
Abstract
Objective:
To investigate whether high-flow nasal cannula oxygen therapy could reduce the rate of endotracheal intubation and improve arterial blood gas values, vital signs, and clinical outcomes of patients with hypoxemic acute respiratory failure as compared with conventional oxygen therapy alone.
Methods:
This retrospective, observational study was performed in the 15-month study period and included adult patients with tachypnea and hypoxemia, whose vital signs and arterial blood gas were monitored. The high-flow nasal cannula oxygen group consisted of patients admitted to the emergency department with acute respiratory failure when high-flow nasal cannula oxygen treatment was available in the hospital, while the conventional oxygen therapy group consisted of patients who have presented to the emergency department with acute respiratory failure in the absence of high-flow nasal cannula oxygen device in the hospital. The primary outcome of the study was improvement in vital signs and arterial blood gas values within first and fourth hours of the treatment. The second outcome was the need for intubation in the emergency department, length of hospital stay, and hospital mortality.
Results:
The decrease in the pulse and respiratory rate of high-flow nasal cannula oxygen–treated group was significantly greater than the conventional oxygen therapy group on the first and fourth hours of treatment (p < 0.001). PaO2 values were significantly higher in the high-flow nasal cannula oxygen group at the first and fourth hours of treatment (p ⩽ 0.001). Likewise, mean SaO2 levels of patients receiving high-flow nasal cannula oxygen treatment was significantly higher than those of patients in the conventional oxygen therapy group (p = 0.006 at 1 h and p < 0.001 at 4 h). In the hypercapnic patients, the decrease in PaCO2 and increase in pH and PaO2 values were significantly greater in high-flow nasal cannula oxygen group (p < 0.001). The difference between the groups regarding the need for invasive mechanical ventilation was not statistically significant (p = 0.179).
Conclusion:
High-flow nasal cannula oxygen treatment has been associated with favorable effects in vital signs and arterial blood gas values in patients with acute respiratory failure. High-flow nasal cannula oxygen might be considered as the first-line therapy for patients with hypoxemic and/or hypercapnic acute respiratory failure.
Keywords
Introduction
Acute respiratory failure (ARF) is a frequent and life-threatening cause of emergency department (ED) presentations. A myriad of diseases such as pneumonia, heart failure, chronic obstructive pulmonary disease (COPD), and exacerbation can trigger dyspnea and/or other manifestations of ARF. 1 The first-line agent in the treatment is oxygen. The preferred method for oxygenation varies from nasal cannula to mechanical ventilator depending on the severity of the patient’s respiratory distress. 2 High-flow nasal cannula oxygen (HFNCO) therapy is rapidly evolving as an alternative to conventional oxygen therapy (COT) in critically ill patients. 3 The HFNCO system is a method in which air and oxygen are mixed and humidified and heated, and given by a single circuit with a high current through the nasal cannula. The advantages of HFNCO are providing positive pressure, high flow, constant FiO2, washout of the nasopharyngeal dead space and allowing the patient to talk and oral intake.4,5
The increase in the number of patients presenting to ED with ARF leads to prolongation of the length of stay in the ED due to the high rates of bed occupancy in hospitals. 6 This situation increases the importance of the treatment of patients in ED critical care units. Therefore, the clinical utility of HFNCO treatment in ED critical care units is increasing day by day. 7
The objective of this study is to investigate whether HFNCO could reduce the rate of endotracheal intubation and improve arterial blood gas (ABG) values, vital signs, and clinical outcomes of patients with hypoxemic ARF as compared with COT alone.
Materials and methods
Study design
This retrospective, observational study was performed in the predefined 15-month study period between 1 May 2017 and 1 August 2018, in the ED of a tertiary care community hospital in an industrialized southern city of Turkey. The annual patient volume of the ED is approximately 350,000 patients. The HFNCO group consisted of patients admitted to the ED with ARF in the period when HFNCO treatment was available in the hospital (after January 2018), while the COT group consisted of patients who have presented to the ED with ARF in the absence of HFNCO device in the hospital. Therefore, the COT group served as a historical control for the HFNCO group. The Institutional Review Board approved the study.
Population
Patients over 18 years of age with tachypnea (respiratory rate > 25 breaths/min) and hypoxemia (PaO2 < 60 mmHg in ABG, SaO2 < 92%) and whose vital signs and ABG values were monitored hourly in critical care unit at least 4 h and whose clinical and laboratory data were completely accessible via the hospital information system were included in the study.
Pulse rates, blood pressures, respiratory rates, and pulse oximetry were monitored closely. Hourly ABG follow-up was performed via invasive arterial lines. All patients in each treatment arms received usual medical care and this was not affected by the study protocols. Patients who were hemodynamically unstable, who had a Glasgow Coma Scale score ⩽ 12 on presentation, those with urgent need for endotracheal intubation, victims of trauma, and those with documented contraindications to non-invasive mechanical ventilation (NIMV) (e.g. suspected of pneumothorax, maxillofacial trauma) and whose data could not be reached completely were excluded from the study.
In the high-volume urban community hospital, only a minority of the patients with ARF can be admitted to the intensive care unit (ICU), and a substantial percentage of critical patients are transferred to another institution due to lack of intensive care beds. During the study period, invasive mechanical ventilation (IMV) has been available in our ED but NIMV was not available, thus we are still unable to use NIMV. HFNCO therapy has been used in the ED after January 2018.
Data collection and measurement
Demographic variables such as age and sex, chief complaint on presentation, comorbidities, presumptive diagnosis, vital signs, ABG values, need for intubation, length of stay, clinical course, and outcome were recorded.
