
Abstract
Background:
The care of critically ill patients is a strong indicator of service quality provided in the emergency department. Since families are the major social support sources, assessing the family members’ needs may reduce their anxiety and depression owing to the acute situation of their loved ones while improving the patients’ recovery.
Objective:
We aimed to evaluate the expectations and needs of relatives of critically ill patients to formulate solutions to improve the quality of emergency department service.
Methods:
We conducted a prospective, cross-sectional survey of 873 relatives of nontraumatic, critically ill patients who completed the Turkish version of the Critical Care Family Needs Inventory in the emergency department of a university hospital in Turkey. The needs statements were evaluated under five subheadings: meaning, proximity, communication, comfort, and support.
Results:
In total, 249 (28.5%) participants were females and 624 (71.5%) were males (mean age, 41.79 years). The “meaning” category was given the highest priority, followed by “communication,” with average points of 3.75 and 3.57, respectively. The most important needs were being informed regularly about the patient’s condition and being assured that the patient is under the best possible care, whereas personal, physical, and emotional needs were the least important.
Conclusion:
Relatives of critically ill patients primarily focus on the quality of patients’ care. Creating a positive rapport based on trust and providing a healthcare environment where the expectations and needs of relatives are met should be prioritized by emergency department physicians, nurses, and other staff while caring for critically ill patients.
Introduction
The word “emergency” refers to urgent medical care when the physical and/or mental health of a person is in peril. The emergency department (ED) is a healthcare unit where unexpected health problems can be quickly diagnosed and treated. Therefore, ED manages frequently encountered critical clinical scenarios including suddenly developing and life-threatening situations such as trauma, burn, cardiac arrest, acute coronary syndrome, cerebrovascular disease, and shock. Unfortunately, these acute clinical conditions negatively impact patients’ and their families’ quality of life due to stress and uncertainty of the unexpected situation. As a result, relatives of critically ill patients can suffer from considerable anxiety and depression. 1
Treatment and care of critically ill patients is an accurate indicator of the quality of service provided in the ED and is also important in terms of the satisfaction of patients’ relatives. However, ED overcrowding in recent years due to the inability of the healthcare system to meet the demand of the critically ill population is associated with increased stay duration in the ED and mistakes by the medical staff causing decreased quality of care leading to decreased patient satisfaction.2,3 Moreover, prominent indicators of service quality such as accurate information on the patient’s condition, physical and functional characteristics of waiting areas, and attitude and behavior of the staff are important to the patients’ relatives. 4 Discrepancy in fulfilling the expectations of the relatives of these patients in the ED may lead to adjustment issues or even crisis situations. 1 Therefore, assessing relatives’ needs and expectations may help reduce families’ stress while facilitating patients’ recovery5,6 and improving staff-relative relations. 7 Moreover, patients’ and relatives’ trust can be gained while creating a pleasant, clean, and functional healthcare environment that enables healthcare providers to focus on the patient.
The Critical Care Family Needs Inventory invented by Molter 8 in 1979 helps define the needs of families of intensive care unit (ICU) patients and has been used in many ICU-based studies.9–17 However, studies focusing on expectations and needs of relatives of critically ill patients being treated in ED are limited.
Here, we aimed to identify the expectations and needs of relatives of nontraumatic critically ill patients admitted to our ED to help improve the quality of service by directing solutions based on the obtained results.
Materials and methods
This prospective, cross-sectional, survey-based research study was approved by Erciyes University Clinical Research Ethics Committee dated 4 March 2012 (no. 2012/226). The relatives’ demographic data and the survey questions for determining the expectations and needs of patients’ relatives were obtained through face-to-face interviews between the first author (U.O.) of this study and the participants. Moreover, participants provided written informed consent to participate in the study as volunteers.
The study enrolled 873 relatives of nontraumatic, critically ill patients admitted to Erciyes University Faculty of Medicine, Department of Emergency Medicine, Internal Intervention Unit between 30 June 2012 and 30 August 2012 who were >18 years of age, preferably blood relatives, who frequently accompanied the patient, and who communicated most with the ED staff.
