
Abstract
Background and Objectives:
There is currently no consensus on the criteria for admitting older adults to the intensive care unit.
Methods:
This single-center retrospective study evaluated the baseline and clinical characteristics of older adults admitted to the intensive care unit between January 2017 and June 2017; patients were analyzed according to their age group. Factors associated with in-hospital mortality were specifically determined using logistic regression analysis.
Results:
Among 582 patients included in the present study, 34.2%, 46.6%, and 19.2% were aged 65–74, 75–84, and over 84 years, respectively. In terms of clinical outcomes, although there were no significant differences in the length of intensive care unit and hospital stay and intensive care unit mortality, significant differences were observed in terms of in-hospital mortality, hospital discharge disposition, and neurologic outcomes at discharge (p = 0.039, p = 0.005, and p = 0.032, respectively). Predictive factors for in-hospital mortality were age (⩾85 years), initial mental status (stupor to coma), a Korean Triage and Acuity Scale level of 1, underlying diagnosis of cancer, abdominal pain or discomfort, apnea, and a chief compliant of dyspnea.
Conclusion:
Compared to those aged 65–84 years, in-hospital mortality was 1.96-fold higher in those aged over 84 years. However, the overall mortality in our cohort was not considerably different from that of the younger population. Intensive care unit admission should be considered in selected older adults after evaluating the risk factors for mortality.
Introduction
The intensive care unit (ICU) is a facility for the advanced monitoring and treatment of critically ill patients with rapidly deteriorating clinical parameters. As the population is aging, the demand for medical resources continues to rise, and the numbers of older patients hospitalized in the ICU are increasing. However, there is still no consensus among clinicians on the criteria for admission of older patients to the ICU. Many clinicians are reluctant to admit them to the ICU, arguing that intensive care treatment may not be preferred by the patient or family and that the admission and treatment reduces the efficiency of social and medical resources. Conversely, other clinicians strongly advocate ICU admission for selected older adults. This inconsistency results from the lack of proven criteria to correctly identify patients who may optimally benefit from ICU care. 1 In particular, chronic health problems and serious illnesses among older patients admitted to the ICU through the emergency room (ER) make it difficult for clinicians to make decisions on admission to the ICU. However, clinical data and research on these older patients, who are hospitalized in the ICU through the ER, are scarce. In the present study, we evaluated the baseline and clinical characteristics of older patients who were admitted to the ICU through the ER, based on their age groups; factors associated with in-hospital mortality were also investigated.
Methods
Study design and patient selection
This study was approved by the Institutional Review Board of our institution. Owing to the purely observational, retrospective, and non-interventional nature of the study, informed consent was deemed unnecessary and not obtained. Our emergency center is a regional emergency center of the Republic of Korea. An estimated 73,000 patients annually visit our emergency center, of whom 11,000 are over the age of 65 years. Elderly patients over the age of 65 years admitted to the ICU through the ER from January 2017 to June 2017 were enrolled. We excluded subjects whose medical records were not available for privacy applications (only two cases in the study period). The enrolled patients were divided into three age groups for analysis: between 65 and 74 years (group aged 65–74 years), between 75 and 84 years (group aged 75–84 years), and ⩾85 years (group aged over 84 years). As of 2017, the age standard to qualify for receiving welfare benefits as an elderly person in Korea was 65 years. In 2017, there were social discussions around raising this age standard. In connection with this issue, we planned to investigate the baseline and clinical characteristics of elderly patients admitted to the ICU through the ER, based on these age groups. We analyzed the data for the first half of 2017 during the second half of 2017. In our hospital, ICU admission priority is based primarily on protocols, but the final decision is made by ICU staff.
Data collection
Electronic medical records of enrolled patients were reviewed. Baseline characteristics (sex, age, insurance status, time of arrival, admission source, and trauma versus non-trauma), underlying disease, Charlson Comorbidity Index (CCI), chief complaint, vital signs, initial mental status, the Korean Triage and Acuity Scale (KTAS) level, discharge diagnosis, and clinical outcomes (length of stay (LOS), in-hospital and ICU mortality, hospital discharge disposition, and neurological outcome at discharge) were obtained and evaluated retrospectively. KTAS is a triage tool of the Korean emergency system. In 2012, the Korean Society of Emergency Medicine developed KTAS by modifying the Canadian Triage and Acuity Scale (CTAS), a Canadian emergency patient classification tool, to suit the medical conditions in Korea. Since 2016, KTAS has been introduced at regional, local, and professional emergency centers nationwide, and the severity of illness in patients is evaluated based on KTAS criteria. In studies by Choi et al. 2 and Lim et al., 3 KTAS was shown to be effective in classifying the severity of illness in relation to the patient’s clinical outcome.