All ABG values were measured at the discretion of the ED physician using Radiometer ABL90 flex machines (Radiometer, Copenhagen, Denmark). Wall-mounted oxygen systems were used to provide COT to the patients with ARF. Oxygen was given by titration with flowmeter according to the needs of the patients with nasal cannula (1–6 L/min) or oxygen facial mask (4–10 L/min). Oxygen supplements were titrated in accordance with the PaO2 levels in the hourly ABG results via the wall-mounted oxygen sources. Vapotherm, Precision Flow (Exeter, ABD) equipment was used for HFNCO treatment. Disposable ventilator circuits and nasal cannulae were used for each patient in the study.
All physicians, nurses, and supporting healthcare personnel working in the critical care unit were informed about the use of HFNCO device. The temperature, flow, and FiO2 parameters of the HFNCO device were adjusted according to the characteristics of the patients and the ABG values. For hypoxemic and hypercapnic patients, FiO2 was set at lower (50%–60%) values, but set at higher values (70%–100%) in normocapnic hypoxic patients. The cut-off value for hypercapnia was PCO2 > 45 mmHg. NIMV mode was not applied to hypercapnic patients because it was not available in the ED. The flow rate was commenced from 20 L/min and adjusted to the patient’s clinical status, diagnosis, radiological findings, and the target positive end-expiratory pressure (PEEP). Maximum flow rate was 40 L/min. The temperature was set as 37°C to be close to body temperature. Oxygen in lower temperatures were given to patients who were not able to tolerate this modality.
If HFNCO or COT treatments failed, endotracheal intubation was performed in the ED. The following clinical criteria were taken into consideration to proceed with endotracheal intubation:
Incessant and worsening hypoxemia despite proper treatment;
Worsening tachypnea;
Increased PCO2 and persistent respiratory acidosis despite optimal standard acute treatment for at least 60 min;
Respiratory muscle fatigue of patients;
Need for airway safety and patency;
Inability of the patient to control their secretions;
Worsening/altered mental status.
The data about the length of hospital stay and the mortality during hospital stay was was reached the hospital automation information system. Study’s mortality rate is mortality during hospital stay.
Primary outcome
The primary outcome of the study was improvement in vital signs and ABG values within 1 and 4 h of commencement of the treatment. The second outcome was the need for intubation in the ED, length of hospital stay, and in-hospital mortality.
Statistical analysis
The variables were divided into two groups as categorical and continuous. Categorical data were shown as number and percentage, compared with chi-square test. The Kolmogorov–Smirnov test was used to determine whether continuous variables were normally distributed. Continuous variables were shown by mean and standard deviation. Normally distributed continuous variables were compared with the paired-sample T-test, and variables that were not normally distributed were compared with related simple test. Statistics were performed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA) in Windows and p < 0.05 was considered statistically significant.
Results
The final study population included 121 patients, 60 were treated with COT and 61 with HFNCO, whose flowchart is given in Figure 1. Demographic characteristics, comorbidities, complaint on presentation, and presumptive diagnosis in the ED are summarized in Table 1. There was no difference between the groups in the percentages of patients requiring HFNCO or COT in the ED.
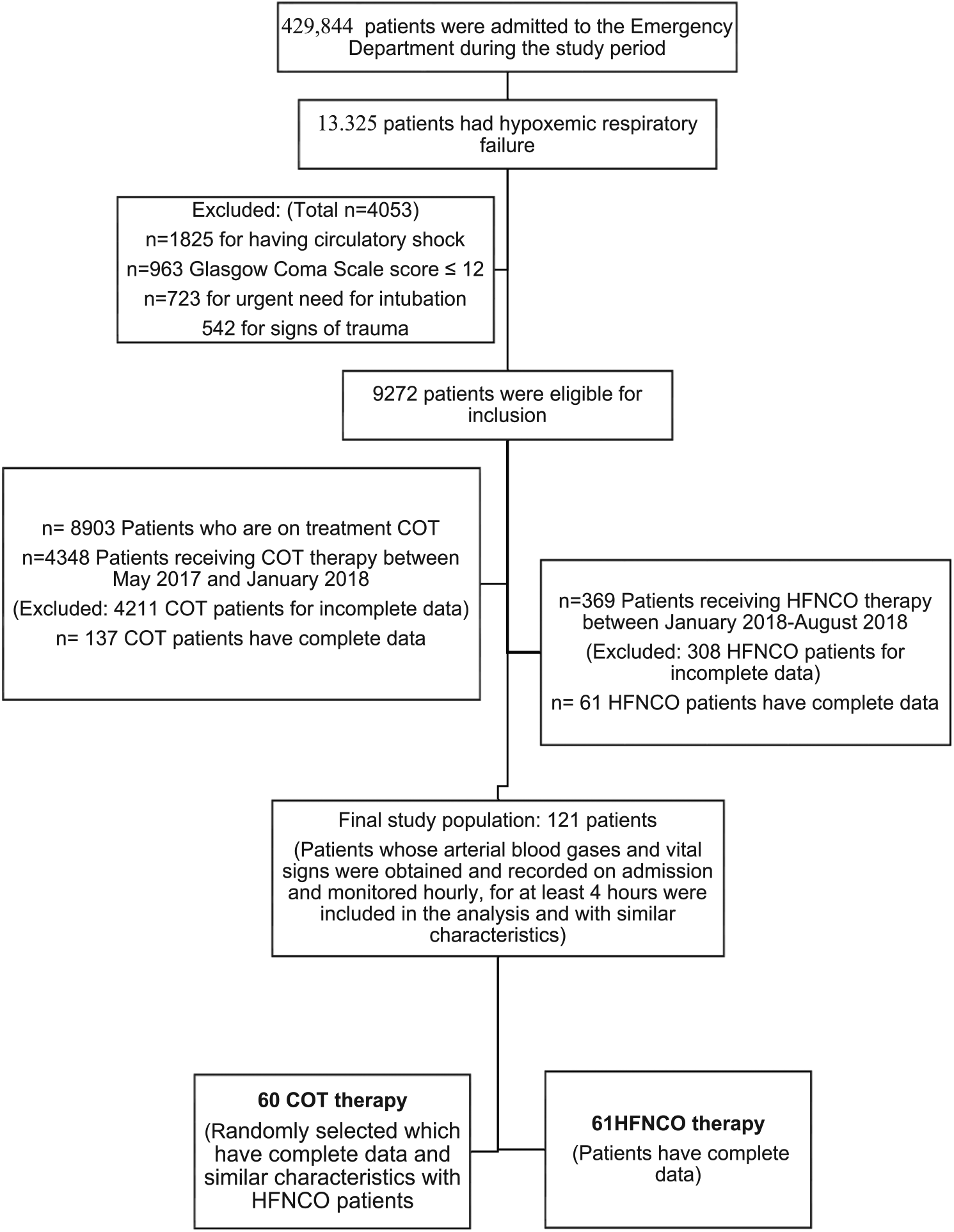
Flow chart of the patients included in the study.