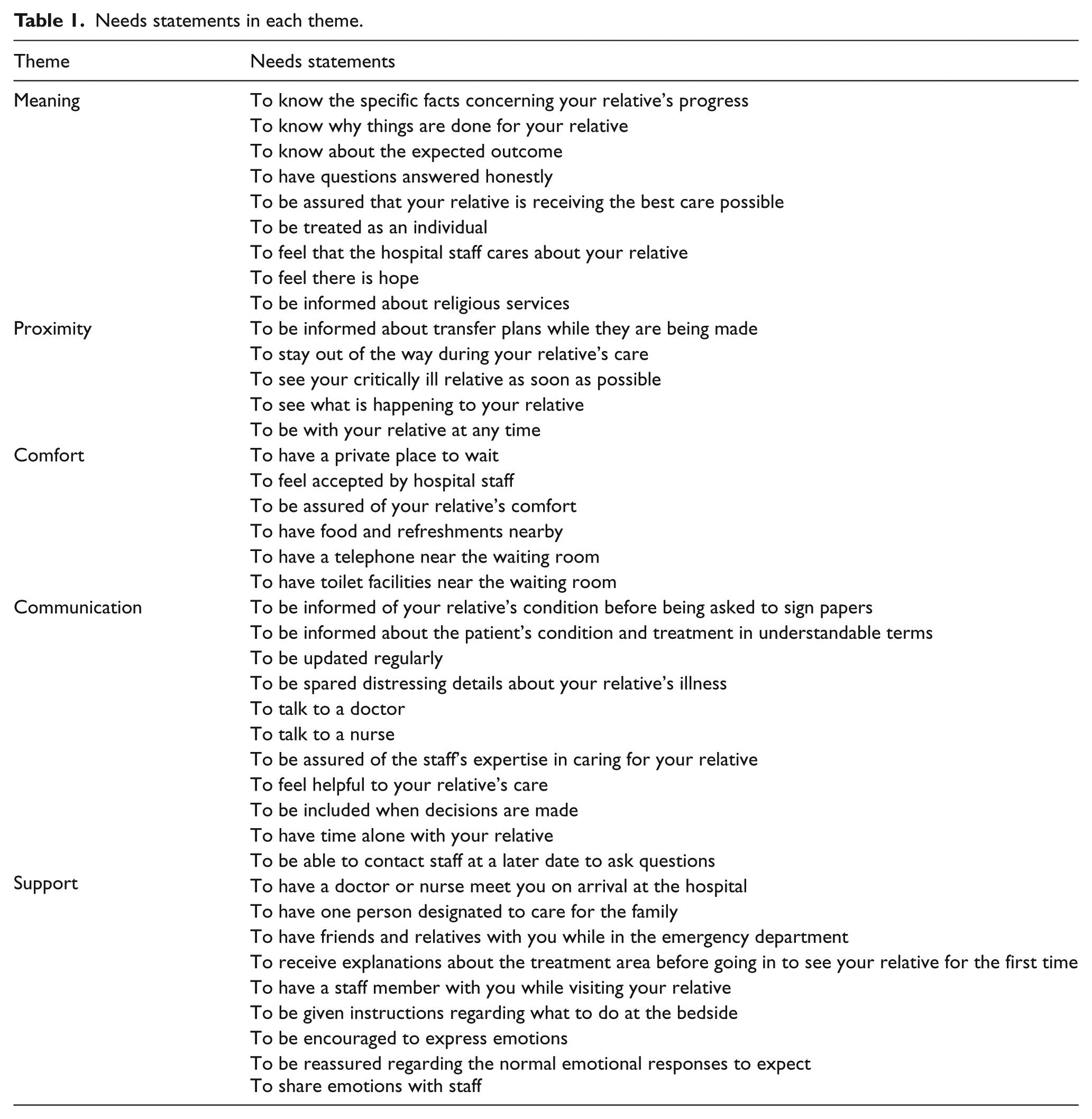
The demographic data form consisted of questions regarding age, sex, education status, and relationship of the participants to the patient. As previously described, the questions in the expectation and needs survey were derived from the Turkish version of the quadruple Likert-type questions under five headings (meaning, proximity, communication, comfort, and support).4,18,19 A total of 40 Likert-type questions were answered as “1 = not important,” “2 = slightly important,” “3 = important,” and “4 = very important.” The meaning, proximity, communication, comfort, and support categories consisted of 9, 5, 11, 6, 9 questions, respectively (Table 1).
Needs statements in each theme.