Statistical analyses
The normality of data distributions was evaluated using the Kolmogorov–Smirnov test to select the appropriate parametric and non-parametric statistical methods. Categorical variables were analyzed using the chi-square or Fisher’s exact tests. Continuous variables were expressed as medians (25th–75th percentile) and were analyzed using the Mann–Whitney U test and Kruskal–Wallis test. Independent risk factors associated with in-hospital mortality in patients who were admitted to the ICU through the ER were evaluated using multivariate backward stepwise logistic regression, after adjustment for confounding factors (defined as factors found to be significant on univariate analysis, based on a type I error of 0.05). Logistic regression analysis was conducted for the variables of age (⩾85 years), initial mental status (stupor to coma), and KTAS level (1). Subsequently, the performance of age ⩾85 years in predicting in-hospital mortality was evaluated. For all comparisons, tests were two tailed and group differences were regarded as statistically significant when p values were less than 0.05. The SPSS version 18.0.0 statistical software package for Windows (SPSS, Inc., Chicago, IL) was used for all analyses.
Results
Baseline and clinical characteristics of patients according to age group
Among 582 patients included in the present study, 34.2%, 46.6%, and 19.2% of the study population comprised patients aged 65–74, 75–84, and over 84 years, respectively. Among the patients included in the group aged over 84 years, seven patients were aged over 95 years (data not shown). The patients’ baseline characteristics have been summarized in Table 1. Although no significant differences were observed in terms of health insurance, time of arrival, admission source, and underlying disorders between the three age groups, there was significant difference in terms of sex (male patients in the 65–74, 75–84, and over 84 years of age groups were 62.8% versus 46.9% versus 40.2%, respectively; p < 0.001). In terms of comorbidities or underlying diseases, the older group had higher rates of hypertension, dementia, and chronic heart disease (p = 0.005, p < 0.001, and p = 0.003, respectively) (Table 2). Diabetes mellitus and dementia were highest in the group aged 75–84 years and were the lowest in the group aged over 84 years. Among the chief complaints, only chest pain or discomfort, and dyspnea were significantly different (p = 0.013 and p = 0.009); chest pain and dyspnea were the highest in the groups aged 65–74 and over 84 years, respectively. In terms of vital signs, there were no statistical