Characteristics of patients in the treatment arms.
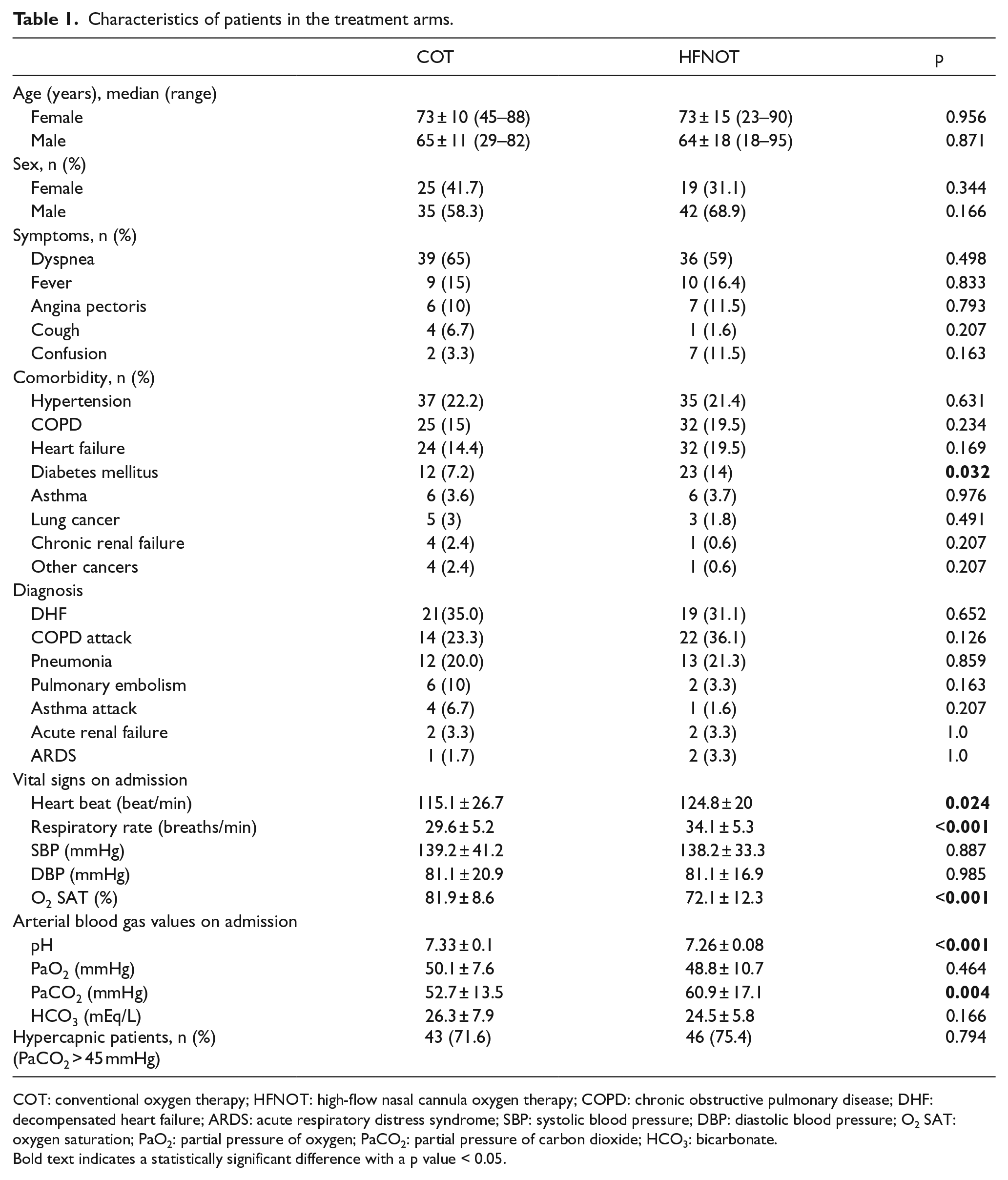
COT: conventional oxygen therapy; HFNOT: high-flow nasal cannula oxygen therapy; COPD: chronic obstructive pulmonary disease; DHF: decompensated heart failure; ARDS: acute respiratory distress syndrome; SBP: systolic blood pressure; DBP: diastolic blood pressure; O2 SAT: oxygen saturation; PaO2: partial pressure of oxygen; PaCO2: partial pressure of carbon dioxide; HCO3: bicarbonate.
Bold text indicates a statistically significant difference with a p value < 0.05.
