
Abstract
Background:
Resuscitative endovascular balloon occlusion of the aorta is used as adjunctive management for a profound shock in some trauma centers. We report our early experience of resuscitative endovascular balloon occlusion of the aorta to describe the implementation and possible indications of resuscitative endovascular balloon occlusion of the aorta.
Objective:
This study was designed to investigate the feasibility and effectiveness of resuscitative endovascular balloon occlusion of the aorta based on our experience and share our implementation process by trauma surgeons in Korea.
Methods:
We performed a retrospective review of consecutive cases of resuscitative endovascular balloon occlusion of the aorta in profound shock due to noncompressible torso hemorrhage at a single Korean trauma center. Resuscitative endovascular balloon occlusion of the aorta was introduced and implemented with written protocol and endovascular training courses.
Results:
All cases (n = 24) were done for blunt mechanisms. Twelve cases (50%) were resuscitative endovascular balloon occlusion of the aorta in zone I, three cases (12.5%) were zone II, and nine cases (45%) in zone III. Mean pre-occlusion systolic blood pressure was 47 mm Hg and mean systolic blood pressure increase was 41.3 mm Hg. Twenty-one patients (87.5%) survived at trauma bay and seven patients (29.2%) survived and discharged without neurologic deficit. There were two complications directly related to the procedure.
Conclusion:
Resuscitative endovascular balloon occlusion of the aorta is a useful adjunctive skill for trauma surgeons, and a brief training course can help in the implementation of the procedure.
Introduction
Although resuscitative endovascular balloon occlusion of the aorta (REBOA) was first described in 1954, it was not used globally before the last decade.1–6 REBOA was practiced in Japan and Europe for a long time; however, there has been a recent increase in the utilization of REBOA in trauma centers in the United States. 7 The first case of REBOA in Korea was described in 2015, and since then, some trauma centers have begun using this procedure. 8
The goals of REBOA include the prevention or reversal of hemodynamic collapse by minimizing ongoing bleeding and restoration of adequate perfusion pressure to the heart, lungs, and brain. Before the introduction of REBOA, resuscitative thoracotomy and clamping of the descending aorta was the only procedure to achieve the above-mentioned goals. These procedures were very invasive and could induce possible complications, but the efficacy and survival in blunt trauma were very low, even when performed by the most experienced doctors. 9 Therefore, REBOA was introduced as an alternative procedure for better bleeding control and can be the “bridging modality” for trauma and non-trauma patients with life-threatening hemorrhage.
Despite the increasing use of REBOA, there have been a small number of studies with this technique as well as limited clinical studies regarding its effectiveness and complications. In addition, education, training, and post-REBOA management have not been clearly defined. The aim of this study was to investigate the feasibility and effectiveness of REBOA based on our experience and share our REBOA implementation process by trauma surgeons in Korea.
Method
Setting
Gachon University Gil Medical Center is an academic hospital with 1500 beds in Incheon city, South Korea, and serves a population of 3 million people. The regional trauma center of Incheon was the first trauma center established in Korea, and the overriding goal was to establish a regionalized Level I trauma center. The number of trauma-related admissions were more than 3000 per year, of which 500–550 patients have an injury severity score (ISS) of >15. The trauma center is equipped with a trauma bay, two operating rooms dedicated to trauma, a 20-bed dedicated trauma ICU, and a trauma interventional radiology (IVR) suite. Nineteen full-time trauma surgeons, four trauma coordinators, and nine physician extenders currently work at the center. Emergency physicians, anesthesiologists, and neurosurgeons are activated with trauma call as a member of trauma team. Furthermore, orthopedic consultants are available at all times.
Patients and data collection
Trauma patients who underwent REBOA at the regional trauma center of Incheon city between December 2015 and January 2019 were chosen as the participants. During this period, 24 patients underwent REBOA at the trauma bay or operation room. We did not exclude any patients, and the data were extracted from trauma registry of the trauma center. Data regarding the patient characteristics and physiologic status, initial systolic blood pressure (SBP), SBP just before REBOA, heart rate, initial fluid, blood transfusion, time courses, and SBP change after REBOA inflation were investigated. Laboratory data such as hemoglobin, pH, lactate, and base deficit were collected, and trauma scores were also calculated with commonly used formulas. Our institutional review board waived the need for obtaining informed patient consent because we used only existing materials and documents (approval number: 2018-037). Data were collected and processed anonymously; patients were able to refuse their participation at any time without any adverse consequences.
