
Abstract
Background:
The video-optical intubation stylet (VS) is a slim, rigid but flexible intubating device that aids physicians to intubate patients, particularly with difficult airways.
Objectives:
The objective of this study was to compare the performance of emergency department doctors in using different intubating devices for intubation in an airway manikin simulating different difficult airway scenarios.
Methods:
Thirty emergency department doctors were recruited in a pilot study. Their performance of using traditional Macintosh laryngoscope, GlideScope®, Airtraq® and C-MAC® Video Stylet were compared in three situations: normal, restricted cervical motion and limited oral aperture. The time for intubation, first attempt success rate, failure rate, dental injury and the subjective ease of different devices by the participants were compared.
Result:
The mean intubation time by VS in each scenario was significantly shorter compared with other devices (Normal: 19.77s vs 24.67–28.19s, p = 0.014; Cervical restriction: 20.85 vs 26.17–31.26s, p = 0.008; Limited oral aperture:19.03 vs 29.35, p = 0.001). However, there was no significant difference in failure rate or first attempt success rate. The incidence of dental injury was significantly lower with VS than other laryngoscopes (p = 0.001, p < 0.05 and p < 0.05 in normal, cervical restriction and limited oral aperture scenarios, respectively). Moreover, participants appreciated that VS was the easiest device to intubate in each scenario. (p < 0.05 in all scenarios)
Conclusion:
The performance of VS was comparable to or even better than the commonly used laryngoscopes in the emergency department in airway management. When adequate training is provided, VS can be a potentially good alternative for tracheal intubation in different situations.
Keywords
Introduction
Endotracheal intubation (ETI) is a bread-and-butter skill of emergency physicians to safeguard our patients’ lives. However, encountering difficult airways is not uncommon and it poses a huge challenge and stress to us, even for well-trained and experienced emergency physicians. In recent decades, numerous airway gadgets were invented to help tackle these undesirable situations, for example, GlideScope®(GS), Airtraq®(AQ) and C-MAC®. These gadgets not only provide optimal views for endotracheal intubation, but also reduce the risk of air and droplet-borne disease transmission during intubations, especially during the COVID pandemic.
Doctors in Hong Kong are advanced to have pioneering equipment in aid of their practices. Nearly every emergency department (ED) in Hong Kong is equipped with at least 1–2 video laryngoscopes, according to our informal survey to other EDs, in addition to the conventional direct laryngoscopes (DL). AQ, GS and C-MAC® are usually ready for use in our local ED. On the other hand, video-optical intubation stylet (VS) is used in other countries in managing various difficult airway situations while it is not widely used in local EDs. Therefore, we conducted this study to evaluate the performance of VS.
Video stylet is a non-disposable rigid stylet with flexible distal end incorporated with camera chip and light source that allows clinicians to obtain a direct camera view from the tip of the endotracheal tube (ETT) during ETI. It has several advantages over other video laryngoscopes, including the following: (1) Its view reflects the direct site of tracheal tube placement; (2) its slim profile is useful in patients with limited mouth opening or oropharyngeal obstruction; (3) its rigidity improves manoeuvrability, especially in conjunction with a laryngoscope blade and allows accommodation through soft tissue obstruction; (4) its flexible distal end enhances better view and minimizes gross movement while adjusting the orientation; (5) it has better endoscopic orientation than flexible fiberoptic laryngoscopes; 1 (6) it can provide oxygen during intubation via the supply from side port; (7) there are studies suggesting the learning curves are comparable to other video laryngoscopes.2,3 As a result, VS is especially helpful in difficult airway intubation including patients with cervical spine immobilization, space-occupying processes in the mouth and restricted jaw opening or trismus. North Lantau Hospital is a regional hospital located on an outlying island in Hong Kong; it is relatively remote from the city and without on-site anaesthesiology or intensive care service. Therefore, our emergency department has recently introduced VS, branded C-MAC® Video Stylet, into our daily practice to aid in tackling difficult airways.
Methods
This was an experimental manikin study. The performances of our department doctors in using DL, GS, AQ and VS to intubate in different situations were evaluated and compared. All the doctors had at least 2 years of clinical experience with exposure to conventional and video laryngoscopes in the emergency department.
Pre-experiment preparation
Standardized training was offered to all doctors before participating in the study. The training session includes a lecture with a video presentation explaining the use of VS, followed by hands-on practice. The training time was 2 h in total, 1 h for the presentation and 1 h for the hands-on. Immediate constructive feedback was provided by the investigators during the training.
Experiment setting
After completing the training session, each participant was randomly assigned to a sequence of ETI in three scenarios using DL, GS, AQ and VS, 12 combinations in total.
There were three intubating scenarios: (1) normal, (2) restricted cervical motion and (3) limited oral aperture. We used standardized and objective measures to simulate difficult airways in the manikin. For simulating patients with cervical injury on neck collar, that is, restricted cervical motion, we used Stifneck® Select™ Collars set at the same size and adjustment. To simulate limited oral aperture, the inter-incisor distance was set as 3 cm in the manikin, after reference to previous studies4,5 which suggested that less than or equal to 3–4 cm could be regarded as difficult airway. To fix the manikin jaw movement and set the inter-incisor distance at 3 cm, we used a strong tying system wrapping around the manikin’s head and mandible. Forceful displacement of the jaw in the manikin was expected and a study showed the maximum force during difficult intubation with DL, C-MAC and Airway scope (similar to Airtraq) would be 80 N. 6 Hence, we set 100 N as the limit and our tying system would be strong enough to resist a force of 100 N, which was tested and quantified by a force metre. All the ETI were performed by using a 7.5-mm cuffed endotracheal tube (Figure 1).