Changes in the vital signs of the patients with respect to the treatment they received were compared in Table 2. The decrease in the pulse and respiratory rate of HFNCO-treated group was significantly greater than the group treated with COT (p < 0.001) on the first and fourth hours of treatment (Table 2). SaO2 values of patients receiving HFNCO were statistically significantly lower on admission (p < 0.001) (Table 1). Mean SaO2 levels of patients receiving HFNCO treatment was significantly higher than those of patients in the COT group (p = 0.006 at 1 h) and (p < 0.001 at 4 h) (Table 2).
Comparative changes in vital signs and arterial blood gas values in both groups, that is, patients treated with conventional oxygen therapy and high–flow nasal cannula during the first 4 h of treatment.
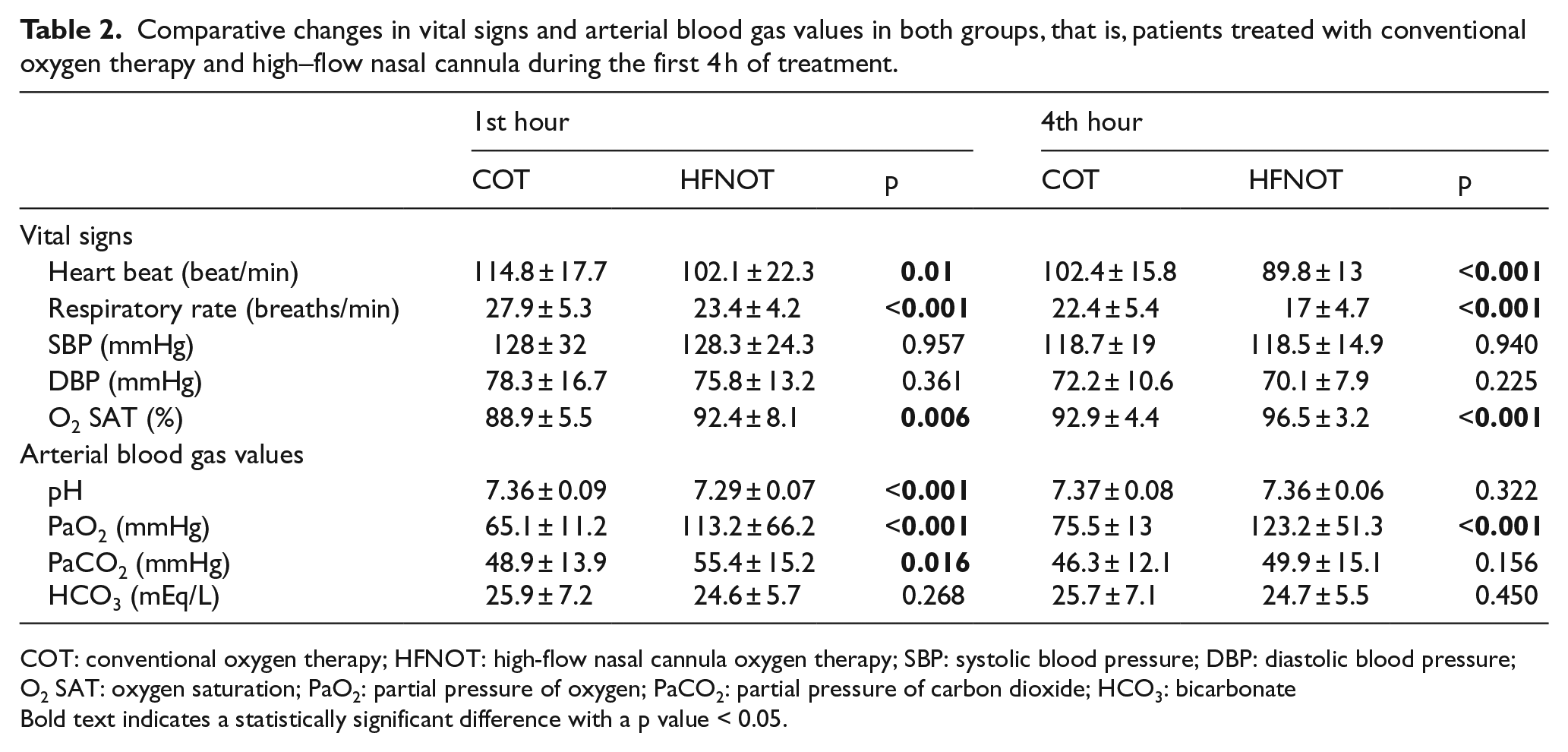
COT: conventional oxygen therapy; HFNOT: high-flow nasal cannula oxygen therapy; SBP: systolic blood pressure; DBP: diastolic blood pressure; O2 SAT: oxygen saturation; PaO2: partial pressure of oxygen; PaCO2: partial pressure of carbon dioxide; HCO3: bicarbonate
Bold text indicates a statistically significant difference with a p value < 0.05.
Patients with hypoxemia and PaCO2 > 45 mmHg were evaluated as hypoxemic-hypercapnic respiratory failure. Of the patients who received COT, 44 (73.3%) were hypercapnic patients, while 46 (75.4%) patients receiving HFNCO were hypercapnic. There was no statistically significant difference between the number of hypercapnic patients in the HFNCO and COT groups (χ2 = 0.068, p = 0.794) (Table 1).
Table 1 shows the statistically significant variables. Regression analysis with statistically significant variables (respiration rate, pulse rate, O2 saturation, pH, PCO2), pH (odds ratio (OR): 0.482, 95% confidence interval (CI) = 0.291–0.796, p = 0.004), and O2 saturation (OR: 0.932, 95% CI = 0.891–0.975, p = 0.002) were determined as independent predictors for the HFNCO group.
