
Abstract
Background:
Emergency nurse practitioners have traditionally been reluctant to treat acute red eyes in Hong Kong emergency departments. The Edinburgh Red Eye Diagnostic Algorithm is the only validated tool to assist non-ophthalmologists to make diagnoses.
Objectives:
This study investigates the utility of a modified version used by emergency nurse practitioners.
Methods:
This is a prospective single-centre cohort study in a university hospital emergency department in Hong Kong, comparing red eye patients seen by emergency nurse practitioners with the aid of the algorithm to patients seen by emergency doctors. Data on patient-reported symptom severity were obtained on the day of consultation and information on resolution of symptoms at 1 week following emergency department attendance via telephone interviews.
Results:
A convenience sample of 50 patients was recruited to the emergency nurse practitioner group and 130 patients were recruited to the doctors’ group over 9 weeks. Reductions in symptom severity were seen in both groups (>70% in both groups reported moderate to very severe discomfort on day 0; ~90% in both groups reported none or mild discomfort on day 7). There was no difference between the two groups (p = 0.55, analysis of covariance). Symptom resolution was reported in 96% in the emergency nurse practitioner group and 98.5% in the doctor’s group, which was not statistically significant (p = 0.31, χ2 test).
Conclusion:
Emergency nurse practitioners using the Edinburgh Red Eye Algorithm to manage red eye patients in a Hong Kong emergency department achieve similar patient-reported outcomes compared to emergency department doctor consultations.
Keywords
Introduction
Acute red eye is one of the most common ophthalmological conditions that lead people to seek emergency medical care. Preliminary data from Prince of Wales Hospital in Hong Kong prior to this study revealed that half of the emergency department (ED) attendances for ophthalmological conditions were presentations with acute red eye. However, other work showed that eye problems formed only 4% of patients seen in a local emergency nurse clinic (ENC) (Chung JYM, Lee KH, Cheng R, et al. A six-year analysis of an emergency nurse practitioner clinic in Hong Kong. Poster presented at the Hospital Authority Convention, Hong Kong, 7–8 May 2014, Personal communication, Ms JYM Chung). This reflects an obvious reluctance among Hong Kong emergency nurse practitioners (ENPs) to treat eye problems, which probably stems from their limited exposure and training in ophthalmological emergencies. Current training of ENPs in Hong Kong has a significant focus on orthopaedics and minor trauma. As most emergency nurses do not work in an ophthalmology department after graduation, their limited undergraduate knowledge fades over time.
Red eye diagnostic algorithm
The use of a validated diagnostic algorithm offers a possible solution. Algorithms are clinical decision tools written by experts for use by non-experts to allow them to make evidence-based decisions. It can be an efficient method to save time and costs for novice practitioners to minimise unnecessary exhaustive investigations. Algorithms have previously been adopted in the ED with promising results.1–4
Nine red eye algorithms were identified from the literature. Two algorithms classified patients according to the severity of pain.5,6 However, pain is a subjective indicator, and healthcare professionals often inaccurately estimate patient’s intensity of pain.7–9
Two algorithms classified patients according to the presence of pain. Carter’s algorithm 10 was felt to be too complicated, while Marrow and Abbott’s algorithm 11 was considered too simple for clinical use. Sallustio 12 classified red eyes according to the pattern and depth of redness. This approach was risky as it is not easy for non-experts to identify clear differences. Berta et al.’s algorithm 13 and Granet’s algorithm 14 mainly focused on conjunctivitis, with less attention to other red eye diagnoses.
Kabari and Nwachukwu 15 developed an algorithm through the training of artificial neural networks. The algorithm offered limited educational value as the clinician just needed to enter the signs and symptoms and a computer would ‘do the rest’. Besides, the algorithm also included conditions other than red eyes.
Timlin et al., 16 introduced the Edinburgh Red Eye Algorithm. They invited ED doctors, ENPs, general practitioners and opticians to use the algorithm on red eye patients, and patients were then seen by an ophthalmologist. The concordance of diagnosis was assessed and found to have a 72% overall diagnostic accuracy.
However, the Edinburgh study can be criticised. First, there was no independent blinding of the ophthalmologist with respect to the original diagnosis. Second, a sampling bias was present as not all patients visiting during the study period were included; accuracy may be overestimated as patients being referred directly to an ophthalmologist usually have more apparent signs and symptoms. Third, the inclusion and exclusion criteria were not reported too, leaving questions on the applicability of the study results. It may have been too early to conclude that the diagnostic accuracy of non-ophthalmologists was greater with the algorithm, as the accuracy before and after using the algorithm was not available. The generalisability of the Edinburgh study was also limited by the small sample size, as half of the algorithm diagnoses were not reported at all.
In summary, most of the algorithms were not suitable for the use by ENPs. The Edinburgh algorithm was the only one validated, clearly designed and easy to use; however, current evidence was not enough to allow its use in the ED without further external validation.
This prospective study aimed to investigate the utility of a modified version of the Edinburgh red eye algorithm used by ENPs in a single centre in Hong Kong, for the initial management of patients presenting to the ED with (an) acute red eye(s).
Methods
Study design and setting
This study adopted a prospective cohort design. Some modifications to the algorithm were suggested by a senior ophthalmologist (H.H.-W.L.) in an attempt to make the algorithm more comprehensive, practical and educational for the use of ENPs in the local Hong Kong setting.