differences in systolic and diastolic blood pressure, heart rate, respiratory rate, and body temperature between the three groups; only the oxygen saturation on pulse oximetry showed significant difference (p = 0.048) (Table 3). With respect to the mental status at admission from the ER, alert to drowsy states were more common than stuporous to comatose states. However, there were no statistical differences between the three groups. Although the highest and lowest number of patients in all the three groups had KTAS levels of 2 and 4, respectively, there were no significant differences between the three groups. Table 4 demonstrates the diagnosis at discharge and clinical outcomes of the patients in the individual age groups. In terms of the age group, the diagnosis at discharge showed no statistical differences except for in anaphylaxis and renal disease. With respect to clinical outcomes, although there were no significant differences in the length of ICU and hospital stay, and ICU mortality, significant differences were observed in terms of in-hospital mortality, hospital discharge disposition, and neurologic outcomes at discharge (p = 0.039, p = 0.005, and p = 0.032, respectively). Those aged over 84 years had the highest in-hospital mortality and lowest cerebral performance category scores.
Baseline characteristics of patients according to age group.
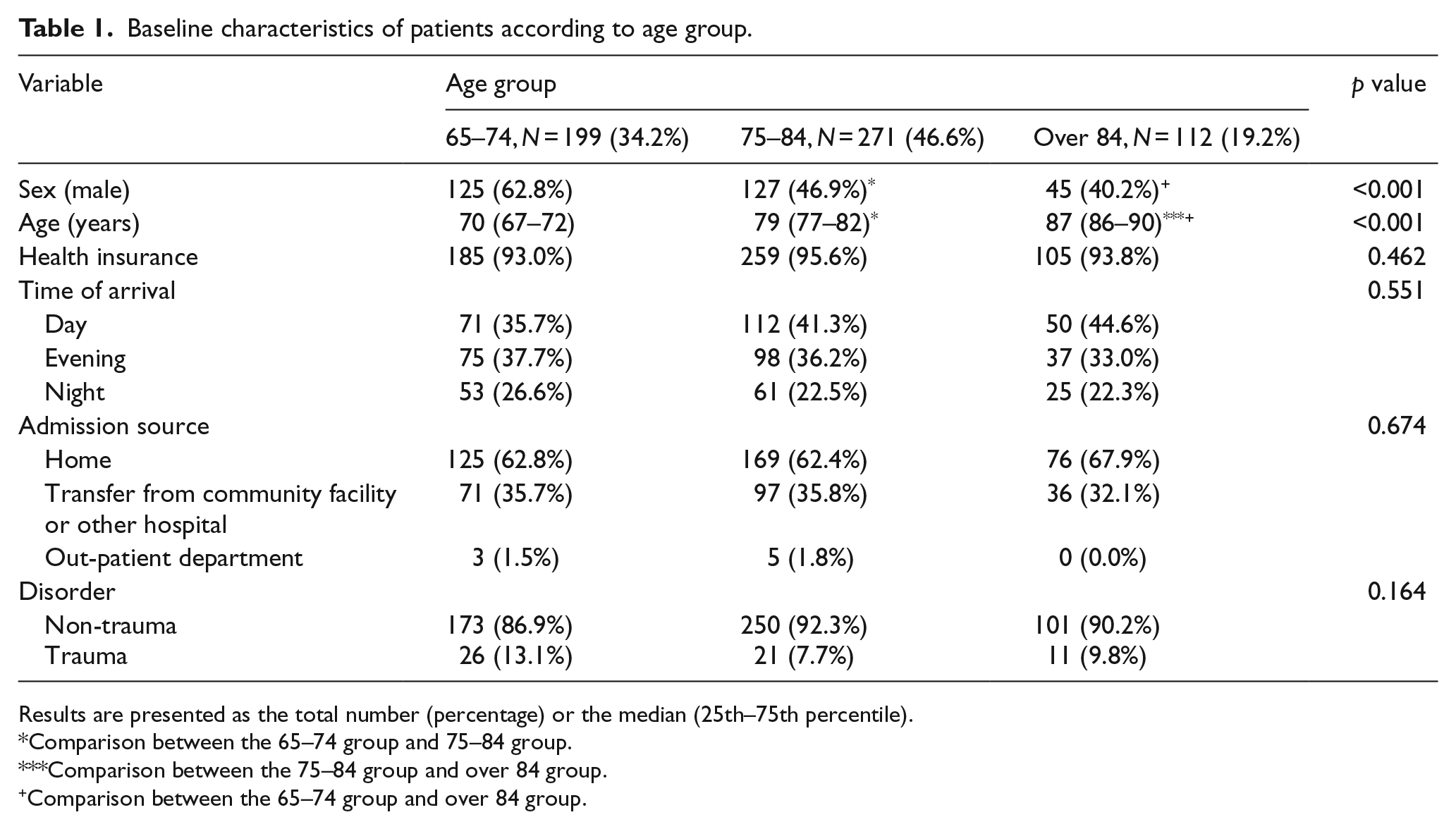
Results are presented as the total number (percentage) or the median (25th–75th percentile).
Comparison between the 65–74 group and 75–84 group.
Comparison between the 75–84 group and over 84 group.
Comparison between the 65–74 group and over 84 group.
Underlying diseases and chief complaints of patients according to age group.
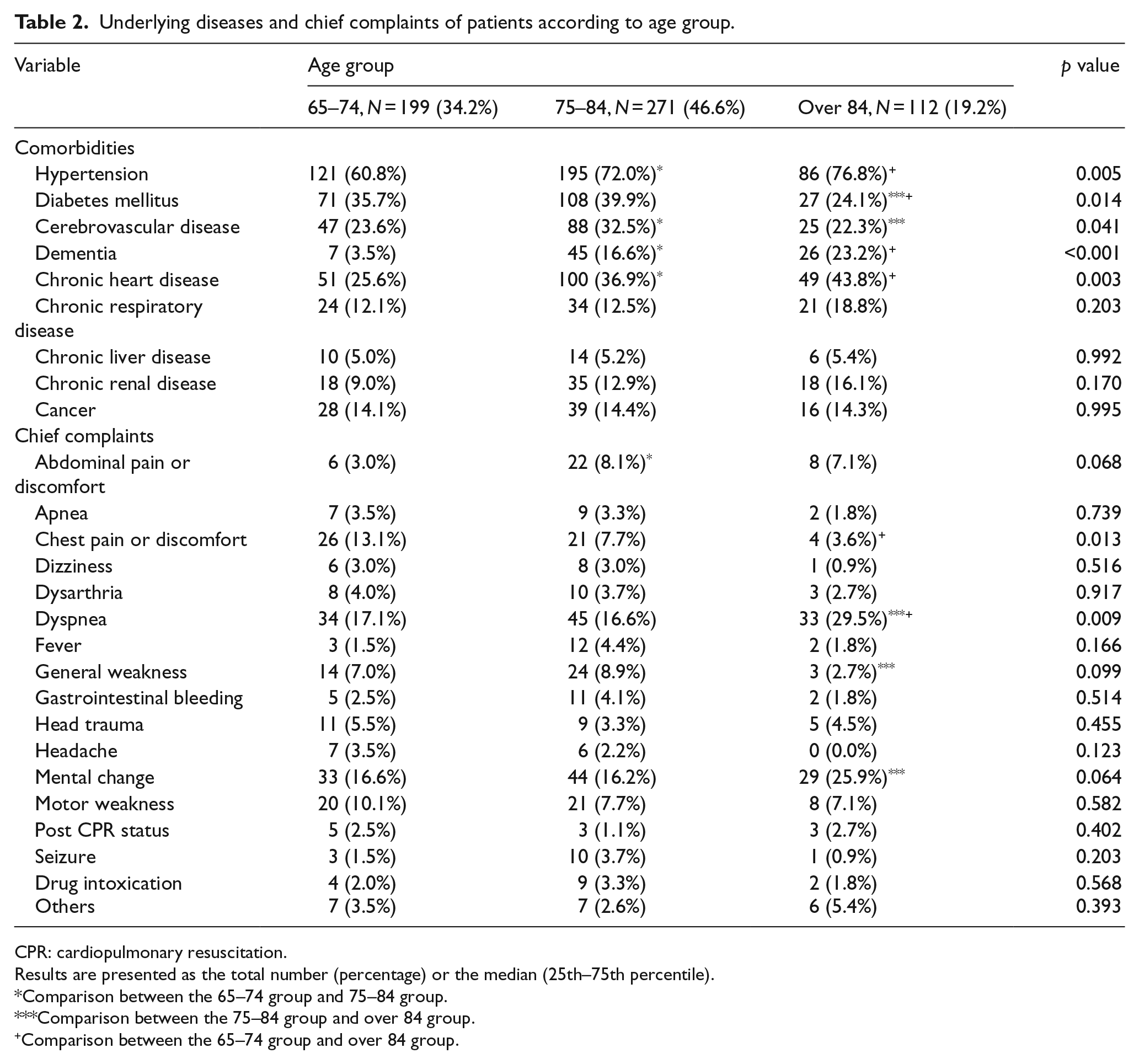
CPR: cardiopulmonary resuscitation.
Results are presented as the total number (percentage) or the median (25th–75th percentile).
Comparison between the 65–74 group and 75–84 group.
Comparison between the 75–84 group and over 84 group.
Comparison between the 65–74 group and over 84 group.
Vital sign and KTAS level of patients according to age group.
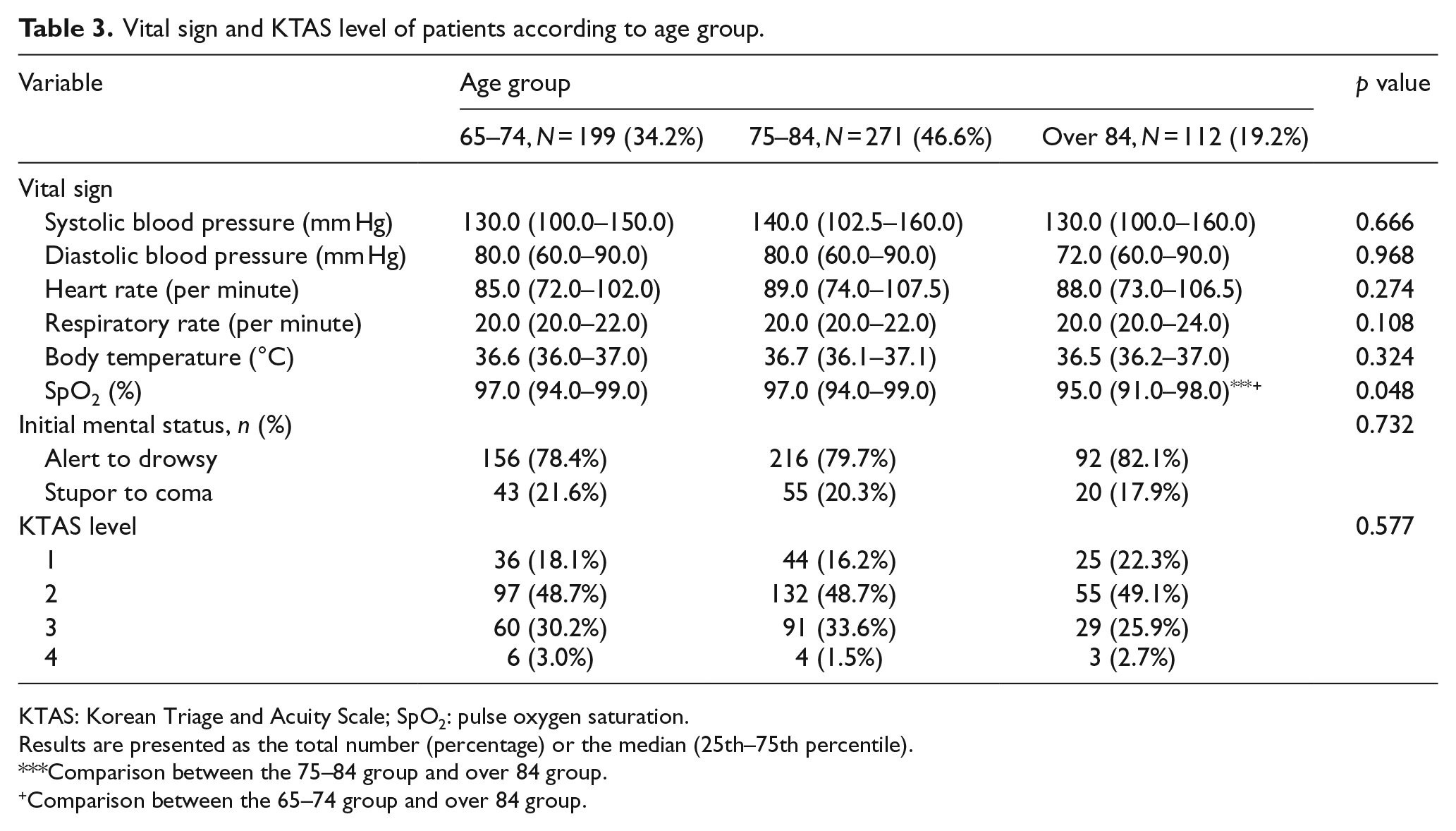
KTAS: Korean Triage and Acuity Scale; SpO2: pulse oxygen saturation.
Results are presented as the total number (percentage) or the median (25th–75th percentile).
Comparison between the 75–84 group and over 84 group.
Comparison between the 65–74 group and over 84 group.
Discharge diagnosis and clinical outcome of patients according to age group.
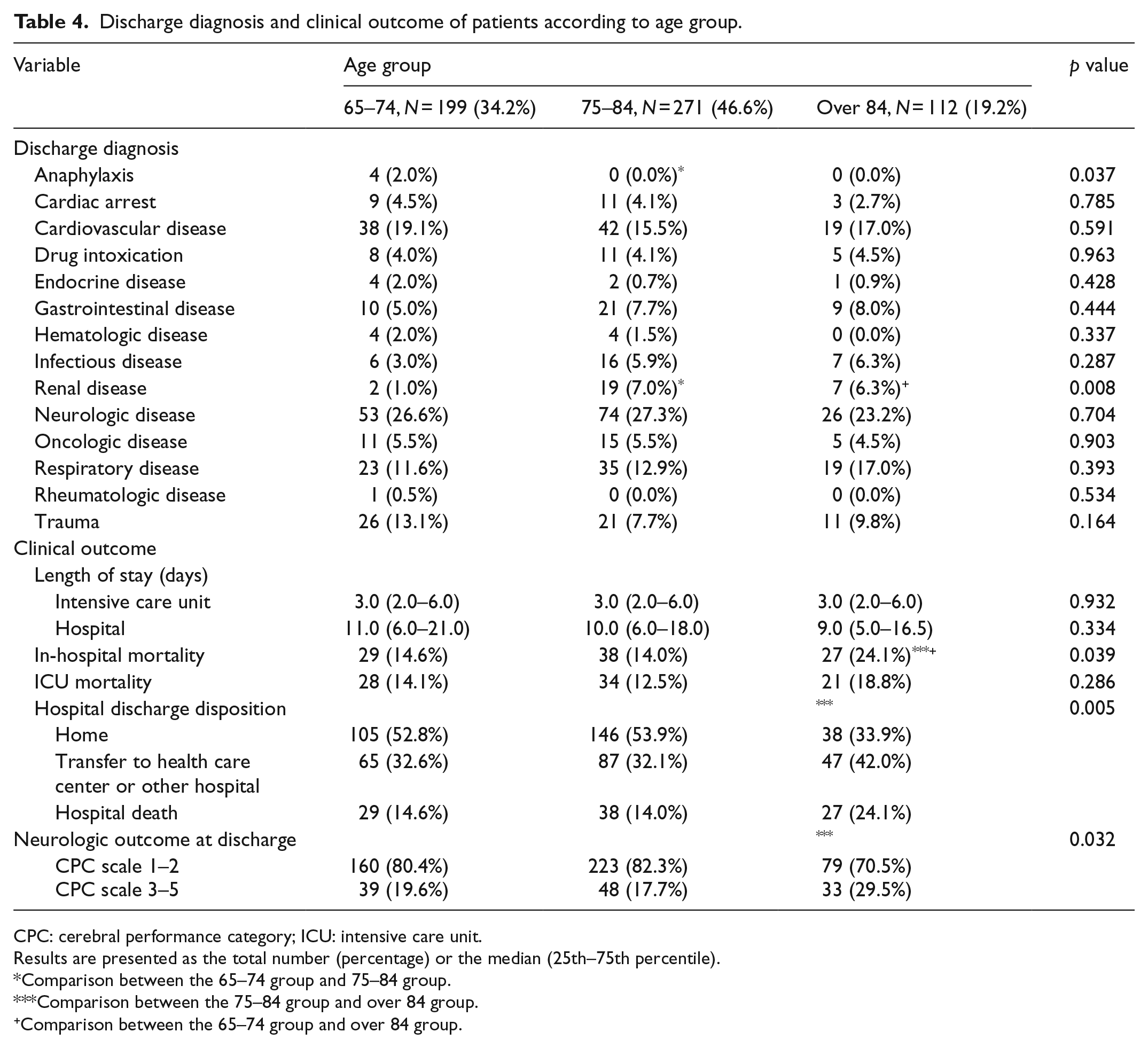
CPC: cerebral performance category; ICU: intensive care unit.