Each unit increase in respiratory rate increases the probability of being in the HFNCO group by 15.1%. Each 0.1 unit increase in pH decreases the probability of being in the HFNCO group by 51.8%. Every 1 unit increase in saturation reduces the likelihood of being in the HFNCO group by 6.8%.
Changes in the vital signs of the hypercapnic patients in accordance with the treatment they received are shown in Table 3. Heart rate (p = 0.01), respiratory rate (p < 0.001), and oxygen saturation values (p < 0.001) of patients receiving HFNCO were statistically significantly lower than those of COT group on admission. The reduction of the mean pulse and respiratory rates of HFNCO-treated group were statistically significant when compared to COT group on the first and fourth hours of treatment (p < 0.001 for both). Mean SaO2 level of patients receiving HFNCO treatment was higher than the SaO2 level of patients in the COT group and the difference was statistically significant at 1 h (p = 0.031) and 4 h (p < 0.001).
Comparative changes in vital signs and arterial blood gas values in the hypercapnic patients in both groups, that is, patients treated with conventional oxygen therapy and high–flow nasal cannula during the first 4 h of treatment.
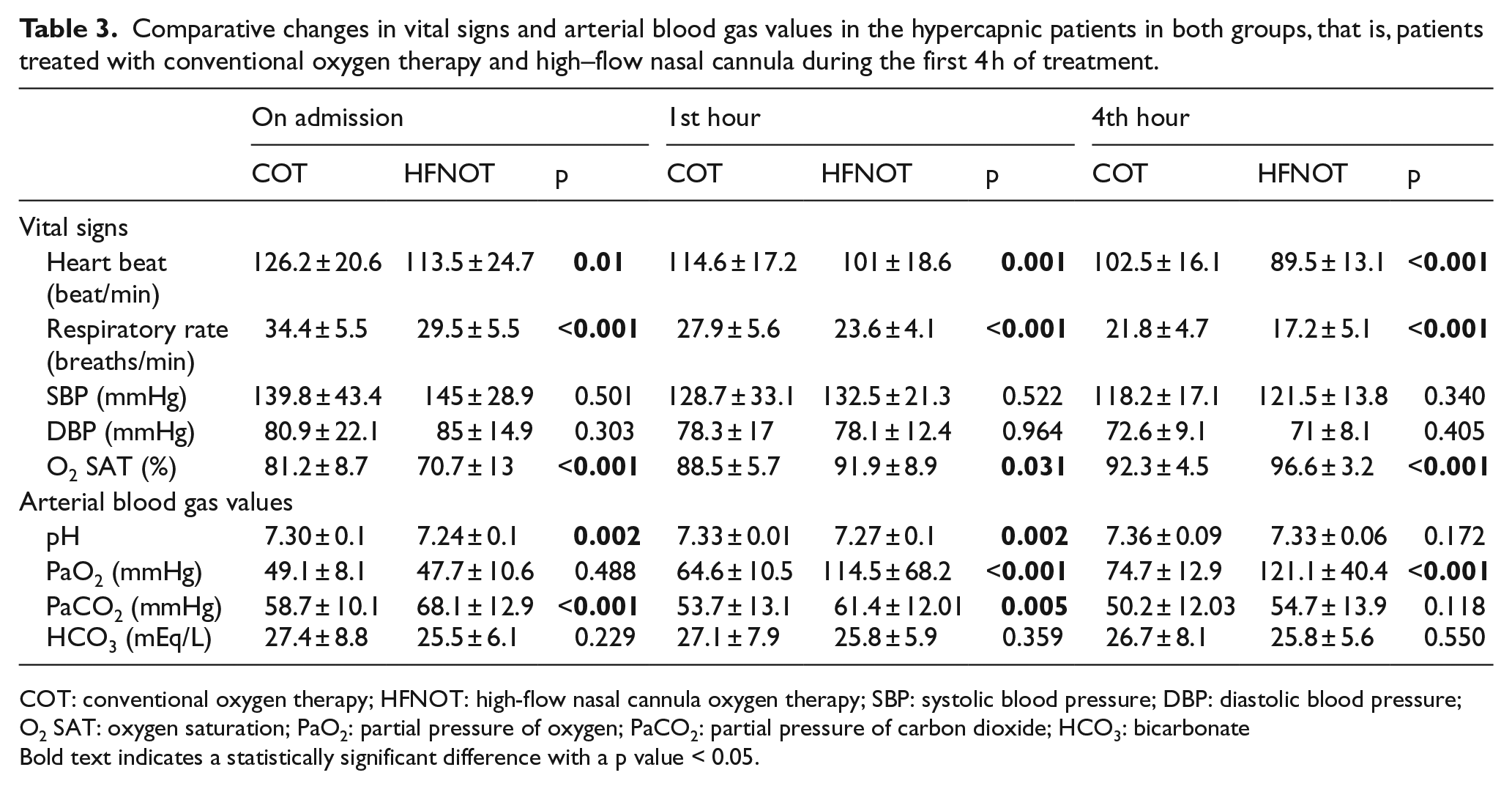
COT: conventional oxygen therapy; HFNOT: high-flow nasal cannula oxygen therapy; SBP: systolic blood pressure; DBP: diastolic blood pressure; O2 SAT: oxygen saturation; PaO2: partial pressure of oxygen; PaCO2: partial pressure of carbon dioxide; HCO3: bicarbonate
Bold text indicates a statistically significant difference with a p value < 0.05.
Table 4 depicts the changes in vital signs of hypercapnic patients receiving HFNCO therapy within hours. Within hours, the decrease in pulse, respiratory rate, and blood pressure and increase in oxygen saturation were found to be statistically significant (p < 0.001).