Patient-reported outcomes
This study did not focus on the diagnostic accuracy of the algorithm. Although comparing to a reference standard is the preferred method in diagnostic studies, a red eye algorithm does not end up with a simple positive or negative result as most diagnostic tests do. A patient-oriented approach was adopted. This study used a patient-reported outcome (PRO) as an index to evaluate the performance of ENPs in managing red eyes.
Patients presenting with acute red eyes assessed by ENPs with the aid of the modified Edinburgh algorithm were compared to those seen by ED doctors without using the algorithm. The two groups were followed up over 1 week to see whether there were any differences in their reported outcome. The study was conducted in the ED of a university hospital ED with around 138,000 annual visits. Patients were recruited over a 2-month period (December 2015–January 2016).
Definition
In this study, ‘acute red eye’ was defined as sudden onset of red eye within 2 weeks of ED presentation, with blood between the conjunctiva and the sclera. Any eyes with redness of the surrounding skin without involvement of the conjunctiva were excluded.
Population
Patients were recruited when they attended the ED with a complaint of acute red eyes. To be eligible, the red eyes could result from trauma or non-trauma and be confined to situations described as an emergency or less urgent according to the Hong Kong Hospital Authority triage guidelines. 17 Exclusion criteria were the following: a recent history of eye surgery; a concurrent physical complaint which was outwith the ENP scope of practice; haemodynamic instability; vulnerable groups; and language barrier, dementia or cognitive impairment which would affect patient’s ability to understand the study and give informed consent. Patients with signs of red eye that indicates 360° subconjunctival haemorrhage (SCH) or a suspected partial SCH associated with elevated blood pressure or current use of anticoagulants were also excluded because these conditions point to an underlying medical cause which is outside the ENPs’ scope of practice. Non–Hong Kong citizens were excluded as they are not eligible for public ophthalmology services.
The targeted sample size was 50 for the ENP group for pragmatic reasons. The sample size of the control group was not limited to 50 so as to minimise selection bias.
Subjects were identified at triage and were selected based on a convenience sampling method. Patients were seen by ENP or ED doctors depending on ENP availability. Patients who attended during the ENC service hours were seen by ENPs with written consent. Those who attended at other times were seen by ED doctors, and the principal investigator (L.-K.C.) then reviewed the records and contacted the eligible patient by telephone to gain verbal consent for study inclusion.
Study procedure
Figure 1 presents a flow diagram of the study design. For the ENP group, the patient was seen and treated by the ENP with the aid of the study algorithm. There were six ENPs involved in the study, and all ENPs involved were experienced nurses with at least 5 years of ENP experience and at least 18 years of nursing experience. For the control group, patients were seen and treated by ED doctors according to standard practice. Patients with appropriate clinical indications would be referred to ophthalmologists. The ophthalmologists would see and treat the patient according to the clinical urgency. If referral to ophthalmologists was not clinically indicated, the patient would be discharged with any necessary medication. All the patients were invited to complete a questionnaire on the day of consultation and 1 week after.
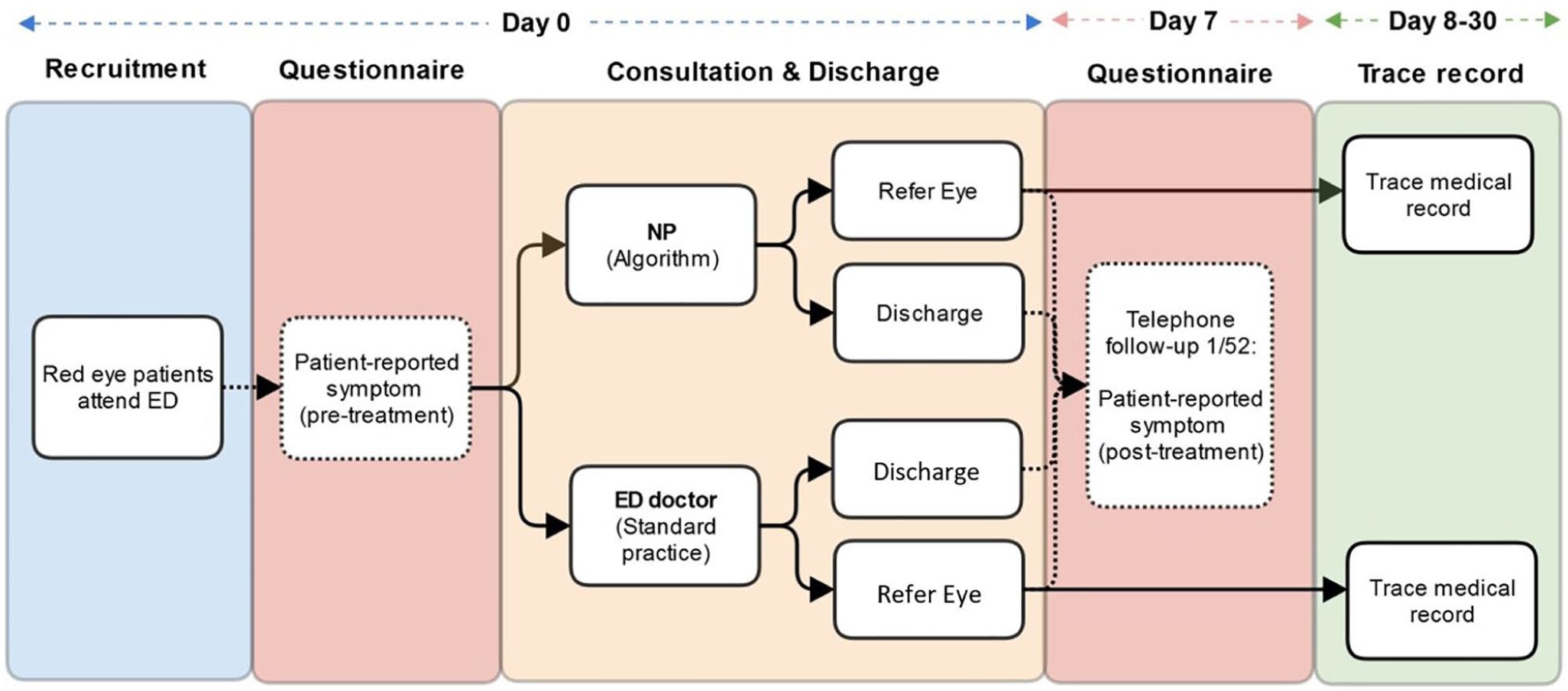
Patient flow in the red eye study.
