
Abstract
Background:
Hyperglycemia in the acute phase after trauma is a stress response and a metabolic reflection in humans with injury, which could adversely affect outcome in trauma patients. In this study, we attempted to identify if hyperglycemia a reliable predictor for mortality in major trauma patients.
Objectives:
In order to identify if hyperglycemia a reliable predictor for mortality in major trauma, we designed and proformed a prospective observational study in a tertiary hospital.
Method:
We performed a prospective observational study to review the records of 601 patients with major trauma (injury severity scores >15) who visited our hospital’s emergency department from August 2012 to July 2015. Logistic regression was performed to assess the effect of hyperglycemia on mortality.
Result:
Major trauma patients in the hyperglycemia group had low systolic/diastolic blood pressure at triage, low initial Glasgow Coma Scale score, high incidence of hypotension episodes, coagulopathy, acidosis, and anemia. Hyperglycemia was significantly correlated with mortality in major trauma patients in this study (odds ratio: 1.97, 95% confidence interval: 1.04–3.74).
Conclusion:
In major trauma patients with injury severity scores >15, hyperglycemia has a positive correlation with mortality, which could be a predictor of mortality in clinical practice.
Introduction
Trauma is not only a medical problem but also a public health issue. The magnitude of the economic burden associated with injury-associated deaths underscores the need for effective prevention. 1 Similar injuries may lead to different outcomes in similar populations. For this reason, several models have been developed to predict outcome after injury. Hyperglycemia in the acute phase after trauma is a stress response and a metabolic reflection in humans with injury, which could adversely affect outcome in trauma patients. Hyperglycemia in trauma victims has been associated with significant traumatic brain injury (TBI), low Glasgow Coma Scale (GCS) score, and poor neurological outcome.2–5 Stress hyperglycemia has also been associated with increased morbidity and mortality in both trauma and critically ill patients.6–8 Yendamuri et al. 9 reported in a retrospective study of 738 patients that admission hyperglycemia was an independent predictor of increased intensive care unit (ICU) and hospital length of stay and mortality in the trauma population. Emergency department (ED) physicians are concerned with the resuscitation and identification risk of trauma patients. We try to measure the association of the initial serum glucose level in ED with the mortality of trauma. Our objective in this study was to prospectively evaluate whether hyperglycemia in ED is associated with increased mortality in major trauma (injury severity score (ISS) > 15) patients.
Materials and methods
Patient selection
We prospectively collected data on trauma patients who had ISS >15 and visited the ED in our hospital from April 2013 to March 2016. Patients who lost vital signs at any time before arrival at our hospital were excluded (insert Figure 1). Our hospital, located in south-central Taiwan, is a general hospital with surgeons and operating rooms available throughout the day. Our hospital is the only one in our region rated as “severe-grade emergency care ability hospital,” a rating similar to a level I trauma center, and can receive any major trauma patients for definitive care.
Flow chart of patient selection.
Data analysis
All trauma patients who visited our ED were monitored prospectively and were enrolled into our study once their ISS had been completed and was >15. We reviewed charts and recorded variables including age, ISS, systolic and diastolic blood pressure at triage, Glasgow Coma Scale (GCS), transfer from other hospitals, discharge diagnosis, and mortality or survival on discharge. Patients with initially serum glucose >200 mg/dL in our ED were defined as “hyperglycemia group,” otherwise as “normal group.” We defined these variables as follows: episodes of hypotension; episodes of systolic blood pressure less than 90 mmHg at the ED; hypothermia, body temperature less than 36°C; hyperthermia, body temperature ⩾38°C; acidosis, pH less than 7.35 in arterial blood gas test at the ED; coagulopathy, a prolonged prothrombin time test (international normalized ratio) result greater than 1.5; thrombocytopenia, platelet counts less than 100 × 103°µL; anemia, hemoglobin less than 10 mg/dL at the ED; and episodes of SpO2 < 90%, oxygen saturation less than 90% at the ED. Initial GCS scores were recorded as the first data assessed by physicians—either the initial evaluation in the ED in the case of transferred patients, or evaluation by our emergency physicians in the case of patients directly transported to our hospital. Prothrombin time test, hemoglobin, platelet counts, and blood gas test were assessed by first laboratory analyses.
