
Abstract
Background:
Unstable pelvic fractures are highly lethal injuries.
Objective:
The review aims to summarize the landmark management changes in the past two decades.
Methods:
Structured review based on pertinent published literatures on severe pelvic fracture was performed.
Results:
Ten key management points were identified.
Conclusion:
These 10 recommendations help diminish and prevent the mortality. (1) Before the ABCDE management, preparedness, protection, and decision are essential to optimize patient outcome and to conserve resources. (2) Do not rock the pelvis to check stability, avoid logrolling but prophylactic pelvic binder can be life-saving. (3) Computed tomography scanner can be the tunnel to death for hemodynamically unstable patients. (4) Correct application of pelvic binder at the greater trochanter level to achieve the most effective compression. (5) Choose the suitable binder (BEST does not exist, always look for BETTER) to facilitate body examination and therapeutic intervention. (6) Massive transfusion protocol is only a temporizing measure to sustain the circulation for life maintenance. (7) Damage control operation aims to promptly stop the bleeding to restore the physiology by combating the trauma lethal triad to be followed by definitive anatomical repair. (8) Protocol-driven teamwork management expedites the completion of the multi-phase therapy including external pelvic fixation, pre-peritoneal pelvic packing, and angio-embolization, preceded by laparotomy when indicated. (9) Resuscitation endovascular balloon occlusion of aorta can reduce the pelvic bleeding while awaiting hospital transfer or operation theater access. (10) Operation is the definitive therapy for trauma but prevention is the best treatment, comprising primary, secondary, and tertiary levels.
Keywords
Introduction
Severe unstable pelvic fracture with ring disruption and shock is associated with high mortality of 40%–60% despite treatment.1–5 Early death is most often due to severe hemorrhage as a result of acute blood loss. 5 Significant mortality reduction has occurred after adoption of standardized management algorithms.6–8
Hence, a modern structured, organized, and expeditious multi-phase and inter-disciplinary approach is indicated to maximize or to further improve the patient outcome by quick external pelvic binder compression for the reduction the pelvic volume, optimization of the initial hemostatic/balanced fluid resuscitation, and timely attainment of the life-saving venous, bone marrow as well as arterial bleeding control to rescue the patient of deranged physiology before a definitive follow-up anatomical correction operation through an explicit protocol-driven teamwork.
Commandment 1—before the ABCDE steps, preparedness, protection, and decision are essential to optimize patient outcome and to conserve resources
The standard polytrauma management sequence of primary survey (ABCDE) with simultaneous resuscitation is applied according to the Advanced Trauma Life Support (ATLS) principles. 9 Kam et al. 10 introduced the PD-ABCDE, with P standing for “personal protective equipment (PPE),” while D refers to “decision” by prompt assessment of salvageability to determine continuation or termination of resuscitation. Another P is now added to indicate the “preparedness” to stress on the pre-planning and teamwork to meet the complexity of the highly lethal pelvic disruption.
Maintenance of a patent airway with cervical spinal movement restriction (to replace immobilization which is not achievable by the non-rigid neck collar) as introduced in the ATLS 10th edition 9 is the first step. When indicated, drug-assisted endotracheal intubation (to replace rapid sequence intubation or induction, which requires higher level of anesthetics beyond the regular practice of frontline trauma care in the underprivileged facilities) 9 is applied.
While checking the circulation and setting up intravenous (IV) access, external bleeding is controlled mainly by compressive dressing. When necessary, proximal arterial tourniquet11,12 and hemostatic dressing (by clotting factor concentration, muco-adhesive, or pro-coagulants)13–15 may be, respectively, applied for severe limb and torso bleeding not amenable to direct compression. In severe limb bleeding, Kragh et al. 16 have found that proximal arterial tourniquet substantially reduced mortality by 92% if applied than not, 80% when applied before shock than after, and 13% if applied in prehospital care than in the emergency department (ED).
There are recent advances in junctional compression devices to control bleeding at joints and in Abdominal Aortic Compression Tourniquet to reduce pelvic and lower limb bleeding.17–19
Commandment 2—do not rock the pelvis to check stability, avoid logrolling but prophylactic pelvic binder can be life-saving
In patients with shock with severe mechanism of injury (MOI) and evident pelvic wounds, deformity, or shock, prophylactic pelvic binder should be applied in accordance with the National Institute for Health and Care Excellence (NICE) guideline in 2016. 20 The principle of acute management is to treat or implement harm reduction before confirming anatomical diagnosis when physiology is grossly deranged.
Besides, do not rock the pelvis to check for instability, which can worsen the hemodynamics by inducing more bleeding by aggravating the fracture displacement and causing blood clot disruption. The first blood clot formed is the strongest and subsequent clotting is impaired by the previously consumed coagulation factors and platelets. 21 Moreover, logrolling (which can further jeopardize the pelvic instability) requires risk–benefit assessment and may be performed if active bleeding wound or the obstructed airway indicates the maneuver to save life as recommended by NICE 2016. 20 Logrolling examination aims to identify soft tissue injury of the back, and clinical diagnosis sensitivity of thoracolumbar fracture is very low of 27.5% only. 22 The alternative is to inspect the bed sheet for bleeding hints and placement of the gloved hands gently underneath the back to palpate for any major wounds or bony deformity. 23
Commandment 3—computed tomography scanner is the tunnel to death for patients with hemodynamic instability—use clinical examination and bedside imaging instead
If the patient can be stabilized or optimized in terms of the hemodynamics, secondary survey (thorough physical examination, AMPLE history, and detailed investigation including computed tomography (CT) scan) will ensue.
However, CT imaging for hemodynamically unstable patients (non-responders to initial fluid resuscitation) is the tunnel to death. 24 In non-responders, careful bedside physical examination and history evaluation coupled with rapid plain X-ray examination of the pelvis and chest together with the bedside ultrasonography (USG; focused assessment with sonography for trauma (FAST), extended focused assessment with sonography for trauma (eFAST), point-of-care ultrasonography (PoCUS)) are utilized to identify internal hemorrhage clues (hemoperitoneum and hemothorax), and the obstructive shock is the most important bedside armamentarium to determine the shock etiology to expedite definitive treatment.
In the new generation of clinicians, “Seeing is Believing” has generated overdependence on sophisticated imaging including CT, which is contraindicated in exsanguinating patients because imaging involves patient transfer, takes significant time for completion, and delays the life-saving bleeding control operation. It takes the clinical acumen to identify and decide when and where to treat first with damage control surgery (DCS) approach without a definite organ injury diagnosis but a global trauma perspective of harm containment and reduction.
Diagnostic peritoneal lavage (DPL) for blunt abdominal trauma (BAT) was born in 1965 and pronounced dead in 2005 by Jansen et al., 25 a Scottish military surgeon, owing to oversensitivity of DPL leading to a high rate of non-therapeutic laparotomy.
However, the diagnostic peritoneal aspiration (DPA) has a role to evaluate significant hemoperitoneum in abdomino-pelvic injuries because the distorted abdomino-pelvic anatomy in severe pelvic ring disruption has rendered USG identification of intra-peritoneal free fluid (IPFF) unreliable.26,27
If either FAST or DPA is positive, emergency laparotomy is indicated. Aspiration of greater than 10 mL of gross blood is a positive DPA.28,29 However, new findings published in 2018 by Christian et al. 30 have shown that FAST is of good reliability with sensitivity and specificity of 96% and 96%, respectively. Placing the patient in the Trendelenburg position and serial FAST can further increase the sensitivity.
Trauma Point-of-Care Test (POCT) USG31,32 has evolved from mere IPFF visualization to inferior vena cava (IVC) caliber and respiratory collapsibility evaluation to help differentiate between the two important trauma shock causes of hypovolemia versus obstruction. Besides, USG can reliably diagnose hemothorax and pneumothorax even in the supine position, which is the most common posture of the severely injured, whereas supine chest X-ray (CXR) often cannot elucidate the pathology.
Pericardial collection and right ventricular end-diastolic collapse (RV EDC) are useful USG signs to diagnose pericardial tamponade even when the clinical Beck’s triad is not typical due to concomitant hemorrhagic hypovolemia. Moreover, USG can assess the site of maximum pericardial collection to guide the bedside pericardiocentesis approach, subxiphoid or apical.
USG reveals not only anatomical abnormalities but also hemodynamic functions including the cardiac contractility, wall motion, and IVC caliber changes with respiration in pathological conditions.
In addition, USG is relevant for vascular imaging and blood flow evaluation to diagnose vascular occlusion and to attain vascular access for fluid resuscitation and invasive arterial blood pressure (BP) monitoring.
Commandment 4—correct application of pelvic binder at the greater trochanter level to achieve the most effective compression
Pelvic binder not only acts as a temporizing hemorrhage control device but also facilitates subsequent damage control operation (DCO).
Pelvic binder may be applied in the prehospital setting basing on severe MOI with high impact force usually related to motor vehicle crash (MVC to replace road traffic accident (RTA) to stress on prevention) or fall from a great height in industrial or suicidal attempt incidents. Besides, the shock is another indication for the binder application. The low-level fall due to slipping on ground usually results in hip fracture (femoral neck or trochanter) instead of pelvic ring disruption. The application of pelvic binder may cause further hip fracture displacement than providing benefit in those femoral neck or trochanteric injuries. Pelvic ring disruption is often associated with more extensive pelvic and perineal wounds beyond the hip sites.
Similarly, prophylactic pelvic binder application may be performed in the ED before the X-ray (XR) imaging, aiming to reduce the pelvic volume to produce a tamponade effect to slow down the bleeding.
On the contrary, clinical pelvic stability may be checked if the MOI is assessed to be mild, patient is hemodynamically stable, and the initial plain XR pelvis does not show any suspicious pelvic ring disruption. One important clinical pitfall is the obscuration of pelvic ring instability shown on plain XR after the pelvic binder application.
The four common types of pelvic fractures according to Burgess et al. 33 are antero-posterior compression (APC), lateral compression (LC), vertical shear (VS), and combination of any two or all three of the above. Irrespective of the fracture types, pelvic binders when properly applied can help stabilize the fractures and reduce or restrict the pelvic volume to improve the survival, diminish transfusion need, and shorten hospital stay, especially the APC and VS types.34–36
The most effective compression sites of the pelvic binders are at the greater trochanters as the easily palpable prominent bony landmarks.34,37 The binder placement is centered over the greater trochanters, extending to the buttocks in most patients according to the Western Trauma Association guidelines. 29 The binder should not be left in place longer than 24–36 h owing to skin pressure necrosis. 38
In case of concomitant proximal hip or acetabular fracture shown in bedside plain pelvic XR, the binder may be shifted upward to the center at the iliac crest level to prevent aggravation of the fracture displacement.
Commandment 5—choose the suitable binder (BEST does not exist, always look for BETTER) to facilitate body examination and therapeutic intervention
Currently in Hong Kong, the choices of the pelvic binder lie between the two commonly used trauma pelvic orthotic device (T-POD) and Sam Pelvic Sling. T-POD 39 is a softer belt of one size fitting most adult patients but may require cutting when length is too long for small subjects (only suitable for body weight at least 25 kg or above). It is softer with greater vertical span of 8 in, and hence, the theoretical compression pressure is smaller and pain felt by the conscious subject is less. Owing to its greater vertical span, it more extensively covers the lower abdomen, the groin, perineum, and upper thighs. Consequently, assessment of those parts is more restricted. More shifting and trimming of the T-POD are required for interventional procedures at those sites.
Because the Sam Pelvic Sling 40 is of much shorter vertical span of 5.5 in only, it provides wider access to the lower abdomen, groins, perineum, and upper thighs for examination as well as for procedural intervention when necessary.
However, the Sam Pelvic Sling requires several sizes to meet the needs of the patients of various body dimensions/sizes. Because the Sam Sling is of shorter vertical span, the compression pressure is higher, resulting in more patient discomfort.
To prevent skin pressure necrosis, pelvic binders are recommended not to be applied for more than 24 h. However, soft tissue injury can occur if a continuous pressure compression exceeding 9.3 kPa (73 mm Hg) lasts for more than 2–3 h. 41
In the cadaveric study by Prasarn et al., 42 the mean pressure by Sam Sling was 32.97 kPa as compared with 28.53 kPa exerted by T-POD, although not statistically significant.
In the Hong Kong setting of quick access to hospital and definitive care, most binders should be removed after pelvic disruption exclusion or interim therapy by external pelvic fixation (EPF) within a few hours.
In the systematic review of Bakhshayesh et al., 43 there is no perfect pelvic binder. While there is evidence to indicate that the pelvic circumferential compression device (PCCD) can help reduce the pelvic ring disruption, the hemorrhage control and physiological improvement require further verification. However, the recommendation for well-judged PCCD application continues.
In some centers, the simple draw sheet is used as the PCCD owing to its inexpensive cost, wide availability, and versatility to change the contact surface areas to avoid the surface wounds. 42
Concerning the application, Sam Pelvic Sling is easier to place (three steps of slide, click, and lock) by manual holding of the pelvis (stabilization at the ASIS (anterior superior iliac spine) levels) while carefully and gently elevating the lower legs to slide the Sling to the center at the greater tronchanter level. There is a traction device to produce a specific endpoint of 150 N of force indicated by a “click” sound and tactile sensation. The clinical pitfall is the omission of the hearing of the “click” sound in the noisy trauma room of high stress level and failure to feel the tactile signal resulting in overturning and pelvic compartment syndrome. On reaching the compression endpoint, the Sling is locked by the Velcro adhesion.
On the other hand, the T-POD application is more complicated, requiring the clinicians to understand the Velcro-backed mechanical advantage pulley system, separation gap distance between the two ends of the binder of 6–8 in to generate the required tension. However, the visual endpoint (apposition of the two ends of the T-POD) is easier to recognize and monitored by the teammates. The whole application involves five steps of sliding, trimming, pulley application, compression, and anchor.
The choice is often dependent on the clinical experience and training of the trauma facility personnel. There is no direct head-to-head clinical comparison of the two pelvic binders for the patient outcome. The features and interventional accesses of the two devices are, respectively, shown in the subsequent Table 139,40 and Figures 1 and 2. 44
Comparison of PCCD—Sam Pelvic Sling versus T-POD.
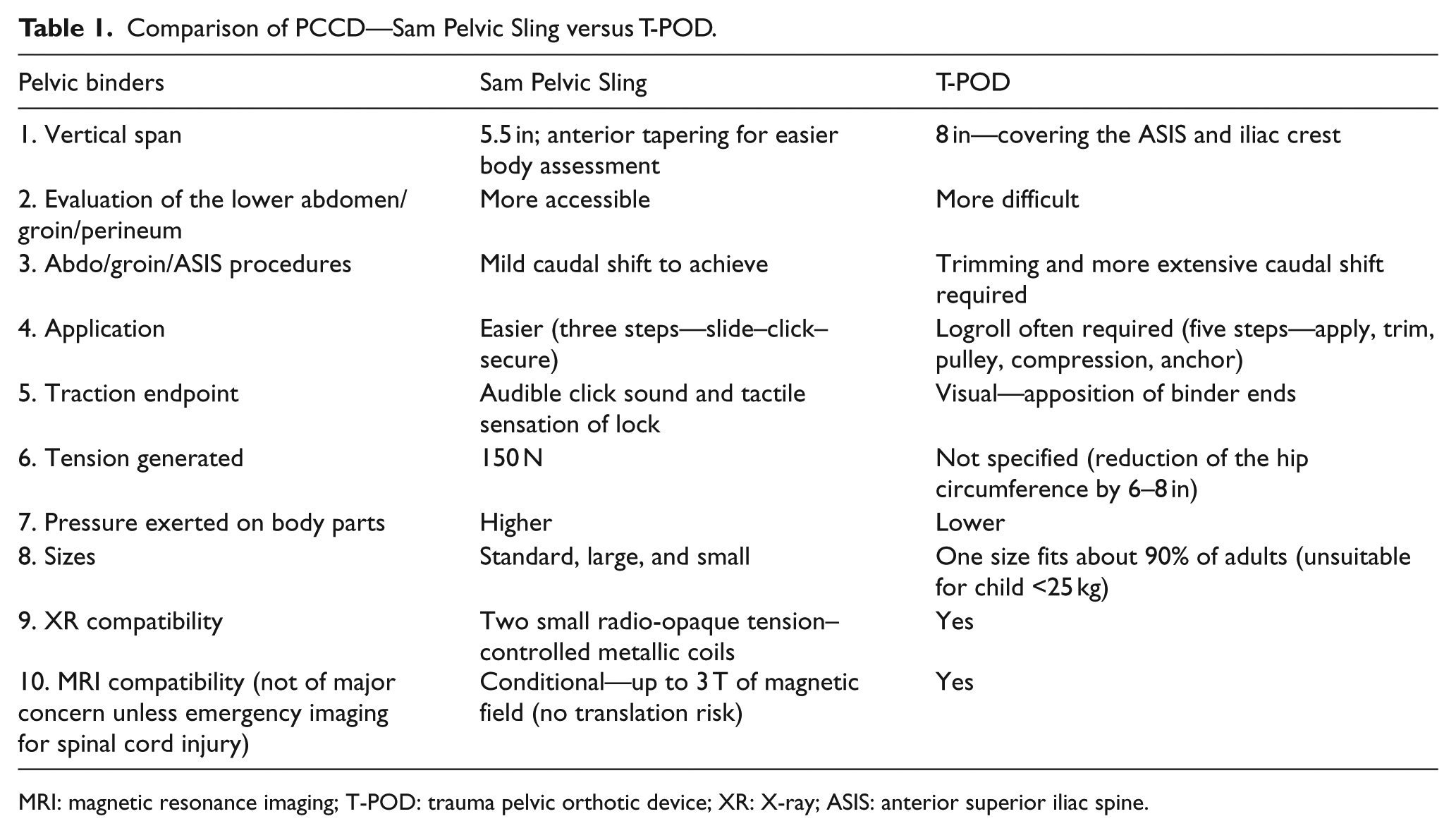
MRI: magnetic resonance imaging; T-POD: trauma pelvic orthotic device; XR: X-ray; ASIS: anterior superior iliac spine.
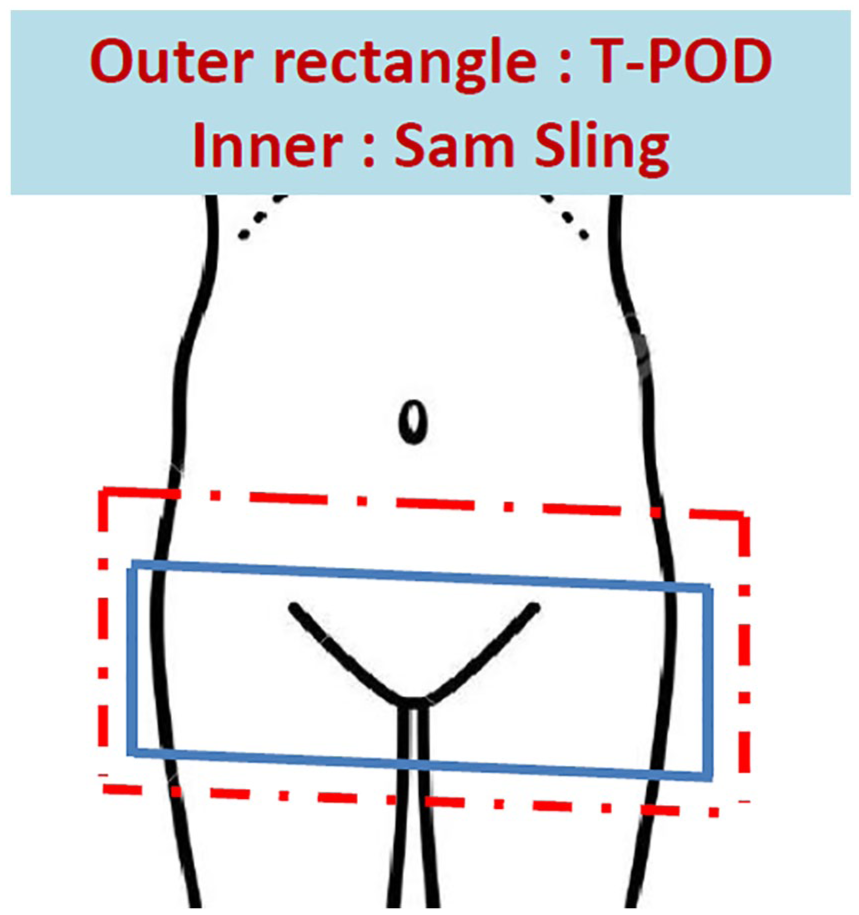
Abdomino-pelvic assessment—wider and easier access by Sam Pelvic Sling versus T-POD. 44
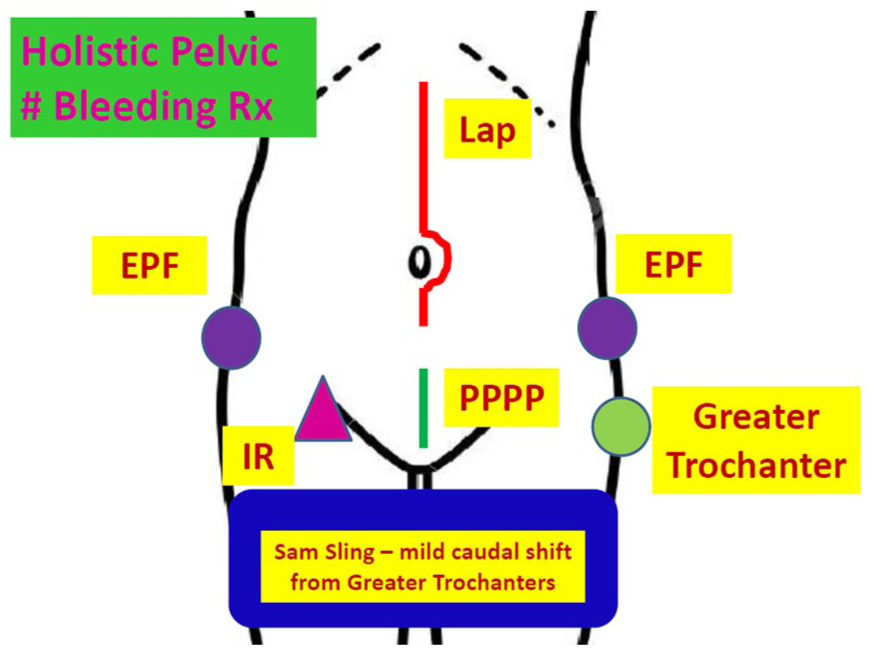
Abdomino-pelvic intervention—wider and easier access by Sam Pelvic Sling versus T-POD. 44
One important precaution on Sam Pelvic Sling use is to regularly check the Velcro anchorage to ensure that there is no inadvertent loosening, especially during and after transfer, particularly in the re-use devices to ascertain the circumferential traction force maintenance.
Commandment 6—massive transfusion is only a temporizing measure to sustain the circulation for life maintenance
The three core components in damage control resuscitation (DCR) are permissive hypotension, hemostatic resuscitation, and DCO.
Permissive hypotension
Despite the Bickell et al. 45 study published in 1994 on penetrating torso injury revealing delayed volume replenishment carried better outcome than immediate large-volume resuscitation when definitive operation was readily available, the ATLS approach took many years or decades to step down the initial resuscitation volume of 1–2 L of crystalloid to the current recommendation of 1 L (ATLS 10th edition—2017). 9 It is understood that large-scale organizations encounter great inertia to change and have low maneuverability to swiftly update (ATLS takes 4–5 years for a revision) any necessary changes. Hence, readers should realize knowledge is rapidly evolving in the ever-accelerating modern world on research with rapid evidence generation. Too large initial resuscitation volume leads to re-gain of a high BP causing hydrostatic dislodgement of the temporary blood clot before the definitive operation to arrest hemorrhage, not to mention the dilutional coagulopathy effect.
Hemostatic/balanced resuscitation
Hence, massive transfusion protocol (MTP) by balanced blood components (packed red blood cell (PRBC):fresh frozen plasma (FFP):platelet concentrate (PC) at 1:1:1) has been introduced to address the issues as a temporizing means to maintain life-sustaining circulation before the operation to achieve hemostasis.
MTP, when properly applied with a high ratio of plasma and PC, not only reduces coagulopathy and improves survival46–51 but also reduces septic shock, ventilator-associated pneumonia (VAP), abdominal compartment syndrome (ACS), heart failure, liver failure, and multi-organ failure (MOF). 52 Moreover, the total amount of blood products transfused is diminished 53 because bleeding control due to coagulopathy is achieved earlier. Hence, it is an evidence to demonstrate “Invest to Save,” meaning that a higher but justified expenditure at the beginning can decrease the total cost ultimately. However, acquired respiratory distress syndrome (ARDS) or the acute lung injury (ALI) rate is higher. 51
Platelet deficiency is not a problem at the beginning of a severe trauma of an otherwise healthy subject. Hence, PC may not be included in the first batch of MTP comprising only the PRBC and thawed FFP in 1:1 ratio.
Tranexamic acid, an anti-fibrinolytic, has been shown to reduce all-cause death in severe trauma in the Clinical Randomization of an Antifibrinolytic in Significant Hemorrhage (CRASH-2) study 54 when administered within 8 h of injury. In a subsequent exploratory study, the mortality reduction was only significant if initiated within the first 3 h of injury; otherwise, the reverse result would occur as shown in Table 2. 55 The drug is inexpensive, and a health economic analysis has found the incremental cost was US$64 to save one life by tranexamic acid for the prevention and treatment of significant hemorrhage in trauma patients. 56
Impact of tranexamic acid on death reduction in severe trauma patients.