Protocol and education
To identify traumatic shock patients who needed REBOA, shock was defined as SBP < 90 mm Hg, shock index > 1.3, or base excess > 5. Among the patients in shock, patients who do not respond to the initial resuscitation with a liter of crystalloid and two units of RBC transfusion, or with impending cardiac arrest were considered for REBOA. Contraindications for the procedure included cardiac arrest for more than 10 min, mediastinal widening, and cardiac tamponade. Institutional indications for REBOA were initially agreed but not formally defined, and the decisions were made by the trauma surgeon in charge.
Aortic zones were considered as zone I, II, and III from cranial to caudal (Figure 1). Zone I is the descending thoracic aorta between the origin of the left subclavian and celiac arteries. Zone II is the para-visceral aorta from celiac arteries to the lowest renal artery and zone III is the abdominal aorta between the lowest renal artery and the aortic bifurcation. In most cases of profound shock and impending cardiovascular collapse, the target position could be zone I. If there is a pelvic injury or junctional femoral injury without thoracoabdominal injury, then the inflation of the balloon in zone III could be recommended. Because the inflation of the balloon in zone II is related to severe splanchnic ischemia, we should avoid zone II REBOA in any circumstances.
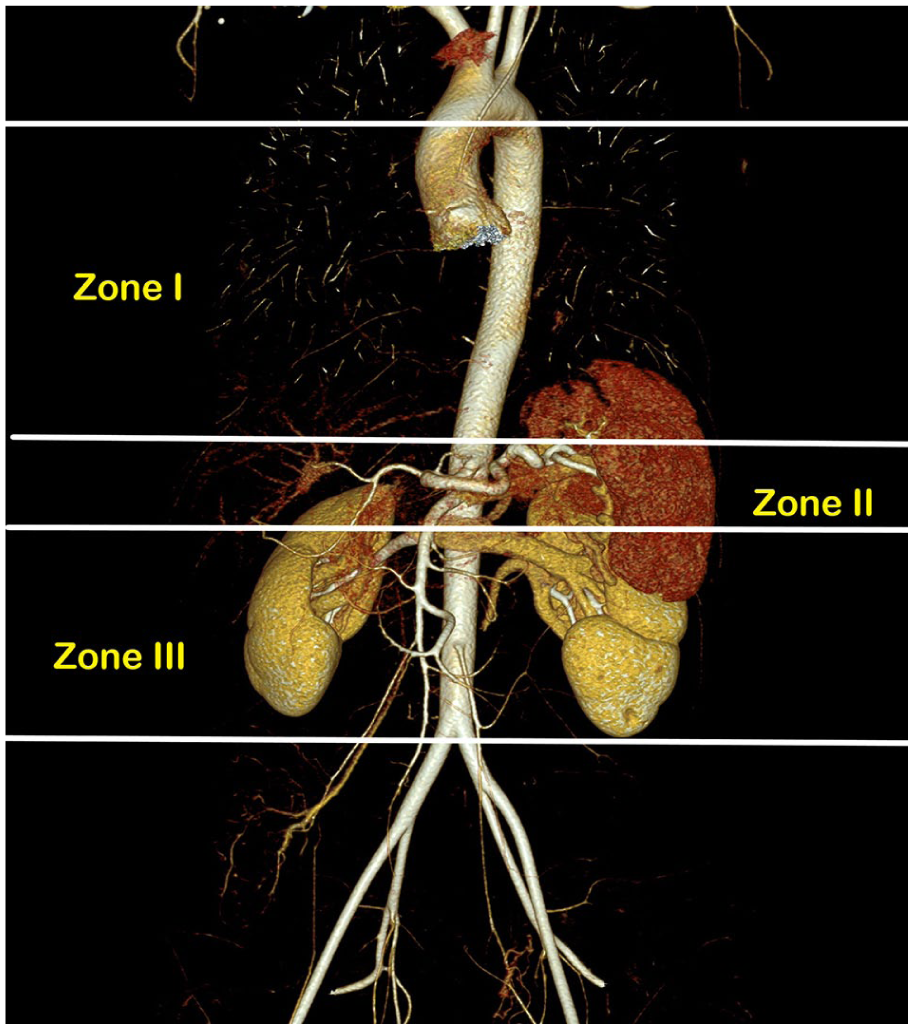
Aortic zones related to REBOA.