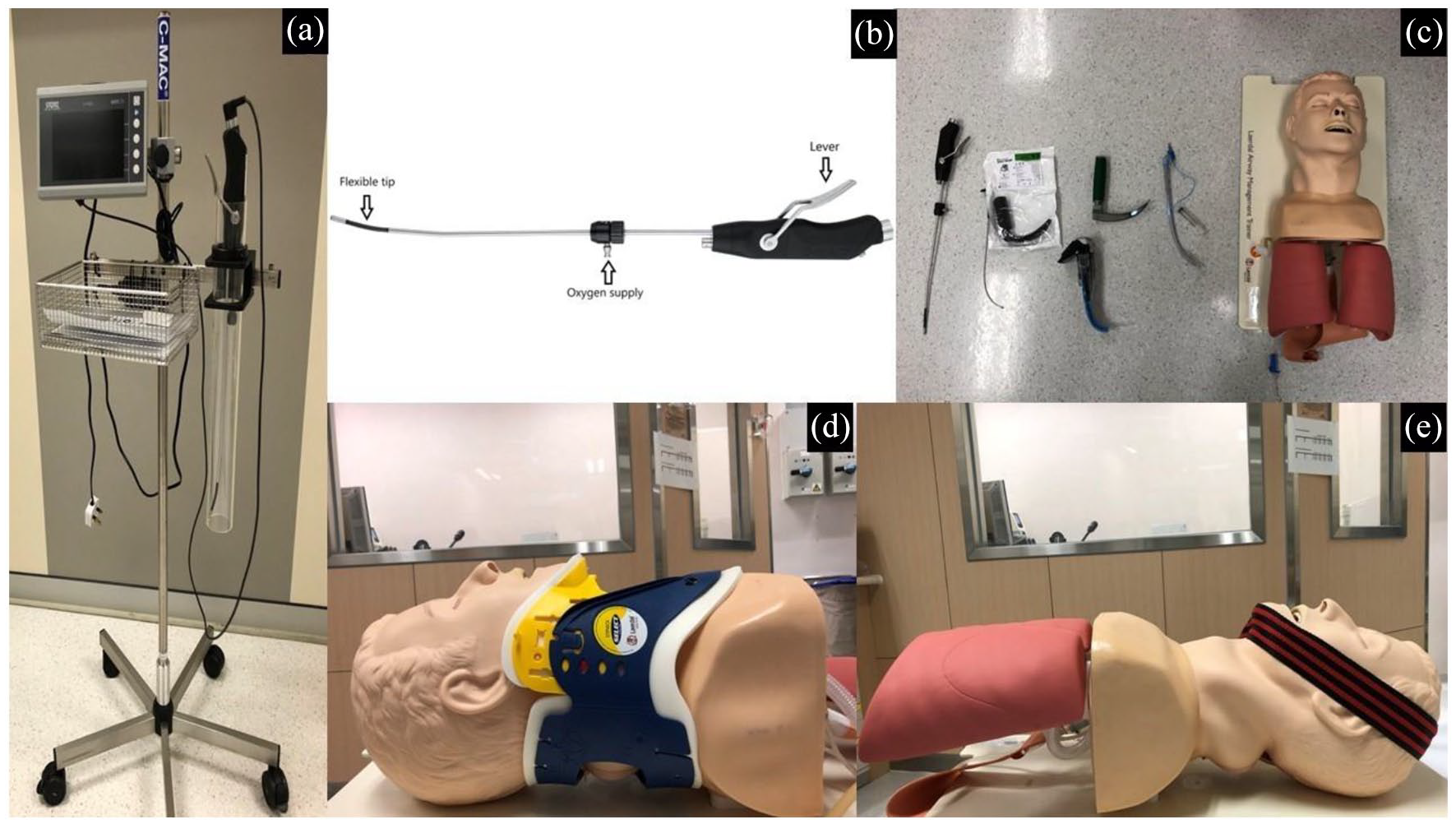
The equipment and settings.
There are two main approaches to intubate with video stylet: (1) the midline approach and (2) the retromolar approach.
In the midline approach, we simply insert the VS into the patient’s mouth along the oral axis. Once the tip of VS arrives at the pharynx, the lever is pulled and the flexible tip of VS is bent until the vocal cord is seen and centralized. Then the endotracheal tube (ETT) is pushed downwards, and the passage of ETT can be directly visualized (Figure 2).
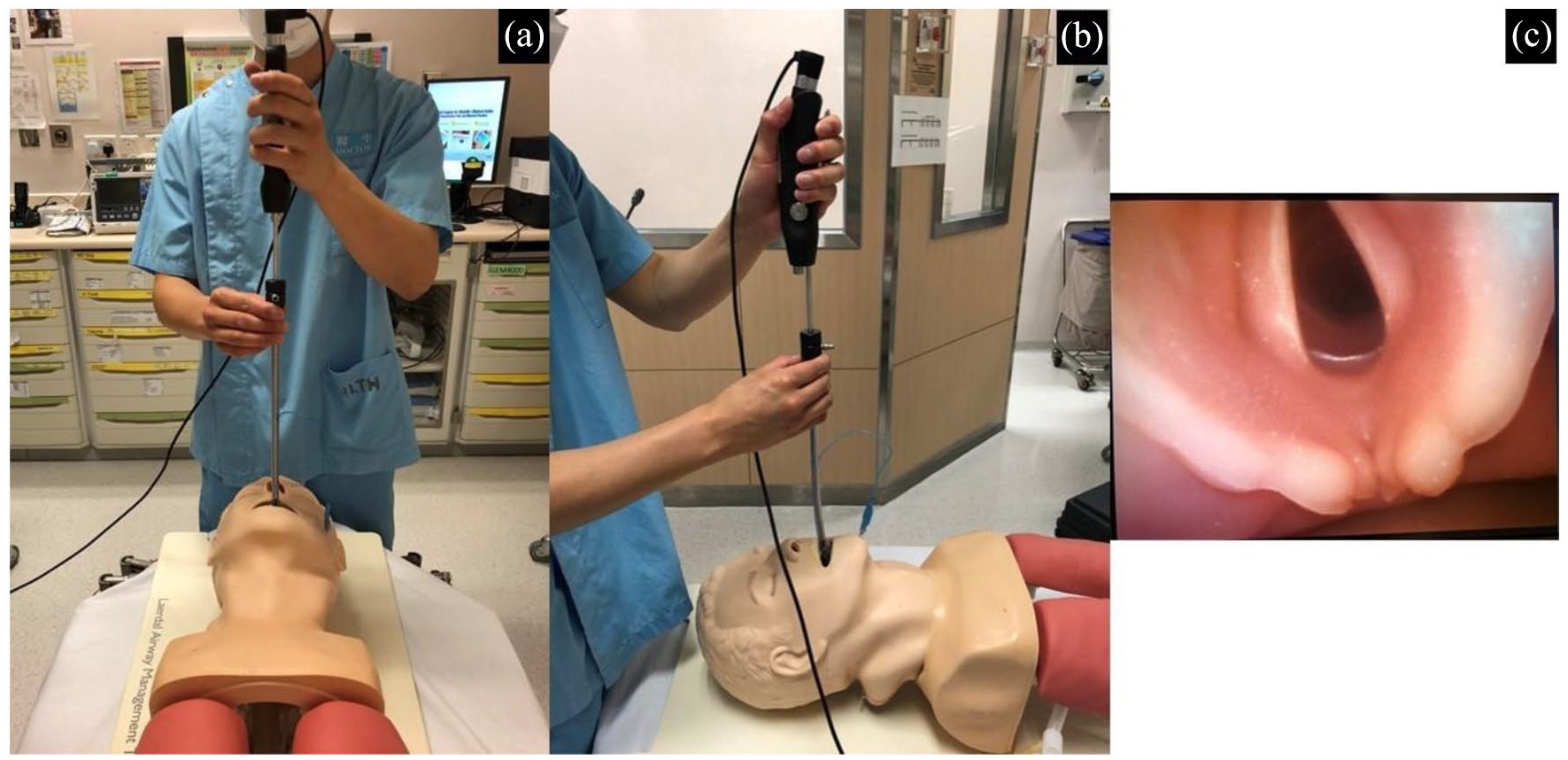
Midline approach of video stylet.