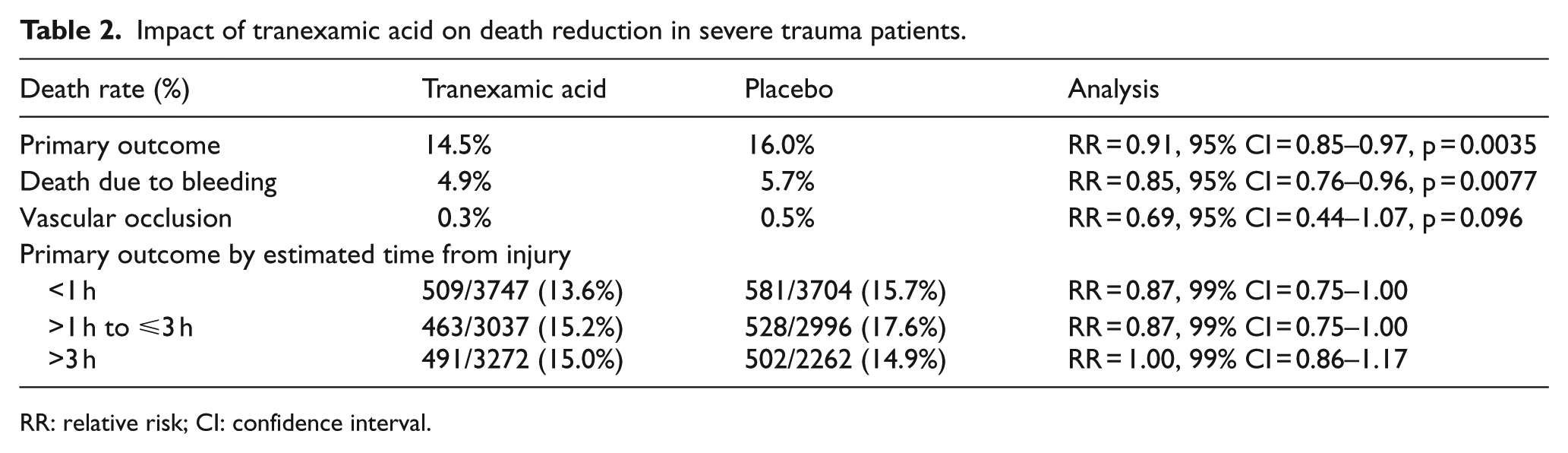
RR: relative risk; CI: confidence interval.
Conventionally, clinicians would request 10 units of PRBCs, 6 units of FFP, and 6 units of PC to manage major bleeding. The simultaneous arrival of 22 units of blood products creates tremendous problem of space occupation and insufficient devices to warm up the PRBCs and to thaw the FFP, not to mention the too low ratio of plasma to PRBC to achieve adequate coagulation, and cold fluid transfusion further worsens bleeding control by the induced hypothermia.
The structured provision of blood components in MTP in organized batches in the ratio of 1:1:1 (four units each for an adult patient) of PRBCs of about 250 mL per unit (to be transfused by a rapid infusion pump with warmer as fast as 500–1000 mL/min, depending on the caliber of the IV catheter placed), thawed FFP of about 250 mL per unit, and PC of 50 mL per unit renders the blood management much easier to control with an interval of 20–30 min between batches until the MTP is deactivated when hemostasis is achieved and adequate replenishment is attained or when salvageability is exceeded.
Currently, MTP is protocol driven including the administration of the adjunctive agents comprising cryoprecipitate and tranexamic acid because the laboratory assay result turn-around time (TAT) cannot meet the immediate assessment need. Hence, the bedside visco-elasticity assay (thromboelastography (TEG) or rotational thromboelastometry (ROTEM)) might give a more precise guidance on the exact deficiency (clotting factors—ExTem, InTem, Fibtem, HepTem). The assay is expensive and hence is not commonly employed. If the patient blood management (PBM) principles are considered, however, saving the non-essential blood products and reducing the total volume of transfusion can improve survival, prevent circulatory overload and ALI, and reduce blood-borne infection risks.57–59 Consequently, it is another level of consideration of “Invest to Save.”
The common MTP activation or decision rule in Hong Kong is the PWH scoring system using the readily accessible three vital signs (heart rate (HR), BP, and Glasgow Coma Scale (GCS)), three blood test results (two Hb levels and base excess (BE)), and two imaging findings (pelvic disruption and hemoperitoneum) by Rainer et al. 60 However, its sensitivity can be escalated when the dynamic change of the Hb level (decrease by 3 g/dL) is included as indicated in the Dynamic MTP score by Lui et al. 61
The current research quest is to identify the most optimal blood product ratios. 62 The other hot issue is to assess whether visco-elasticity assay-guided therapy is superior to protocol driven in the trauma PBM. 63 Current studies only have shown definite benefit in cardiac surgery patients but no available randomized trials on traumatic coagulopathy management.64,65
Commandment 7—DCO/S aims to restore physiology before the definitive anatomical correction
The types of bleeding in major pelvic fractures are multiple, including the pelvic venous (around 85%), arterial (10%–15%), bone marrow, or other associated pelvic or abdominal visceral hemorrhage. 66
Conventional EPF followed by laparotomy to perform intra-peritoneal pelvic packing to control the pelvic hematoma has not been effective because the abdominal compartment is too spacious to fill up to produce an effective compression effect. Pre-peritoneal pelvic packing (PPPP) has been employed for replacement because the pelvic space is very confined after the EPF or pelvic binder application. Consequently, tamponade effect can be more readily achieved (but needs to watch for pelvic compartment syndrome as the risk–benefit balance in the life-saving procedure).
PPPP is a re-kindled armamentarium in the European approach and later adopted in US centers as a first-line rescue treatment instead of angio-embolization.67,68
The operative skills are not difficult to attain. The PPPP requires a lower midline incision of about 8 cm in length from below the umbilicus to just above the pubic symphysis with a separation of about 5 cm from the upper midline incision if prior laparotomy is required to manage any hemoperitoneum. The skin, subcutaneous tissue, and fascia are dissected in the midline. The urinary bladder is retracted away from the fractures. Caution must be observed to avoid avulsing any vascular connections between the iliac and obturator vessels. Two to three surgical packs are inserted in the retroperitoneal space on each side toward the iliac vessels and reaching the posterior sacroiliac joint (SIJ) level, followed by closure. In experienced hands, it merely took about 20 min to accomplish. Removal or exchange of the packs (if hemorrhage continues after pack removal) should be performed in 24–48 h.2,69
On immediately application of PPPP with a PCCD as a component of the severe pelvic fracture bleeding management instead of angio-embolization first, Cothren et al. 2 revealed no deaths were attributed to hemorrhage. Moreover, lower amount of blood transfusion was required. The bleeding control success rate was 83% with 17% requiring angio-embolization. Subsequent PPPP study has also shown significant mortality reduction.70,71
The access interval to PPPP was 45 min as compared with 130 min for angio-embolization. 68 There is a wide variation in the time interval from ED arrival to angio-embolization, indicating improvement measures are badly required to expedite this potentially life-saving emergent percutaneous procedures. 72 The important roles of EPF in pelvic fracture management according to the World Society of Emergency Surgery (WSES) are summarized in Table 3. 20
Roles of EPF in pelvic fracture management—WSES 2017.