Analysis: IBM SPSS Statistics software, version 20.0 (IBM Corp., Armonk, NY, USA) was used for statistical evaluation. Descriptive statistics are given as number of units (n), percentage (%), median, and average ± standard deviation
Results
Characteristics of study participants
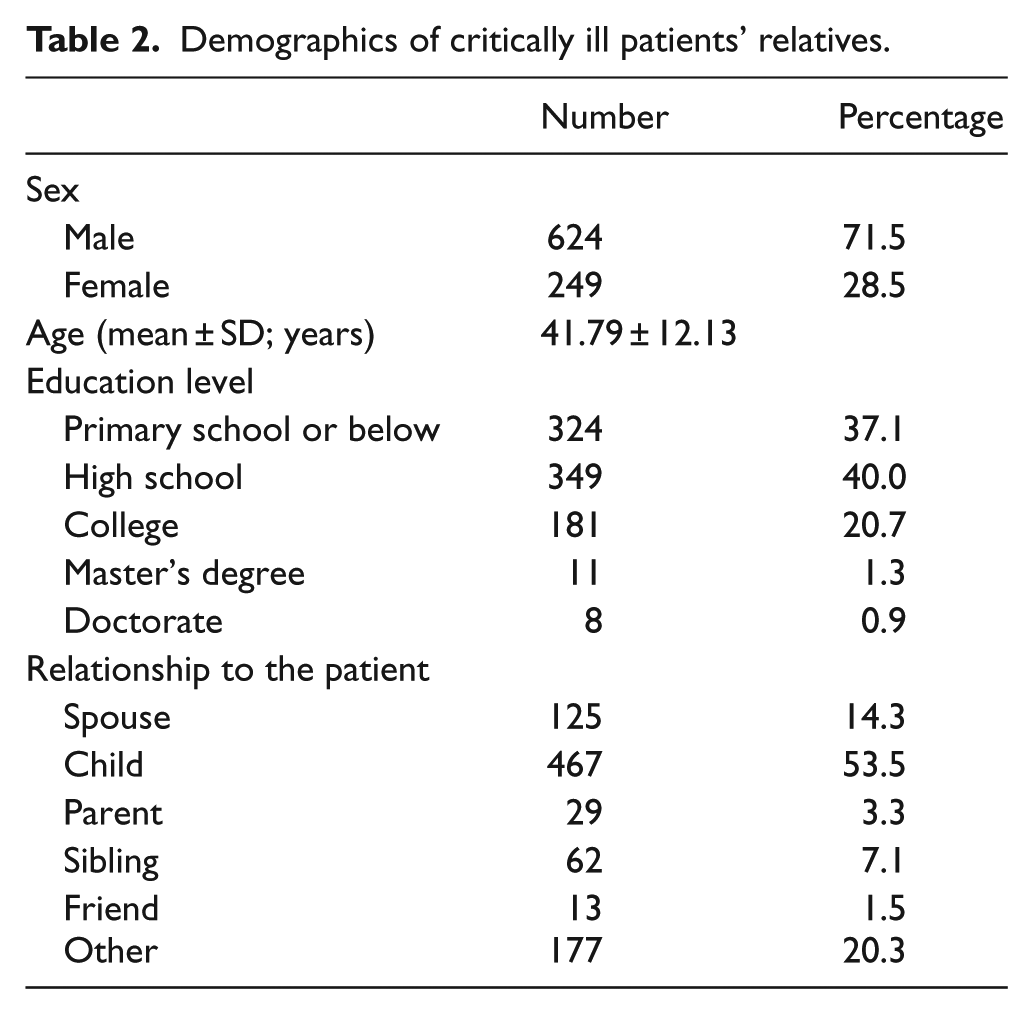
The response rate to the questionnaire was 100% (873/873). Of 873 participants, 249 (28.5%) were female and 624 (71.5%) were male (average age, 41.79 ± 12.13 years). Of participants, 29 (3.3%) were patients’ parents, whereas 62 (7.1%) were siblings, 125 (14.3%) were spouses, 467 (53.5%) were children, 13 (1.5%) were friends, and 177 (20.3%) were others. Of the enrolled participants, 324 (37.1 %) had studied up to primary school or below, and 349 (40%) had a high school education. A total of 20.7% (n = 181) participants had college education. Demographic characteristics of the participants are presented in Table 2.
Demographics of critically ill patients’ relatives.
Main results
In the meaning category, 77.2%–94.6% of the participants responded to the following needs as “very important”: having questions answered honestly (94.6%), being assured that the patient is receiving the best care possible (92.6%), feeling that the hospital staff cares about the patient (91.8%), knowing specific facts concerning the patients’ progress (90.0%), being informed about the expected outcome (88.2%), being treated as an individual (84.0%), knowing why things are being done for the patient (83.3%), feeling that there is hope (77.2%), and being informed about religious services (49.3%). The average number of points for this category was 3.75 ± 0.30 (range, 3.71 ± 0.59–3.94 ± 0.28).