The retromolar approach is mainly used for difficult airways with oral obstruction, for example, edematous tongue, large intra-oral tumour, unremovable foreign body or extreme limited oral aperture in significant facial injury or post-radiation trismus. It is useful when the midline approach is not feasible due to obstruction. VS can be inserted on the left or right side in the retromolar approach, depending on the site of obstruction. For the left-side approach, VS is first turned towards the left, and then it is inserted through the left angle of mouth running between the teeth and buccal mucosa. Once the retromolar space is reached, that is, posterior to the last molar teeth, a 90-degree anti-clockwise turn is made, and theoretically the vocal cord is immediately seen and ETT can be inserted. The right-side approach is the other way round (Figure 3).
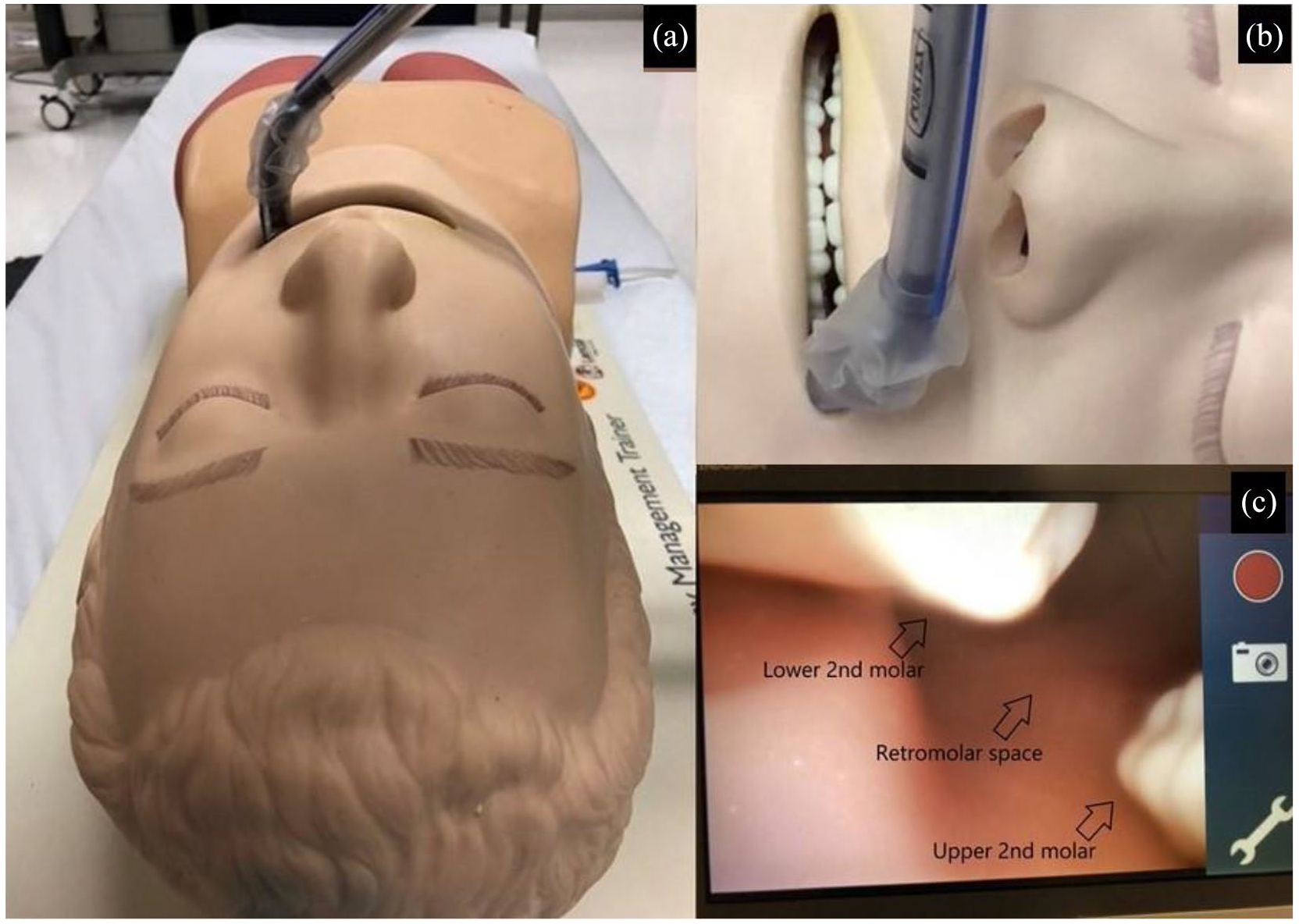
Retromolar approach of video stylet.
Outcome
The primary outcomes were the time for intubation, failure rate, first attempt success rate and dental injury. The failure to intubate within 120 s was regarded as a failed attempt and more than three attempts were regarded as a failed ETI. The time required for a successful ETI was defined as the time (in seconds) from picking up the laryngoscope to ETT position confirmation by bagging the artificial lungs. An intubation attempt was described as a withdrawal of the intubating device from the mouth followed by repositioning. Dental injury was evaluated by the presence of ‘clicks’ when excessive pressure is acted on the upper incisors.