All of the aortic occlusion balloons were inserted by a trained trauma surgeon without radiologic assistance. A 5-Fr, 7-Fr, or 12-Fr sheath was inserted in the femoral artery, and the sheath size was selected depending on the availability of balloon catheters (Coda Balloon™, Rescue Balloon™). There was a written procedure protocol, and some trauma surgeons in our trauma center participated in REBOA and endovascular training courses in Korea; however, initially, only a few trained surgeons performed the procedure. Our center started a training course for vascular and endovascular skills for the trauma surgeons in 2017, and since then, all trauma surgeons are capable of performing REBOA.
Statistical analysis
Continuous data were presented as means and standard deviation, or median and interquartile range. A univariate analysis was performed using the Student’s t-test for continuous variables and the χ2 test for categorical variables. Statistical significance was achieved at p < 0.05. All statistical analyses were performed using the IBM SPSS PASW version 20.0.
Results
During study period, REBOA was performed in 24 severely injured trauma patients. The mechanism of injury was blunt trauma in all of the patients, and the mean age was 48.7 ± 17.5 years. Most of the patients (67.9%) were males with a mean ISS of 36.2 ± 12.3. The most common injuries that had an AIS (Abbreviated Injury Scale) > 3 were located in abdomen (Table 1). We used low profile balloon catheter (7 Fr) for 14 patients and used conventional catheter (12 Fr) for 10 patients. The utilization of REBOA increased since 2017 when we started the education courses in the hospital (Figure 2). Cardiopulmonary resuscitation (CPR) was performed in 42% of the patients (10/24) before REBOA insertion. The mean initial Glasgow coma scale score (GCS) was 9, and only one patient (4.2%) had a head injury with an abbreviated injury score of >3 (Table 1).
Baseline characteristics.
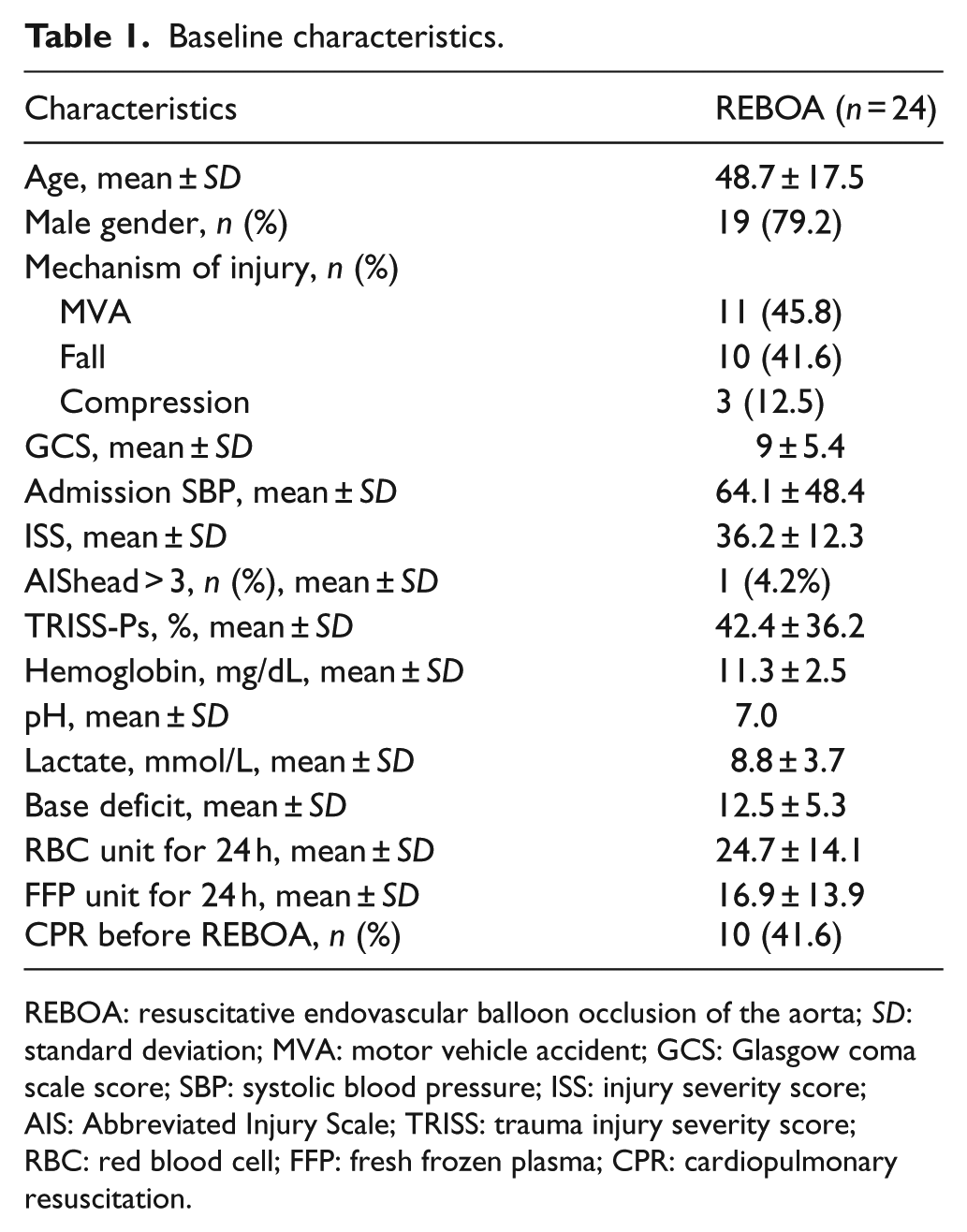
REBOA: resuscitative endovascular balloon occlusion of the aorta; SD: standard deviation; MVA: motor vehicle accident; GCS: Glasgow coma scale score; SBP: systolic blood pressure; ISS: injury severity score; AIS: Abbreviated Injury Scale; TRISS: trauma injury severity score; RBC: red blood cell; FFP: fresh frozen plasma; CPR: cardiopulmonary resuscitation.
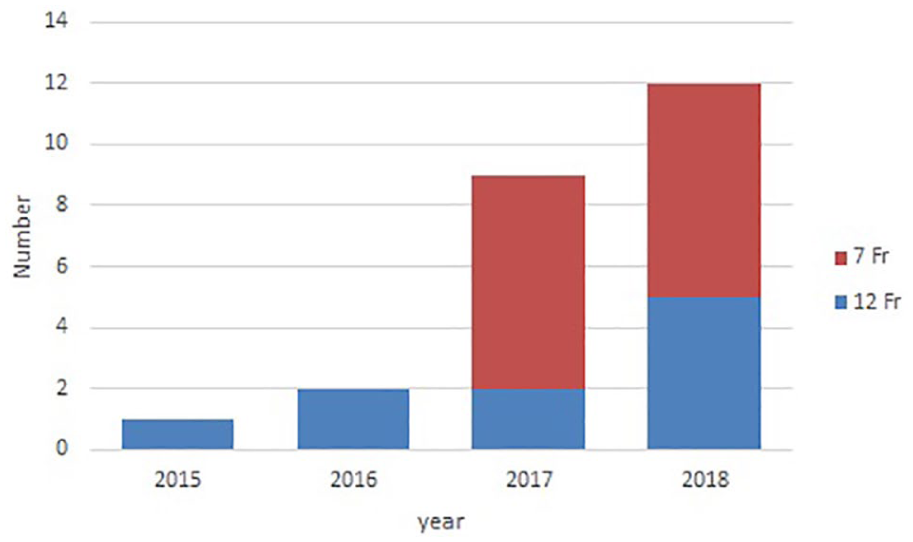
Number of REBOA—case numbers by year and used catheter type.