Changes in vital signs and arterial blood gas values of hypercapnic patients receiving high–flow nasal cannula oxygen therapy during first 4 h of treatment.
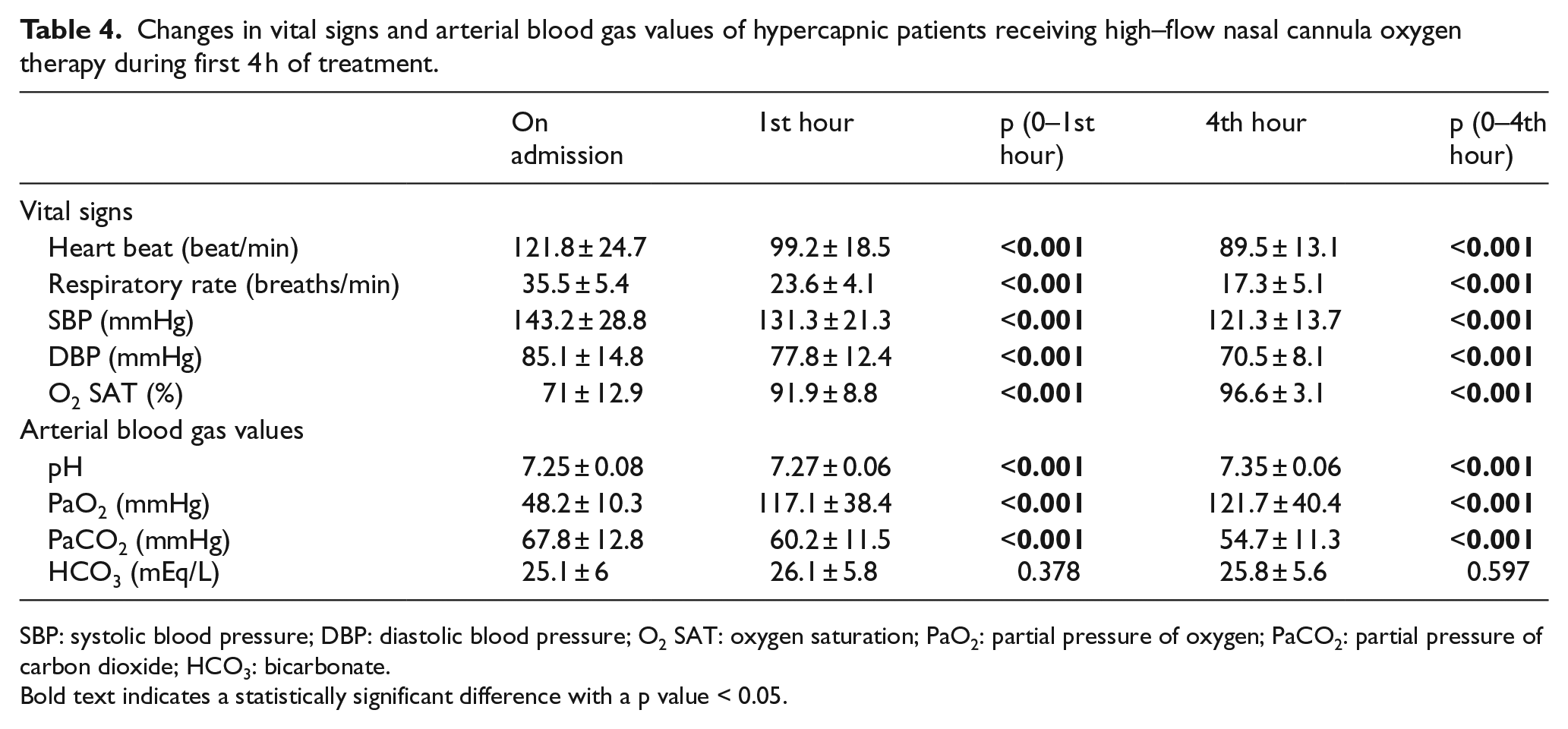
SBP: systolic blood pressure; DBP: diastolic blood pressure; O2 SAT: oxygen saturation; PaO2: partial pressure of oxygen; PaCO2: partial pressure of carbon dioxide; HCO3: bicarbonate.
Bold text indicates a statistically significant difference with a p value < 0.05.
The comparative changes in ABG values based on the treatment of all patients are demonstrated in Table 2. The pH value was statistically significantly lower in the HFNCO group on presentation (p < 0.001) and at the first hour (p < 0.001) as compared to COT group. The pH values of the patients who received HFNCO at the fourth hour of the treatment were increased, although not statistically significant (p = 0,322). There was no statistically significant difference between PaO2 values on admission (p = 0.464). PaO2 values were significantly higher in the HFNCO group at the first and fourth hours of treatment (p < 0.001 for both). PaCO2 value was statistically significantly higher in the HFNCO-treated group on admission (p = 0.004) and at the first hour of treatment (p = 0.016). Mean PaCO2 value of patients receiving HFNCO treatment was lower at the fourth hour of treatment, although not statistically significant (p = 0.156). There was no statistically significant difference in HCO3 values between the two groups at the time of presentation (p = 0.166), at the first hour (p = 0.268), or at the fourth hour (p = 0.450).