Instrument
The algorithm used in this study was a modified version developed from the Edinburgh Algorithm. All the amendments were suggested and approved by a senior ophthalmologist in the study team (H.H.-W.L.). The modified algorithm and the list of changes are provided in the Supplementary File 1.
Measures and endpoints
A pre and post questionnaire was used to assess two complementary outcomes: patient-reported symptom severity and symptom resolution. On day 0 and day 7, patients were asked to rate their symptom severity using a Likert-type question which was identified from the validated Visual Functioning Questionnaire (VFQ-25).18,19 On day 7, patients also rated their perceived symptom resolution, using a question identified from the Medical Outcomes Study Questionnaire Short Form 36 Health Survey version 2(SF-36v2).20,21 The day 7 questionnaire also contained three more questions to rule out confounding factors concerning ED re-attendance, medical consultation outside the study hospital and any use of non-hospital medications.
Statistical analysis
The SPSS package 22.0 (IBM Corp., Armonk, NY. USA) was used for statistical analysis. Independent-samples t tests and χ2 tests were used to examine the comparability of the two groups on all baseline variables. The outcomes of the two cohorts according to the patients’ reported symptom severity and symptom resolution score were compared. Analysis of covariance (ANCOVA) was used to analyse longitudinal changes in symptom severity. For symptom resolution, ordinal variables were grouped into categorical counterparts and analysed using the χ2 test.
Results
Patient characteristics
Figure 2 shows the study profile. One hundred eighty-three patients were recruited to the study; one patient was excluded from analysis as the patient was treated by an ophthalmologist directly in the ED. One patient was lost to follow-up in each group. A total of 180 patients completed the second questionnaire on day 7. The number of patients in the intervention (n = 50) and the control (n = 130) group was different as planned, due to the limited ENP service hours.
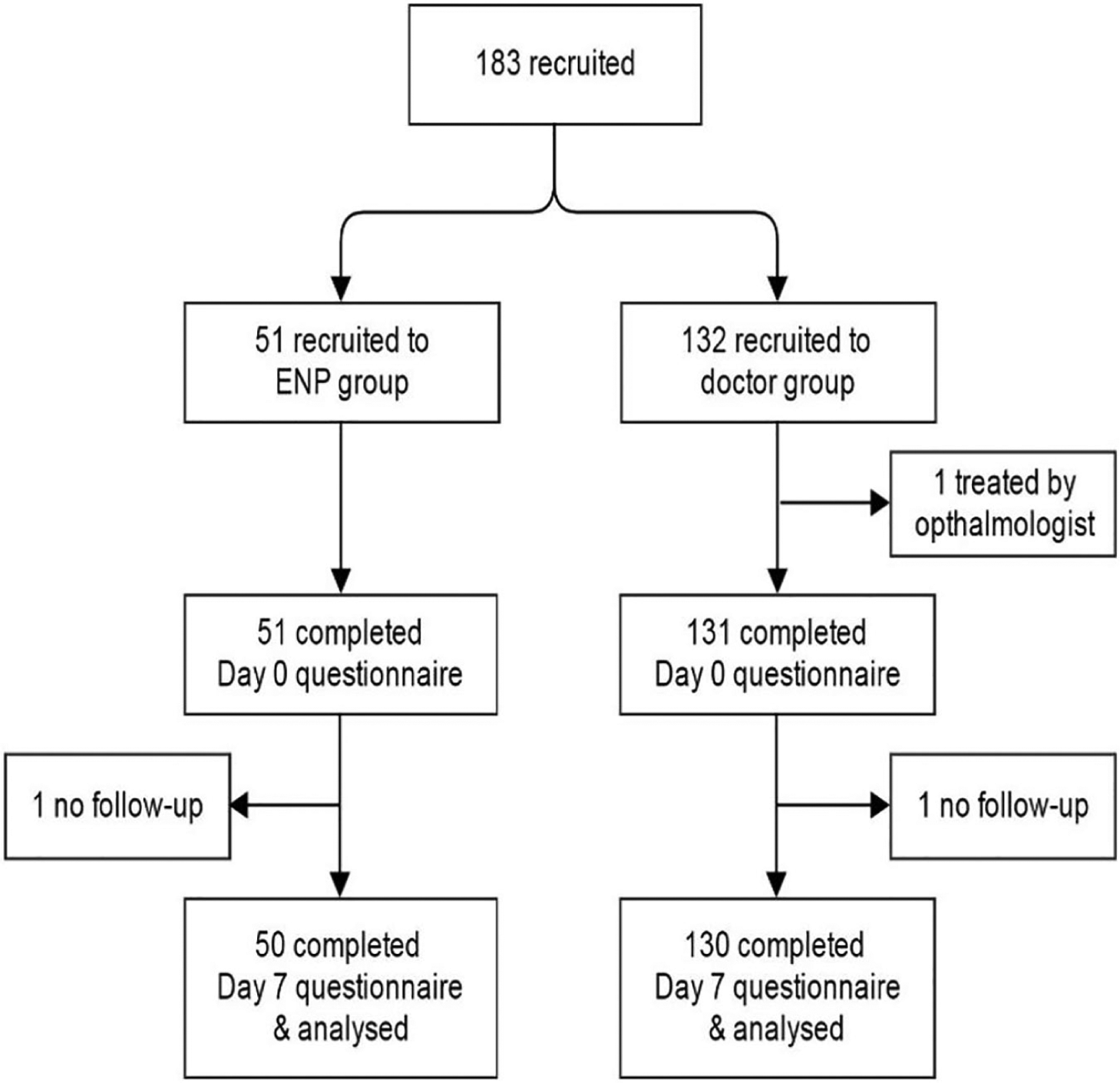
Study profile.
