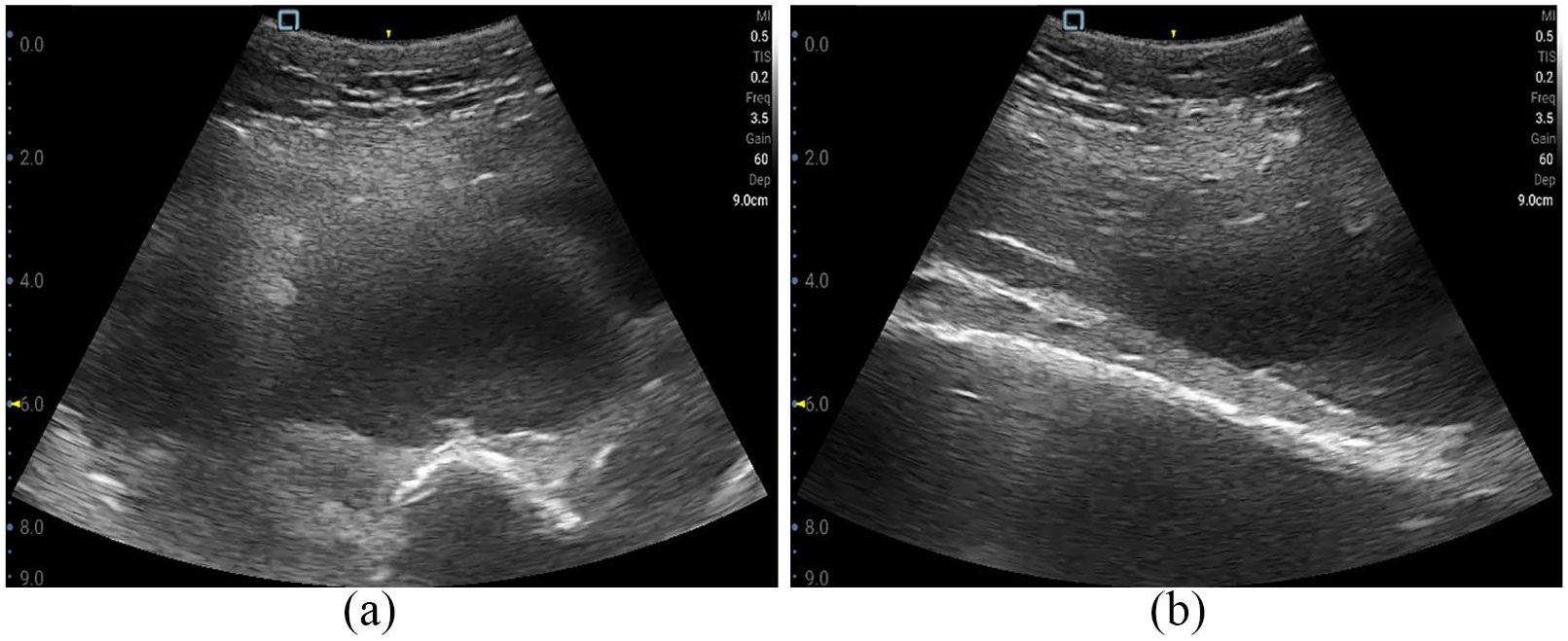
(a) Transverse view of the left mid-thigh level (a snapshot of Supplemental Video 1) and (b) longitudinal view showing the same collection in Figure 1(a).