The comparative changes in ABG based on the treatment of hypercapnic patients are shown in Table 3. On admission and at first hour, the pH value was statistically significantly lower in the HFNCO group (p = 0.002). The pH values of the patients who received HFNCO treatment at the fourth hour of the treatment were increased, although not statistically significant (p = 0.172). There was no statistically significant difference between PaO2 values on admission (p = 0.488). PaO2 values were significantly higher in the HFNCO group at the first and fourth hours of treatment (p ⩽ 0.001). PaCO2 value was statistically significantly higher in the HFNCO-treated group on admission (p < 0.001) and at the first hour of treatment, when compared to COT group (p = 0.005). PaCO2 value of patients receiving HFNCO treatment at the fourth hour of treatment decreased and there was no statistically significant difference between PaCO2 values of both treatment groups (p = 0.118). There was no statistically significant difference in HCO3 values between the two groups at the time of presentation (p = 0.229), at the first hour (p = 0.359), or at the fourth hour (p = 0.550).
The changes in the ABG of the hypercapnic patients receiving HFNCO treatment within hours are delineated in Table 4. The decrease in PaCO2 and increase in pH and PaO2 values were found to be significantly greater in HFNCO group, when compared to COT group within hours (p < 0.001 for all three comparisons). There was no statistically significant difference in HCO3 values at the first hour (p = 0.378) and fourth hour (p = 0.597) between the groups.
Of the 60 patients who received COT, 75% (n = 45) were admitted to intensive care and 25% (n = 15) to the ward. Of the 61 patients who received HFNCO treatment, 80.3% (n = 49) were admitted to the ICU and 11.5% (n = 7) to the ward. None of the patients who had received COT treatment was successfully discharged from the ED, while five (8.2%) patients from the HFNCO-treated group did (p < 0.001).
No statistically significant difference was found with regard to the need for intensive care admissions for both treatment arms (p = 0.485). The mean duration of hospitalization in 60 patients with COT treatment was 9.6 ± 8.2 days (range, 1–44 days). The mean duration of hospitalization in 56 patients with HFNCO treatment was 13.7 ± 19 days (range, 2–119 days). The difference between the mean number of days of hospitalization was not statistically significant (p = 0.127).
In the ED, 11 patients (18.3%) receiving COT treatment and 6 patients (9.8%) receiving HFNCO treatment required endotracheal intubation. The difference between the groups regarding the need for IMV was not statistically significant (p = 0.179).
Among all, six patients undergoing HFNCO treatment warranted intubation. Their chief complaints were shortness of breath (n = 4) and chest pain (n = 2). All six patients had PaO2 < 50 mmHg, PaCO2 > 55 mmHg, and pH < 7.20. Four patients were intubated in the first hour of treatment. Final diagnoses comprised acute exacerbation of COPD in four, decompensated heart failure in one, and pneumonia in one. Mean length of stay in hospital was 30 days. One of the patients died during the hospital course.
Five patients (8.3%) who received COT and another five (8.2%) among the HFNCO group died in the ICU (mean length of stay: 14.6 ± 11.4 days and 36 ± 46.7 days, respectively). No patients died in the ED.
Potential side effects of HFNCO treatment, such as pneumothorax, arrhythmia, epistaxis, and wounds in the nose, were not seen in any of the cases in this study.
Discussion
In this study, a comparison of patients who received HFNCO treatment with patients who received COT, who presented to the ED with hypoxemic ARF, was undertaken. HFNCO treatment was associated with a significant reduction of PaCO2, respiration rate, and heart rates while PaO2, pH, and SpO2 increased in the same group. There was no statistically significant difference between the length of hospital stay, endotracheal intubation needs, and mortality rate.
HFNCO treatment was shown to decrease respiratory and heart rate and increase oxygen saturation.4,8 It is possible to facilitate the mucociliary transport and reduce the viscosity of the secretions in the airway by feature of humidified oxygen in the treatment of HFNCO. By high rate of oxygen flow administered, the anatomical dead spaces of the upper airway are washed and CO2 is replaced by oxygen. Likewise, improved oxygenation augmented the end-expiratory lung volume, alleviated the respiratory workload, decreased fatigue in the respiratory muscles, and thus corrected hypoxemia and hypercarbia. 9 Better tolerability of the nasal cannula compared to oxygen masks, high FiO2, PEEP effect, dead space wash-out, and the physiological effects of HFNCO result in reduced respiratory workload and hence decreased respiratory rate and heart rate, and increased oxygenation. 10
Patients with ARF often have increased respiratory demand and oxygen demand and have a high inspiratory flow rate. It has been reported that dry and cold air given to the nasal cavity cause bronchoconstriction with vagal maneuver in COPD patients, smokers and nonsmokers, and also decrease lung compliance.11,12 Humidified and heated oxygen in the treatment of HFNCO reverses this effect and thus result in bronchodilatation, together with loosening of bronchial smooth muscles, increase in airflow, decrease in air trapping due to decreased functional residual capacity, hyperinflation, and respiratory workload, and an increase in inspiratory capacity. High oxygen flow rate with HFNCO reduces inspiratory airway resistance by providing nasopharyngeal flow rates that exceed the patients’ inspiratory demands. 13 This high inspiratory flow rate causes an increase in oxygenation and tidal volume and a decrease in respiratory workload and respiratory rate.14,15 Due to the high flow rate, the washing effect removes CO2 from the potential dead space in the pharynx and allows a greater part of the lung to be incorporated into the gas exchange. This reduces blood CO2 levels quickly. 16 In a study in which the effect of HFNCO treatment on the PaCO2 level in patients with hypercapnic ARF was investigated, ABG was evaluated at 1st and 24th hours. Significant improvement in hypercapnia was observed during the course of treatment, but the statistical significance was not observed at the 24th hour (p = 0.062) but only at 1 h after initiation of HFNCO (p = 0.006). 17 In this study, the decrease in the mean PCO2 value of ABG in the hypercapnic patients treated with HFNCO at the 1st and the 4th hour was significant. In addition to PCO2 values of hypercapnic patients, increase in pH values and pO2 values and improvement in vital signs were significant. In a study, the intrinsic PEEP caused by extrinsic PEEP induced by HFNCO treatment in severe COPD patients is claimed to be as effective as NIMV in decreasing pCO2 level. 18 It can be postulated that all of these mechanisms are effective in the correction of hypoxia and hypercapnia in patients receiving HFNCO therapy.