In the proximity category, 88.8%–43.2% of the participants rated the following needs as “very important”: being informed about transfer plans while they are being made (97.7%), observing what is happening to the patient (70.9%), seeing the patient as soon as possible (68.7%), being with the patient at any time (55.1%), and staying out of the way during the patient’s care (43.2%). The average number of points for this category was 3.51 ± 0.46 (3.08 ± 0.97–3.85 ± 0.44).
In the comfort category, 45.8%–91.1% of the participants rated the following needs as “very important”: being assured of the patient’s comfort (91.1%), having toilet facilities near the waiting room (80.9%), feeling accepted by the hospital staff (74.6%), having a telephone near the waiting room (68.5%), having a private place to wait (60.9%), and having food and refreshments nearby (45.8%). The average number of points for this category was 3.56 ± 0.46 (3.12 ± 0.99–3.89 ± 0.38).
In the communication category, 55.4%–91.8% of the participants rated the following needs as “very important”: being informed about the patient’s condition and treatment in understandable terms (91.8%), talking to a doctor (91.5%), being regularly updated (85.3%), being informed of the patient’s condition before being asked to sign papers (82%), being included in decisions regarding the patient’s care (76.3%), being able to contact staff at a later date to ask questions (69.2%), feeling helpful to the patient’s care (67.8%), being spared distressing details about the patient’s illness (67.1%), feeling comfortable about the expertise of the staff caring for the patient (55.4%), having time alone with the patient (54.8%), and talking to a nurse (40.8%). The average number of points for this category was 3.57 ± 0.38 (3.08 ± 0.94–3.89 ± 0.38).
In the support category, 28.8%–83.5% of the participants rated the following needs as “very important”: having a doctor or a nurse meet them on arrival at the hospital (83.5%), being given instructions regarding what to do at the bedside (75.6%), having a staff member with them while visiting their relative (73.4%), having one designated person to care for the family (73.4%), receiving explanations about the treatment area before going in to see the patient for the first time (65.6%), being reassured regarding the normal emotional responses to expect (47.9%), being encouraged to express emotions (44.6%), sharing emotions with staff (28.9%), and having friends and relatives while in the ED (28.8%). The average number of points for this category was 3.21 ± 0.53 (2.59 ± 1.15–3.73 ± 0.67).
The distribution of answers given to the following questions was statistically significant according to sex: Having a staff member with them while visiting their relative, being informed of the patient’s condition before being asked to sign papers, having friends and relatives while in the ED, having a private place to wait, being updated regularly, knowing why things are being done for the patient, talking to a doctor, talking to a nurse, being confident about the expertise of the staff assigned for the patient, being informed about the expected outcome, having questions answered honestly, staying out of the way during the patient’s care, seeing the patient as soon as possible, receiving explanations about the treatment area before going in to see the patient for the first time, having a staff member with them while visiting the patient, observing what is happening to the patient, being with the patient at any time, being given instructions regarding what to do at the bedside, feeling helpful to the patient’s care, being included in decisions made about the patient, having time alone with the patient, being treated as an individual, being encouraged to express emotions, feeling that there is hope, having food and refreshments nearby, having a telephone near the waiting room, and having toilet facilities near the waiting room (p < 0.05). The percentage of female relatives answering all of the questions above as “very important” was higher than male relatives. There was no statistical difference between the distributions of answers to other questions according to sex (p > 0.05).
The distribution of answers given to the following questions was statistically significant according to educational status: Having a doctor or a nurse meeting them on arrival at the hospital, having a staff member with them while visiting their relative, having friends and relatives with them while in the ED, being informed about the patient’s condition and treatment in understandable terms, being spared distressing details about the patient’s illness, staying out of the way during the patient’s care, being with the patient at any time, feeling helpful to the patient’s care, having time alone with the patient, feeling accepted by the hospital staff, being encouraged to express emotions, being reassured regarding the expected normal emotional responses, sharing emotions with staff, being informed about religious services, having food and refreshments nearby, having a telephone near the waiting room, having toilet facilities near the waiting room, and being able to contact staff at a later date to ask questions (p < 0.05).