Differences between hyperglycemia group and normal group were assessed using the chi-square test for categorical variables. The independent t-test was used to evaluate differences in continuous variables between these two groups. To identify the possible effects on mortality, the logistic model was applied for variables with p values <0.1 for differences between the hyperglycemia and normal groups.
Differences between mortality and survival were also assessed using the chi-square and independent t-test, as described between hyperglycemia and normal groups. Factors with p values <0.1 for the difference between the mortality and survival were also included into the logistic regression model. Because hyperglycemia is the major factor we evaluated, it was included in the logistic regression model. The logistic regression model was based on the enter procedure.
All statistical assessments were two-sided. Differences with p values <0.05 were considered statistically significant. Statistical analyses were performed using SPSS 20.0 statistics software.
Results
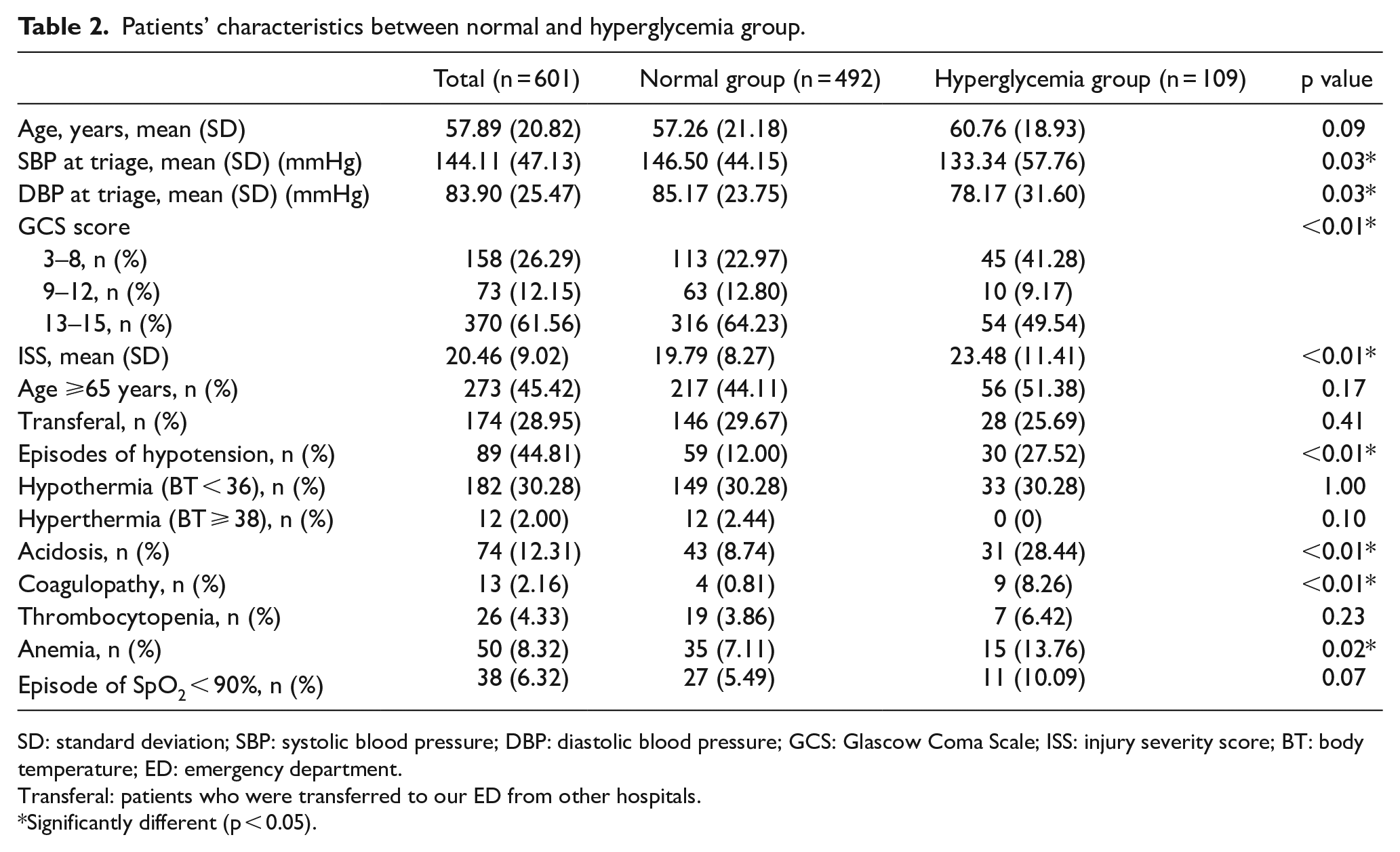
As shown in Table 1, in the analysis of initial variables recorded at ED, there were statistically significant differences with systolic blood pressure at triage (146.50 vs 133.34 mmHg, p = 0.03), diastolic blood pressure at triage (85.17 vs 78.17 mmHg, p = 0.03), episodes of hypotension (12.00% vs 27.52%, p < 0.01), acidosis (8.74% vs 28.44%, p < 0.01), coagulopathy (0.81% vs 8.26%, p < 0.01), anemia (7.11% vs 13.76%, p = 0.02), and initial GCS score between these two groups. Mortality rate in the hyperglycemia group was significantly higher than the normal group (13.62% vs 34.86%, p < 0.01). There was also significant difference in ISS between two groups (19.79 in normal group vs 23.48 in hyperglycemia group, p < 0.01). Age was similar in both groups.