The secondary outcome was the participant’s subjective ease of ETI with different devices, which was evaluated on a Likert-type scale from 1 to 5 at the end of the study. Other open comments were also collected and reviewed.
Data analysis
The Statistical Package for Social Sciences (SPSS) version 20.0 for Windows was used for analysis. The performance of the participants using different intubating devices under different situations mentioned above was investigated. The time for ETI was compared using one-way analysis of variance (ANOVA), and Tukey’s method was used for post hoc multiple comparisons. The first attempt success rate and the failure rate were analysed using chi-square test. The dental injury was evaluated by chi-square test. The subjective ease of ETI was analysed by Kruskal–Wallis test with Bonferroni correction of p-value, and the result was shown in a bar chart (Figure 4). For all statistical analyses, a p-value of less than 0.05 was considered to be statistically significant.
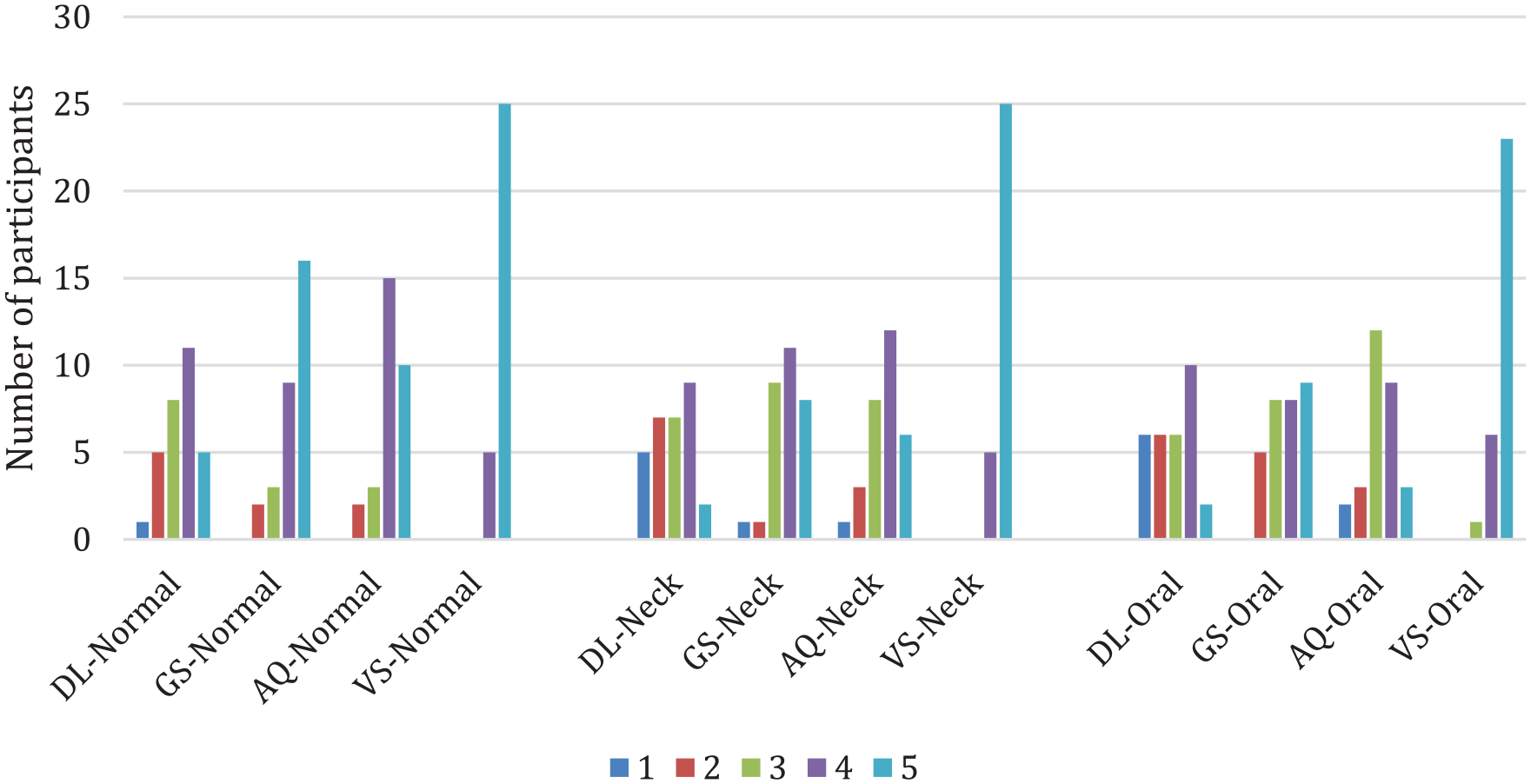
Bar chart of participant’s subjective ease.
Since there was no previous study comparing video stylet and other intubating devices under different situations in the Emergency Medicine specialty, we performed a pilot study to evaluate the performance of video stylet in an experimental setting (Table 1). A convenient sample of 30 ED doctors was recruited. The result of this pilot study could help further evaluation of the video stylet in different settings.
Baseline characteristics of the participant doctors (n = 30).
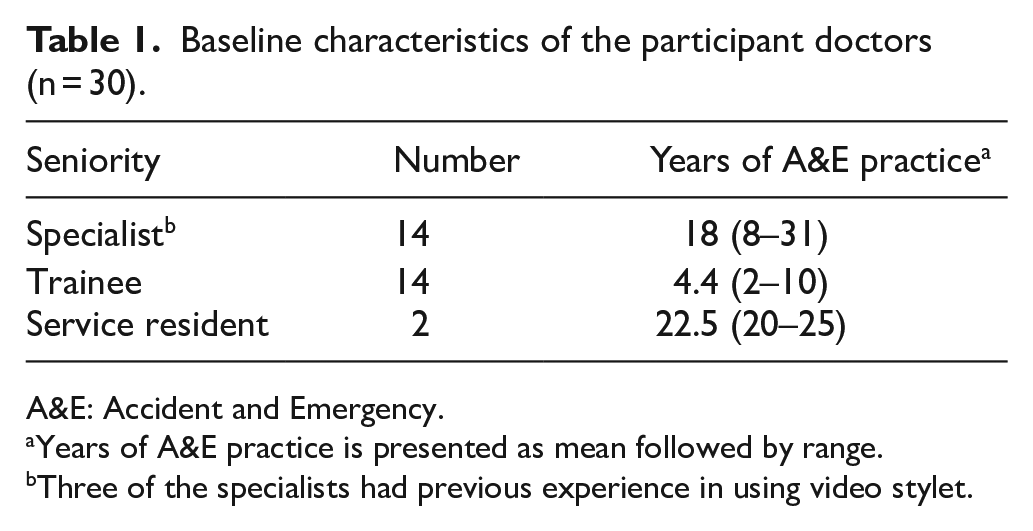
A&E: Accident and Emergency.
Years of A&E practice is presented as mean followed by range.
Three of the specialists had previous experience in using video stylet.
Results
Comparison of ETI failure rate
The success rates of ETI in different scenarios with different intubating methods were generally good and nearly none of the participants failed to intubate, although some required more than 1 attempt. There was no significant difference among the devices in failure rate (Table 2).
Analysis of the failure rate and first attempt success rate of ETI by different devices.
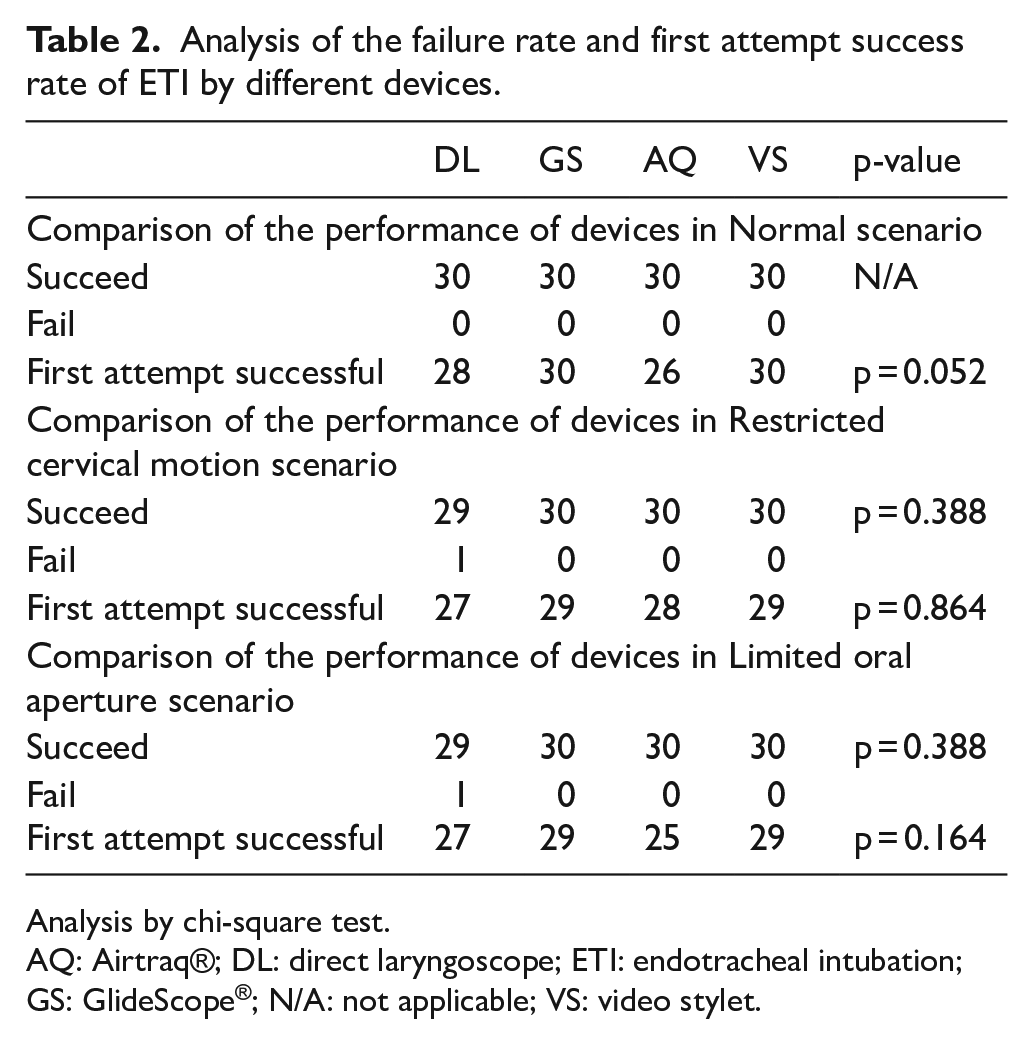
Analysis by chi-square test.
AQ: Airtraq®; DL: direct laryngoscope; ETI: endotracheal intubation; GS: GlideScope®; N/A: not applicable; VS: video stylet.
Comparison of the first attempt success rate
The first attempt success rates of the four intubating devices in three situations were similar. Intubation with video stylet had the least number of attempts in different scenarios, but the difference between all the devices was not statistically significant (Table 2).
Comparison of the intubation time
When using video stylet, the mean intubation time was lowest compared with other equipment in all three scenarios. The result was most remarkable and significant in the group of restricted oral aperture. It had the lowest mean intubation time compared with other devices (mean intubation time: 19.03; vs DL: 28.33s, p = 0.009; vs GS: 28.88s, p = 0.005; vs AQ = 29.35, p = 0.003). While in the other situations, video stylet also had a significantly shorter mean intubation time compared with certain methods (Normal: vs DL: p = 0.025 and vs GS: p = 0.025; Restricted cervical motion: vs GS: p = 0.004) (Table 3).
Analysis of intubation time by different devices in different scenarios.