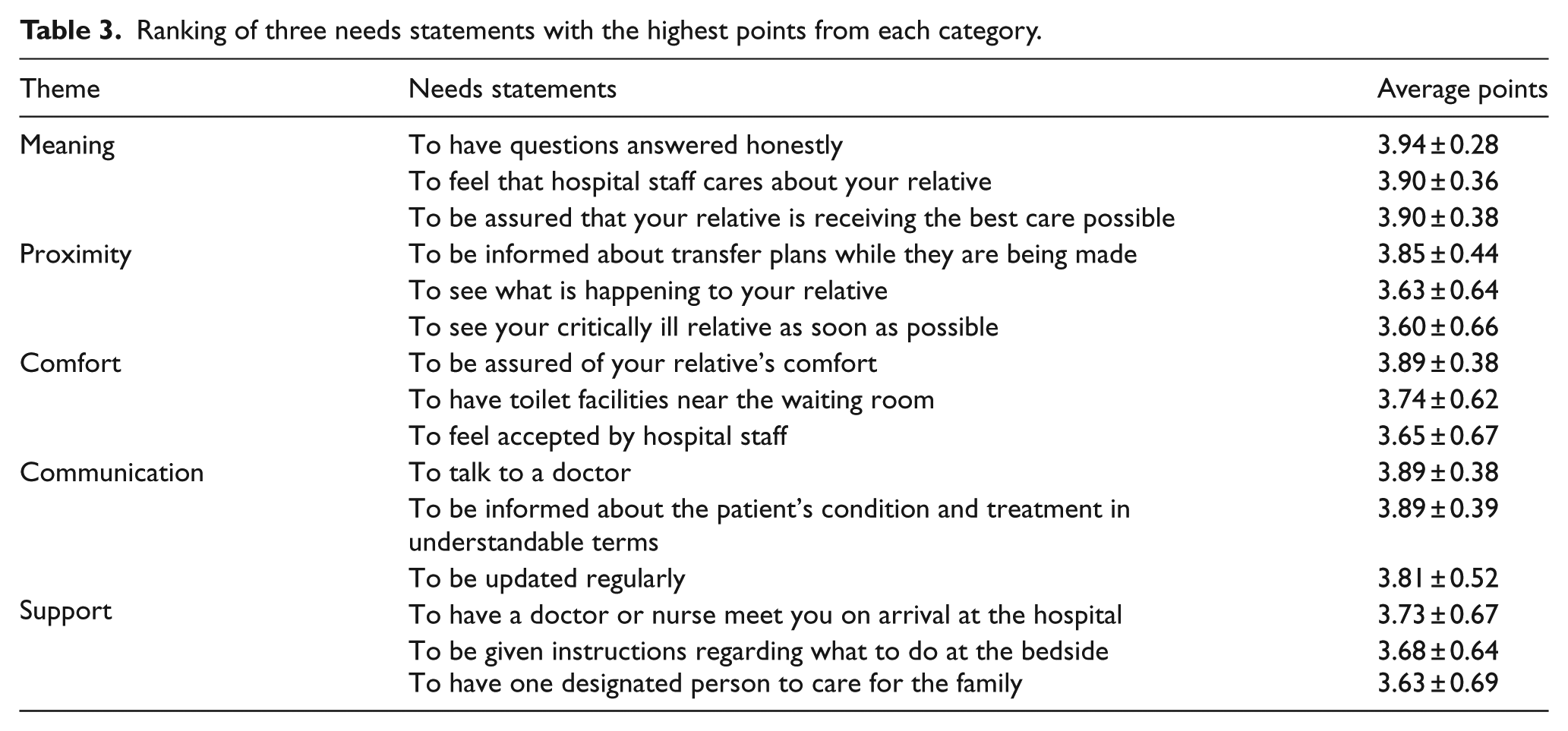
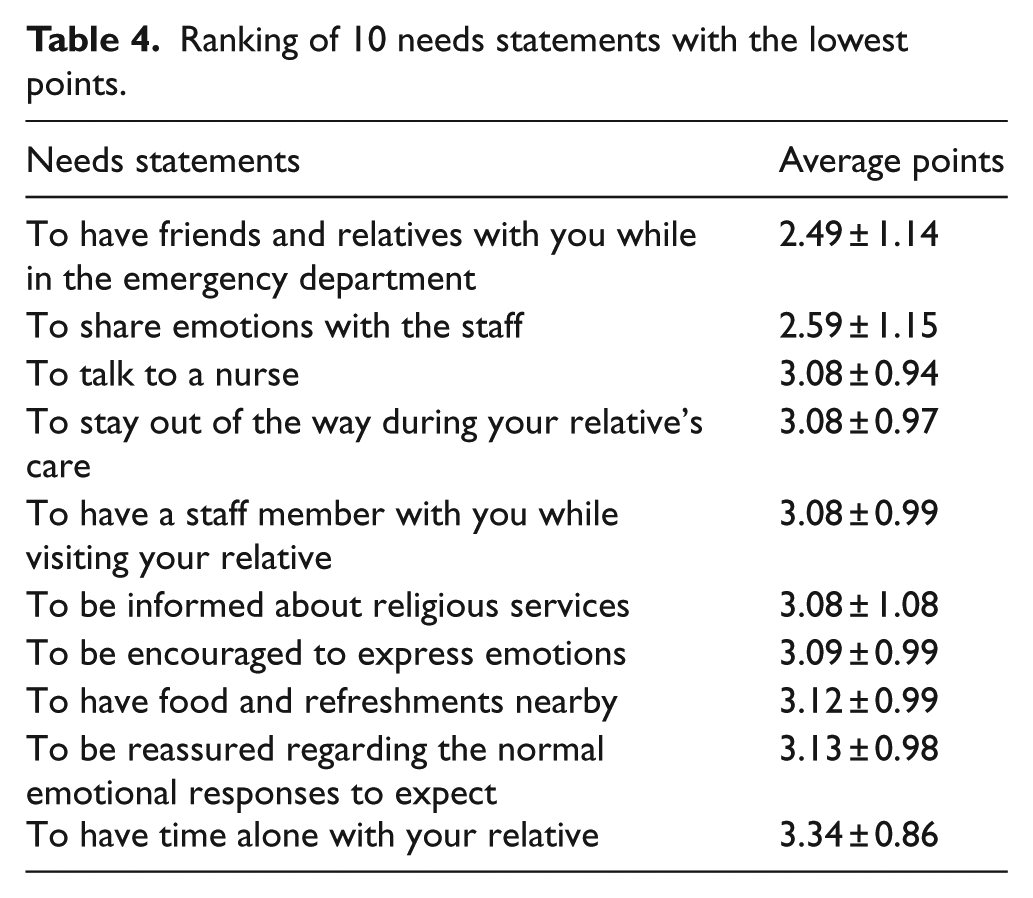
The 3 most important needs from each category and the 10 least important needs according to the average number of points are summarized in Tables 3 and 4, respectively. The total average number of points for each category is shown in Figure 1.
Ranking of three needs statements with the highest points from each category.
Ranking of 10 needs statements with the lowest points.
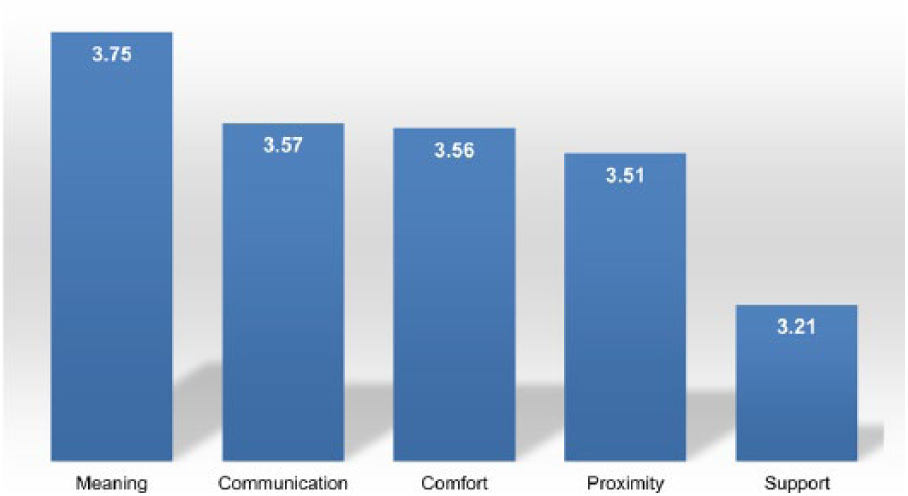
Average points of each need category in decreasing order of frequency.
