
Abstract
Objective:
(1) To compare adherence of Ministry of Health Singapore Guidelines of Acute Asthma in the emergency department, in data 10 years apart, and ascertain if any difference observed impacted 72-h return rates and (2) to describe enhancement in hospital and community medical services for asthma, and its effect on disposition trends.
Methods:
A retrospective comparison in guideline adherence with regard to systemic steroids administration, anti-cholinergic administration in moderately severe exacerbations and patient education in discharged patients was done. Rates of unscheduled 72-h returns were compared. A description of new community and hospital services was described, and disposition trends were compared.
Results
In total, 630 patients 10 years ago and 635 patients in the current year were studied, after exclusions and systematic sampling applied. Steroid administration improved by 29% (adjusted p < 0.001). Steroids started in the emergency department improved by 43% (adjusted p < 0.001). Ipratropium addition to second nebulizer improved by 63% (adjusted p < 0.001). Patient education improved by 66% (adjusted p < 0.001). Unscheduled 72-h returns rate were unchanged at 4.2% (adjusted p = 0.912). Although there was no significant difference in the admission and discharge disposition (adjusted p = 0.173), there was a trend towards admission to the short stay unit as an admission option and referral to the primary healthcare provider for discharged patients.
Conclusion:
Although guideline adherence improved in the current year, rates of 72-h unscheduled returns were similar. Disposition trends reflected emphasis and availability of healthcare services in the community and hospital.
Introduction
Asthma is a common presenting condition in the emergency department (ED). While there have been appreciable advances in the knowledge of the pathophysiology of asthma and in the construction of guidelines regarding asthma control, there is still evidence of suboptimal asthma control and poor compliance to guidelines. 1
Locally, there have been initiatives to improve asthma care at the national level. Significant enhancements to medical services, both in the community and in the hospital, were introduced. For the emergency physician, the decision-making processes for patient disposition will necessarily evolve.
Objectives
The objectives of the study were twofold in comparing data 10 years apart as follows:
To compare adherence to the asthma guidelines in the same ED and the rates of 72-h unscheduled re-attendances among discharged patients
To describe enhanced medical services to asthma care, and disposition trends among ED patients
Methods
A retrospective review of two sets of medical records, 10 years apart (in 2003 and 2013), each covering a 12-month period, was done. Patients above age 12 with diagnosis code ‘493 Asthma’ were shortlisted. Based on statistical calculations (in ‘Statistics’), systematic sampling was done, and records were reviewed.
Three guideline recommendations specific to ED management of acute asthma, from Ministry of Health Singapore Guidelines of Acute Asthma, were used to study management patterns as follows:
1. ‘Systemic steroids, for example, prednisolone 30 mg, immediately and repeated for 7–10 days for all patients. No “tail” is required, and oral steroids are as rapid and effective as injection’. (Grade A, Level Ib)
We studied if our acute asthmatic patients were given systemic steroids at all, and if they were, we studied if this was given to them immediately (started in the ED) or not (started upon discharge).
2. ‘Addition of ipratropium 0.5 mg in adults to an aerosolised solution of beta2-agonist has been shown to cause additional bronchodilation, particularly in those with severe airflow obstruction, and to reduce hospitalisation’. (Grade A, Level Ia)
In our study, we defined patients as having moderately severe asthma if they required more than one nebulizer for symptom relief.
3. ‘All doctors treating asthma patients should provide patient education to aid behaviour change’. (Grade A, Level Ia)
We studied documentation of any form of asthma advice – verbal counselling or handing out of asthma education pamphlet, to discharged patients.
We reviewed the records of discharged patients to trace unscheduled ED re-attendances for the same condition in the next 72 h. We reviewed new medical services made available during the 10-year period, and studied disposition trend differences in the two sets of data.
Study approval was obtained from the Singhealth Central Institutional Review Board. The same board approved the waiver of informed consent based on ethical consideration as no patient identifiers were used in analysis.
Statistics
Sample size
We hypothesised a 10% improvement of guideline adherence in current year. For the study to have 90% power with a two-sided significance level of 5%, the minimum sample size in each arm would be 520. Taking into account possible missing or incomplete data of 20%, we aimed to include at least 625 patients into each group.
Statistical methods
All the categorical data were presented as frequency (percentage). Chi-Square test was used to examine the significant associations between two categorical variables. Logistics regression was used to assess the significance level of 10 years ago versus current years as an independent factor contributed to the outcomes with patients’ age, gender, ethnicity and severity of asthma attack were adjusted. Odds ratio (OR) and its 95% confidence interval (CI) were presented.
A two-tailed, p-value of <0.05 was considered statistically significant. Statistical analysis was performed with SPSS statistical software, version 19.0 (IBM Corp. Armonk, NY).