Femoral access, REBOA insertion, and balloon inflation were performed in the trauma bay except for one patient, who had these procedures performed in the operating room. The most frequently used balloon catheter were 7 Fr (58%) followed by 12 Fr (42%). Zone I occlusion was used in 58% of patients (Table 2). The most frequently used modalities to confirm the catheter position were X-ray (38%) and computed tomography (CT) (21%). Time from ER admission to REBOA insertion was 51.9 min and mean ER stay time was 93.4 min (Table 2).
REBOA characteristics and outcomes.
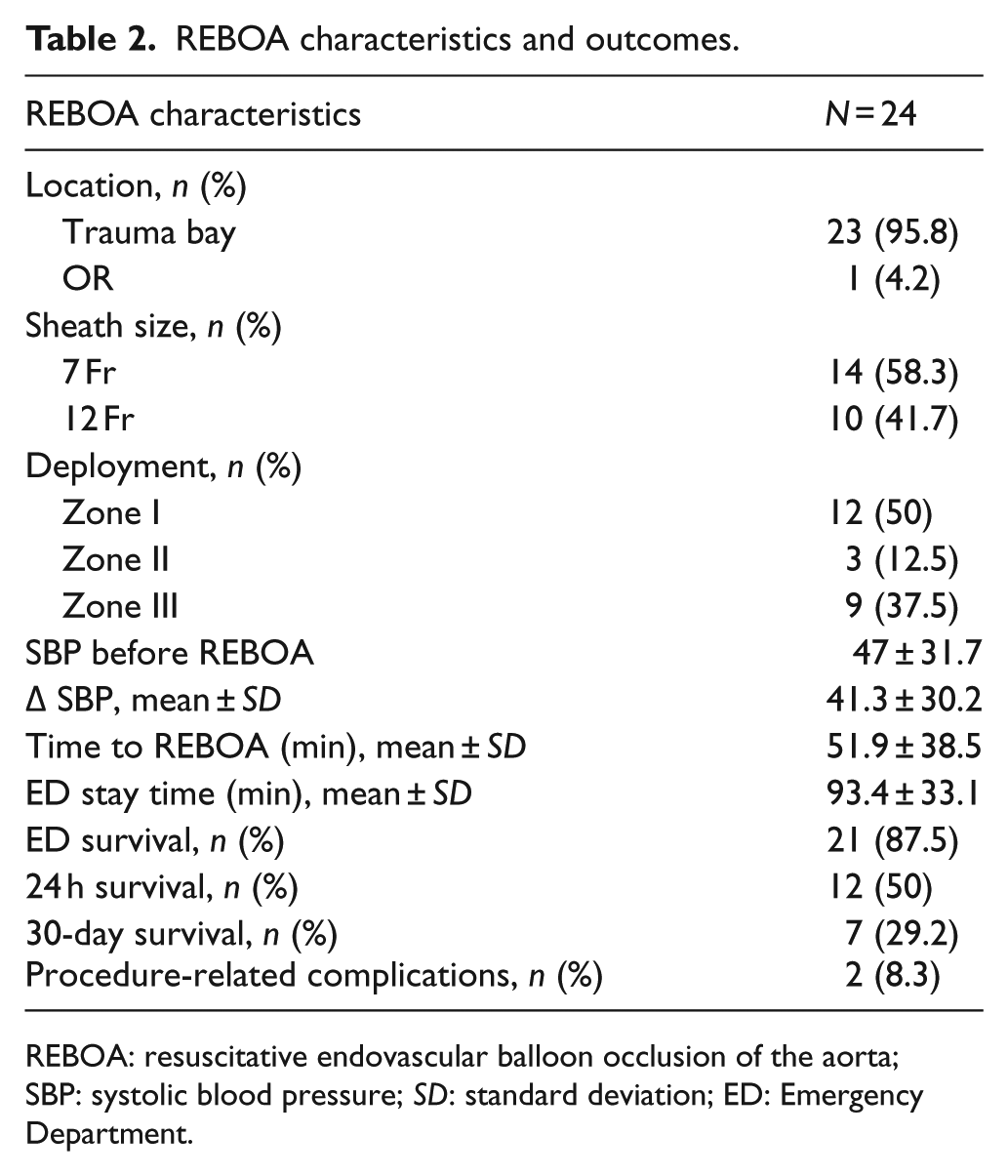
REBOA: resuscitative endovascular balloon occlusion of the aorta; SBP: systolic blood pressure; SD: standard deviation; ED: Emergency Department.