Patients presenting with ARF to the ED may need NIMV or IMV. Patients in need of these treatment modalities are generally exposed to long periods of stay in EDs because of the scarcity of beds in ICUs and in certain periods where bed numbers are limited due to epidemics or other diseases overcrowding the EDs. NIMV is more claustrophobic due to the face-covering mask compared to HFNCO treatment and it is more difficult to tolerate. It also causes pressure wounds on the face and nose and does not allow simple daily life activities such as talking and eating. IMV is a difficult treatment in the ED because of the need for sedo-analgesia, cumbersome nursing care, and need for intensive care follow-up. Iatrogenic barotrauma, risk of aspiration, hospital infections, and ventilator-associated pneumonia caused by NIMV and IMV constitute other important risks of these treatments. 19 In this study, there was no statistically significant difference in need for mechanical ventilation in the groups receiving HFNCO and COT. A study by Nagata et al. showed that HFNCO treatment significantly reduced the need for IMV and NIMV in patients with ARF. 20 A controlled randomized study demonstrated no statistically significant difference in need for mechanical ventilation in the groups receiving HFNCO and COT. 19 In a meta-analysis comparing NIMV, SOT, and HFNCO, HFNCO decreased the need for endotracheal intubation similar to NIMV and greatly decreased the need for endotracheal intubation compared to SOT. 21 This situation can be explained by many different mechanisms. The first one is that the oxygen given by the continuous high current increases the tidal volume and improves the inspiratory flow dynamics, thus providing minute ventilation and oxygen saturation. In addition, it provides thoracoabdominal synchronization by central and reflex mechanism, decreasing the number of breaths and decreasing the respiratory workload. Second, with the rapid washing effect in the potential dead space, it allows to decrease CO2 level, to sustain high levels of oxygen inhalation and to increase the alveolar gas exchange. The PEEP effect (2–5 cm H2O) reduces airway collapse and helps to recruit in atelectatic alveolar areas and allows these areas to participate in gas exchange.21,22 All these mechanisms in patients receiving HFNCO may have resulted in the improvement in ABG and vital signs and this, in turn, may have reduced the need for IMV. However, the small size of the sample limits the reliability and generalizability of the findings. Further studies are needed to conclusively demonstrate the efficacy of HFNCO.
In this study, there was no statistically significant difference in the length of hospital stay and mortality between HFNCO treatment and COT. In two different meta-analyses comparing NIMV, COT, and HFNCO, no statistically significant difference was observed between the number of hospitalization days of all three treatment modalities.21,22 While in the meta-analysis of 3881 patients, there was no statistically significant difference in mortality, 21 in the meta-analysis of 1084 patients, it was found that HFNCO could reduce both intubation and mortality. 22 In a study comparing NIMV, COT, and HFNCO in patients with ARF without hypercapnia, the low mortality rate in HFNCO patients was thought to decrease the need for intubation in patients with severe hypoxemia and reduce mortality by preventing the complications of intubation. 23 In this study, the lack of difference in mortality between HFNCO treatment and COT may be attributed to the poor vital signs on presentation and with the remarkably unfavorable ABG values in patients who received HFNCO treatment.
In this study, no COT-treated patients could be discharged from the ED. Five patients receiving HFNCO therapy were discharged from the ED due to improvement of their respiratory insufficiency. This difference was statistically significant. HFNCO treatment requires less intensive care support than other mechanical ventilation treatments and can be adopted in the ED care as well as other inpatient care. It can be postulated that with the initiation of HFNCO treatment—unless the patient has any contraindications on presentation to the ED with ARF—there will be shorter ED stays, ED and hospital resources will be utilized more cost-effectively, and beds in the ICUs and wards will not be occupied unnecessarily.
Limitations
Our study was a retrospective study. Therefore, we were not able to access all the data. This was the most significant limitation of the study and most significant factor because of not fully accessing the data of all patients. The study included the patients who were admitted to the ED with hypoxemic respiratory failure and whose blood gas and vital signs were monitored hourly and recorded in the critical care unit and all data were accessible. So only 61 patients with fully accessible and recorded complete data (vital signs and hourly blood gas analysis, etc.) of the 369 patients receiving HFNCO treatment between 1 January 2018 and 1 August 2018 included in the study. We randomly selected the COT group. In our data set, we did not record the patients who did not follow up regularly and whose data could not be reached. Therefore, we were not able to do the analysis of the missing data.
Data regarding the duration of treatment with HFNCO after the patients had been admitted to the ward could not be reached. Awareness of this fact would also be useful to identify the impact of HFNCO treatment on the length of hospital stay and mortality. Since the changes in vital signs and ABG in hypoxemic and hypercapnic patients who underwent treatment with HFNCO are significant, broader population-based studies can give robust data regarding mortality and length of stay in hospital.
Conclusion
HFNCO treatment has contributed to positive results from the first hours of treatment in vital signs and ABG values. The present findings suggest that HFNCO might be a first-line therapy for patients admitted to the ED with ARF. However, generalizing this finding to hypercapnic hypoxemic ARF would be premature. Further studies are needed to conclusively demonstrate the efficacy of HFNCO.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data and materials are reachable from hospital automation information systems.
Informed consent
Written informed consent was not necessary because no patient data has been included in the manuscript.
Ethical approval
The ethics committee of the Cukurova University Medical Faculty Hospital approved the study.
Human rights
This manuscript was carried out in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines.