
Abstract
A middle-aged woman had a central venous catheter insertion for fluid resuscitation presented with tachypnea and oxygen desaturation 6 h later. Diagnosis was made based on the chest X-ray performed 6 h after the catheter placement. Thereafter, the patient received appropriate treatment.
Case history
A septic patient in her 40s underwent central venous catheter (CVC) placement into the left internal jugular vein (IJV). A left-sided approach was chosen as for the presence of an erythematous, possibly cellulitic rash on the right side of the neck. The vein was located with static ultrasound (US) prior to insertion. Blood could be aspirated from the CVC lumina, and urgent fluid resuscitation through the CVC was commenced.
Six hours later, she was noted to be gasping, respiratory rate was 30/min, oxygen saturation was 92%, and hemodynamically stable. Electrocardiogram (ECG) and chest X-ray (CXR) performed on arrival were normal. Repeated CXR was performed and revealed striking abnormality (Figure 1(a)). Ultrasound of the neck noted a perivascular position of the CVC.
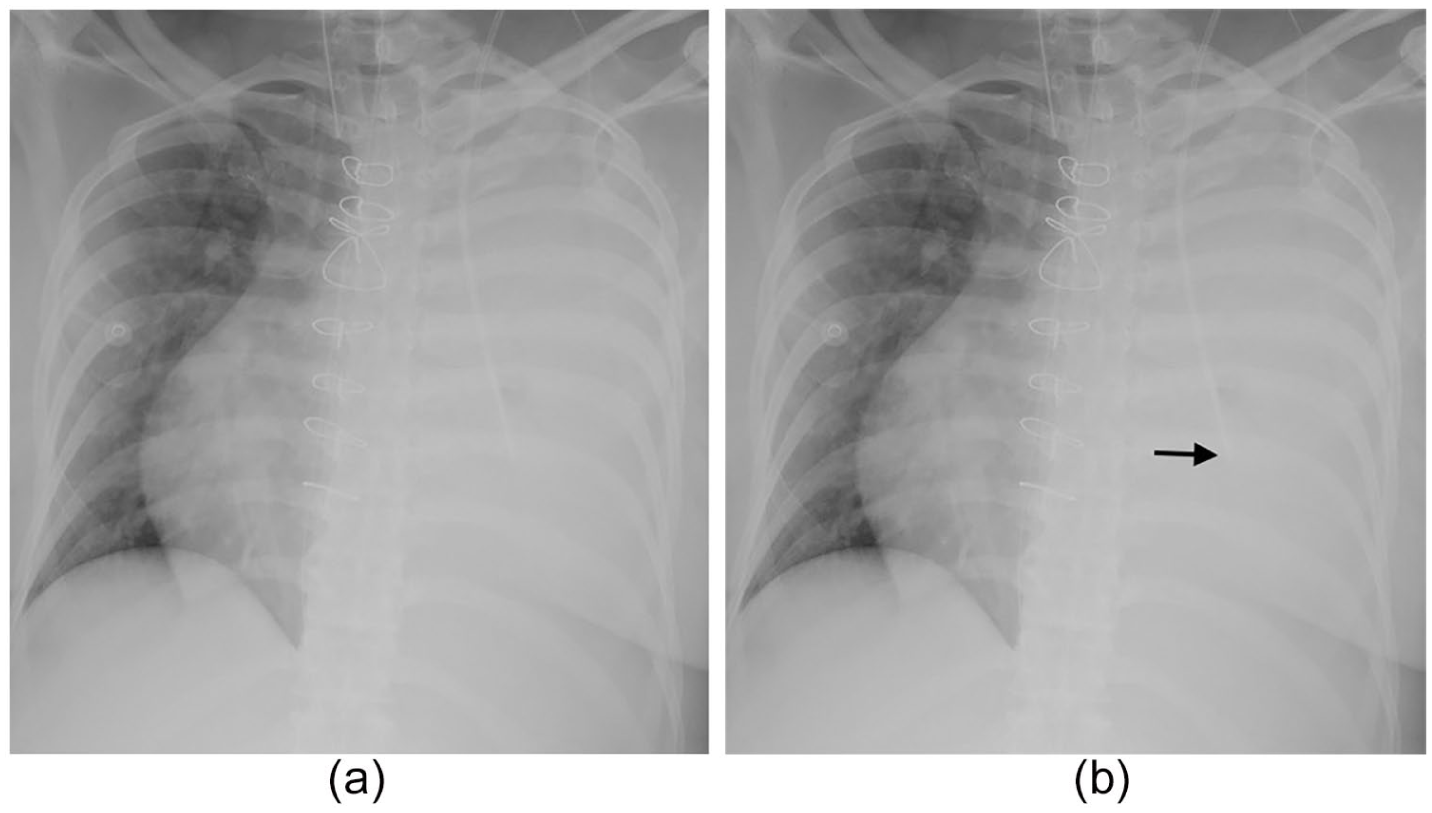
(a) Chest X-ray taken 6 h after central venous catheter insertion and (b) same image with labels showing central venous catheter tip inside the left hemithorax (arrow) with new onset left pleural effusion.