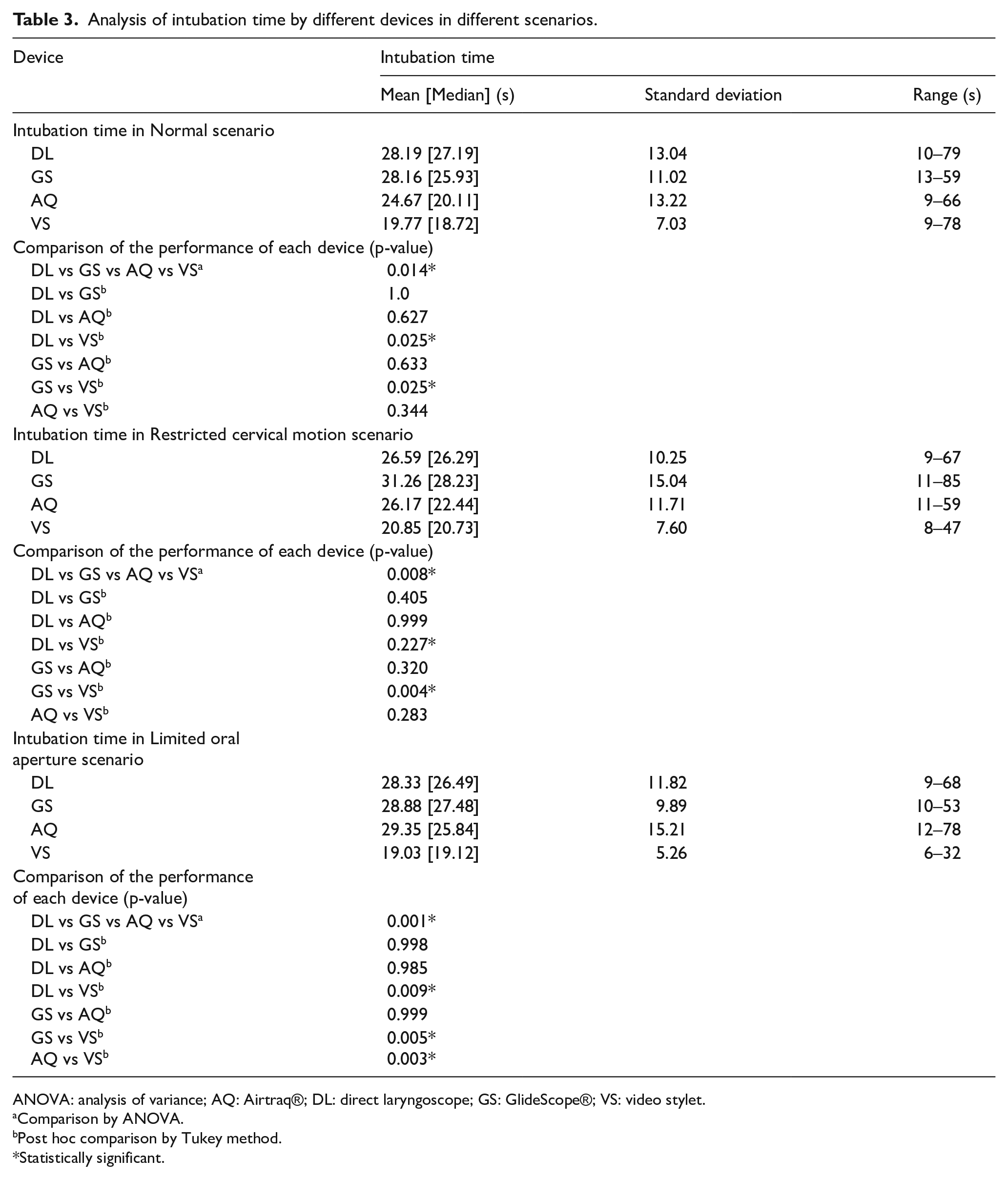
ANOVA: analysis of variance; AQ: Airtraq®; DL: direct laryngoscope; GS: GlideScope®; VS: video stylet.
Comparison by ANOVA.
Post hoc comparison by Tukey method.
Statistically significant.
Comparison of dental injury
In general, intubation with video stylet performed well in the aspect of dental injury. It was statistically significant that there were fewer attempts that would damage the manikin’s teeth compared with other devices in all scenarios (Normal: p = 0.001; Restricted cervical motion: p < 0.05; Limited oral aperture: p < 0.05) (Table 4).
Analysis of the dental injury by using different devices.
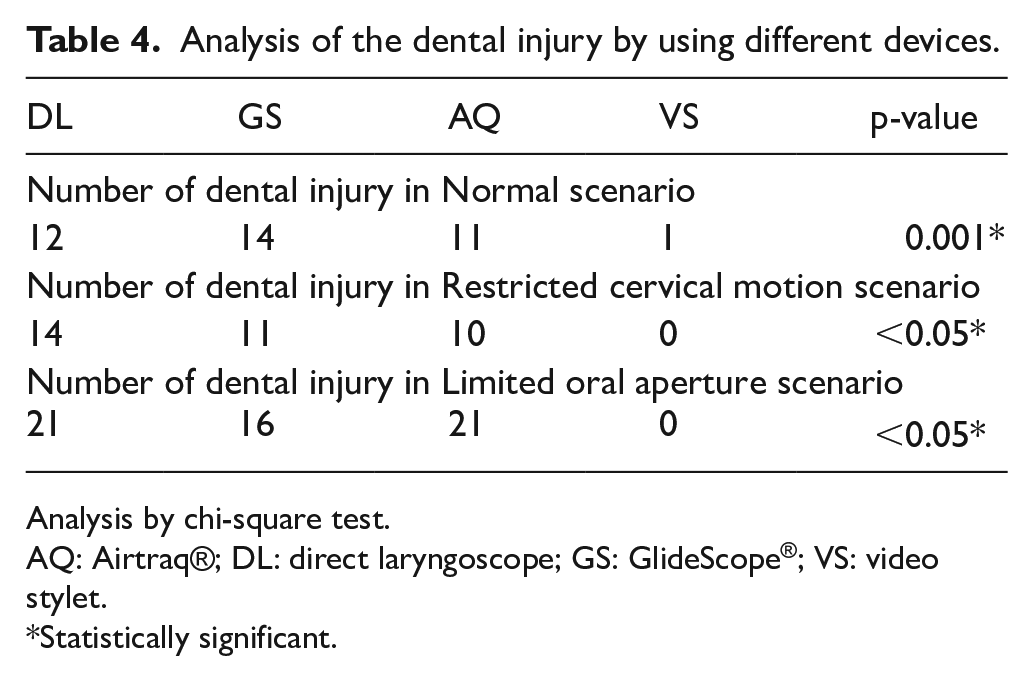
Analysis by chi-square test.
AQ: Airtraq®; DL: direct laryngoscope; GS: GlideScope®; VS: video stylet.
Statistically significant.