On admission, 75% (18/24) were in hemodynamic instability with a SBP of <90 mm Hg and mean SBP just before REBOA was 47 ± 31.7 mm Hg. Mean change of SBP after REBOA was 41.3 ± 30.2. Twenty-one patients (87.5%) survived at the emergency room, and the 24-h and 30-day survival rates were 50% and 29.2%, respectively (Table 2). Two patients (8.3%) experienced procedure-related complications (Table 2). The most common procedures for hemostasis were damage control laparotomy (DCL), preperitoneal pelvic packing (PPP), and IVR, respectively (Figure 3). The survivors showed significantly lower trauma injury severity score (TRISS), higher GCS, higher initial SBP, and lower rate of CPR before REBOA (Table 3).
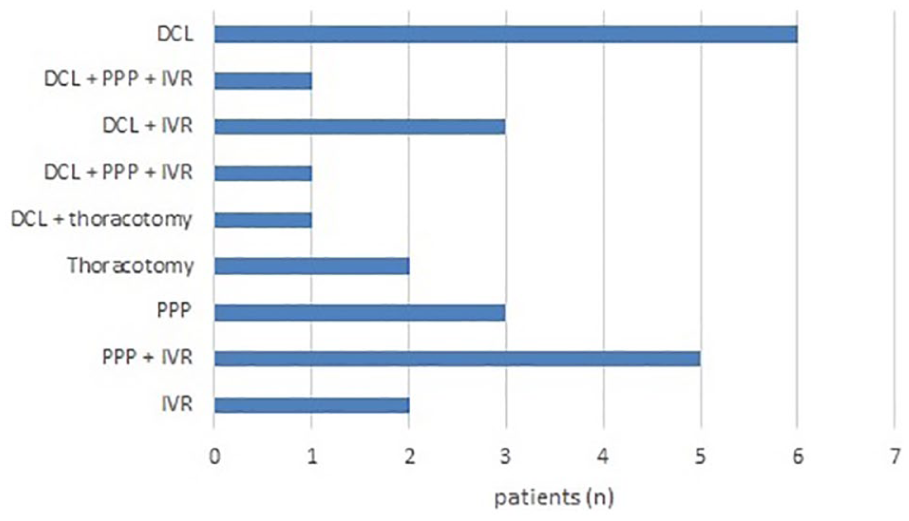
Procedures for hemostasis—every procedure including operation and IVR after REBOA placement.
Comparison of clinical features between survivors and fatalities.
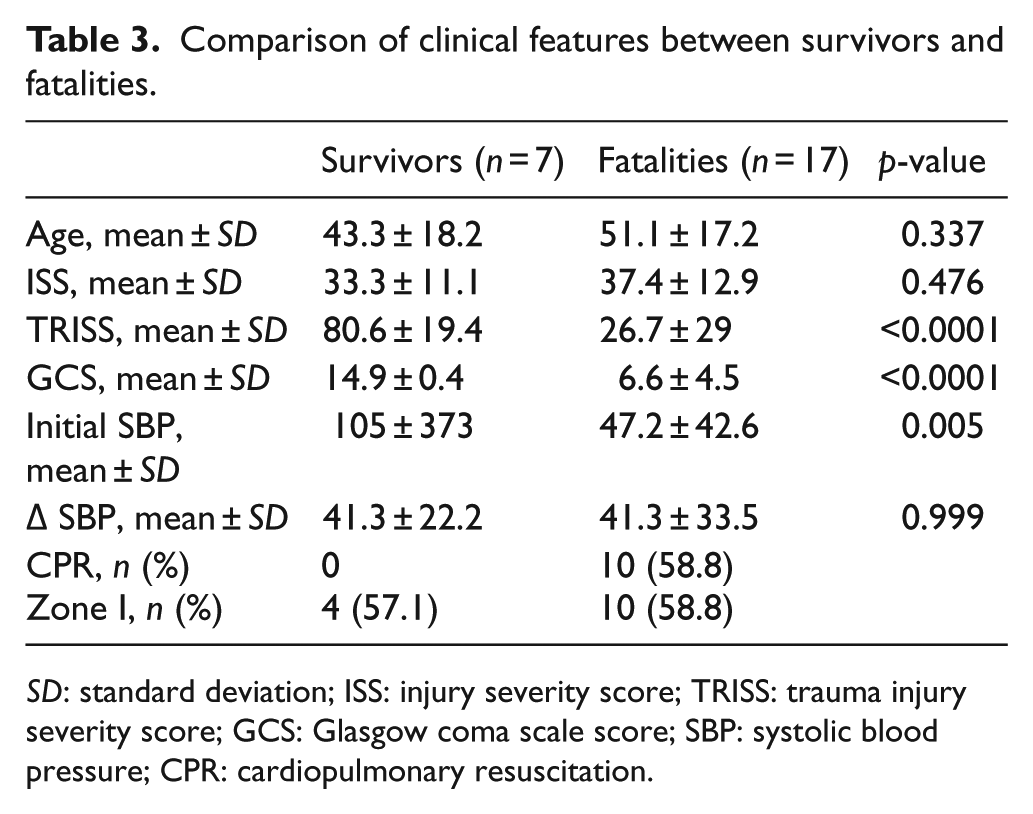
SD: standard deviation; ISS: injury severity score; TRISS: trauma injury severity score; GCS: Glasgow coma scale score; SBP: systolic blood pressure; CPR: cardiopulmonary resuscitation.
Discussion
Although the use of REBOA as an adjunct in traumatic shock patients has been rapidly increasing recently, there have been few large volume studies. Many trauma centers are trying to implement the REBOA technique, but numerous questions regarding the indications, contraindications, complications, and benefits of REBOA remain. Furthermore, educating and training surgeons and nurses remain problematic. Our experience with REBOA was in a small observational and preliminary study, but we believe our investigation can provide a description of the processes and problems regarding the implementation of the procedure at a trauma center. Furthermore, this is one of the first reports of REBOA implementation in Korea, and it can be a useful guide for the adoption of this procedure at other centers.
REBOA is a relatively simple technique and does not require the development of new specific devices. At the beginning of the REBOA implementation, we used the 12 Fr balloon (Coda, Cook Medical), which is not a specific product for REBOA. At that moment, only a few surgeons who had experiences in endovascular techniques could perform the procedure. After the 7 Fr balloon for REBOA (RESCUE, Tokai Medical) became available, we started educating and training surgeons and nurses who did not have specific knowledge on endovascular techniques. The training course includes the sheath placement with sonographic guidance, the sheath upsizing, and the placement of balloon catheter in the endovascular model. Because most surgeons are already familiar with Seldinger technique, after the one training course, most trauma surgeons were able to perform the procedure without serious problems or complications. Therefore, we believe that the implementation of the REBOA technique by surgeons with appropriate education and a training course is feasible.
Our results with patient outcomes after REBOA were similar to those in previous studies.10–14 Indications for REBOA included traumatic persistent shock such as SBP < 90 mm Hg, shock index > 1.3, or base excess > 5 from arterial gas analysis despite initial resuscitative efforts in patients with torso injuries. Cardiac arrest in the emergency room was not a contraindication, but the presence of a thoracic injury was a contraindication as many authors argued.10,12,15 However, we experienced a patient with severe thoracic injury who survived after REBOA placement. The patient fell from heights and initially was not in a shock state. During the initial assessment and resuscitation, the patient’s blood pressure dropped, and the patient was in impending cardiac arrest despite the resuscitation including transfusion. Although the patient’s chest X-ray revealed mediastinal widening, the trauma surgeon in charge decided to place REBOA at zone I to prevent cardiac arrest. After the REBOA, the patient’s blood pressure recovered. A CT scan revealed intercostal artery injuries and an aortic pseudoaneurysm. Subsequently, the patient underwent embolization immediately and survived. We still consider thoracic injuries as a contraindication, but this may change as more studies are published in the future.