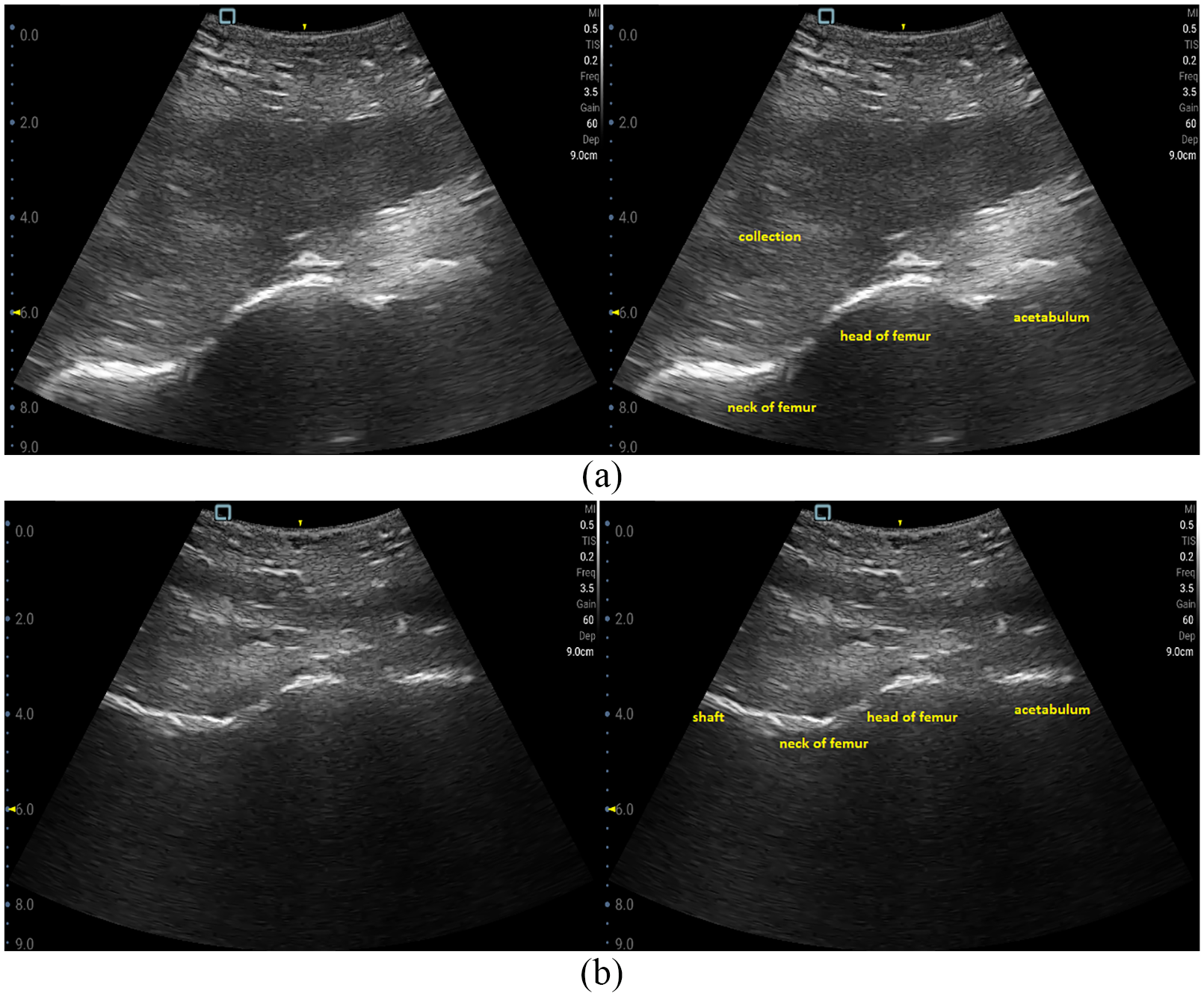
(a) Longitudinal view of the left hip; right: same image with label and (b) the unaffected hip under the same ultrasound settings for comparison; right: same image with label.
Question 1
What is the most striking finding of the POCUS images?
Answer 1
There was a sizable (up to 4 cm in diameter) anechoic collection lying right anterior to the femur, at least extending from the hip to mid-thigh. Heterogeneous materials could be seen therein especially in the dependent regions (frame 270–355 in Supplemental Video 1). There was fluctuance upon gentle compression (frame 133–188 in Supplemental Video 1) with positive swirl sign (frame 330–380 in Supplemental Video 1) and no pulsatility observed. These signs together were highly suggestive of an abscess. An urgent computed tomography (CT) was therefore ordered which confirmed a large abscess collection extending from the left iliopsoas down the anterior thigh to the level of the tibial tuberosity (Figure 3), which did not connect with the left buttock pressure sore mechanically. No intra-abdominal nor spinal pathologies were detected.