Participant’s subjective ease of choice
Overall, participants perceived video stylet as the easiest intubating device in this study. The scores of ease of video stylet were the highest in every scenario (p < 0.05 in all scenarios). Moreover, concerning each scenario, video stylet had a significantly better score when compared with each device individually (Table 5).
Comparison of operator ease.
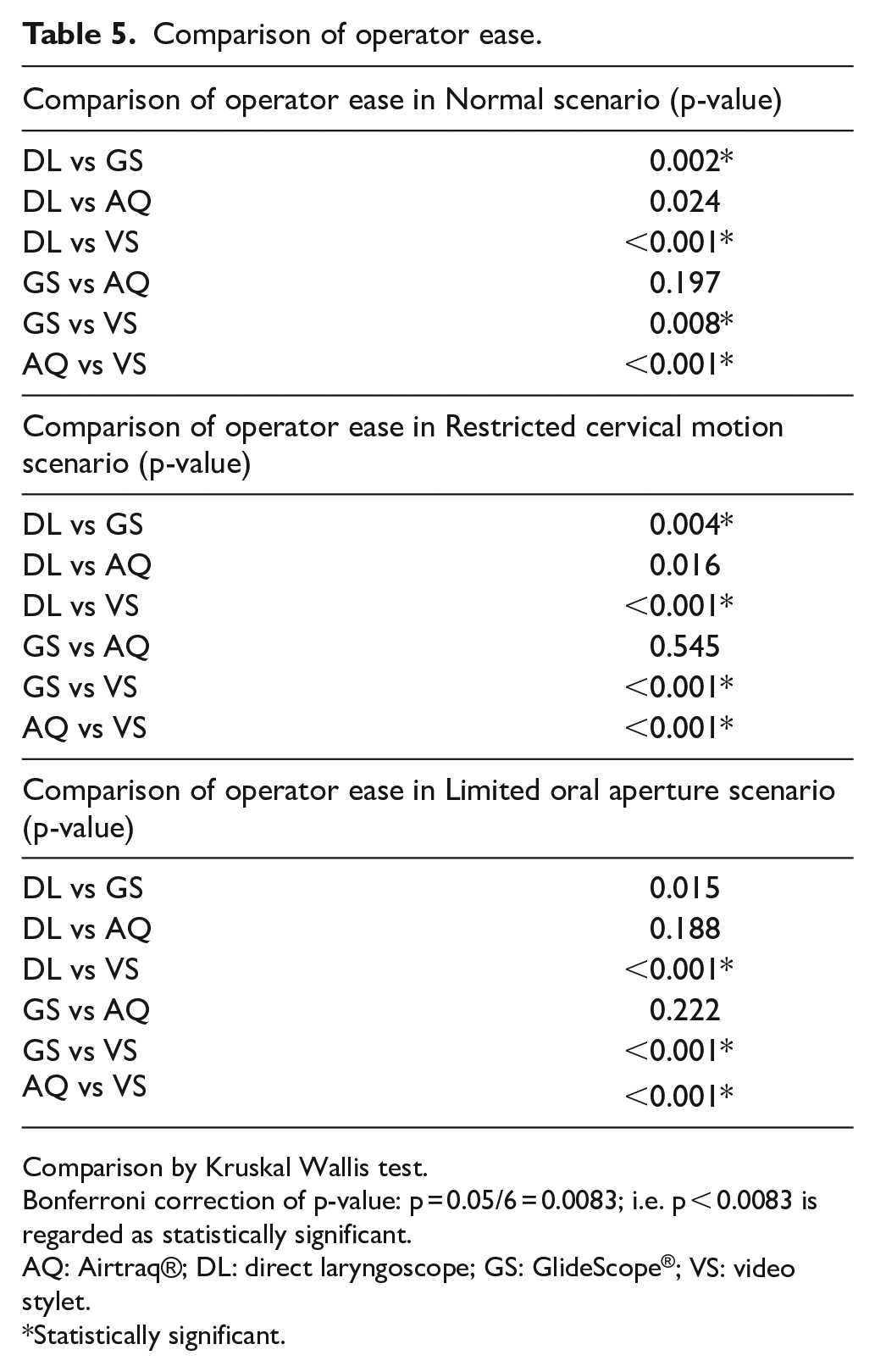
Comparison by Kruskal Wallis test.
Bonferroni correction of p-value: p = 0.05/6 = 0.0083; i.e. p < 0.0083 is regarded as statistically significant.
AQ: Airtraq®; DL: direct laryngoscope; GS: GlideScope®; VS: video stylet.
Statistically significant.
Discussion
Difficult airways are always challenging to emergency physicians. The invention of video laryngoscopes has greatly helped doctors in reducing intubation failure and complications. Nowadays, video laryngoscopes are gaining popularity as the first choice of intubating device, particularly in the era of COVID, video-assisted intubation may potentially become the standard of practice. The introduction of video stylet helps equip emergency doctors with a new airway management technique. Therefore, we perform a study comparing the performance of video stylet with that of other commonly used intubating devices at ED in Hong Kong.
In our study, we have shown that using video stylet had superior performance compared with other intubating devices in different clinical scenarios, among which some were of statistical significance. All participants performed well with VS after a brief training session in which they achieved zero-failure rate and the highest first attempt success rate in all scenarios. Furthermore, intubating with VS struck the shortest intubation time and the least number of potential dental injuries in all three situations. Moreover, VS was the easiest and most favourable choice among all devices in the study.
The mean intubation time with video stylet compared with that of other equipment was shorter in each scenario. The difference varies from at least 5–10 s, and it should be regarded as significant, according to Pieters et al. 7 and Hille et al. 8 Therefore, particularly in a crash airway situation which pre-oxygenation is not feasible or adequate, shortening of intubation time may prevent the patient from having disastrous complications, for example, cardiovascular instability and hypoxemia.9,10 The time of intubation with VS might be even shorter as we observed that participants handled the VS more gently while withdrawing it from the manikin. It could be due to the longer length, and fine movement is required when compared with other devices.