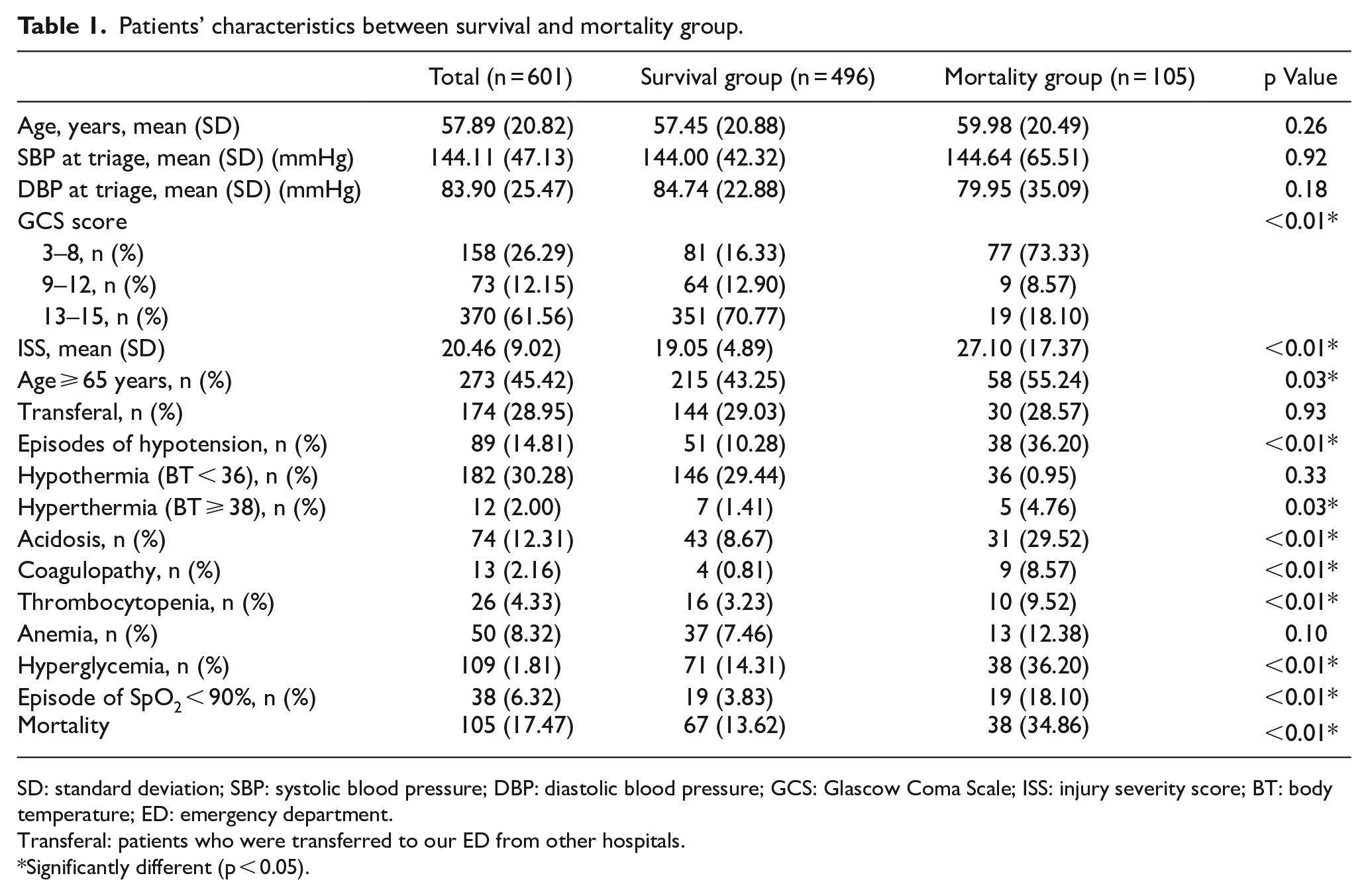
Patients’ characteristics between survival and mortality group.