Results
In the data 10 years ago, 2288 patients with an ICD diagnosis code of ‘Asthma 493’ were shortlisted. After excluding patients below 12 years old and sampling of every third of the remaining patients, 687 patient records reviewed. In the current year data, similar shortlisting and age exclusions on 2781 patients were applied. After sampling of every fourth of the remaining patients, 684 patient records were reviewed. Following medical record reviews, the sample size was reduced to 630 in data 10 years ago, and 635 in the current year (Figure 1). Reasons for exclusions following record reviews are given in Table 1.
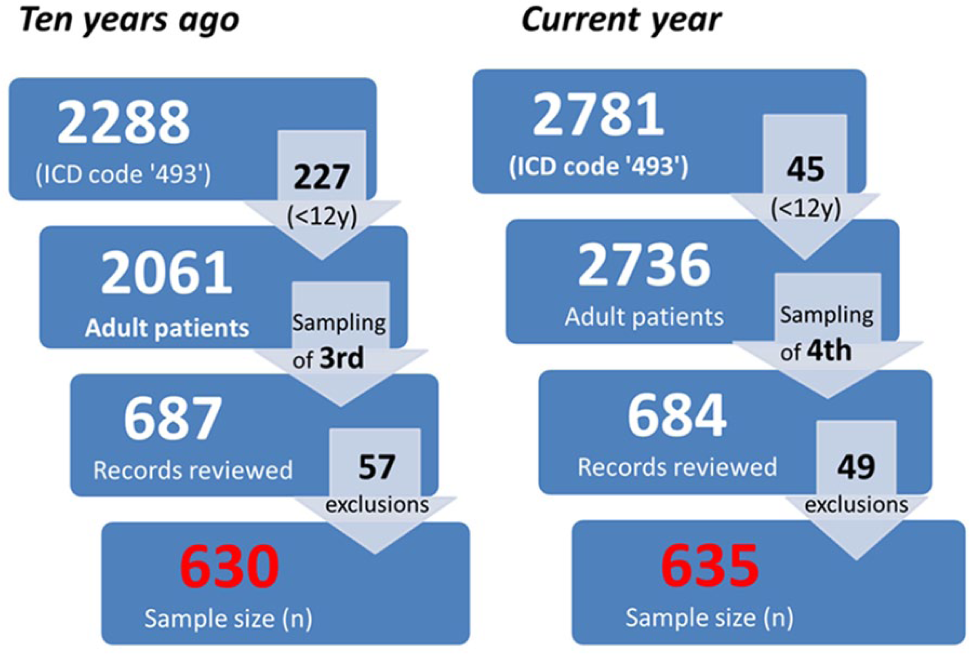
Patient selection.
Reasons for exclusions.
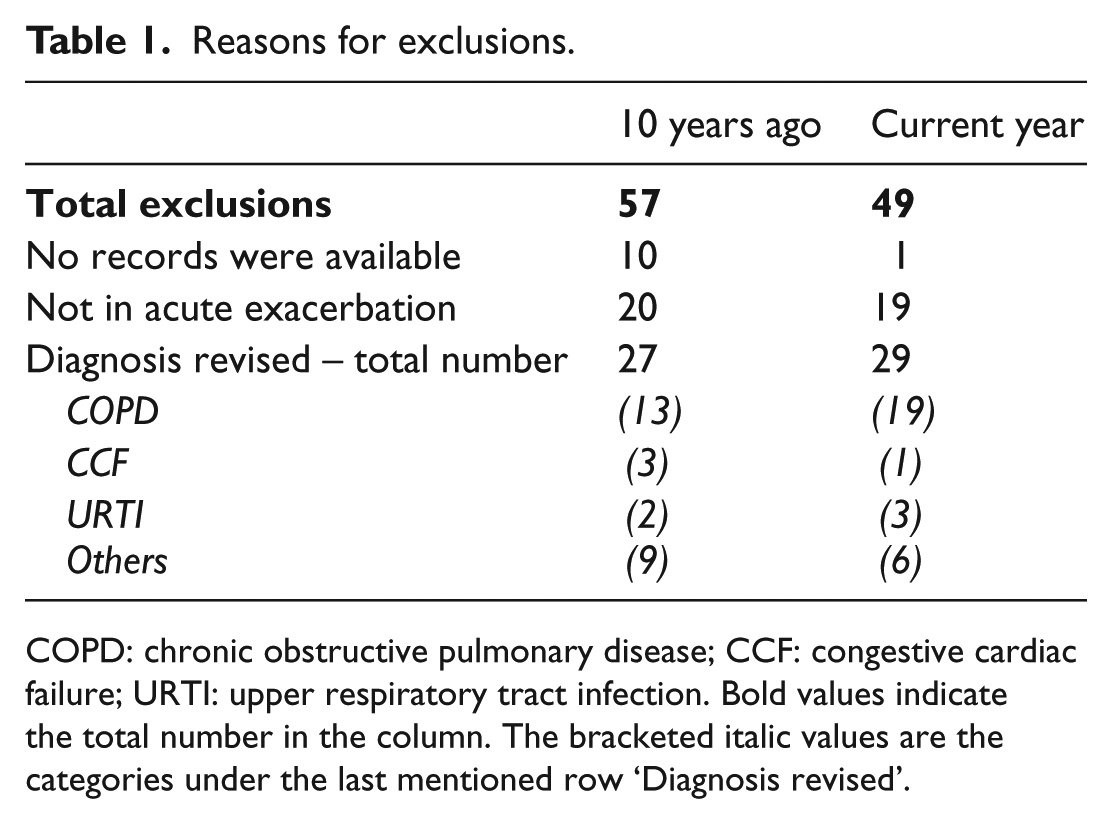
COPD: chronic obstructive pulmonary disease; CCF: congestive cardiac failure; URTI: upper respiratory tract infection. Bold values indicate the total number in the column. The bracketed italic values are the categories under the last mentioned row ‘Diagnosis revised’.
Patient baseline characteristics are shown in Table 2. There were differences in the patient profiles with regard to gender, age and severity of asthma attacks. Severity of asthma attacks were assessed based on parameters listed in Table 3.
Patient baseline characteristics.
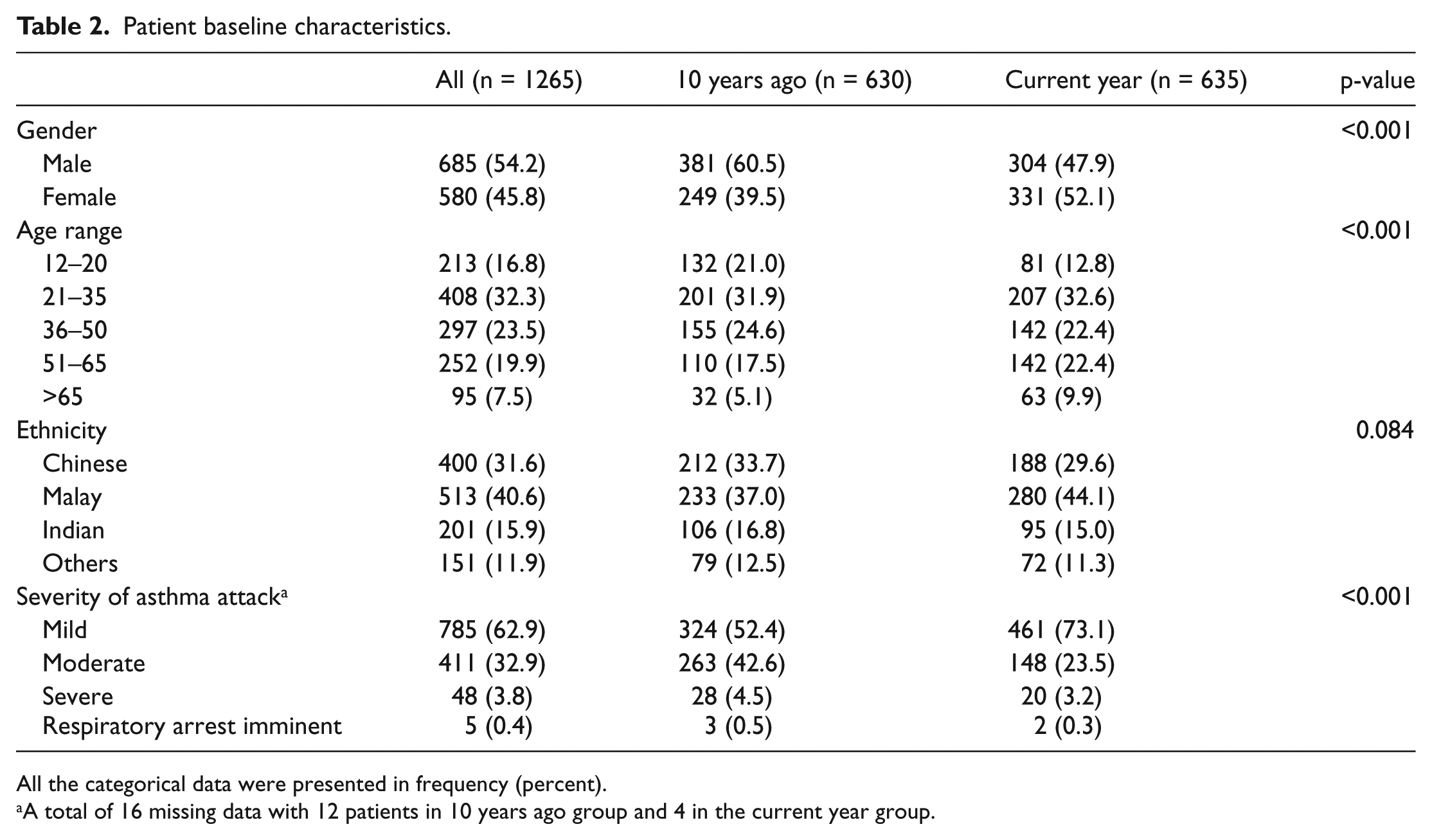
All the categorical data were presented in frequency (percent).
A total of 16 missing data with 12 patients in 10 years ago group and 4 in the current year group.
Severity of asthma attacks.
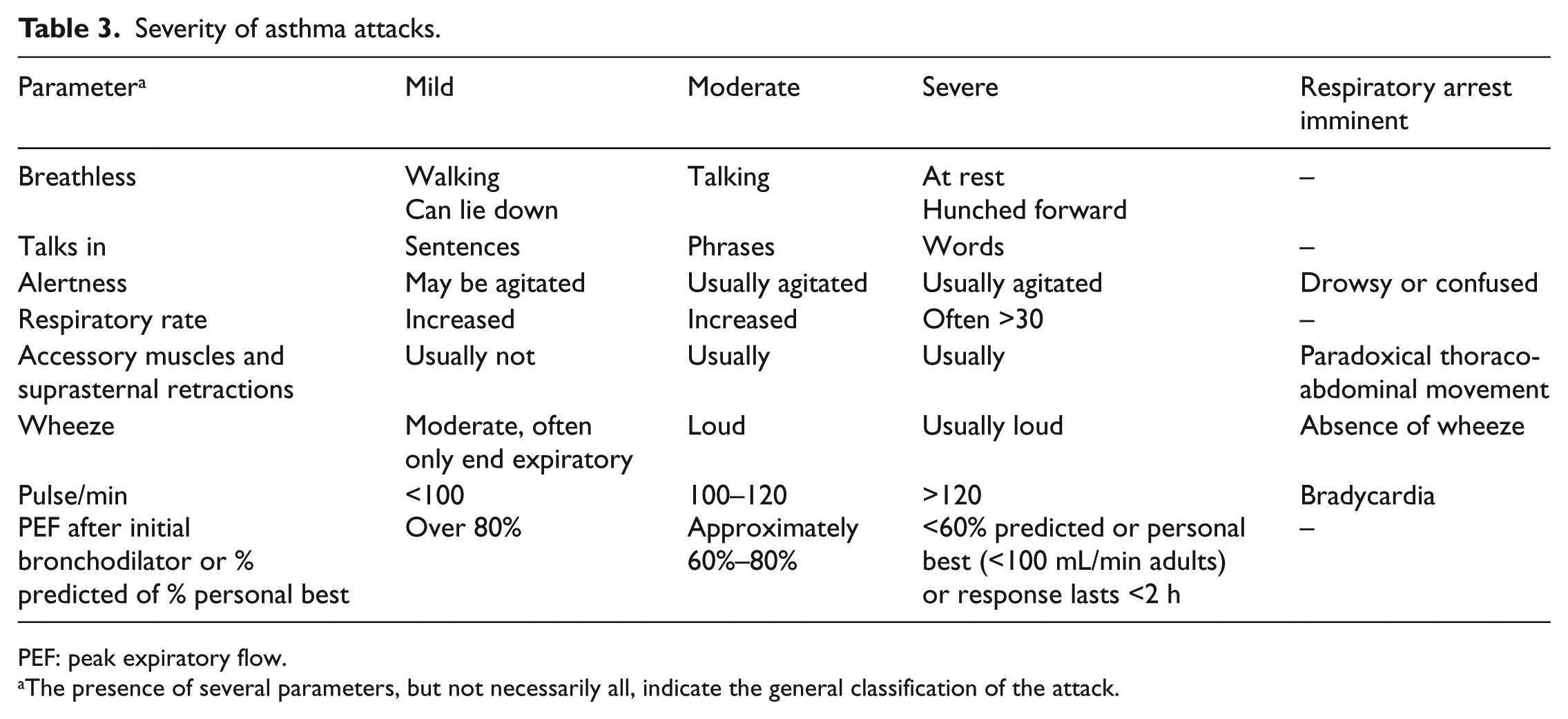
PEF: peak expiratory flow.
The presence of several parameters, but not necessarily all, indicate the general classification of the attack.
In general, there were statistically significant improvements in adherence to all the guidelines studied, after patient variables were adjusted (Table 4). There was a 29% increase in steroid administration rate, with a 43% increase in patients receiving their first steroid dose in ED in the current year. There was an increase in 63% in aerosolized anti-cholinergics administration for patients with moderately severe asthma, and an increase in 66% in patient education for discharged patients in the current year.
Adherence to asthma guidelines.
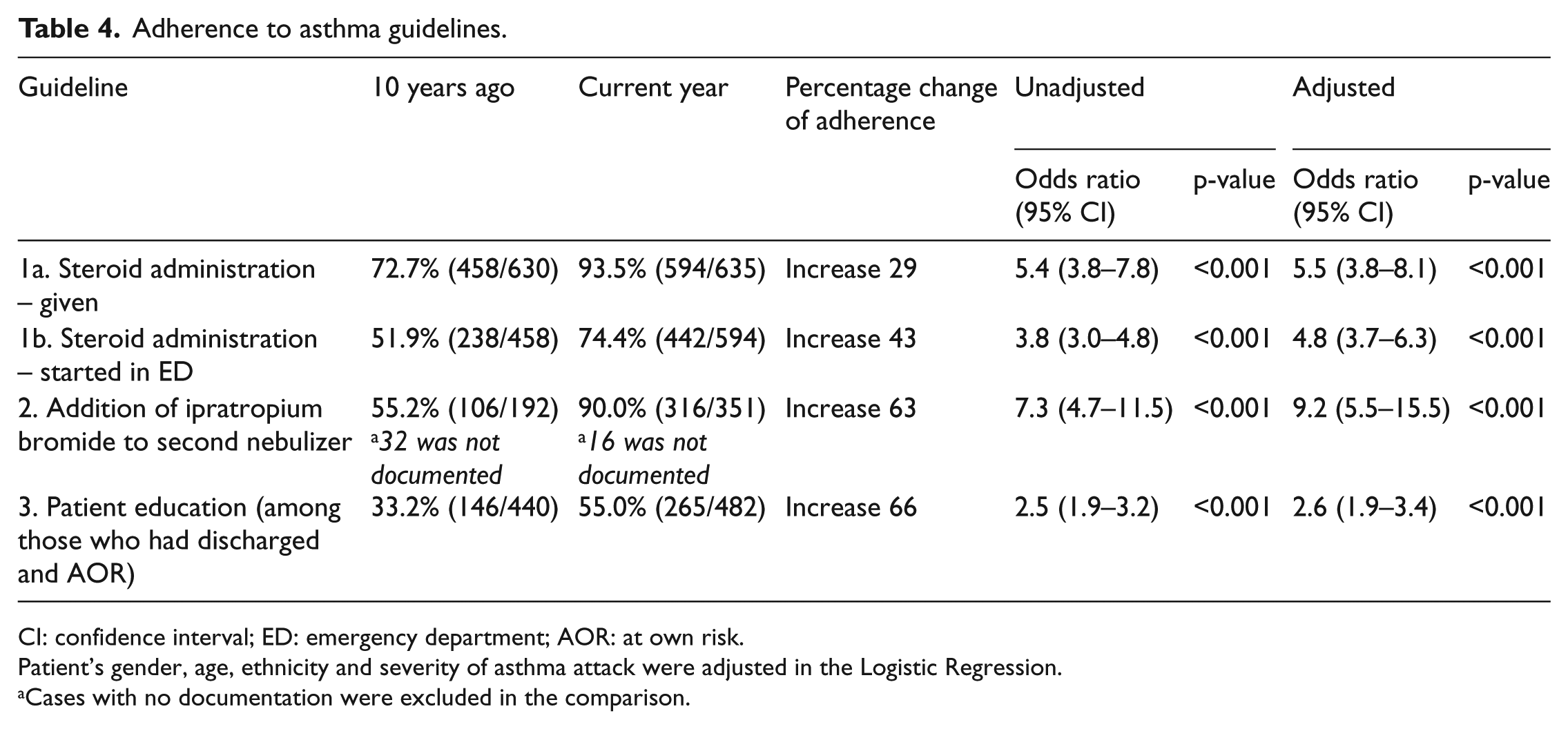
CI: confidence interval; ED: emergency department; AOR: at own risk.
Patient’s gender, age, ethnicity and severity of asthma attack were adjusted in the Logistic Regression.
Cases with no documentation were excluded in the comparison.
However, there was no difference in the rates of 72-h unscheduled re-attendances. In both sets of data, the rate was 4.2% (Table 5).
Rates of 72-h unscheduled re-attendances.
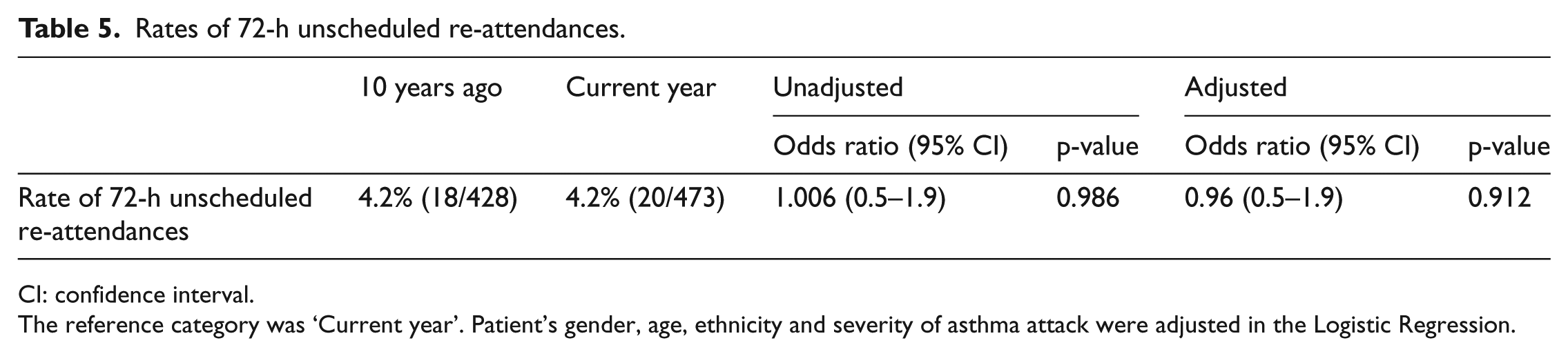
CI: confidence interval.
The reference category was ‘Current year’. Patient’s gender, age, ethnicity and severity of asthma attack were adjusted in the Logistic Regression.
During the 10 years of the study period, two evident initiatives were started. First, within the hospital, the 24-h short stay unit (SSU) was set up to allow patients with singular, uncomplicated and treatable pathology and yet needing to be admitted, to be managed seamlessly from the ED. This frees up inpatient beds for patients who are expected to stay longer than 24 h. Managed by ED physicians, patients are admitted and managed to the unit following a protocol with pre-determined inclusion and exclusion criteria, management and disposition plans. At the time of completion of the study, there were about 20 SSU protocols besides the asthma protocol.
Second, an ongoing nation-wide initiative was promoted by the health ministry to encourage people to seek medical consultation from primary healthcare providers first, especially for simple, non-emergency conditions. Locally, these primary healthcare physicians are the private general practitioners or the government-funded polyclinics. The aim of the initiative was to maximise community health services, while allowing more acute and complicated medical conditions to be managed effectively in the acute hospitals. At the hospital level, patients who had been treated and adequately stabilised by the acute hospital doctors would be referred to their primary healthcare physician for follow-up care.
Although there were clinical differences in disposition trends in terms of hospital admissions and discharges, these were not statistically significant after adjusting to patients’ characteristics (Table 6). In both sets of data, most patients were discharged. In the current year, a higher proportion was discharged with a follow-up to a healthcare provider in the current year (278/473, 58.8%), compared to 10 years ago (203/428, 47.4%), (p < 0.001). In the current year, among those who were referred, a higher proportion was referred to the primary healthcare providers (182/278, 65.4%), compared to 10 years ago (74/203, 36.4%), (p < 0.001).
Disposition trends.
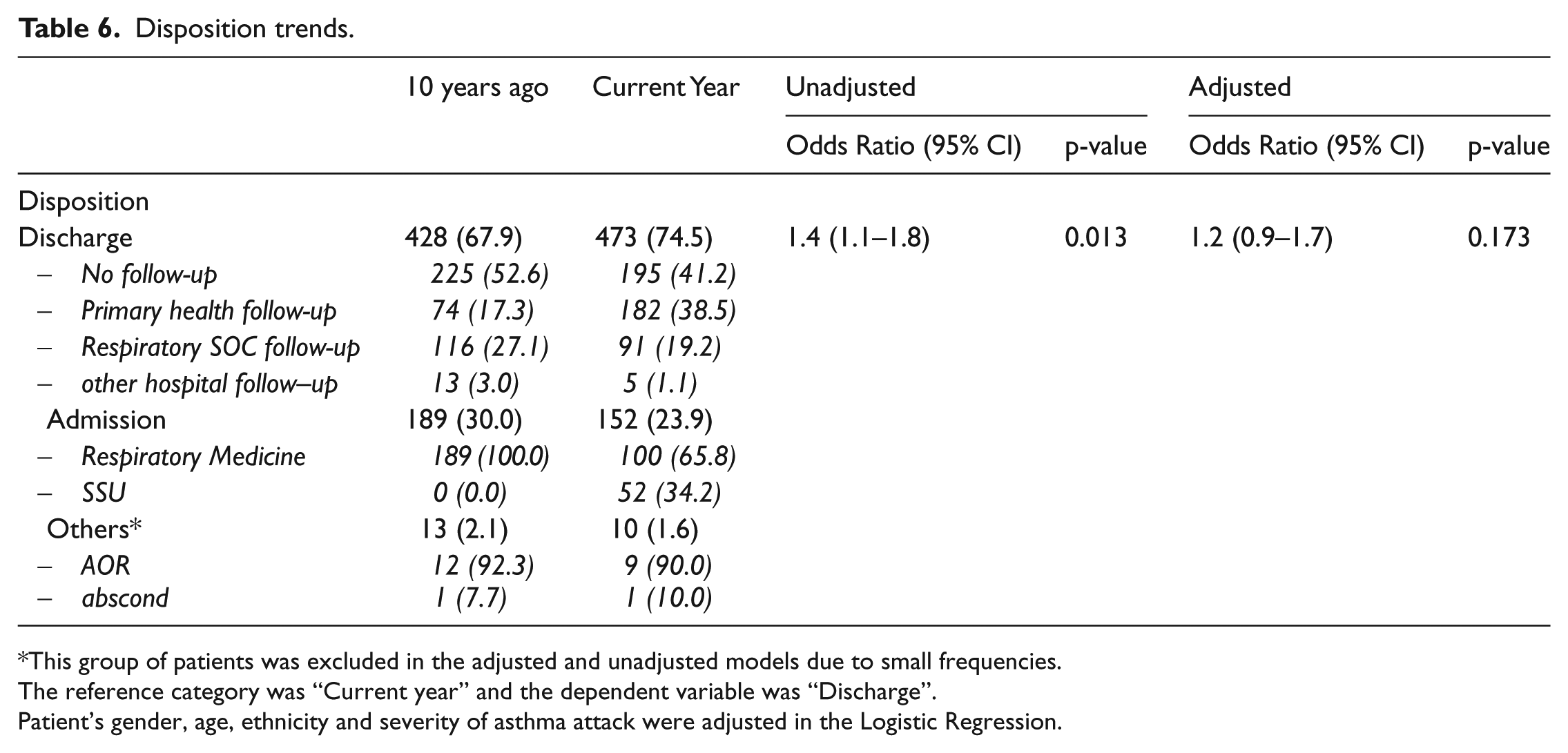
This group of patients was excluded in the adjusted and unadjusted models due to small frequencies.
The reference category was “Current year” and the dependent variable was “Discharge”.
Patient’s gender, age, ethnicity and severity of asthma attack were adjusted in the Logistic Regression.
Hospital admissions accounted for less than a third of dispositions in both sets of data. In both sets of data, a small number of patients were discharged against medical advice (at own risk (AOR)) or absconded before the end of consultation.
Discussion
Asthma is a health problem affecting all age groups, across many continents. In our ED, asthma accounted for 1.9% of all attendances 10 years ago, and 1.8% in the current year. Evidence that adherence to asthma guidelines improves patient outcomes, particularly in reducing hospital admissions and length of stay2,3 was the background to our objective to determine the guideline adherence rates locally. While our audit 10 years ago revealed suboptimal guideline adherence, our findings were not dissimilar to what other authors had published.1,4
Despite the Clinical Practice Guidelines being updated once over the 10-year period, guidelines applicable to the ED remained largely unchanged. Evidence for early administration of steroids in acute asthma is well established. The benefits, seen in both adults and children, included reducing admission rates. Despite similar efficacies in both administration routes, oral is preferred for its relative administration ease and lower cost over the parenteral (pain, phlebitis), unless the patient is too dyspnoeic to take orally, or in patients with anticipated absorption issues. 5 We did not study the differing administration routes.
Ipratropium bromide offers modest improvement in airway obstruction, without the risk of adverse events and possibly reducing hospital admissions.6,7 We had used the clinical judgement parameter (requirement for a second nebulizer for symptom control) to assess the need to add aerosolized ipratropium, instead of using the patient’s initial (pre-nebulizer) severity status. In our study, a higher proportion of patients required a second nebulizer for symptom control in the current year, despite a higher proportion presenting with mild exacerbations.
Patient education in the ED could improve primary healthcare provider follow-up, although its evidence to reduce relapses and readmissions is unclear. 8 In our department, patient education has evolved over the years, with greater involvement of paramedical professionals. Inhaler techniques are reinforced by pharmacists and case managers; precipitant avoidance, medication compliance and action plan counselling are undertaken by nurses and case managers. Patient education aids, such as asthma advice pamphlets, were also made available.
We note the baseline characteristic differences in the two sets of data, possibly pointing to a maturing population over the years. Cases that were excluded based on paediatric age group in the current year were lower, likely due to the establishment of the children’s hospital, thereby reducing our overall paediatric attendance rate. Interestingly, despite nation-wide efforts to promote primary healthcare for mild conditions, more patients were coming to the ED in mild asthma conditions in the current year. We concede that like all community-based initiatives, a desired mindset change and health-seeking behaviour warrant sufficient time and education to materialise. We did not study the period of day these attendances took place, for example, if the preponderance was towards after office hours, when most primary healthcare services may not be available. However, in the light of the differences in patient characteristics, data were adjusted in the multivariate analysis. The adjusted results showed that the two groups remained significant different even after taking into account patients’ gender, age, ethnicity and severity of asthma attack.
We report adherence improvement in all studied guidelines. During the 10-year study period, hospital- and department-wide quality-improvement measures were introduced. Medical and nursing staff education on the importance of steroids administration, anti-cholinergics (such as ipratropium bromide) to the nebulizers in the moderately severe asthma and dispensing of simple asthma advice to patients, was undertaken. This included formal classroom and online platforms, and informal bedside teachings. Education of medical students also emphasised on these key areas of asthma management in the ED. The hospital-wide Asthma Clinical Pathway, which inpatients would be started on, detailed management outlines. It is regularly updated, and its compliance strictly audited.
We attribute the better guidelines adherence largely to these quality-improvement measures. We acknowledge, however, that better documentation of work processes and treatment rendered, with the aid of upgraded electronic systems, could possibly have exaggerated to these results to a certain extent.
An unscheduled return is a patient presentation for the same chief complaint within 72 h of ED discharge. 9 It is often monitored as a quality indicator of the clinical management of patients in their initial ED visit. Unscheduled returns could be unavoidable (in which discharge from the ED was appropriate) or avoidable, due to patient factors (e.g. patient non-compliance to medical advice and treatment, or patient anxiety) or inappropriate medical management. Only in the last instance would one argue it could possibly accurately reflect medical service quality. Its accepted reasonable rates fall between 1% and 5%. 10 We chose 72 h scheduled return rates for discharged patients as an outcome measure to guideline adherence as it would probably be most reflective of proper management of the ED patient. The re-attendance rate 10 years ago was not excessive. Therefore, in the current year, despite better adherence to guidelines, this positive finding did not translate to an improved outcome of reduction in unscheduled re-attendances.
Although other outcome measures such as length of hospital stay, intubation rates, intensive-care facility admission and mortality within the index visit could have been studied, we felt that the studied guidelines applicable to ED might not have impacted these outcomes without many more confounding factors, for example, patient’s medical condition before arriving in ED, co-morbidities and inpatient medical management.
Although there were no significant differences in the admission and discharge dispositions, two trends were observed. First, although hospital admission rates were not dissimilar, SSU admissions accounted for about a third of all hospital admissions in the current year. Second, among the discharged patients, more were being referred for follow-up care, particularly to the primary healthcare provider. This reflected a shift in emphasis on primary healthcare providers as main professional health-caregivers in asthma. This is supported in the Clinical Practice Guidelines as a good practice points (GPPs) practice.
Limitations
As mentioned, our study data were dependent on medical documentation. Observed exaggerated improvement in guidelines adherence, stemming from improvements in medical record keeping over the years, cannot be excluded.
The limitation to using unscheduled returns as a quality indicator of clinical management is discussed above. We reported all unscheduled returns, but have not studied if these cases were truly a result of suboptimal clinical management.
Disposition trends reflected improved services available in the primary care and in-hospital settings and awareness among emergency physicians to make use of these resources. While these indicate a more efficient siting of care in the current year, they do not necessarily point to poorer decisions made with respect to patient disposition 10 years ago.
With the current consistent usage of electronic systems to accurately capture administered treatment and the stabilisation of new services in the hospital and community, a similar study could be undertaken, and cases of unscheduled returns studied more closely.
Conclusion
There was significant improvement in asthma guidelines adherence in the ED. However, there were no significant differences in 72-h unscheduled re-attendance among discharged patients. With the introduction of the SSU and the emphasis on primary healthcare, disposition patterns of asthmatic patients presenting to the ED have evolved over the years.
Footnotes
Acknowledgements
We thank Tan Win Jim, then a medical student of National University of Singapore, and Dr Vishaka Kerner, a medical officer of Emergency Department, Changi General Hospital, for assisting in data collection and data entry.
Author contributions
C Tan contributed to study concept and design, acquisition of data, data analysis and interpretation, drafting and proof-reading of article. M Tai contributed to acquisition of data, data analysis and proof-reading of article. J W Kam contributed to statistical analysis and proof-reading of article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
Data were extracted from electronic medical records, and accessed only by staff-limited password. Data were keyed and analysed using password-protected hospital computers.
Informed consent
Written informed consent was not necessary because no patient data has been included in the article.
Ethical approval and human rights
Study approval was obtained from the Singhealth Central Institutional Review Board. The same board approved the waiver of informed consent based on ethical consideration as no patient identifiers were used in analysis.