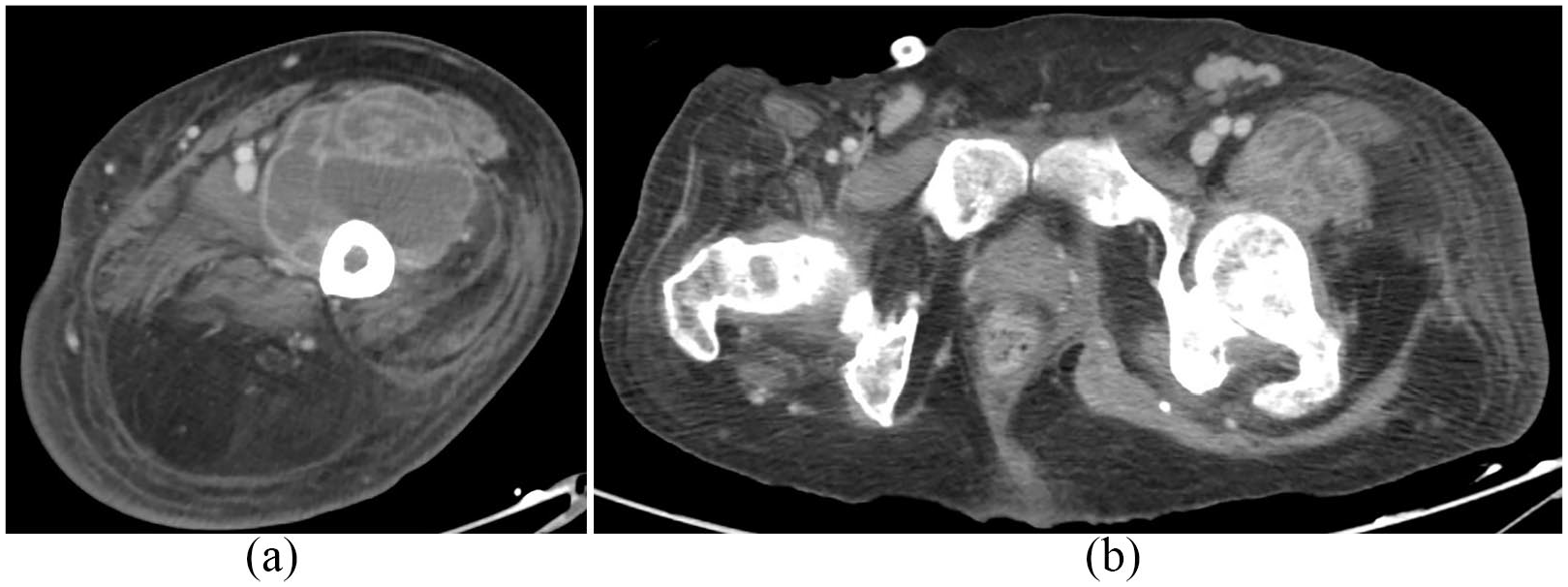
(a and b) CT images showing the abscess at mid-thigh and hip levels.
As the patient was stable then, instead of undergoing bedside drainage at the ED, he was admitted to the orthopaedic ward for urgent open surgical drainage. Before he was transferred to the operating room, he started to become febrile and developed septic shock. Intra-operatively more than 500 mL frank pus was drained, which subsequently grew coagulase-negative staphylococcus.
Discussion
Psoas abscess is a rare disease, and despite it is often taught to present with the ‘classical triad’, namely, fever, flank pain and limited hip movement, patients seldom come to the ED with the full triad. 1 The abscesses could be either primary or secondary usually to sacroiliac joints, gastrointestinal or urogenital pathologies.2,3 Most patients need CT for diagnosis. 4 Risk factors include diabetes mellitus, bed- or chair-bound states, intravenous drug use and being immunocompromised. Many cases require drainage as the definitive management and mortality could be as high as 14% in this locality. 3 EPs should always bear in mind that a swollen LE has many differential diagnoses. When there are no sonographic signs of DVT, one must try to seek for other possible diagnoses.
Footnotes
Author contributions
All authors contributed equally to this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for his anonymized information to be published in this article.
Ethical approval
It is not applicable for this clinical quiz.
Human rights
The data and images obtained were in accordance with the principles outlined in the Declaration of Helsinki.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.