The difference in intubation time between VS and others was statistically most significant in the situation of restricted oral aperture. It could be explained by its slim calibre as the plane needed for intubation with VS is just the cross-sectional area of the ETT. It was much easier for participants to insert the VS through the limited inter-incisor distance. The design of VS also allowed doctors to obtain their desirable laryngeal view without excessive manipulation of the jaw when compared with other devices. This also contributes to a better performance of VS in the scenario of cervical restriction with neck collar. Our findings echoed the conclusion of Tsui et al., 2 Park et al. 11 and Pius et al. 12
Dental injury is an iatrogenic complication and is not uncommon during intubation. Teeth breakage or dislodgement is not only cosmetically undesirable, but it can also possibly result in lower airway obstruction and airway injury. It could be avoided with proper intubation technique in line with good design of the device. When using DL, GS and AQ, a certain amount of force is needed to displace the tongue and jaw so as to obtain a visible view of the larynx or vocal cord. It is common that people tend to rely on incisors as a pivot point of lever when exerting force, particularly a static and continuous force as in intubation. On the contrary, video stylet theoretically does not require any levering forces to displace the patient’s anatomical part to visualize the vocal cord. It can bypass the anatomical structure with its slim profile, and its flexible tip helps to locate the larynx regardless of the laryngeal axis or level. Also, the main stem of VS is not required to move during intubation once it enters the oropharynx. These advantages account for the least dental injuries in the study, only one participant broke the teeth with VS in an attempt out of all three scenarios while at least 10 doctors broke one or more teeth with other devices in each scenario.
Providing apnoeic oxygenation during intubation and hence amelioration of hypoxia13,14 is a potential advantage of video stylet. VS can supply oxygen from the proximal side port to the opening of ETT. Theoretically, it offers a better ‘Apnoeic oxygenation’ compared with the use of nasal cannula as it offers the proximity of oxygen outflow to the lungs. Our study did not investigate this aspect, and further research is warranted to study the effect of apnoeic oxygenation using VS.
In conclusion, video stylet had a better performance than other intubating devices in terms of the time of intubation, avoidance of dental injury and doctors’ satisfaction. However, there was no significant difference in the ETI failure rate and first attempt success rate.
Limitation
As this is a pilot study, the statistical power might not be adequate to discover the differences in the performance of the devices. Outliers may have an accountable impact on the study results, for example, we observed one of the participants could complete intubation with AQ under normal situation in 9 s. This result might cause over-estimation of the performance of AQ and hence under-estimation of VS.
Moreover, this pilot study was non-randomized so that it was subjected to bias. Variable experience in emergency medicine and operation of different intubation devices are potential confounding factors. A further randomized crossover study is suggested to minimize confounding factors.
Although we managed to show significant difference on intubation time in each scenario, the difference of performance between normal and difficult airway situations (restricted cervical motion and limited oral aperture) was not compared and it was apparently similar. The well performance of participants in difficult airway situations was not expected, and extremely difficult situations were not set, for example, setting the inter-incisor distance to be 1 cm in the scenario of limited oral aperture or placing a large intra-oral mass. Therefore, modification of the simulated difficult airway scenarios is warranted in further studies.
The seniority of the participants was not evaluated in this study and bias might occur. Further study with sub-group analysis dividing into basic trainees, higher trainees and specialists may reveal unbiased result. Also, every emergency doctor has his or her own preference and familiarity of intubation devices and the newly introduced video stylet may not be comparable with their well-trained or accustomed conventional devices, in spite of the standard training sessions provided. In addition, doctors from other specialties were not included, for example, anaesthesiologists and intensivists. This limited the generalizability of this study. A larger scale of study involving different specialties is warranted.
Furthermore, it is not possible to blind the participants and investigators, and there would be bias inevitably. Hawthorne effect 15 might also have an effect on doctors’ performance because of their awareness of being observed during intubation as well as the hypothesis of this study. Randomization of the intubation sequence was utilized to minimize the carryover effect that previous intubation attempts may affect the performance of subsequent attempts.
Dental injury was evaluated in this study but not other ETI complications, for example, airway and oropharyngeal trauma. There are several studies suggesting traditional or video laryngoscopes can lead to airway injury including laceration and perforation.16 –20 Although VS may be expected to have a lower incidence of oropharyngeal or airway injury in view of its slim profile, perforation is still possible due to its relatively smaller calibre. Also, in this study, all participants used the midline approach when intubating with VS. This may overestimate the performance of VS as retromolar approach may lead to more oropharyngeal or airway trauma because it involves a narrower pathway and requires a turning manoeuvre. Further studies evaluating oropharyngeal and airway injuries on top of dental injury with sub-group analysis on midline and retromolar approach may help delineate the relationship of the two approaches and the incidence of dental and other injuries.
Last but not least, as this was a manikin study, it could not completely reflect the real-life situation. Concerning the manikin, its stiff plastic parts could not simulate the collapsible soft tissues of real patients, and there was absence of possible challenges such as secretions, vomitus and blood. Moreover, simulated scenario is uncomparable with real resuscitation in which the experience of the stress, distraction from surroundings and the team-based approach are much different.
Conclusion
We have demonstrated that video stylet is a reliable intubating device that has a comparable or even better performance when compared with the commonly used laryngoscopes. Its performance was well supported by evidence in previous studies.21 –23 Also, it was the most favourable device of choice by the participants among the airway gadgets. Further studies are warranted to prove and validate the effectiveness and advantages as well as drawbacks of VS so that it can potentially be a good alternative of intubation device in the emergency department, particularly for difficult airway management.
Footnotes
Acknowledgements
The authors thank all the emergency doctors for participating in this study and Mr. Lee Wing Chung, Secretary of Accident and Emergency Department, North Lantau Hospital for clerical support.
Author contributions
Y.O.L., O.F.W. and S.K developed the study concept and designed the study. Y.O.L. conducted the study. Y.O.L., O.F.W. and S.K. analysed the data. Y.O.L. drafted the manuscript. O.F.W., S.K., H.M.M., C.H.A.L. and Y.N.S. revised the manuscript critically for important intellectual content. All authors read and approved the final manuscript.
Availability of data and materials
All participants’ identifications were removed before storage. The master data set was kept by the investigators in the computer and was password protected. Access to the data would be limited to the investigators and Clinical Research Ethics Committees of Kowloon West Cluster, Hong Kong Hospital Authority. Please contact the corresponding author for further information of data if required.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was not necessary because no patient data have been included in the manuscript. Written consent was obtained from the participants for their anonymized information to be published in this article.
Ethical approval
This study was approved by the Clinical Research Ethics Committees of Kowloon West Cluster, Hong Kong Hospital Authority.
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.