SD: standard deviation; SBP: systolic blood pressure; DBP: diastolic blood pressure; GCS: Glascow Coma Scale; ISS: injury severity score; BT: body temperature; ED: emergency department.
Transferal: patients who were transferred to our ED from other hospitals.
Significantly different (p < 0.05).
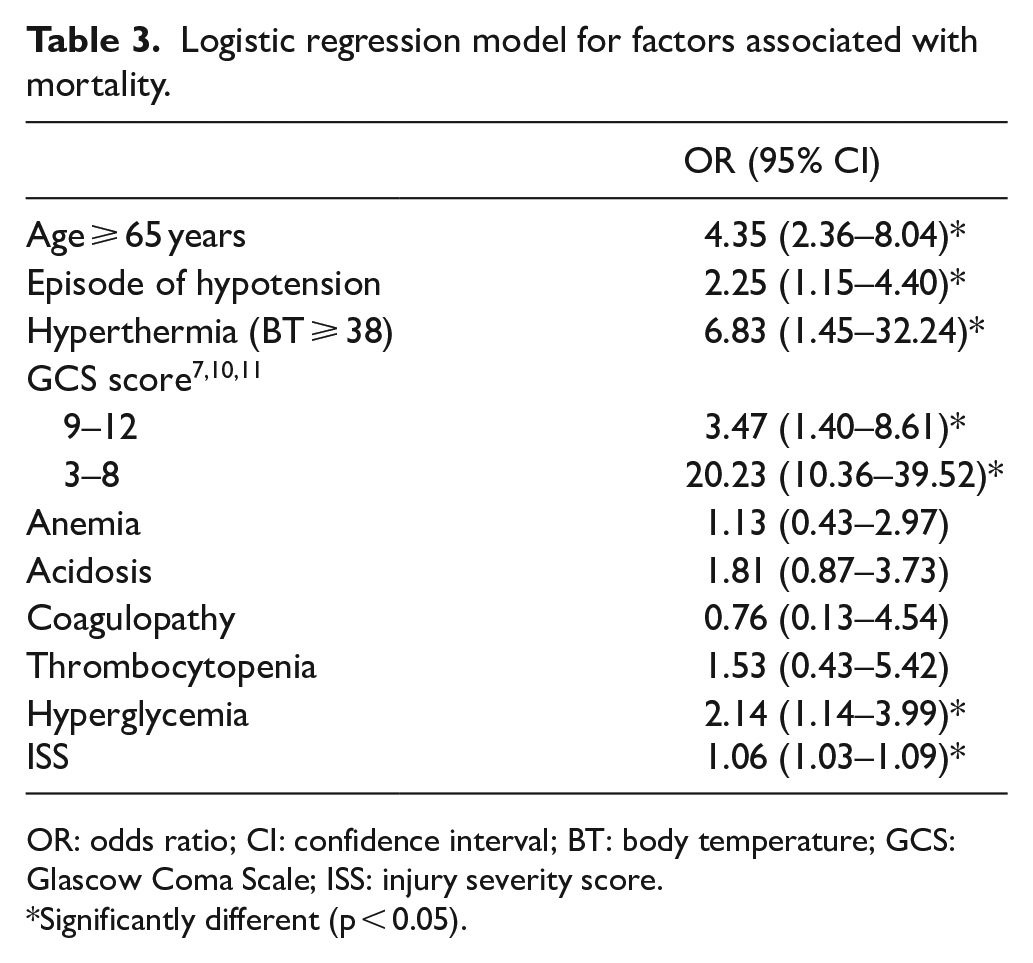
The analysis of variables between survival and mortality is summarized in Table 2. There were significant differences between the patients who survived and those who did not include initial GCS score; ISS score; subgroup of age ⩾65 years; percentage of patients with episodes of hypotension, hyperthermia, acidosis; coagulopathy; thrombocytopenia; hyperglycemia, and episodes of SpO2 < 90% (Table 2). After controlling for the factors significantly related to mortality, we found that age ⩾65 years (odds ratio (OR): 4.37, as shown in Table 3), hyperthermia (OR: 7.12), initial GCS score (OR: 0.73), and hyperglycemia (OR: 1.97), which did significantly affect mortality.