Results are presented as the total number (percentage) or the median (25th–75th percentile).
Comparison between the 65–74 group and 75–84 group.
Comparison between the 75–84 group and over 84 group.
Comparison between the 65–74 group and over 84 group.
Predictive factors for in-hospital mortality
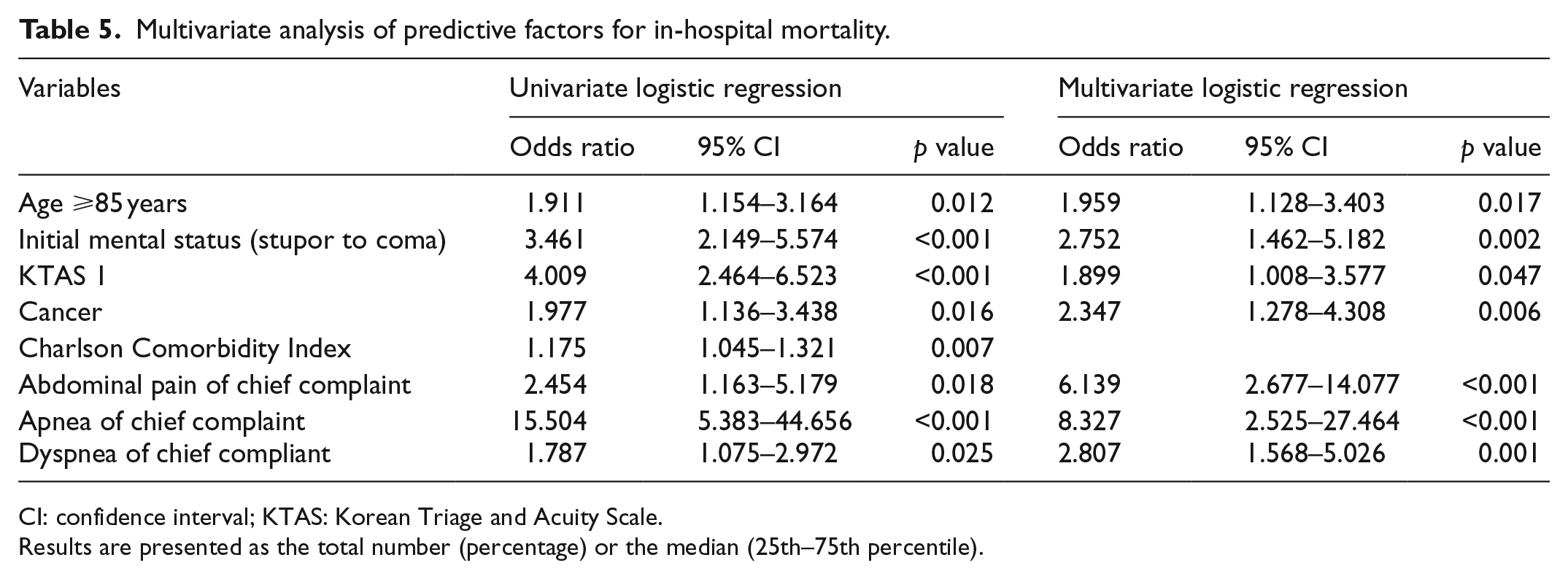
On multivariate logistic regression analysis, age (⩾85 years; odds ratio (OR): 1.959, 95% confidence interval (CI): 1.128–3.403, p = 0.017), initial mental status (stupor to coma; OR: 2.752, 95% CI: 1.462–5.182, p = 0.002), KTAS level of 1 (OR: 1.899, 95% CI: 1.008–3.577, p = 0.047), underlying diagnosis of cancer (OR: 2.347, 95% CI: 1.278–4.308, p = 0.006), chief complaint of abdominal pain or discomfort (OR: 6.139, 95% CI: 2.677–14.077, p < 0.001), apnea (OR: 8.327, 95% CI: 2.525–27.464, p < 0.001), and chief compliant of dyspnea (OR: 2.807, 95% CI: 1.568–5.026, p = 0.001) had sufficient statistical power to discriminate in-hospital mortality (Table 5). The performance of age ⩾85 years is shown in Table 6 (sensitivity 28.7%, specificity 82.6%, positive predictive value 24.1%, negative predictive value 85.7%, and accuracy 73.9%).