The inflation of the balloon in the three zones are well described in many studies.2,5 As described earlier in this article, zone II is where the visceral arteries supplying the GI tract, liver, and kidney originate, which must be considered when doing REBOA. In theory, zone I occlusion still permits collateral or retrograde perfusion of the abdominal viscera, so zone II occlusion is discouraged. 16 There were three cases of zone II inflation in this study. In some circumstances of REBOA, the surgeon couldn’t check the balloon position before the inflation. After notification of the balloon position by X-ray or CT scan, the surgeon changed the position of the balloon from zone II to zone I. Especially it happened in the early phase of REBOA implementation. After the review of cases and re-education, zone II inflation of the balloon did not occur.
A delay in definitive hemostasis after REBOA can be a drawback that results in high mortality. A study from Japan showed that door-to-primary surgery over 60 min could worsen in-hospital mortality. 17 In our study, the emergency room stay time was 93 min on average. Although we did some procedures, such as pelvic packing in the trauma bay, it usually requires more time than the suggested time. The main reasons for delays include CPR, waiting for the IVR team, and diagnostic modalities such as whole-body CT scans. To improve the survival after REBOA in shock patients, the trauma team should clarify the protocol after the procedure.
Although there have been remarkable technological advancements, REBOA is still associated with various complications of vascular access and reperfusion ischemia.11,17,18 In particular, lower limb ischemia is a serious complication that can lead to amputation. 18 In our experience, procedure-related complications occurred in two of 24 patients, and all complications were directly related to sheath insertion. One patient had a thrombosis in the femoral artery bifurcation and underwent surgical thrombectomy on the following day. The patient required amputation, but it was because of chronic osteomyelitis. Another patient developed sheath site hematoma that did not need any further treatment. Both complications occurred when we used the 12 Fr REBOA catheter. Some studies have reported that small sheaths for REBOA may be related to lower complication rates.19,20 Although we could not show the exact data regarding the occlusion type, there have been some studies that reported non-continuous aortic occlusions such as partial and intermittent occlusions. 10 Overall, these techniques may reduce ischemic complications.10,15
This study has some limitations. First, there was a lack of a proper comparison group to evaluate the efficacy of REBOA. Second, because this was a retrospective study, it was difficult to document some data related to the procedure. In particular, it was difficult to accurately document the durations of the inflation and deflation times. Third, before the trauma surgeons were trained, only some surgeons were able to perform REBOA, suggesting that there were more patients who were candidates for REBOA. Therefore, there was an obvious selection bias. Also, the number of patients was too small to show any significant outcomes. Finally, because most patients died within 24 h, there were only two procedure-related complications. We believe there could have been more procedure-related complications if there were more long-term survivors.
Conclusion
Our initial experience showed that REBOA can be an effective “bridging therapy” for severe hemorrhagic shock patients due to sub-diaphragmatic hemorrhage. The introduction of this procedure to clinical settings in trauma centers did not require an extensive training program for trauma surgeons. Instead, a well-structured brief orientation and simulation training were required to prepare the trauma team for the implementation of REBOA to the trauma center. REBOA is a useful adjunctive skill for trauma surgeons, and a brief training course can help in the implementation of the procedure.
Footnotes
Author contributions
Y.P. and B.Y. had full access to all the data and drafted the manuscript. J.L., G.L., A.H., and K.C. participated in the study design and the education.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data and materials can be made available to the public through direct requests to the corresponding author.
Informed consent
Written informed consent was obtained from each patient included in the study.
Ethical approval
This study has approval from Gachon University Ethics Committee (approval number: 2018-037).
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.