Discussion
Focusing on patients is the fundamental duty of ED operations. In addition, considering and meeting the expectations and needs of patients’ relatives is an important component and indicator of overall services. 19 Meeting these needs, which are already the rights of the patients’ relatives, will give them a positive impression of the healthcare institution.20,21 Therefore, this subject should be regularly addressed both in fundamental medical education and in-service training. 22 The expectations and needs become more important when relatives of critically ill patients are considered15,23 as they are generally overlooked. 24
Our findings indicate that “meaning” category was given the highest priority by relatives of critically ill patients in the ED, followed by “communication,” which is consistent with previous ICU and ED-based studies.8,15,18,25 In decreasing order of frequency, comfort, proximity, and support categories were considered less important than the aforementioned categories.
In the meaning category, the need for honest answers to questions was the most important need as per participants, which is consistent with the literature.18,26,27 Moreover, feeling that the hospital staff cares about the patient and being assured that the patient is receiving the best care possible were the most important needs of relatives in this category. In addition, knowing specific facts regarding the patient’s progress and the expected outcome were important to the families, which might be a result of the relatives not being allowed in the care area with the patient in most EDs during procedures in order to avoid possible distressing or uncomfortable situations for the relatives. Due to their feelings of fear, distress, and worry, patients’ families need honest and clear answers from healthcare workers regarding the condition and treatment course of the patient.4,8,15,18,28 Interestingly, being informed about religious services was found to be one of the least important needs in our study. Although consistent with previous studies,7,18,29,30 this result could mean that the patients’ families, even traditional families in Turkey, put their own needs behind the patients’ needs.
Communication was considered as the second most important need in our study, while proximity was considered as the fourth. We believe that these needs should be evaluated together since the relatives of critically ill patients feel that they are supporting their family members by being physically close to them as they try to alleviate their feelings of desperation and loss of control. 31 Therefore, the family’s need to be close to the patient is analogous with the need for direct, accurate, and proper communication from the healthcare staff and vice versa. Evaluating needs in detail according to the needs statements revealed that being informed about transfer plans while they are being made is one of the most important needs of the relatives of critically ill patients in the ED. When discharging is impossible and ICU beds are unavailable or when further treatment cannot be provided due to inadequate equipment or staff, the ED staff is obligated to transfer the patient to another facility. Unfortunately, transferring patients to a distant facility may increase the families’ stress, despair, feeling of uncertainty, and loss of control especially in those with low socioeconomic status. Because talking to a doctor is one of the most important needs in the communication category and being updated regularly in understandable terms, while talking to a nurse is one of the least important, being regularly informed by the physician in charge regarding the patient’s condition and possibilities of transfer to another facility early in the care cycle would clear family members’ minds, provide relief of uncertainty, or provide them enough time to make arrangements, which will in turn decrease their stress and anxiety. Since observing what is happening to the patient and seeing the patient soon after the procedure are the other most important features of proximity needs of relatives of critically ill patients in the ED, understanding and meeting the need for families to see patients as quickly as possible would also decrease the anxiety and stress of relatives while positively affecting staff–family relations.
Although providing both physical and emotional comfort is important in relieving patients’ families of distress, anxiety, and sadness, 15 in this study, the comfort category was given less importance than being informed about the patient’s condition and being assured that the patient is properly cared for. These results are consistent with previous studies.7,8,15,18,28,32 Relatives of critically ill patients in our study felt that being assured of the patient’s comfort was the most important need in this category. In addition, participants stated that they valued the feeling of being accepted by the hospital staff, which means that they should be regarded as an inseparable component of the patient. Having toilet facilities near the waiting room was also important for family members, while having food and refreshments nearby was considered as one of the least important needs, further suggesting that relatives of critically ill patients eschew their own basic needs such as food and drinks for the need and care of the patient; this is probably due to their feelings of desperation and uncertainty regarding the patient. However, our results indicate that providing physical comfort to meet the relatives’ daily personal needs and providing a feeling of acceptance, which meets their emotional need for comfort, are highly expected.
The support category was given the lowest priority by relatives of critically ill patients, which is consistent with the literature.18,32 Having a doctor or nurse meeting them on arrival was rated as the most important need in this category. Since most patients present to EDs due to acute, serious, or even life-threatening clinical problems, relatives of critically ill patients may feel that being met by a member of the hospital staff will save time especially when filling out paperwork. When a nurse or doctor meets the patient upon arrival, their first observation of the patient may reveal valuable information about the clinical problem. Importantly, this need is met worldwide during the triage process by prioritizing patients’ treatments, which are determined according to the severity of their condition. Reportedly, another explanation to this need might be due to the importance of receiving support from available health professionals. 33 Being given instructions regarding what to do at the bedside and having one designated person to care for the family were considered the other most important needs in the support category. Having friends and relatives with them while in the ED was the least important overall needs in our study. Since almost 80% of the relatives arriving to the ED with the patient were nuclear family members such as parents, children, spouses, and siblings; the participants in our study ranked the presence of other family members and friends as less important. Supportive features such as sharing emotions with the staff, being encouraged to express emotions, and being reassured regarding the normal emotional responses were considered as least important needs, further supporting relatives’ desire to focus on the needs of their critically ill family member.