Baseline characteristics of both patient groups were similar, with a mean age of 49.7 years in the ENP group and 49.9 years in the ED doctor group. In the ENP group, 58% were male and 42% were female, while in the ED doctor group, 60.8% were male and 39.2% were female.
Diagnoses
Table 1 showed a distribution of all the diagnoses from both the ENP and the ED doctor’s control group. Conjunctivitis was the most prevalent condition (25%). Other common conditions included corneal abrasion, corneal foreign body and SCH (Table 1). It should be noted that in total, 109 were seen by an ophthalmologist based on the indication by the ENP algorithm and the ED clinician’s clinical judgement (Supplementary File 2). The medical records of those patients being seen by ophthalmologist in both groups were reviewed. When compared with ophthalmologist’s diagnosis with ENP group and doctor’s group, no statistical significant difference in overall diagnostic accuracy was found (p = 0.875, χ2 test) (Supplementary File 3). Nine patients were found to have misdiagnosed, of which seven were algorithm related and two were ENP related (Supplementary File 4).
Distribution of diagnoses.
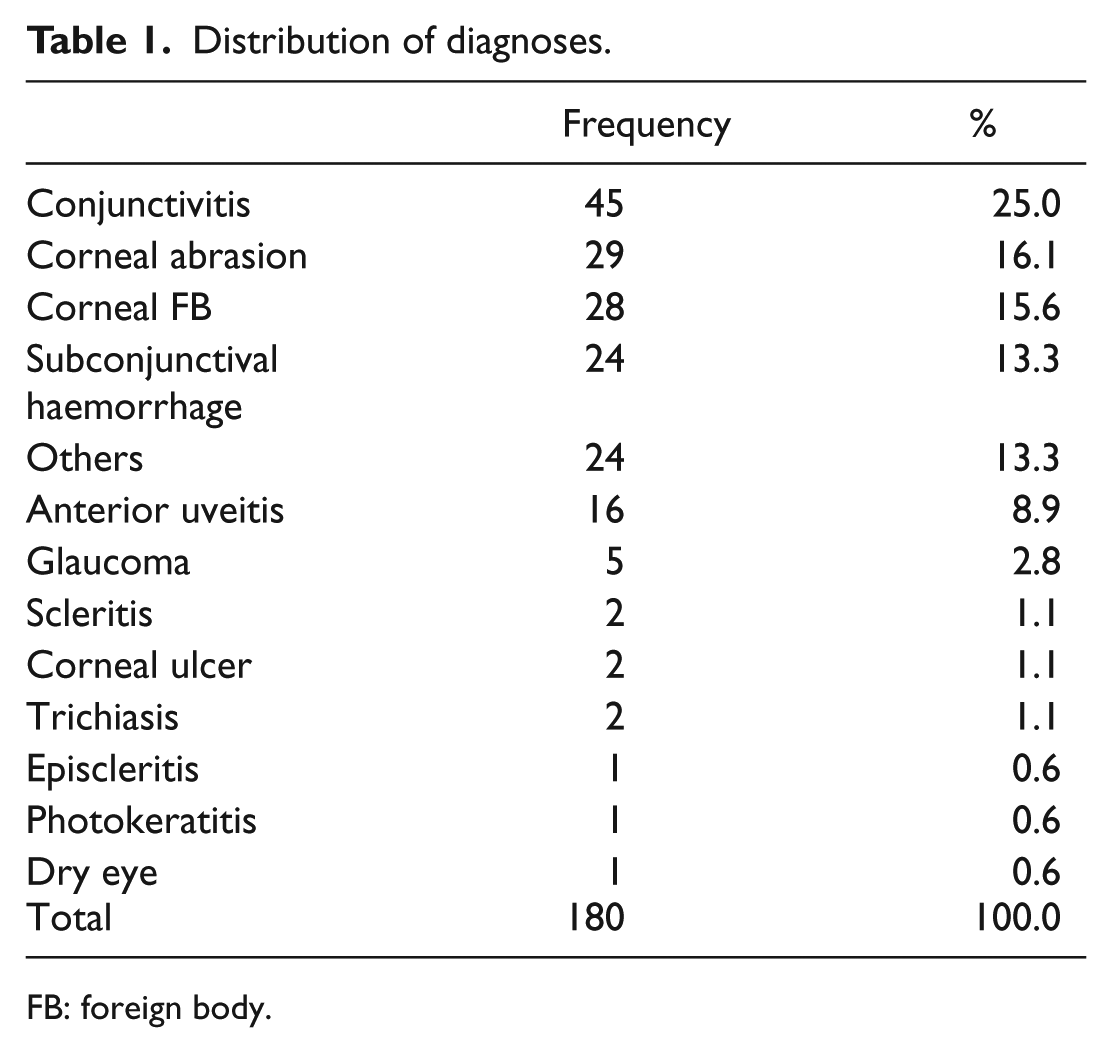
FB: foreign body.