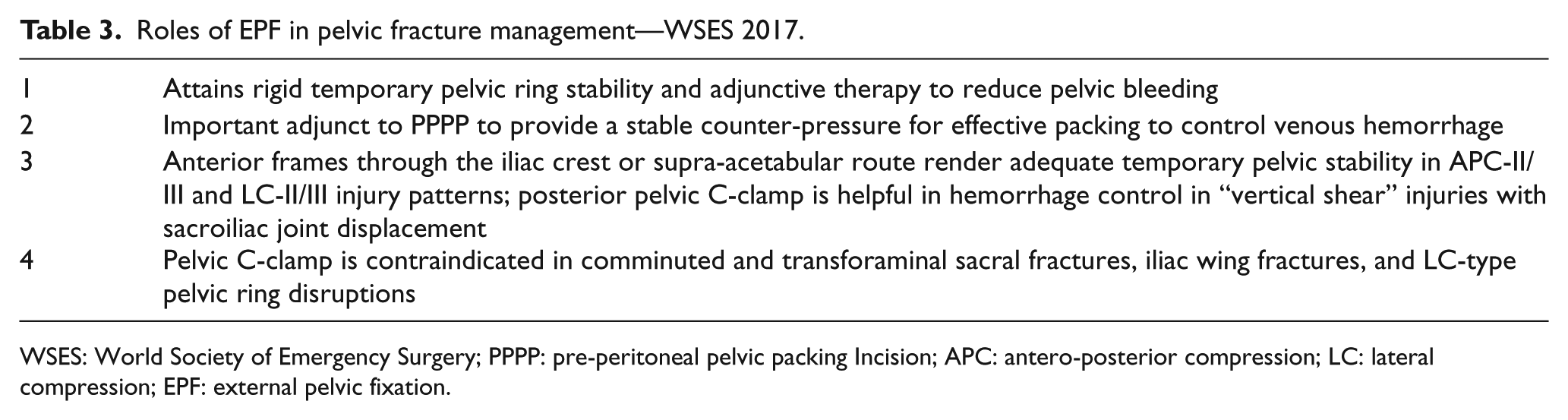
WSES: World Society of Emergency Surgery; PPPP: pre-peritoneal pelvic packing Incision; APC: antero-posterior compression; LC: lateral compression; EPF: external pelvic fixation.
Definitive anatomical reconstruction operation is to be performed 6–8 days (instead of 2–3 days) after injury to decrease the mortality.20,73 A prospective multi-center cohort study showed a substantial increase of hemorrhage and raised interleukin (IL-6 and IL-8) serum levels, indicating systemic inflammatory response exacerbation in polytrauma patients who had early pelvic fracture fixation on day 1 or 2 after injury. 74
The Hong Kong Queen Elizabeth Hospital Center revealed three-dimensional (3D) navigation-assisted minimally invasive percutaneous screw fixation (minimally invasive surgery (MIS)) for pelvi-acetabular fracture was safe with average operative bleeding and time of 179 mL and 141 min, respectively. There were no immediate or early surgical complications, and fracture healing was favorable. 75
If the hemodynamic instability continues after PPPP, urgent pelvic angiography with angio-embolization should be performed according to the Western Trauma Association guidelines. 29 In a study of 18 patients who underwent emergency PPPP, 80% of patients who had subsequent angiography had positive findings for arterial injury and received curative embolization. 76
In the situation of pelvic fracture–related hemorrhage, an aortogram with bilateral runoff is followed by selective injections into both iliac systems. If arterial extravasation of contrast is identified, selective temporary embolization with gelatin sponge is the choice. In case of indicated permanent embolization, N-butyl cyanoacrylate (glue) is employed in traumatic pseudo-aneurysm and coils for arterio-venous fistula. Abrupt cutoff of named vessels due to vascular spasm can be a sign of injury, indicating the need for embolization. 29 This approach is reported successful in 87% in one study. 76 A prospective study of angiography and embolization reports an 80% rate of embolization with pelvic and visceral angiography, with 95% effectiveness. 77
Pelvic angiography with bilateral internal iliac artery (IIA) embolization is safe with few major complications. Gluteal muscle ischemia or necrosis has occurred in patients with shock and prolonged immobilization, while the initial gluteal injury can be an etiology instead of the interventional complication.29,78 Besides, there is no significant male sexual dysfunction resulted. 79
When the hemodynamics is stabilized, the trauma patient should undergo the necessary CT scan and other imaging for thorough evaluation of the abdomino-pelvic injury and other concomitant polytrauma.
Commandment 8—pre-planned and explicitly documented protocol-driven team management shortens decision-making interval
In the past, it was often controversial in choosing what procedure (EPF/PPPP/angio-embolization) to perform first after initial hemodynamic optimization (because stabilization is not expected in exsanguinating pelvic fracture). The management of pelvic fracture with shock has been heterogeneous not only among different centers but also within the same hospital. 80
Because the main bleeding culprits (of around 90%) of severe pelvic trauma are the veins, pre-sacral venous plexus, bone marrows, and soft tissues (with arterial being 10%)66,78 and surgeons are usually more readily available as 24-h in-house staff, it is reasonable and also the current trend to start with PPPP (performed by the general or trauma surgeon with the pelvic binder (of comparable compression effect as EPF)) or after a quick conversion to the EPF (by the ortho surgeon) to provide the rigid fixation. The PPPP in a confined and stabilized pelvic cavity is considered to be the most important tamponade to control the venous/pre-sacral venous plexus bleeding as indicated in the Eastern Association for the Surgery of Trauma (EAST) guidelines. 78
Afterwards, the pelvic angiography is performed to identify any active bleeders for embolization if hemodynamic stability is not restored. Prophylactic temporary bilateral IIA embolization by gel foam is also performed even when hemodynamics is restored as a three-in-one interventional procedure (EPF, PPPP, and transcatheter arterial embolization (TAE)) for major pelvic fracture bleeding to achieve significant mortality reduction.