In our study, female relatives and those with lower educational status were found to be more sensitive regarding most needs, which implies that such relatives have more uncertainty and anxiety and thus feel more need for the support, understanding, and trust of the healthcare staff. Similarly, by increasing the education level, it may be speculated that the expectations and needs of critically ill patients’ relatives might be decreased; however, further studies on this aspect are warranted.
Studies assessing the expectations and needs of relatives of critically ill patients being treated in the ED are limited. Moreover, most of these studies are conducted by nurses who are key players in the healthcare system, especially in the ED where doctors are racing against time.4,7,18,30,34 Family members are a major source of social support and play a crucial role in managing and assisting in recovery of critically ill patients.35,36 Therefore, detailed and accurate communication by healthcare providers with family members may facilitate recovery by providing families’ with absolute cooperation during the treatment process. Thus, creating a positive interaction based on trust and providing a healthcare environment where expectations and needs of relatives are met should be among the top priorities of ED staff while caring for critically ill patients. To be noted, strategies focusing on the overcrowding in the EDs, thus increased length of stay which is one of the most important causes of dissatisfaction, would also help create solutions regarding patients’ and relatives’ satisfaction.2,3 Although these strategies are beyond the scope of this article, we believe giving priority to “communication” need may meet majority of the expectations of patient relatives’ even in cases of problems including overcrowding, boarding, insufficient manpower and shortage of ICU beds. Based on our daily practice experiences, we advocate that supplementary personnel who are well trained in public relations would further assist the communication need particularly in overcrowded ERs.
To our knowledge, this study, which was conducted by face-to-face interview with an ED physician, has the largest number of participants including those in both ICU- and ED-based studies among the literature examining the expectations and needs of relatives of critically ill patients. However, further comparative studies are warranted to examine the specific expectations of families from ED doctors, nurses, and other staff as well as the roles of staff in meeting the families’ needs.
Conclusion
Satisfaction of patients’ relatives is one of the quality indicators of service provided in the ED. In this study, patient-focused needs were highly prioritized by relatives of critically ill patients in the ED rather than their own personal needs. The results of this study may help ED physicians realize their mission and responsibilities in developing methods for patients’ and families’ satisfaction while improving the quality of service in the ED. We believe that this study will contribute toward ED physicians’ ability to see this side of the service and consider these components as a whole since stressful and anxious family members can contribute to an unfavorable healthcare environment, making it impossible to provide the best possible care to patients.
Limitations
There are several limitations in this study. First, the data were collected at one time point within the ED since this was a cross-sectional study. Thus, the study did not consider the expectations and needs of the relatives after the patients’ discharge or transfer from the ED. In addition, the exclusion of the relatives of the traumatic critically ill patients might have introduced a response bias in this study. These limitations could be overcome by categorizing and further comparing the family needs of traumatic and nontraumatic patients as well as needs of patients arriving to the ED for the first time and of those who experience multiple admissions for the same reason. Moreover, families’ perception of needs may have been affected by the type and severity of the clinical scenario, including the possibility of mortality or serious morbidity as well as acute diseases or the acute exacerbations of chronic diseases. In addition, although our results seem not to be suitable to be generalized as the survey tool was based on Turkish, similar results in previous studies disclose the prevalent feelings of humanity and being a family regardless of their religion, language, and area of the world.
Footnotes
Acknowledgements
This manuscript has been carefully reviewed and edited by a professional editing company experienced and specialized in editing papers written by scientists whose native language is not English. U.O. and L.A. conceived and designed the study. U.O. conducted the trial, collected, and analyzed the data. U.O. drafted the manuscript. U.O. takes responsibility for the paper as a whole. The results of this study were presented as “podium presentation” in the 9th National Congress of Emergency Medicine, Eskisehir, Turkey, 2–6 October 2013.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the participants for their anonymized information to be published in this article.