Patient-reported outcomes
Symptom severity
On day 0, over 70% of patients in both groups reported moderate to very severe symptoms (Figure 3). On day 7, 90% of the ENP group and 87% of the doctors’ group reported none or mild symptoms (Figure 4). There were reductions in symptom severity for both groups, and the differences between the two groups on longitudinal changes of symptom severity were not statistically significant (p = 0.55, ANCOVA).
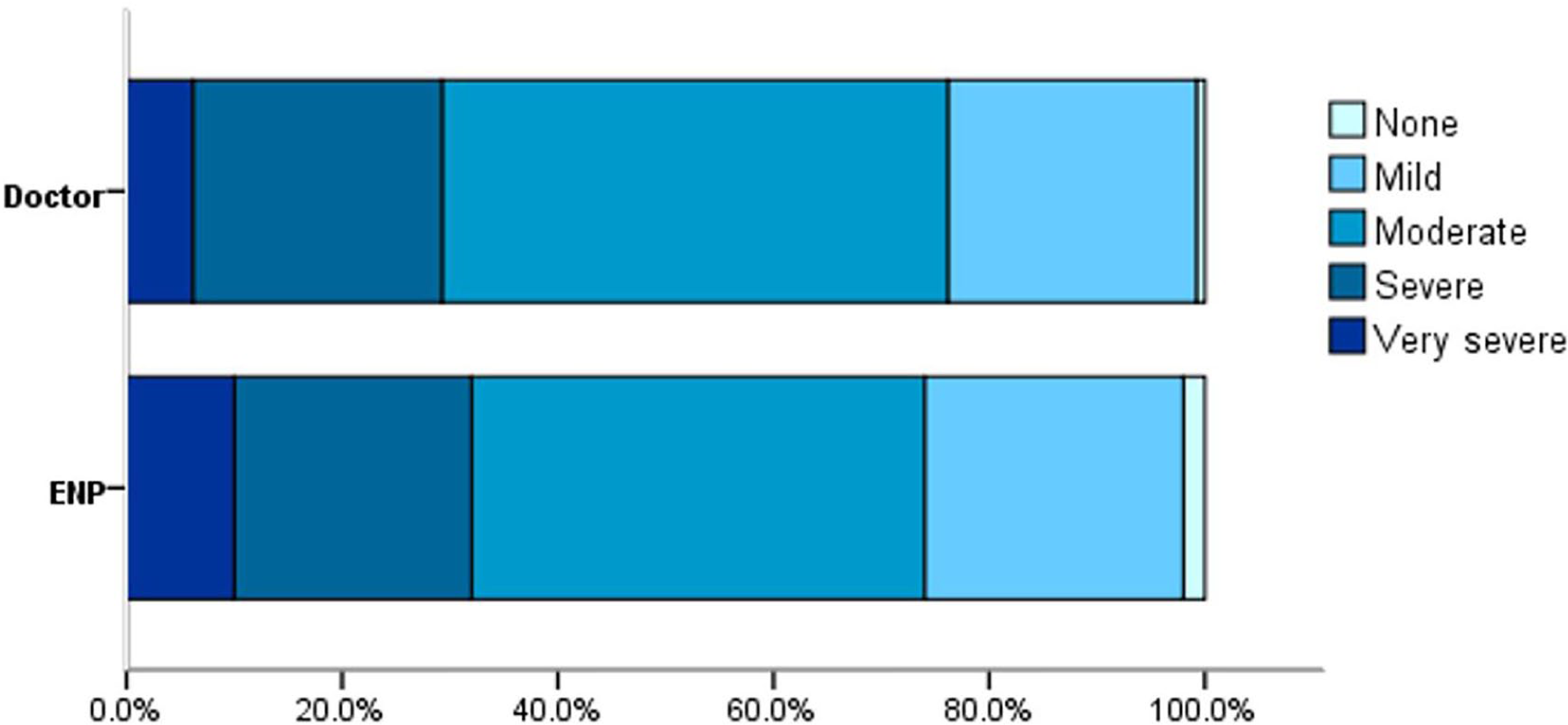
Symptom severities between cohorts on day 0.