Cheng et al. 81 of the Hong Kong Queen Elizabeth Trauma Center has revealed in her historical comparison study a substantial mortality reduction from 63.5% in the EPF phase (1996–2001) to 42.1% with addition of angio-embolization (2002–2008) and to 30.6% by the three-in-one approach (EPF, PPPP, and angio-embolization; 2008–2011) with a bundle of trauma care evolution (trauma triage, diversion, team, operation theater (OT) access, and intensive care unit (ICU) care) through protocol establishment. Moreover, the three-in-one approach was identified as the most important independent positive factor for survival in a subsequent Hong Kong multi-center study with an overall mortality of 12.5% (2010–2014). 82
The WSES recommends the five steps in the management of major pelvic trauma with unstable hemodynamics as indicated in Table 4. 21
Pelvic fracture management—WSES 2017.
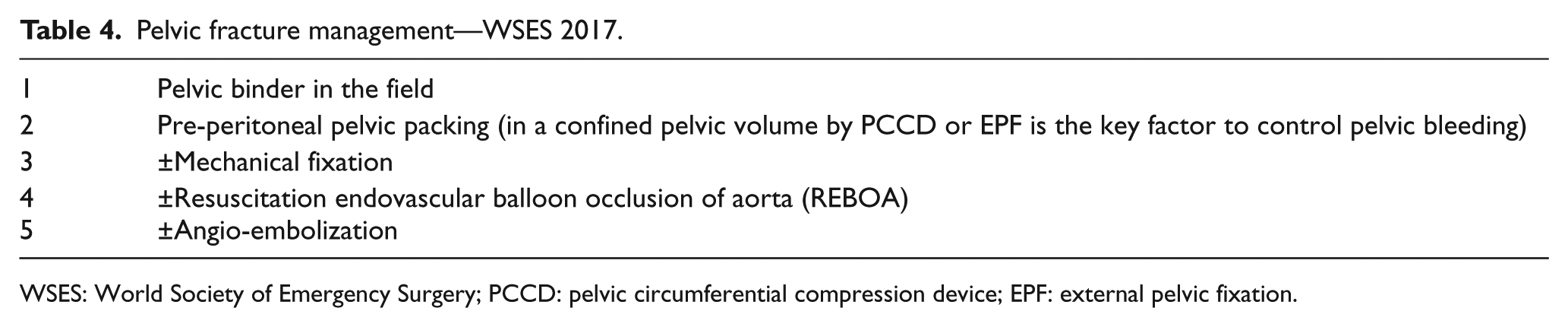
WSES: World Society of Emergency Surgery; PCCD: pelvic circumferential compression device; EPF: external pelvic fixation.
When the lethal triad of trauma (coagulopathy, acidosis, and hypothermia) has been overcome by the DCO and ICU care, subsequent pelvic ring disruption is managed by open reduction with internal fixation (OR + IF) or by the less invasive closed reduction and 3D navigation-assisted fixation by screws as discussed above.
The efficient and effective trauma care is delivered through teamwork led by a proficient leader with both sound clinical and communication skills. Successful trauma resuscitationist/resuscitologist expertise is attained by repeated exposure to gather the clinical experience together with ample mental rehearsal to systematically and promptly complete the complex multi-tasks through the coordinated teamwork with concerted effort. 83
When USG or DPA reveals hemoperitoneum, laparotomy should precede the pelvic intervention. Figure 3 shows a management algorithm in severe pelvic fracture (±abdominal injury).21,82
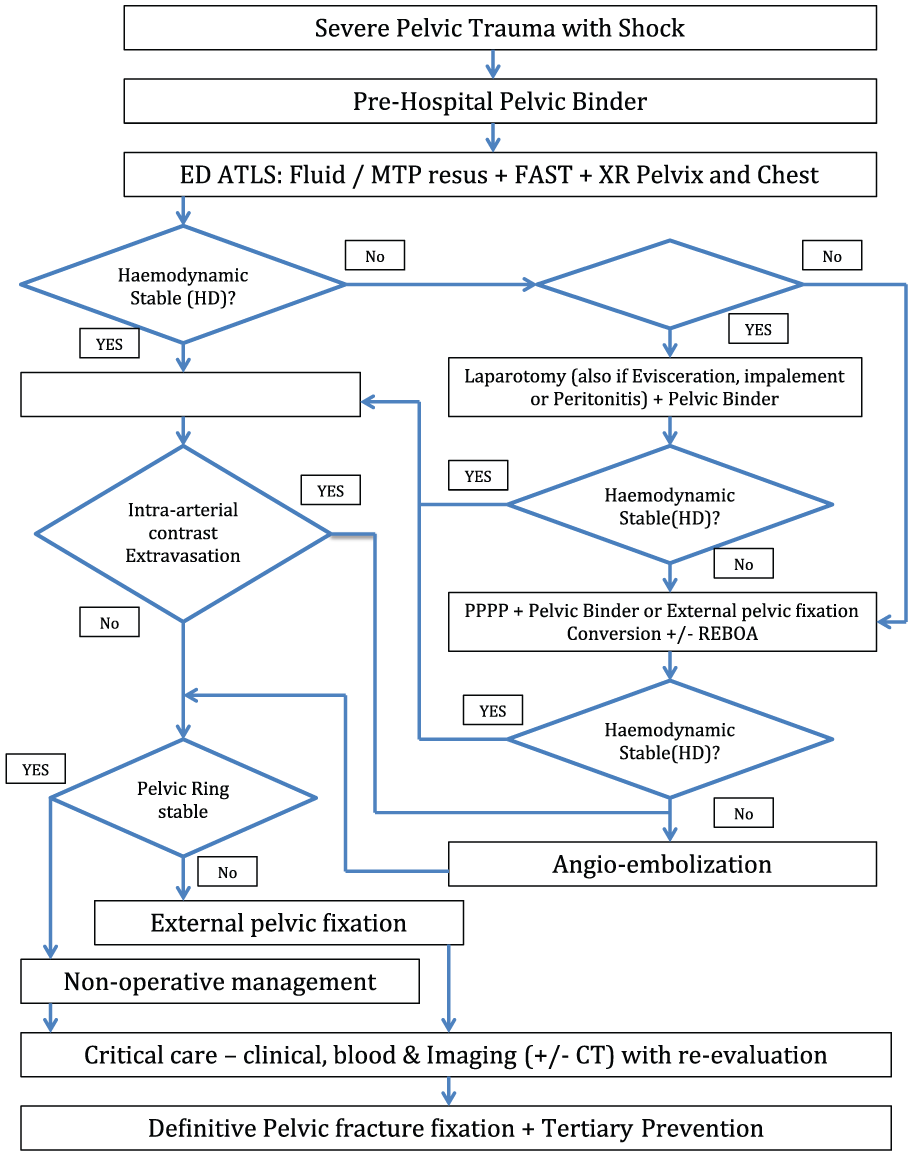
Management algorithm in severe pelvic fracture (±abdominal injury).
An important clinical pitfall is the omission to identify other concomitant extra-pelvic life-threatening hemorrhage such as hemoperitoneum, which may have higher treatment priority or can be managed simultaneously. Over 90% of major pelvic fractures are associated with other significant injuries. 84
Commandment 9—REBOA can be a temporizing device before DCO
REBOA is a new device to arrest or diminish the internal abdomino-pelvic bleeding of non-compressible torso hemorrhage (NCTH).85,86 When the inflated balloon is placed in the supra-diaphragmatic zone I in the descending thoracic aorta (from the left subclavian artery to the celiac artery), the intra-peritoneal and pelvic bleeding can be controlled while maintaining or improving the cerebral and coronary perfusion. Zone II of the aorta is between the celiac trunk and renal arteries. Zone III is between renal arteries and aortic bifurcation. When REBOA is positioned in zone III in the infra-renal site, the renal perfusion is maintained while the pelvic hemorrhage can be controlled.
REBOA effectively cuts off the blood supply to the lower body. Occlusion at zone I or II is least tolerated. Systematic review showed that the median occlusion time for zone I is 58.4 min, for zone II is 43.6 min, and for zone III is 55.2 min. 87 For zone I occlusion, it appears that less than 30 min is appropriate, but over 60 min is dangerous. Zone II is a visceral territory and deployment of balloon should be avoided. For zone III occlusion, 2 h is the appropriate cutoff time, although placement for up to 6 h has been reported but not recommended.88,89
The combination of REBOA and other endovascular hybrid
Endovascular resuscitation and trauma management (EVTM) procedures are becoming more prevalent in clinical trauma therapy including pelvic hemorrhage in major trauma services.90–93
New data have supported the positive survival outcome of REBOA in trauma patients and benefit of zone III REBOA including partial REBOA (incomplete balloon occlusion) and intermittent REBOA. 92
REBOA as compared with laparotomy is a minimally invasive procedure of substantially lesser metabolic and surgical demand on the shock subject.94–97
It can be a temporizing life-sustaining device while awaiting transfer to hospital, during secondary diversion, or when immediate access to the hospital operation theater for internal bleeding control is unavailable.19,98
Although REBOA can help save life, it carries major complication of lower limb ischemia.99,100 Small-caliber 7-Fr REBOA can help prevent the limb complications. 101
Another complication is the ischemia-reperfusion organ injury resulting in MOF, which might be prevented by short REBOA time, intermittent or partial REBOA.102,103
Partial REBOA refers to incomplete balloon inflation leading to incomplete aortic occlusion to maintain partial aortic flow to concurrently mitigate the adverse effects of complete aortic occlusion on both proximal and distal vascular beds while reducing the internal hemorrhage.
REBOA complications may occur in arterial access, balloon positioning, inflation, during occlusion, deflation, and removal of the sheath.
Commandment 10—the definitive treatment of injury is operation but the BEST is PREVENTION
It is not uncommon that many clinicians consider injuries as “accidents” and happen by chance and are beyond prevention. On the contrary, we should rename accidents as incidents, injuries (road traffic injuries (RTIs) instead of RTAs), crashes, or collisions in order to assess the cause and consequently evaluate the preventability in a serious manner.
The Haddon Matrix provides a very robust framework on the three strata of injury prevention from precrash, crash, and postcrash.104,105 Nowadays, prevention has been expanded to the primary, secondary, and tertiary level.
The input of the clinicians in conjunction with other professionals to the safe road and work design, community education, legislation to reduce risk, and law enforcement to achieve high standard of safety with constant re-evaluation is invaluable. The 6-E acronym including Education, Empowerment, Engineering, Enforcement, Economic Incentive, and Evaluation is a key principle of the Ontario Injury Prevention Guidelines of Canada. 106
In the population health impact pyramid, 107 the essential elements for favorable outcome are the positive socioeconomic factors, facilitation of healthy default decision of individuals, durable protective interventions, effective clinical intervention, and counseling with education.
In the Hong Kong situation, as a modern and peaceful civilian metropolitan city, blunt injury (including but not limited to pelvic disruption) predominates over penetrating trauma and is usually due to MVC/RTI or work/construction site or suicidal fall.108–112
Clinicians can contribute to primary injury prevention through community, school, and road safety and industrial education enhancement on promoting safe behavior and deterring risky behavior during travel/commuting or at work/in sports as well as the PPE use (safety belts and supplementary restraint system (SRS)—air bags, helmets, and other tools) in addition to the mental health maintenance to avoid deliberate self-harm.105,113,114
Secondary injury prevention refers to the harm reduction during the impact and harm containment soon after the injury.105,113,114 Clinicians may inform the engineers on impact force diminishment design concerning road construction, vehicle manufacture, and fall prevention devices. The formulation and implementation of a rapid response prehospital emergency medical service (EMS) with the fire fighters and ambulance crew are pivotal to attain the life-saving extrication and rescue procedures because time is blood and blood is life. The provision of a 24-h structured high-quality trauma team capable to perform DCR is another key element to maximize the victim’s outcome.
Tertiary injury prevention aims at avoiding the future re-injury by modifying the work, travel, sports, and activity behavior,115–117 which is often omitted in the ED owing to the short patient contact time or in the in-patient care due to a lack of holistic management. This should be attempted at any feasible stage in the patient’s treatment journey from hospital arrival to discharge, bearing in mind the psycho-status, comprehension ability, and preparedness of the patient and the family. A dedicated trauma nurse team supported by the allied health workers may provide the complementary service to attain the comprehensive treatment (from resuscitation, operative, rehabilitation, and prevention therapy) with the understanding that doctors are often too busy to provide the counseling. The participation of the psychiatrist, psychologist, and master of social work (MSW) cannot be overemphasized, especially in the suicide attempt subjects and those with significant financial and mental burdens.
Zero tolerance should be the goal if the injury is preventable and the consequence of severe trauma including and not limited to exsanguinating pelvic fracture leading to devastating disability or death with tremendous impact on patients, families, and society!
Best (safety) does not exist, always look for BETTER (safety)!
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.