The primary cardiology team was consulted, and 1650 mL of haemoserous fluid were aspirated through the catheter with a complete resolution of the effusion (Figure 2). The CVC was removed without complication.
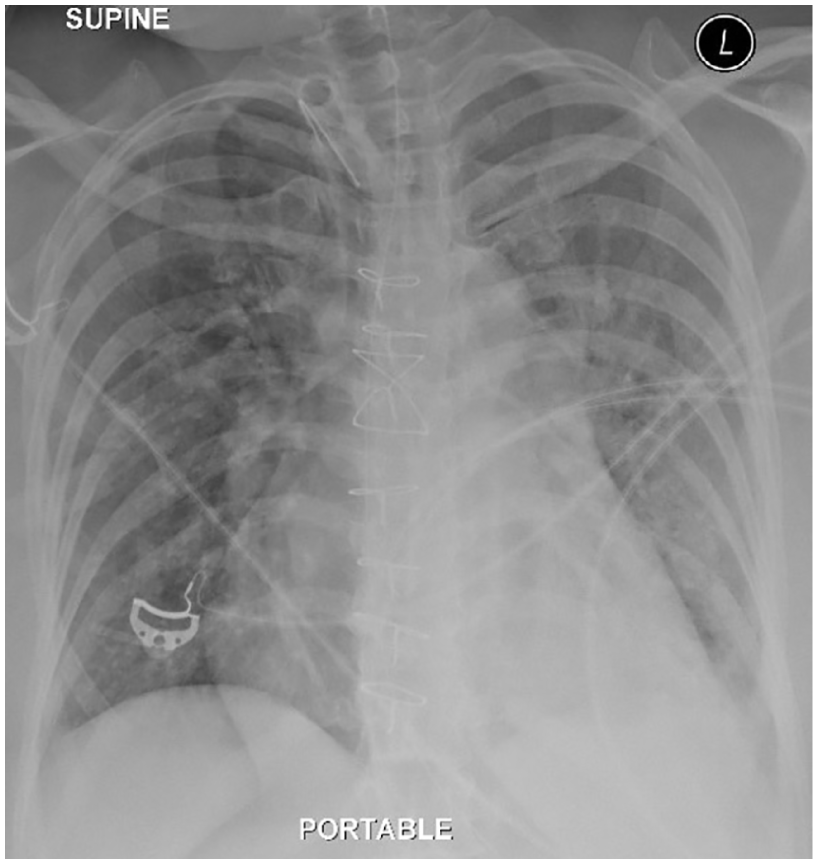
Chest X-ray after aspiration of 1650 mL haemoserous fluid through the CVC. Complete resolution of the pleural effusion.
Questions
What are the chest X-ray findings? (Figure 1(a))
What is the most likely diagnosis?
Answers
Central venous catheter tip inside the left hemithorax (arrow) with new onset left pleural effusion (Figure 1(b))
The chest X-ray and ultrasound findings suggestive of iatrogenic pleural effusion secondary to CVC malposition.
Discussion
CVC is a routine procedure performed in emergency departments and intensive care units for administration of medications, blood products, and fluids resuscitation. The most common complications associated with CVC insertion are bloodstream infection, pneumothorax, and haemothorax. 1 Iatrogenic pleural effusion is a rare complication of CVC malposition or migration.1,2 Landmark-based CVC insertions have complication rates as high as 30%. 3
Knowledge of anatomical landmark and selecting the right-side venous system as first preference for cannulation associated with a lower incidence of malposition. 1 The evidence is clearly in favour of the addition of real-time US-guided CVC placement in the IJV.4,5 The ultrasonography technique enables the physician to CVC tip positioning after insertion. 5 Finally, correct CVC position should be confirmed by CXR prior to use even if there is clinical urgency. 1
For our case, the intrathoracic CVC can be used for safe aspiration of pleural effusion.
Footnotes
Authors’ contribution
K.S.S.W., H.Q.H., and A.L. prepared the manuscript. All authors have seen and have approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Ethical approval
University Malaya Medical Centre does not require ethical approval for reporting individuals case for all the cases that are sufficiently anonymized.
Human rights
How the data and images obtained was in accordance with the principles outlined in the Declaration of Helsinki.
Informed consent
Written informed consent was obtained from the patient for the anonymized information to be published in this article.