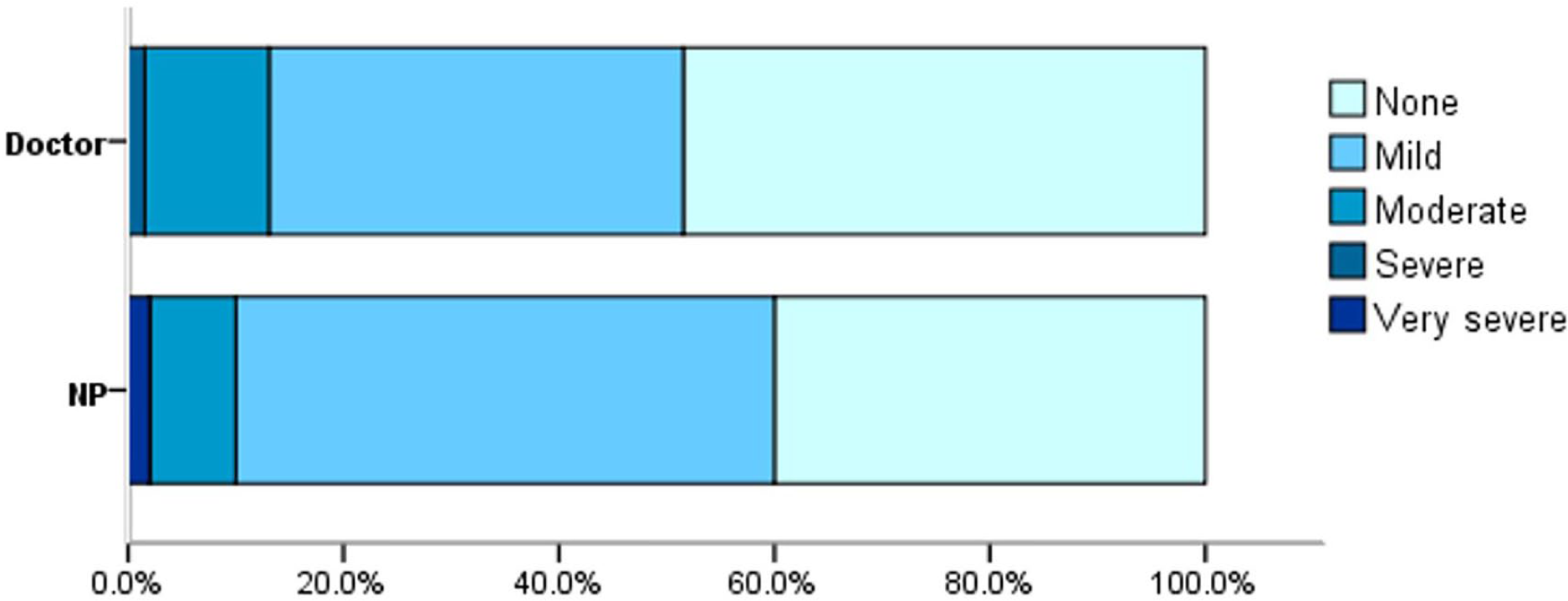
Symptom severities between cohorts on day 7.
Symptom resolution
On day 7, patients were asked to rate their perceived level of symptom resolution using five ranked responses. Results presented in Figure 5 showed that a similarly large proportion of patients in both groups reported significant improvement after their first consultation (ENP group 84%, doctors’ group 80%).
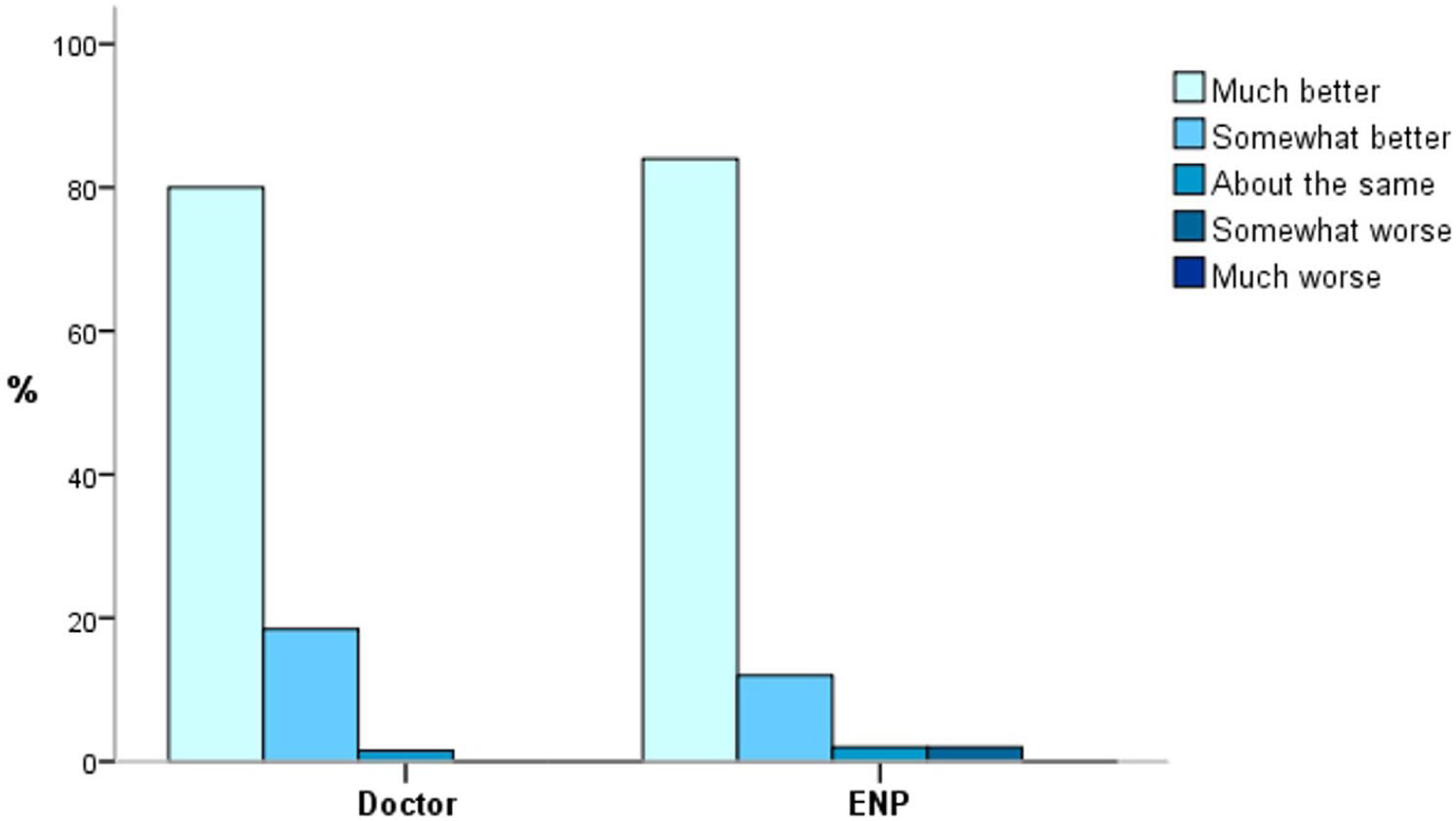
Comparison of perceived symptom resolution on day 7 between cohorts.