Patients’ characteristics between normal and hyperglycemia group.
SD: standard deviation; SBP: systolic blood pressure; DBP: diastolic blood pressure; GCS: Glascow Coma Scale; ISS: injury severity score; BT: body temperature; ED: emergency department.
Transferal: patients who were transferred to our ED from other hospitals.
Significantly different (p < 0.05).
Logistic regression model for factors associated with mortality.
OR: odds ratio; CI: confidence interval; BT: body temperature; GCS: Glascow Coma Scale; ISS: injury severity score.
Significantly different (p < 0.05).
Discussion
In logistic regression model for factors associated with mortality, hyperglycemia was an independent risk factor (OR: 1.97) in major trauma based on our findings. ED physicians are often the first to evaluate patients with major trauma and therefore should be aware of the risk and management. Major trauma patients with hyperglycemia in ED should be monitored closely and receive aggressive treatment to prevent mortality. Hyperglycemia has been observed after injury in both diabetic and nondiabetic patients. 12 Among trauma patients, the association of outcome with hyperglycemia has been studied extensively in brain-injured patients, in whom it portends a poorer prognosis. 13 Yendamuri et al. 9 showed that admission hyperglycemia is associated with increased mortality and length of ICU and hospital stay in trauma patients. Limited data exist in major trauma populations. We found that hyperglycemia group in major trauma has high incidence of hypotension, low GCS score, acidosis, coagulopathy, and high ISS. Paladino et al. 14 reported that triage hyperglycemia is a prognostic indicator of major trauma, which can be used in differentiating minor from major injury. Abrupt metabolic response to injury could include major modifications of circulating cortisol, glucagon, and epinephrine resulting in impaired metabolism of glucose associated with insulin resistance, high blood and tissue glucose levels, intracellular acidosis, lactate accumulation, and consequently neuronal injury, which may increase severity of injury.5,7,10 Normalization of blood glucose using an intensive insulin protocol improved clinical outcomes and decreased mortality by 42%. 11 Age ⩾ 65 years, hyperthermia, GCS score, and ISS were also significant predictors, which were compatible with recent studies.15–17
This study has several limitations. Its relatively small sample size and study design (we use the initial blood glucose level in ED) may result in a wide range in the confidence interval of our factors and also limits the evaluation of other significant predictors. It does not analyze the effect of hypoglycemia on outcome, as glucose distribution may cause a bimodal increase in mortality. We also did not analyze differences between penetrating and burn injuries. Furthermore, trauma patients’ past medical history was hard to clarify in ED setting, especially for those who need resuscitation. The mortality may be caused by poor comorbidity. More large studies are required to determine the significance of these findings.
Conclusion
In conclusion, we found hyperglycemia as a positive predictor of mortality (OR: 1.97) in major trauma patients (ISS > 15), who had not lost vital signs before arrival at our hospital. More studies are required to determine the significance of these findings and develop guideline or scoring system including hyperglycemia or glucose level for major trauma patients’ management.
Footnotes
Acknowledgements
The authors thank all the participants who participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Chang Gung Memorial Hospital Research Project Grant, Taiwan (No. CMRPG6C0151, CMRPG6C0152, CMRPG6C0153).
Availability of data and materials
Please contact author for data requests.
Ethical approval
This study was approved by Institutional Review Board of Chang Gung Memorial Hospital (No. 101-4497C, 104-0559C)