Multivariate analysis of predictive factors for in-hospital mortality.
CI: confidence interval; KTAS: Korean Triage and Acuity Scale.
Results are presented as the total number (percentage) or the median (25th–75th percentile).
Performance of age 85 years in the prediction for in-hospital mortality.

Sensitivity 28.7%, specificity 82.6%, positive predictive value 24.1%, negative predictive value 85.7%, and accuracy 73.9%.
Discussion
In the present study, significant differences were observed in terms of in-hospital mortality, hospital discharge disposition, and neurologic outcomes at discharge. Predictive factors for in-hospital mortality were age (⩾85 years), initial mental status (stupor to coma), a KTAS level of 1, an underlying diagnosis of cancer, abdominal pain or discomfort, apnea, and a chief compliant of dyspnea.
Baseline and clinical characteristics of older adults in our cohort
Our results show that the number of older adults who were admitted to the ICU through the ER was higher in the 75- to 84-year group (46.6%) compared to the 65- to 74-year group (34.2%). However, the numbers declined in the group aged over 84 years (19.2%). The proportion of men in the group aged 65–74 years (65.2%) was higher than that of other groups (46.9% and 40.2%, respectively). These results may be explained by data from the Korean Statistical Information Service (KOSIS). In 2017, KOSIS showed an average life expectancy of 82.7 years (79.7 and 85.7 years for male and female individuals, respectively). Consequently, the number of older patients who were admitted to the ICU showed trends of rise and fall according to the life expectancy. In males, the death rate in the 75- to 85-year group was higher than that of females (25.1% versus 14.7%). Fuchs et al. 4 reported similar proportions in the United States. The number of older patients who were admitted to the ICU increased from the 65–74 years (35.6%) to the 75–84 years (41.3%) groups and declined in the group aged over 84 years (23.1%). The proportion of men in the group aged 65–74 years (53.7%) was higher than that of the other groups (49.7% and 39.4%, respectively). With respect to comorbidities or underlying diseases, Fuchs et al. 4 also demonstrated that the older group had higher rates of hypertension and chronic heart disease; the incidence of diabetes mellitus was highest in the group aged 75–84 years and was lowest in the group aged over 84 years. The oxygen saturation in the group aged over 84 years was significantly lower than that of the other groups; this may have been related to the significantly larger number of patients with complaints of dyspnea in this group. Although there were no significant differences in the KTAS level between the age groups, 14 patients in this cohort were classified as level 4 on initial assessment. Even if the initial triage is classified as for minor patients, careful physical examination and observation of progress is essential in older patients, who are unable to actively express worsening of symptoms.
Clinical outcomes and predictive factors for in-hospital mortality
Patients aged 65 years or older who are admitted to the ICU have an average LOS of 2–5 days and 7–10 days in the ICU and hospital, respectively.4–6 The present study showed similar results (an average LOS of 3 and 10 days for the ICU and hospital, respectively). The average ICU and in-hospital mortality has been reported to be 13.1%–32% and 22.8%–38.1%, respectively.4–8 The ICU and in-hospital outcomes in our cohort were better than that of previous studies (14.3% and 16.2%). We speculate that there are several reasons for the lower ICU and in-hospital mortality in our cohort. First, the entire population of the Republic of Korea is covered by the national health insurance system. Most of the people receive adequate medical benefits. Second, compared with the studies by Vosylius et al., 6 Fuchs et al., 4 and Sim et al. 5 (1998–2000, 2001–2008, and 2003–2012, respectively), the period of data collection in our cohort was relatively recent. Third, Guidet et al. 8 demonstrated the different outcomes for 30-day mortality according to limitations in treatment (18.5%, 53.1%, and 93.1% in the no treatment limitation, treatment withheld, and treatment withdrawal groups, respectively). In the Republic of Korea, caregivers are reluctant to admit patients with do-not-resuscitate orders to the ICU; therefore, ICU admissions are less likely. In addition, the prevalence of withdrawal of life support is lower in Asia than in the USA or Europe.9,10
Previous studies have demonstrated that age, sex, mechanical ventilation, cardiogenic shock, acute kidney injury, and underlying disease were all associated with poor outcomes in older patients.7,11–14 We intended to find factors affecting in-hospital mortality in the initial situation of the ER. So, rather than the Sequential Organ Failure Assessment (SOFA) or Acute Physiology and Chronic Health Evaluation (APACHE II) scores used in the ICU, we wanted to evaluate mortality through the underlying disease and CCI of the patients. In the present study, age (⩾85 years), initial mental status (stupor to coma), a KTAS level of 1, an underlying diagnosis of cancer, chief complaints of abdominal pain or discomfort, apnea, and chief complaints of dyspnea were predictive factors for in-hospital mortality. In particular, previous