The five answer options were further grouped into two for analysis. Patients answering ‘much better’ or ‘somewhat better’ were classified as ‘symptoms resolved’; patients answering ‘about the same’, ‘somewhat worse’ or ‘much worse’ were classified as ‘symptoms not resolved’. Symptom resolution was reported in 96% of patients in the ENP group and 98.5% in the doctors’ group, a difference that was not statistically significant (p = 0.31, χ2 test).
Confounding factors
Data were collected on three potential confounding factors identified a priori: ED re-attendance, seeking help from other healthcare providers and using non-hospital prescribed medication. Only a few patients re-attended ED with similar proportions in both groups (2.3% for the doctor group and 2% for the ENP group). There was also no difference in the proportion of patients using non-hospital prescribed medication (12.3% in the doctor group and 14% in the ENP group). There was an obvious difference in the proportion of patients who had sought assistance from other healthcare provider (10% in the doctor group and 2% in the ENP group). It was impossible to get more information on this aspect because all patients who had sought assistance from other healthcare providers within 1 week had reported symptom resolution. Table 2 lists the reasons why patients sought other healthcare provider’s assistance; this shows that only a small number did this due to unsatisfactory progress.
Reasons for patients seeking other healthcare provider (n = 14).
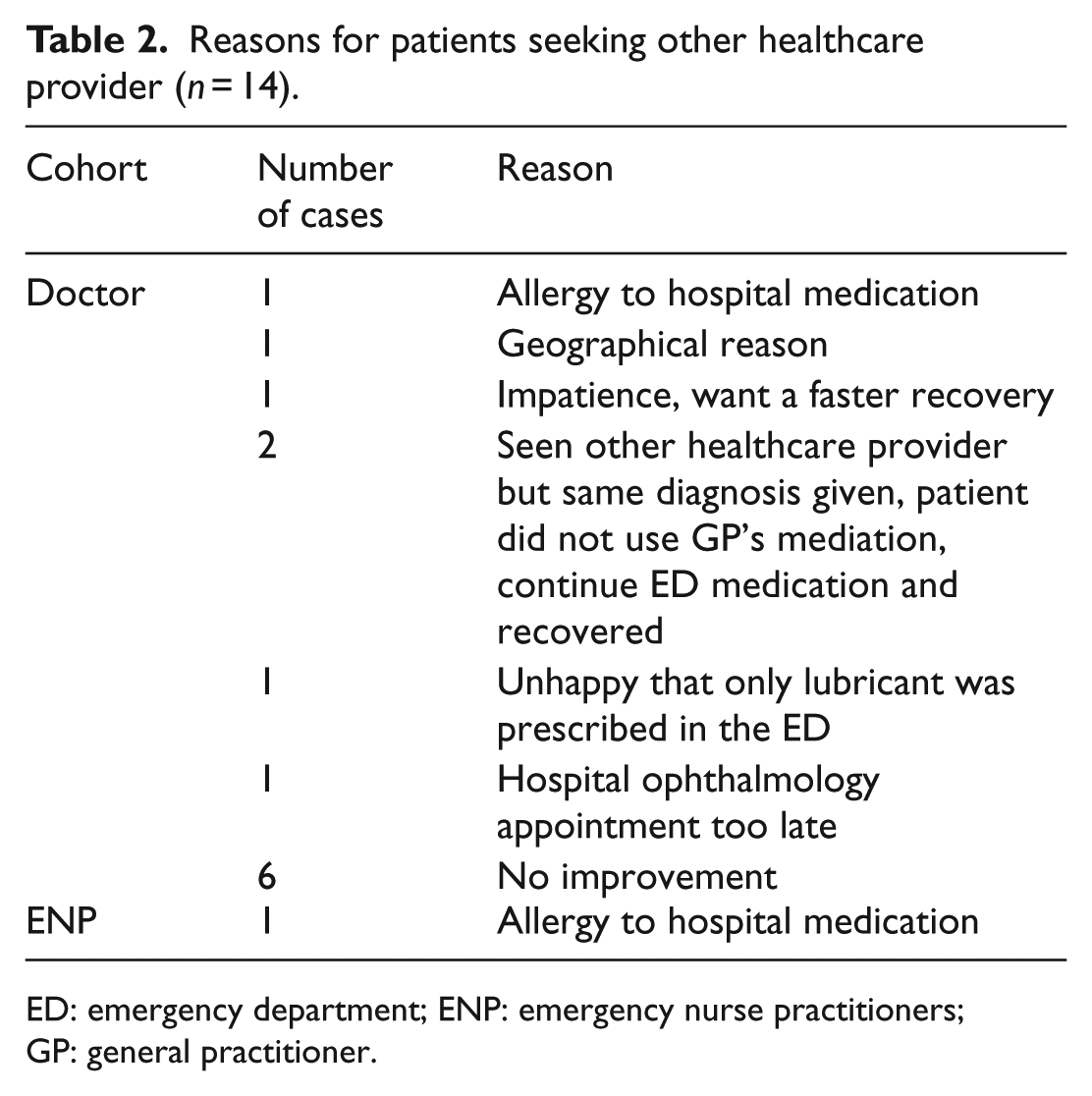
ED: emergency department; ENP: emergency nurse practitioners; GP: general practitioner.
Discussion
With the aid of a modified algorithm, this study showed that acute red eye patients treated by ENPs experienced improvement in symptoms, which was no different to the outcomes found in those treated by ED doctors. There were five patients in the ENP group who reported the same severity score, increased severity score or no resolution on day 7. When reviewed, none of these cases were caused by a failure of the ENPs to manage the patient appropriately. In the ENP group, all patients who presented with alarming signs or symptoms were referred to an ophthalmologist accordingly.
The two questions about patients’ symptom severity and symptom resolution together demonstrate a coherent picture of the patients’ outcome. A few patients rated the same level of symptom severity on day 0 and day 7, but they also reported symptom resolution on day 7. This may be because patients could have forgotten their initial score. Although they had not fully recovered, the fact that they were improving was important as the recovery process sometimes takes more than 1 week. Some patients perceived no discomfort on day 0 but still reported symptom resolution on day 7. This was possible as some benign conditions, like SCH, cause no discomfort and the only sign of recovery is the subsidence of redness. When brought together, the outcome measured by these two questions strengthen our conclusion that the majority of patients recovered well and that our ENPs were providing appropriate management.
Confounding factors
Four potential confounding factors were highly likely to affect the outcome of our patients. The first was referral to ophthalmology services. Patients were sometimes referred for a benign diagnosis, but occasionally, the true diagnosis could turn out to be something much more serious. However, there was no difference in the referral rate in the two cohorts. According to the algorithm, at least 60% of those referred cases in each group were indicated to receive an urgent referral, and of course there were some non-urgent conditions which also frequently received referrals.
The other three confounding factors were ED re-attendance, seeking help from other healthcare providers and use of non-hospital prescribed medication. The data showed that in the ENP group, only one patient reported ED re-attendance but that was a scheduled ED follow-up appointment; one patient had visited another healthcare provider because of an allergic reaction to prescribed hospital medication. Seven patients reported the use of non-hospital provided medication, but only two of them did that because of an unsatisfactory response to hospital prescribed medication.
Limitations
The small sample size was the major limitation of this study. The number of patients recruited in the ENP group was limited by the ENP service hours in the study centre.
Second, not all the subjects (in the ENP or the control group) were reviewed by the ophthalmologist because of resource limitation. There may have been cases who did not have the correct diagnosis but reported symptom improvement.
This study demonstrated the usefulness of the modified algorithm, and it may be more obviously demonstrated if one could compare the outcomes of ENP treated patients before and after using the algorithm. However, this approach was impossible because there were insufficient data at the baseline for comparison as ENPs were reluctant to treat eye problems at the beginning of the study.
Finally, this modified algorithm was designed to be used in an ED equipped with non-contact tonometry and a slit lamp. This limits the generalisability of the study results to other EDs or other primary care setting where this equipment is not available.
In conclusion, this study provides evidence in support of the use of a modified algorithm as an effective diagnostic tool to help ENPs treat ED patients with acute red eye. A larger study could confirm the encouraging results provided by this study.
Supplemental Material
supplementary_material – Supplemental material for Emergency nurse practitioners’ use of a modified Edinburgh red eye diagnostic algorithm: Prospective observational study
Supplemental material, supplementary_material for Emergency nurse practitioners’ use of a modified Edinburgh red eye diagnostic algorithm: Prospective observational study by Lee-Kwan Chuk, Josephine Yuen-Man Chung, Henry Hing-Wai Lau, Ling Yan Leung, Kevin KC Hung and Colin A Graham in Hong Kong Journal of Emergency Medicine
Footnotes
Author contributions
L.-K.C., H.H.W.L. and C.A.G. conceived the study and designed the study. L.-K.C., J.Y.-M.C., L.Y.L., K.K.C.H. and C.A.G. provided statistical advice on study design and analysed the data. L.-K.C. conducted the study and performed data collection; managed the data, including quality control; and drafted the manuscript. All authors contributed substantially to its revision. All authors approved the version to be published and take public responsibility for appropriate portions of the content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Informed consent
Written consent was obtained for patients who were seen by ENPs. For the control group, the principal investigator (L.-K.C.) obtained verbal consent via telephone before study inclusion.
Ethical approval
This study was approved by the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (CREC reference number 2015.479).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.