studies that evaluated the association between age and ICU outcomes in older patients have shown that the outcomes worsen with increasing age.4,5,15 In the study by Flaatten et al., the 30-day mortality in acute admissions increased 1.19-fold for every 5-year increment in age. Since older patients have a wider variety of underlying diseases compared to younger patients and they lack the physical ability to overcome acute illnesses, mortality rises. In terms of social costs and medical resources, there is a view that intensive care for older patients reduces the efficiency of utilization of resources. However, Zivot et al. 16 suggested that an assumption of poor prognosis in older adults may lead to discrimination. Compared to the 65- to 84-year group, our study showed a 1.96-fold higher mortality in those aged over 84 years. However, the overall mortality (14.3% and 16.2%) in our cohort was not considerably different compared with younger patients admitted to the ICU. 6 We suggest that in older patients, active treatment is necessary if there are indications for ICU admission, particularly, in those aged less than 85 years.
Impaired levels of consciousness may affect the mortality rate since dysfunctions of the central nervous system impair the ability to protect the upper airway; this prolongs mechanical ventilation or possibly introduces new nosocomial infections. 6 Altered mental status is also an important measure of disease severity; a lower level of consciousness at the time of admission may indicate greater severity of disease. 17 In the present study, cancer had a statistically significant impact on hospital mortality. An underlying diagnosis of cancer in older patients may be a considerable risk factor owing to the many treatments, including antibiotics, surgery, or chemotherapy, that the patient has been exposed to. Sim et al. 5 demonstrated that cancer was a baseline and clinical characteristic that affected clinical outcomes. In the study by Soares et al., 18 older age was associated with higher mortality in patients with cancer. Previous studies have rarely explored the impact of chief complaints on the clinical outcomes in older adults. We found that chief complaints of abdominal pain or discomfort, apnea, and dyspnea were predictive factors for in-hospital mortality. Since older patients often present with non-specific and ambiguous symptoms, the possibility of intra-abdominal sepsis or emergent surgery should be considered during evaluation. It is important to elucidate the illnesses in older patients through careful history taking and physical examination, even if they complain of common symptoms. Apnea results from cardiac arrest. These patients are more likely to have hypoxic brain damage and multi-organ failure due to the post cardiac arrest syndrome. Baseline conditions that may cause cardiac arrest have also been considered to influence in-hospital mortality. Dyspnea, the most common complaint in the present study, is associated with various severe conditions such as respiratory, cardiovascular, renal, and infectious diseases.
Our study has several limitations. First, the small number of patients and single-center study design carry inherent risks of bias. Second, our retrospective study design may be associated with selection biases, as this study only included patients already admitted to the ICU. Third, sample size was not calculated because we simply planned to investigate the baseline and clinical characteristics of elderly patients admitted to the ICU through ER, based on the age groups. Fourth, it is likely that bias has already been involved for inpatients admitted to the ICU. Older patients for whom the decision has been made not to admit them to the ICU have a lower level of care compared to those who are admitted to the ICU, which increases their mortality. Moreover, there are more requests to withdraw intensive care from older patients than younger patients. Fifth, long-term prognosis was not investigated. Sixth, we looked at the intuitive factors that help clinicians in the ER, rather than scoring models or severity scores. Therefore, scores such as SOFA or APACHE II could not be analyzed.
Conclusion
There is still no consensus among clinicians on the admission of older patients to the ICU. Compared to those aged 65–84 years, our study showed a 1.96-fold higher in-hospital mortality in those aged over 84 years. However, the overall mortality was not considerably different from the younger population. We suggest that ICU admission should be considered in selected older adults after evaluating the risk factors for mortality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Our data in this manuscript were obtained from older adults admitted to the intensive care unit through the emergency room at Hallym University Sacred Heart Hospital between January 2017 and June 2017. All data regarding this manuscript are available upon request.
Informed consent
This was a retrospective study using medical records. Informed consent was waived by the Institutional Review Board of Hallym University Sacred Heart Hospital.
Ethical approval
The protocol of this study was approved by the research ethics board of Hallym University Sacred Heart Hospital (HALLYM 2019-05-020).
Human rights
This study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s Human Research Committee.